Embed Size (px)
Citation preview

S113Abstracts / Brachytherapy 13 (2014) S15eS126
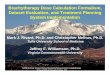
types, seed strength did not influence the relative rectal dose changeswith rectal separation in the source strength ranges studied (two tailedprobability p50.23).Conclusions: Irrespective of the seed type, reduction in rectal separationis associated with increase in rectal dose. Changes in rectal separationsin the 2 to 6mm range due to edema resolution or seed displacementwill result in higher magnitude of rectal dose changes from plannedfor Pd-103 seed implants compared to I-125 or Cs-131 seed types, dueto higher radial dose function of Pd-103 seed. Clinically, the potentialfor larger variation in planned rectal dose with prostatic edemaresolution should be considered while implanting Pd-103 seeds in theclose proximity of rectum.
Figure 1. Rectal Dose vs. Rectal Separation: A Dosimetric Study from a
Single I-125. Cs-131 and Pd-103 Seed.
PO60
5-Alpha-Reductase Inhibitors in Combination with Permanent Seed
Prostate Brachytherapy
Daniel Taussky, MD1, Vimal Krishnan, MSc2, Guila Delouya, MD1.1Radiation Oncology, University of Montreal, Montreal, QC, Canada;2University of Montreal, Montreal, QC, Canada.
Purpose: A combination of permanent seed brachytherapy (PB) with 5-alpha-reductase inhibitors (5-ARI) has the potential benefit of increasingthe efficacy of radiation through its antiandrogen effect. We investigatedthe effect of a combination of 5-ARI and PB on biochemical control andurinary symptoms post-PB.Materials and Methods: We identified 49 patients from our database of850 patients treated with at least 1 month of 5-ARI before PB with I125
between 2005 - 2011 and with a minimum followup of 2 years. Mediantime (range) of a 5-ARI before PB was 3 months (1-12) and mediantreatment duration after PB was 1 months (1-7).All patients had either low risk or low-tier intermediate risk prostate cancer.A 5-ARI was most commonly prescribed because of either the waitingperiod for PB was judged too long by the patient or physician, to reduceprostate volume for an easier implant or for urinary symptoms pre-PB.Patients were seen 1 month after PB and if urinary symptoms werejudged as reasonable, the 5-ARI was stopped at that time. Patients takinga 5-ARI were compared to 236 patients randomly chosen amongst thosewho did not receive any 5-ARI. IPS scores and biochemical control datawas collected at 1-4-months intervals for the first year. Biochemicalfailure (bF) was defined as nadir þ2. Both groups were compared usingT-test or Fisher’s Exact Test.Results: Pre-treatment PSAwas significantly lower (p50.017) in the 5-ARIgroup (mean55.1ng/mL) than in the control group (6.1ng/mL). Prostatevolume at the time of PB was similar (38.9 cc for 5-ARI vs. 37.5 cc,p50.43) as well as the IPSS baseline score (4.45 vs. 4.53, p50.91).
Although there was no bF in the 5-ARI group compared to 3.8% in thecontrol group, this was not statistically significant (p50.37 Fisher’s ExactTest and p50.30 Log Rank test). This could be due to a significantlylonger (p5!0.001) followup in the control group (mean 46.8 vs. 33.4months). The last PSA in patients without any bF between both groupswas not significantly different (p50.83, mean 0.32 vs. 0.28 ng/mL) butthe time to nadir was much shorter (p!0.001) for patients in the 5-ARIgroup (mean 25.4 months SD14.2 vs. 40.4 months SD 17.5). In the 5-ARIgroup there was a trend (p50.084) towards less PSA bounces (18.4% vs.31.8%, RR50.48, 95% CI 0.223-1.047). IPSS within the first yearbetween the two groups were not different (p50.5-0.9).Conclusions: Our data suggest that short-term 5-ARI use potentiates theeffect of PB. The PSA bounce rate has nearly halved and there was ashorter time to PSA nadir and so far no recurrence has occurred inpatients with a 5-ARI. Urinary symptoms were not different within thefirst year.
PO61
Salvage Low-Dose-Rate 125Iodine Partial Prostate Brachytherapy
after Dose-Escalated External Beam Radiotherapy
Lynn Chang, MD1, Mark K. Buyyounouski, MD2. 1Radiation Oncology,
Fox Chase Cancer Center, Philadelphia, PA; 2Radiation Oncology,
Stanford University, Stanford, CA.
Purpose: To report outcomes on 5 patients treated with salvage partial low-dose-rate (LDR) 125iodine (125I) permanent prostate seed brachytherapy(BT) for biopsy proven locally persistent prostate cancer following failureof dose-escalated external beam radiotherapy (EBRT).Materials and Methods: A retrospective review of the Fox Chase CancerCenter prostate cancer database identified five patients treated with salvagepartial LDR 125I seed implant for locally persistent disease following dose-escalated EBRT. All patients had post-EBRT biopsies confirming unilaterallocally persistent prostate cancer. Pre-treatment, EBRT and BT details andpost-treatment characteristics were documented and assessed.Results: The median followup post-implant was 41 months. All fivepatients exhibited low acute genitourinary and gastrointestinal toxicities.Increased erectile dysfunction was noted in three patients. There were nobiochemical failures following salvage LDR 125I seed BT to date, with amedian post-salvage PSA of 0.4 ng/mL.Conclusions: In carefully selected patients with local persistence ofdisease, partial LDR 125I permanent prostate seed implant appears to bea feasible option for salvage local therapy with an acceptable toxicityprofile. Further study is needed to determine long-term results of thisapproach.
PO62
Toxicity Associated with High-Dose-Rate Monotherapy for Prostate
Cancer
Robyn Banerjee, MD1, D. Jeffrey Demanes, MD2, Sang-June Park, PhD2,
Sherif Gamal, MSc3, Alexander Rodgers, BSc4, Julia M. Fallon, BSc2,
Mitchell Kamrava, MD2. 1Oncology, University of Calgary, Calgary, AB,
Canada; 2Radiation Oncology, University of California Los Angeles, Los
Angeles, CA; 3Clinical Oncology and Nuclear Medicine, Mansoura
University Hospital, Mansoura, Egypt; 4University of California Los
Angeles, Los Angeles, CA.
Purpose: High-dose-rate (HDR) monotherapy is associated with favorableoutcomes and low toxicity for the treatment of favorable risk group prostatecancer. Given multiple treatment choices associated with excellent diseasecontrol, comparing adverse effects is key to patient and physiciandecision making. Detailed HDR toxicity analyses, however, are few. Inthis study we prospectively assessed toxicities in a recent cohort of HDRmonotherapy patients using several validated symptom scoring instruments.Materials and Methods: Toxicity analysis was carried out on 52consecutive patients treated between March 2010 and February 2012.HDR monotherapy was delivered in two separate implants, 1 week apart,