Embed Size (px)
Citation preview

Safety and Risk/Benefit Analysis ofWwtilide for AcuteConversion of Atrial
Fibrillation/FlutterPeter R. Kowey, MD, James T. VanderLugt, MD, John R. Luderer, MD
5ofetydatuwerereviewedfromseveralcontrolledclin-iccaltrialsof ibutilide,anewclassIIIantiarrhythmicdrugrecentlyapprovedfortheacuteinterruptionofatrialfib-rillationand flutter.Noncardiovascularadverseeffcktsof ibutili&weresimilarin frequencytothosew“thpla-cebo.Cardiovascularadverseeffectsoccurredin24.9%of 586 ibutilide-treatedpatienk as comparedwith22.2%of 108sotalol-treatedpatients,and7.1%of 127patientswho receivedplacebo.Polymorphousventric-ulartuchycardia,diagnosedastorsadesdepoinies,wasmorecommonwithibutilidethanwithplaceboorsotaloltreatment.Itoccurredin4.3%ofpatients,including1.7%0whose tarsades de pointeswassustainedandrequiredcardioversion.In theibutilidegroup,4.9’XO of patientshadnonsustainedmonomorphicventriculartachycardiacomparedwith3.7??of patientswho receivedsotcdaland 0.8%of patientswho receivedplacebo.All of thesustainedarrhythmiasexcept1 wcurredwithin1 hourof theendof ibutilideinfusion,andallweresuccessfully
terminatedwithoutsequelae.In a multiplelogisticre-gressionanalysis,bmdycardia,lowbodyweight,andhistoryofcongestiveheartfailurewerepredictiveof theoccurrenceof torsadesde pointes.Hypatension,con-ductionblock,bradycardia,andallothercardiovascularadverseeffectsalloccurredatsimilarratesintheibutil-ide-andplacebo-treatedgroups.Forpatientswhofailedto convertwhilereceivingibutilide,therewas no de-creasein theefllciencyof cardioversion,norwastherean increasein themeanenergyrequirementsfor sub-sequentelectricalcardioversion.Analysisof a 3-monthfollow-upstudyshowedthatpatienkreceivingibutilidehadsimilaroutcomescomparedwithpatientsreceivingplacebo.One placebo-treatedpatientdied.~er thantorsadesdepointes,ibutilidehasaverygoodsafetypro-file.Undertheproperclinicalconditions,thiscomplica-tionof ibutilidetherapycanbe rapidlydiagnosedandeffectivelytreated.
(AmJCardiol1996;78(suppl8A):46-52)
1’he efficacy of ibutilide for the acute conversionof atrial fibrillation and atrial flutter (Afib/Aflu)
has been established in well-executed placebo- andpositive:controlled clinical trials, several of whichare detailed in this review.1’2Ibutilide delays depo-larization and, “likealmost all other drugs producingthis electrophysiologic effect, it can cause torsadesde pointes.3The central issue in determining the clin-ical utility of ibutilide is one of assessing its relativesafety. In preparation for an extensive review con-ducted by the Cardiorenal Advisory Panel of theFood and Drug Administration, we examined all ofthe safety data from trials that had been conductedup to the time of that review and attempted to asse’ssthe risldbenefit ratio of ibutilide in the intended treat-ment groups. This report contains a review of thatinformation, specifically as it relates to terminationof acute arrhythmia.
METHODSThe clinical trials from which information was
extracted for this analysis are listed in Table I.They include Phase I studies of the effects of ibu-tilide in normal volunteers in the cardiac electro-
From the Division of Cardiovascular Diseases, !-ankenauHospital andMedical Research Center, Wynnewood, Pennsylvania (P,R.K.); De-partmentof Medicine, JeffersonMedicol College, Philadelphia, Penn-sylvania; and Phormacia & Upiohn, Kalamazoo, Michigon (J.T.V.,ID)\
J. N. L./.
Address for reprints: PeterR. Kowey, MD, I.onkenauMedical Of-fice Building East, Suite 556, 100 lancoster Avenue, Wynnewood,Pennsylvania 19096,
physiology laboratory, dose-ranging studies, andplacebo- and positive-controlled efficacy trials.Of the 1,049 patients who were exposed to thedrug, 586 were included in the main efficacy anal-ysis. The remaining patients received ibutilide inPhase I studies of hemodynamic and electrophys-iologic effects, or were drawn from efficacy trialsin progress. Safety data from ibutilide-treatedsubjects were compared with the incidence of ad-verse effects in 127 placebo- and 108 sotalol-treated patients.
Safety data were extracted from individual casereports submitted by individual investigators andcategorized into cardiovascular and noncardiovas-cular adverse experiences. A panel of consultants re-viewed recordings of ‘sustained arrhythmia eventsfrom all of the trials, as well as Helter monitor re-cordings that were made in the sotalol comparisontrial. The cardiovascular events were segregated byarrhythmia and nonarrhythmic effects, and were or-ganized by the degree of “seriousness” as deter-mined by the investigators.
A multiple logistic regression analysis using 19clinical variables was conducted to ascertain whetherany clinical characteristic could identify patients atrisk of developing torsades de pointes. This was donein 2 steps. The first was an exploration of a possiblerelation using a univariate analysis, and the second,a stepwise logistic regression analysis of variablesthat were significantly correlated in the first step. Asa general expression of the relative safety of ibutil-ide, and to test the correlation of adverse effects with
46 01996 by ExcerptaMedico, Inc.All rightsreserved.
0002-9149/96/$15.00PllS0002-9149(96)00566-8
TABLEI Clinical Program—Number of Sublects
placebo Sotalal Ibutilide
Healthyvolunteers 19 88Hemodynamics/electrophysiology 12 — 90Atrial fibrillation/airialfluhr
PilotDose_FindingStudies(0003, 0005) 36Dose-ResponseStudy(0014) 11 — 159RepeatDose Study (0015] 86 — 180S@alolComparisonStudy(0019) — 108 211
Total in atrial fibrillation/atrial flutter 127 loft 586
Number in completedtrials 158 108 76AEstimatednumberin ongoing trials 66 — 285
Total in completedond ongoingtrials 224 108 1,049
Numbers in parentheses represent protocol identification number.
TAMEII Medical Eventsby Body System (Incidence >1 %)
Placebo, % Sotalol, % Ibutilide, %Body System (n = 127] (n= 108) ~ (n= 586)
Whole bodyCardiovascular”DigestiveMetabolic/nutritionalNervousRespiratorySkinUrogenital
15.07.17.12.42.45.50.8
I 2.4
7.422.2
2,81.94,66.51.90.9
8.524.9
3.12.92.62.71.02.0
I *lb.tilidesignificqn+ly dihrenttromplaceboi. theplacekontrolledstidies;psO.O5.
I TABLE III Selected Cardiovascular Medical Events
I Placebo, % Sotalol, % Ibutilide, %(n = 127) (n = 108) (n = 586)
VentricularextrosystOles*Atrial tachycardiaHypotensianBundlebranch blockAV blockBradycardiaAngina pectorisPolymorphicVT
SustainedNon.sustoined
Monomorphic VTNonsustained
0.8 (1]0.8 [1)1.6 (2)– [0)0.8 (1)0.8 (1]– (o)
– [0]– (0)
0.8 (1)
1.9 (2)– (o)4.6 (5)6.5 (7)1.9 (2]6.5 (7]– [0)
– (o)– (o)
3.7 (4)
5.1 (30]2.7 (16]2.0 (12)1.2 (11)1.5 (9)1.2 (7]0.7 [4)
1.7 (lo) o.7-2.7%t2.6 (15) 1.3–3.9%T
4.9 (29) 3.2-6.6%T
●Significantly different from placek, p s0.05.
‘Confidence intervals (95%}.
dose, we constructed dose–response tables of effi-cacy and toxicity variables using the doses actuallyemployed in the trials.
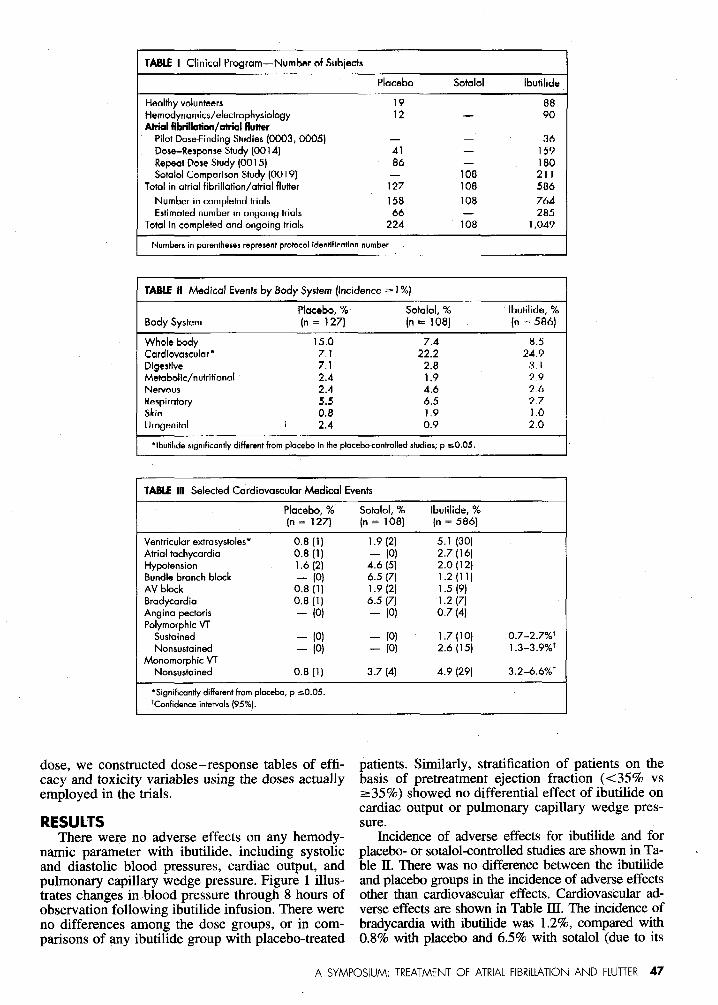
RESULTSThere were no adverse effects on any hemody-
namic parameter with ibutilide, including systolicand diastolic blood pressures, cardiac output, andpulmonary capillary wedge pressure. Figure 1 illus-trates changes in blood pressure through 8 hours ofobservation following ibutilide infusion. There wereno differences among the dose groups, or in com-parisons of any ibutilide group with placebo-treated
patients. Similarly, stratification of patients on thebasis of pretreatment ejection fraction (<35% vs=35~o) showed no differential effect of ibutilide oncardiac output or pulmonary capillary wedge pres-sure.
Incidence of adverse effects for ibutilide and forplacebo-or sotalol-controlledstudiesare shown in Ta-ble II. There was no difference between the ibutilideand placebo groups in the incidenceof adverse effectsother than cardiovasculareffects. Cardiovascular ad-verse effects are shown in Table III. The incidence ofbradycardia with ibutilide was l.2’%o,compared with0.870 with placebo and 6.5940with sotalol (due to its
A SYMPOSIUM: TREATMENT OF ATRIAL FIBRILLATION AND FIUTTER 47
5-Changainayatolkblood preaaura
,s. .*
mmHg .5.
-1o-
-15 ,012345676
Time (houra)
5Change in diaatolic bloodpressura
0.
mmHg .5.
-10.
-15
012345676Tima (hours)
---- Placebo (N=41)
----0.005 mg/kg (N=41)
- -0.010 mg/kg (N=40)
.--- .0.015 mglkg (N=36)
— 0.025 mg/kg (N=40)
FfGURE 1.Cho esinsystolic(top)anddiastolic(bottom)blood%rpressureinthe se-responsestudy.Tharawarenodifferences
amen the 4 dose groups,orbetweenanyparticulardosegroupmclptrcabo-traatadpoiients.
&blocking properties). There was one death in thetrial: a patientwho died of respiratorydecompensation4 hours after receiving a placebo infusion.The inves-tigatorand the consultantsdid notbelievethat the deathwas due to study medication.
The majority of cardiovascular adverse effectsnoted with ibutilide were ventricular tachyarrhyth-mias (Figure 2). There was a higher incidence ofpolymorphic and monomorphic ventricular tachy-cardia (VT) in patients treated with ibutilide as com-pared with other groups (Table III). Based on theinvestigators’ opinions and an analysis by the panelof experts, all of the episodes of polymorphic VTconstituted torsades de pointes. The association withQT prolongation, pattern of initiation, and charac-teristic morphology were thought to confirm this di-agnosis. Torsades de pointes occurred coincidentallywith QT prolongation and when ibutilide concentra-tions were at a maximum (Figure 3). All of the ep-isodes of sustained torsades de pointes except 1 oc-curred within 1 hour of dosing and all weresuccessfully terminated electrically. In 2 of the 10cases of sustained torsades, multiple shocks were re-quired to restore electrical stability. Sustained mono-morphic VT was not seen in any of the groups, buta nonsustained arrhythmia of uniform morphologywas seen in 29 patients who received ibutilide. Theelectrocardiographic recordings obtained from allpatients with a diagnosis of nonsustained monomor-phic VT were reviewed by the panel of experts. At
TAMEfv PosttreatmentPatient Experience; 3-MonthRetrospectiveFollow-up Data
Placebo, % Ibutilide, ‘%(n = 188) (n = 313)
Any event 47.5 (56) 44.1 (138)Death 3.4 [4] 3,5 (11 )Cardiovascularevent 32.3 [38] 34.8 (109)
Ventriculartachyarrhythmia’ 1.7 (2) 2.6 (8)
*includessustained❑nd nonsustainedmonomorphicand polymorphic VT,
ventricular fibrillation, and ventricular tochycordia.
TA6LE V Electrical Cardioversion in Nonresponders
Placebo Ibutilide p Value
Atrial flutterSuccessfulcardioversion 86% [25] 95% (18) 0.3441Meon numberof shocksta canvert 1.4 1.2 0.1973Mean ioulesto convert 240 178 0.2392AtriolWrillatianSuccessfulcardioversion 76% (19) 88% (30) 0.2158Mean numberaf shocksto convert 1.8 1.6 0.2742Mean’ ioulesto convert 454 321 0.0740
Foratrial flutter, n = 29 and 19 for placebo and ibutilide, respectively; for
atrial fibrillation, n = 25 and 34, respectively. Numbers in parentheses corre-
spond to the percentage shown.
least 40% were considered aberrant conduction ofAfib/Aflu, and another 50% were considered ques-tionable, with no consensus as to the mechanism ofthe arrhythmia.
The multiple logistic regression analysis identi-fied 3 factors predictive of the development of tor-sades de pointes—small body size (independent ofthe dose received; p = 0.0093); a history of conges-tive heart failure (p = 0.0033); and slow pretreat-ment heart rate (p = 0.00’46).The occurrence of tor-sades de pointes was independent of total dose, doseper kilogram, gender, or pretreatment QT interval.Patients who had a long QT interval, hypokalemia,or other factors that might predispose to torsades depointes had been excluded from the trials.
Follow-up information was gathered for 3months from 431 patients —3’l3 received ibutilide,and 118 received placebo. The clinical outcomesof these 2 groups were identical. There was no in-crease in the occurrence of serious adverse eventsor an excess of deaths during the 90 days aftertreatment (Table IV).
An analysis of outcomes for patients who re-ceived ibutilide and did not convert to sinus rhythmshowed that the majority of these patients went onto have electrical conversion. The rate of successfulelectrical conversion was comparable in those whoreceived ibutilide or placebo before cardioversion,but the cumulative amount of energy necessary toconvert Afib/Aflu to sinus rhythm was less in theibutilide-treated patients, but was not statisticallysignificant (Table V).
Finally, efficacy and safety across the entire doserange used in the trials was plotted as a graphic dis-
48 THE AMERICAN JOURNAL OF Cardiology@ VOL 78 (8A) OCTOBER 17, 1996
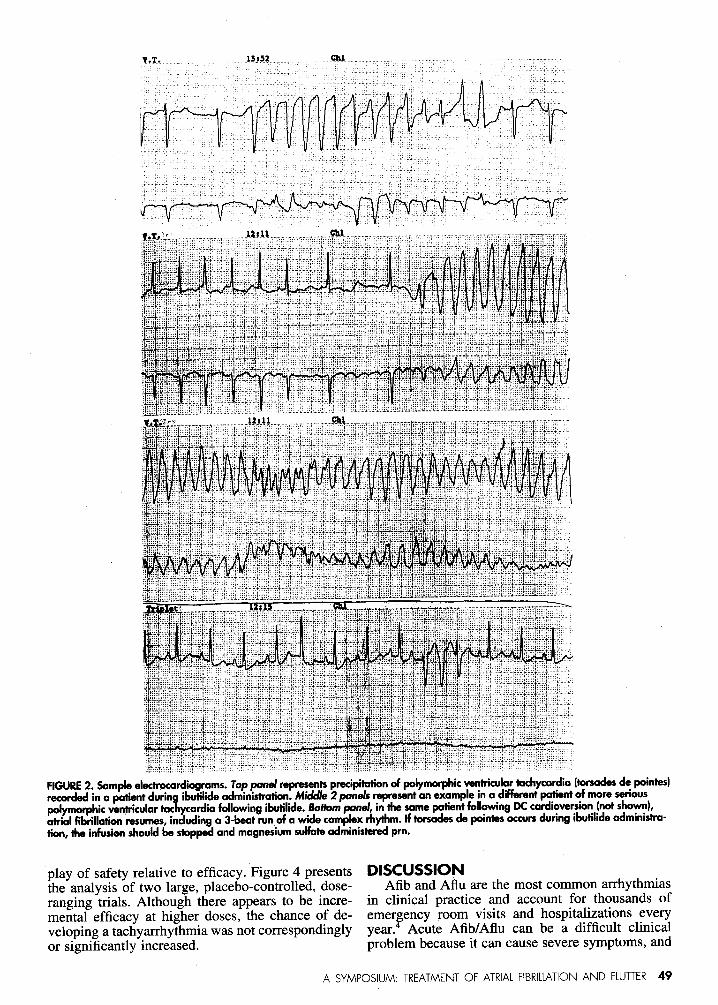
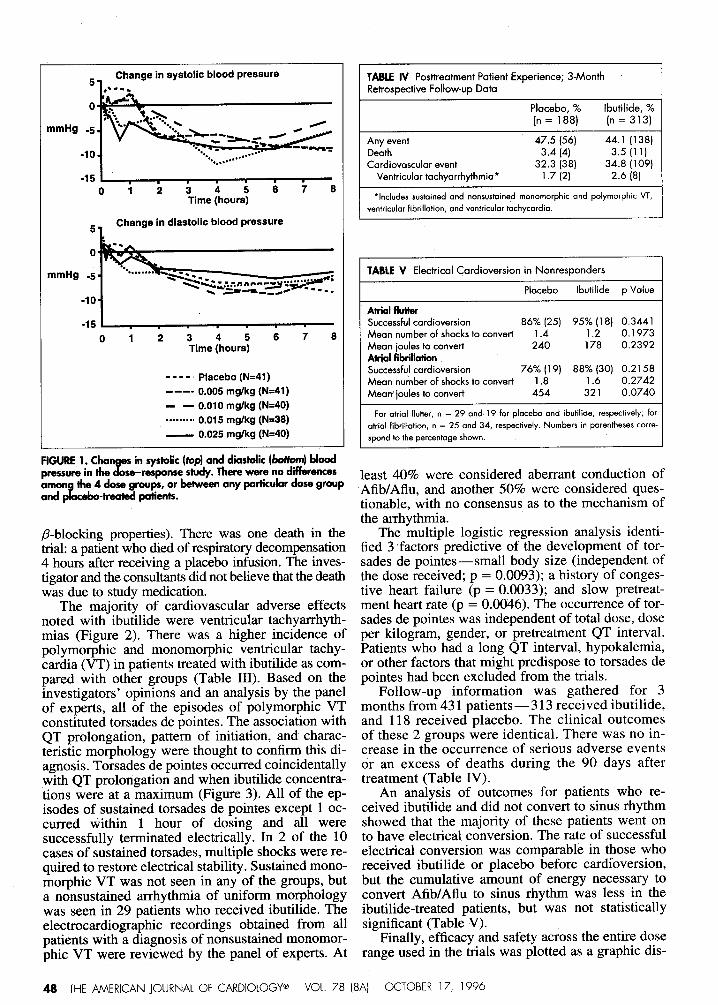
FIGURE2. Sampleelectrocardiograms.Toppondrepresentsprecipitationofpalymqhicventriculartachycardia(torsadesdepaintes)recordedina patientdurin ibsstilideadminisiraticm.Mic/dhs2 panelsrepresentanexampleina differentpatientofmoreserious
[email protected],inthesamepatientfollow”ngDCcardioversion(notshown),atrialfibriHationresumes,includinga 3-beatrunofawidecomplexrhythm.Iftorsadesdepainiesoccursduringibutilideadministra-tion,theinfusienshouldbestoppedandrrsagnedumsulfateadministeredpm.
play of safety relative to efficacy. Figure 4 presents DISCUSSIONthe analysis of two large, placebo-controlled, dose- Afib and Aflu are the most common arrhythmiasranging trials. Although there appears to be incre- in clinical practice and account for thousands ofmental efficacy at higher doses, the chance of de- emer~ency room visits and hospitalizations everyveloping a tachyarrhythrnia was not correspondingly year. Acute Afib/Aflu can be a difficult clinicalor significantly increased. problem because it can cause severe symptoms, and
A SYMPOSIUM: TREATMENT OF ATRIA1 FIBRILLATION AND FLUTTER 49
I 20,
1
I Mean*SD I.. s-..
Ibutilideconcentration(ng/mL)
(Elderlyhealthyvolunteera)
QTc interval(msec)
(Elderlyhealthyvolunteer),
Numberof patientsandtimeof PVT(Efficacyatudiea) iL25)
01 2 34Time after dosing (hours)
FIGURE3.Coincidenceinlimebetweenoccurrenceofpaiymqhk VTinIheefficacydrrdies(be- panel),peakibutilidepfasmrsconcentrationdefhedinelderlyhealthyvolunteers(ng/mq(tappanel),andQT.intervalchange(msec)dehad inalderiyheahhyvolunteers(middk pond). Sustainedpolymorphicventriculartcschycardia(PVT)eventsareindicatedbyiheopenbarsandnonsustainedbytheclosedbars.
,nc,dence%Atrial flutter70
!! E10 ---9-*.*wm.9 9.9....
0Low Mid High
Ibutilide dose range
Atria! fibrillationIncidance%7060 “50 “
: !/’
oLow Mid High
Ibutilide dose range
— Conversion--o All PVT¤~”=-~SPVT
FIGURE4. Incidenceof~$-wJ’*~’TdandSuSkrimcJF=h-P@Js VT(m -’=f-Jdihifide’sekrcy in#srmmah“ngCdrialflu&r(
%!anddicl#XJa-
tiarr(6a&xIslacmesthe3 dosemngesusedin “ “ .
methods to terminate these arrhythmias are not easilyapplied. There is increasing evidence that Afib/Afl;may perpetuate itself either by geometric or electri-cal remodeling in which electrophysiologic derange-ments become more severe the longer the arrhythmiais present.5
The literature concerning the acute administra-tion of antiarrhythmic drugs for termination ofAfib/Aflu is scant, and that which is available ishighly anecdotal and, in many cases, without a pla-cebo controlG—a particular problem, given the rel-atively high chances of spontaneous conversion tosinus rhythm. Ibutilide is the first drug to be ap-proved by the Food and Drug Administration forthe acute termination of Afib/Aflu. Drugs that areroutinely used for the acute treatment of Afib/Afluslow the ventricular response rate, but have con-verted Afib/Aflu to sinus rhythm no betjer than pla-cebo in the trials in which they have been carefullystudied.7’8Electrical conversion is frequently used,especially in patients who are hemodynamicallyunstable. This requires general anesthesia, whichmay not be available or feasible in all circum-stances. Electrical conversion carries some risksof its own, which may be related to the use ofgeneral anesthesia in individuals who are alreadyhemodynamically compromised, to postshockphenoihena (such as heart block or sinus arrest),or to skin burns. In addition, when cardioversionis applied in the absence of antecedent drugtherapy, there is a substantial chance of rhythmreversion, in part because of the sympatheticdischarge that may be an accompaniment of elec-trical conversion.9’10
Studies with ibutilide represent the first attemptto describe systematically the efficacy of a pharrna-
50 THE /-WERICAN JOURNAL OF CARDIOLOGY@ VOL 78 (8A] OCTOBER 17, 1996
Cumulativenumbarofpatients(%)5 . I
I!
4 - j Firstacxwrence~sustaln6dI OrnO~us~~ P~(N=z5)I
3 - I
II
2 - I
I Flrstoccurrence of1 - : sustainedPVT(N.1O)
I
o 1, 2 3 22 23 24lime afterstartof infusion(hours)
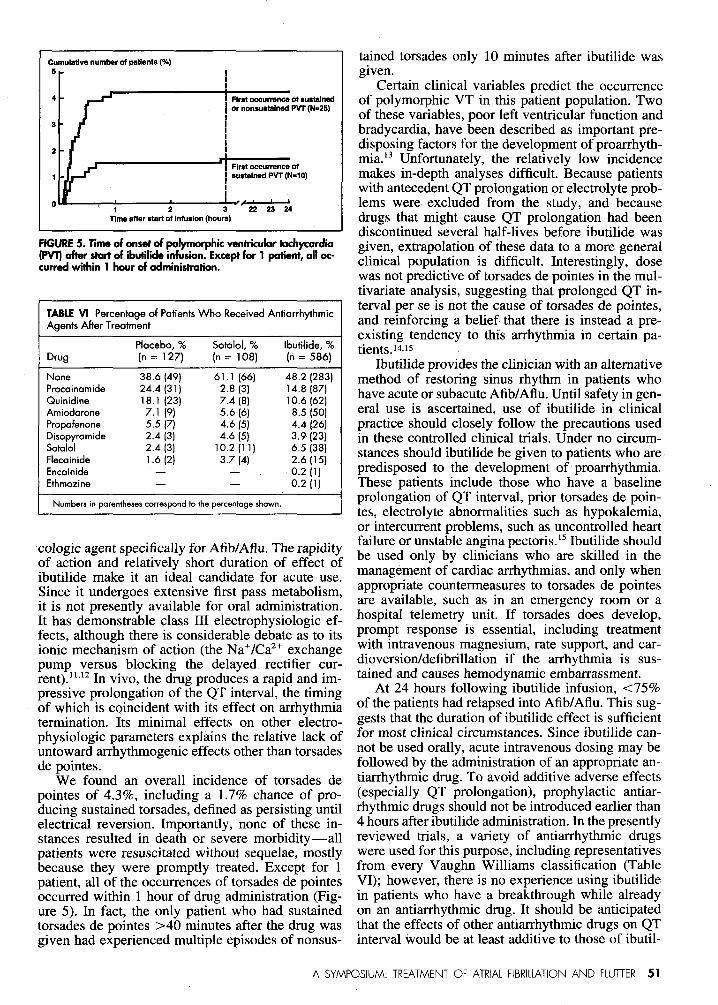
FfGURE5. Timeofonsetofpolymorphicventriculartachycardia(~ af$erstartof ibutilideinfusion.Exceptfar1patient,alloc-curredwithin1hwr ofadministration.
TABLEVI Percentage of PotientsWho Received AntiorrhythmicAgents After Treotment
Plocebo, % Sotolol, % Ibutilide, %Drug (n= 127) [n = 108) (n= 586)
None 38.6 (49) 61.1 (66] 48.2 (283)Procoinamide 24.4 (31) 2.8 (3) 14,8 (87)Quinidine 18.1 (23) 7.4 (8) 10.6 (62)Amiodorone 7.1 (9) 5.6 (6) 8.5 (50]Propofenone 5.5 (7) 4.6 [5) 4.4 [26]Disopyramide 2.4 [3] 4.6 (5) 3.9 (23)Sotalol 2.4 [3] 10.2 (11) 6.5 (38)Flecainide 1.6 (2) 3.7 (4) 2.6 (15)Encainide — — 0.2 (1)Ethmazine . — 0.2 [1)
Numbers in parentheses correspond to the percentage shown.
cologic agent specifically for Afib/Aflu. The rapidityof a~tion-and ~elatively-short duration of eff~ct ofibutilide make it an ideal candidate for acute use.Since it undergoes extensive first pass metabolism,it is not presently available for oral administration.It has demonstrable class III electrophysiologic ef-fects, although there is considerable debate as to itsionic mechanism of action (the Na+/Ca2+exchangepump versus blocking the delayed rectifier cur-rent).11’12In vivo, the drug produces a rapid and im-pressive prolongation of the QT interval, the timingof which is coincident with its effect on arrhythmiatermination. Its minimal effects on other electro-physiologic parameters explains the relative lack ofuntoward arrhythmogenic effects other than torsadesde pointes.
We found an overall incidence of torsades depointes of 4.3%, including a 1.7% chance of pro-ducing sustained torsades, defined as persisting untilelectrical reversion. Importantly, none of these in-stances resulted in death or severe morbidity—allpatients were resuscitated without sequelae, mostlybecause they were promptly treated. Except for 1patient, all of the occurrences of torsades de pointesoccurred within 1 hour of drug administration (Fig-ure 5). In fact, the only patient who had sustainedtorsades de pointes >40 minutes after the drug wasgiven had experienced multiple episodes of nonsus-
tained torsades only 10 minutes after ibutilide wasgiven.
Certain clinical variables predict the occurrenceof polymorphic VT in this patient population. Twoof these variables, poor left ventricular function andbradycardia, have been described as important pre-disposing factors for the development of proarrhyth-mia.13 Unfortunately, the relatively low incidencemakes in-depth analyses difficult. Because patientswith antecedent QT prolongation or electrolyte prob-lems were excluded from the study, and becausedrugs that might cause QT prolongation had beendiscontinued several half-lives before ibutilide wasgiven, extrapolation of these data to a more generalclinical population is difficult. Interestingly, dosewas not predictive of torsades de pointes in the mul-tivariate analysis, suggesting that prolonged QT in-terval per se is not the cause of torsades de pointes,and reinforcing a belief that there is instead a pre-existing tendency to this arrhythmia in certain pa-tients.14ils
Ibutilide provides the clinician with an alternativemethod of restoring sinus rhythm in patients whohave acute or subacute Afib/Aflu.Until safety in gen-eral use is ascertained, use of ibutilide in clinicalpractice should closely follow the precautions usedin these controlled clinical trials. Under no circum-stances should ibutilide be given to patients who arepredisposed to the development of proarrhythmia.These patients include those who have a baselineprolongation of QT interval, prior torsades de poin-tes, electrolyte abnormalities such as hypokalemia,or intercurrent problems, such as uncontrolled heartfailure or unstable angina pectoris.15Ibutilide shouldbe used only by clinicians who are skilled in themanagement of cardiac arrhythmias, and only whenappropriate countermeasures to torsades de pointesare available, such as in an emergency room or ahospital telemetry unit. If torsades does develop,prompt response is essential, including treatmentwith intravenous magnesium, rate support, and car-dioversion/defibrillation if the arrhythmia is sus-tained and causes hemodynamic embarrassment.
At 24 hours following ibutilide infusion, <7590of the patients had relapsed into Afib/Aflu. This sug-gests that the duration of ibutilide effect is sufficientfor most clinical circumstances. Since ibutilide can-not be used orally, acute intravenous dosing may befollowed by the administration of an appropriate an-tiarrhythmic drug. To avoid additive adverse effects(especially QT prolongation), prophylactic antiar-rhythmic drugs should not be introduced earlier than4 hours after ibutilide administration. In the presentlyreviewed trials, a variety of antiarrhythmic drugswere used for this purpose, including representativesfrom every Vaughn Williams classification (TableVI); however, there is no experience using ibutilidein patients who have a breakthrough while alreadyon an antiarrhythmic drug. It should be anticipatedthat the effects of other antiarrhythmic drugs on QTinterval would be at least additive to those of ibutil-
A SYMPOSIUM: TREATMENT OF ATRIAL FIBRILLATION AND FLUTTER 51

ide, if not synergistic. A postmarketing evaluation ofthis indication is necessary.
CONCLUSIONSThe safety of ibutilide has been well described in
these clinical trials. Its principal toxicity is proar-rhythmia, specifically, provocation of torsades depointes in 4–590 of patients. The nature of the proar-rhythmia, the circumstances of its occurrence, andthe risk factors for its development have been delin-eated, as have methods for its prompt and propertreatment. As long as patients are selected appropri-ately, and appropriate precautions “aretaken duringadministration, we anticipate that ibutilide will bewell accepted by physicians accustomed to manage-ment of acute arrhythmia. The benefit to the patientof avoiding electrical conversion or prolonged epi-sodes of Afib/Aflu, with attendant morbidity, out-weighs the small proarrhythmic risk and makes ibu-tilide a useful new antiarrhythmic drug.
AcknowledgmentDr. Kowey is an ad hoc con-sultant for the Pharrnacia & Upjohn Inc. His depart-ment was the recipient of grants for clinical researchfrom which Dr. Kowey derived no salary support.
The authors wish to thank the investigators fortheir hard work in recruiting and following-up pa-tients in the clinical trials, and Rose Marie Wells forher usual competent help in the preparation of themanuscript.
1. Ellenbogan KA, Starnbler BS, Wood MA, Sager FT, Wesley RC, MeissnerMD, Zoble RG, Waketield LK, Perry XT, Vanderlugt JT, for the Rmtilide In-
vestigators. Efficacy of intravenous ibutilide for acute termination of atrial fib-rillation and atrial ‘flutter: a dose response study. J Am Co/l Cardiol1996;28:13W136.2. DiMarco J. Cardioversion of atrial flutter by intravenous ibutilide, a newclass III arrtiarrhythrnic agent. (Abstr.) J Am Coil Cardiol 1991;17:324A.3. Buchanan LV, Kabell G, Bnrnden MN, Gibson JK. Comparative assessmentof ibutilide, d-sotalol, clofilium, E-4031, and UK-68,798 in a rabbit model ofproarrhytfrmia. J Car-diovascPhrrrrmrcol 1993;220:540–549.4. Pritchett ELC. Management of atrial fibrillation. N Engl J Med1992;326:1264–1271.5. Wijffels MCEF, Kirchof CJHJ, Dorlarrd R, Allessie MA. Atritd fibrillationbegets atrial fibrillation. A study in awake chronically instrumented goats. Cir-culation 1995;92:1954–1968.6. Ferrster PE, Comess KA, Marsh R, Katzenberg C, Hager WD. Conversionof atrial fibrillation to sinus rhytbrn by acute intravenous procairrarnide infusion.Am Heart J 1983;106:501-504.7. Anderson S, Blarrski L, Byrd RC, Das G, Engler R, Laddu A, Lee R, RajferS, Scfrmeder J, Steck JD, Sung R, Turlapaty P, Williams D, Wilrrer G, ZobleR. Comparison of the efficacy and safety ofesmolol, a short-acting beta-blacker,with placebo in the treatnrerrt of supraverrtricular tachyarrhytbmias. Am HeartJ 1986;111:43–48.8. Falk RH, Knowlton AA, Bemart SA, Gottlieb NE, Battinelli NJ. Digoxin forconverting recent-onset atriaf fibrillation to sinus rhythm: a rarrdonrized,double-blinded trial. Arm Intern Med 1987;106:503–506.9. VanGeldcr IC, Ctijns W, VanGilst WH, Verwcr R, Lie KL Prediction of urre-verrt6dcardioversionand maintenanceof sinus drytbrnfmm direct-currentelccticalcardioversiorrof chronicahial fibrillationand flutmr.Am JCar&rl 1991;68:41-46.10.D&elf GW, AndersnrrJ, Adgey AA. Factors determhing success and energyrequirementsfor cardiovemionof amid fibrillation.Q JMed 1990;76:W3-913.11.Wesley RC, Farkharri F, Morgan D, Zimmerman D. Ibutilide: enhanceddefibrillation via plateau sodium current activation. Am J Physiol1993;264:H1269-H1274.12..Yang T, Snyders DJ, Roden l’)M. Ibutilide is a potent blocker of IK,,in cultured atrial tumor myocytes (AT-1 Cells). (Abstr.) JJiophys J 1994;66:A67.13. Podrid PJ, Lanbert S, Graboys TB, Blatt CM, Lown B. Aggravation ofarrbythrnia by antiarrhythrnic drags-incidence and predictors. Am J Cardiol1987;59(suPP1):38E–44E.14. Kurita T, Ohe T, Mami N, Aihara N, T&aki H, Kamakura S, MatsuhisaM, Shirnomura K. Bradycmlia induced abnormal QT prolongation in patientswith complete atrio-ventricukir block with torsades de pointes. Am J Canfiol1992;69:628-633.15. Priori SG, Diehl L, Schwartz PJ. Torsades de pointes. In: Podrid PJ, KoweyPR, eds. Cardiac Arrhythmia: Mechanism, Diagnosis and Management. Baf-timore: Williams and Wilkins; 1995:951-963.
52 THE AMERICAN JOURNAL OF CARDIO1OGY” VOL 78 (8A) OCTOBER 17, 1996













![Dysrhythmias (002) [Read-Only] - Aventri · Atrial AV node Ventricular Classification of Rhythm Abnormalities Supraventricular Atrial origin Atrial fibrillation Atrial flutter Atrial](https://img.dokumen.tips/doc/110x75/5f024baa7e708231d4038f22/dysrhythmias-002-read-only-aventri-atrial-av-node-ventricular-classification.jpg)















