Embed Size (px)
Citation preview
Safety and Efficacy of Liraglutidein Patients With Type 2 Diabetesand End-Stage Renal Disease:An Investigator-Initiated,Placebo-Controlled,Double-Blinded, Parallel Group,Randomized TrialDOI: 10.2337/dc15-1025
OBJECTIVE
To evaluate parameters related to safety and efficacy of liraglutide in patientswith type 2 diabetes and dialysis-dependent end-stage renal disease (ESRD).
RESEARCH DESIGN AND METHODS
Twenty-four patients with type 2 diabetes and ESRD and 23 control subjects withtype 2 diabetes and normal kidney function were randomly allocated to 12 weeksof double-blinded liraglutide (titrated to a maximum dose of 1.8 mg) or placebotreatment (1:1) injected subcutaneously once daily as add on to ongoing antidi-abetic treatment. Dose-corrected plasma trough liraglutide concentration wasevaluated at the final trial visit as the primary outcome measure using a linearmixed model.
RESULTS
Twenty patients with ESRD (1:1 for liraglutide vs. placebo) and 20 control subjects(1:1) completed the study period. Dose-corrected plasma trough liraglutide con-centration at the final visit was increased by 49% (95% CI 6–109, P = 0.02) in thegroup with ESRD compared with the control group. Initial and temporary nauseaand vomiting occurred more frequently among liraglutide-treated patients withESRD compared with control subjects (P < 0.04). Glycemic control tended toimprove during the study period in both liraglutide-treated groups as assessedby daily blood glucose measurements (P < 0.01), and dose of baseline insulin wasreduced in parallel (P < 0.04). Body weight was reduced in both liraglutide-treatedgroups (22.46 0.8 kg [mean6 SE] in the groupwith ESRD, P = 0.22;22.96 1.0 kgin the control group, P = 0.03).
CONCLUSIONS
Plasma liraglutide concentrations increased during treatment in patients withtype 2 diabetes and ESRD, who experienced more gastrointestinal side effects.Reduced treatment doses and prolonged titration period may be advisable.
1Department of Nephrology, Rigshospitalet, Uni-versity of Copenhagen, Copenhagen, Denmark2Center for Diabetes Research, Gentofte Hospital,University of Copenhagen, Hellerup, Denmark3The Novo Nordisk Foundation Center for BasicMetabolic ResearchandDepartment of BiomedicalSciences, Faculty of Health and Medical Sciences,University of Copenhagen, Copenhagen, Denmark4Department of Endocrinology, Rigshospitalet,University of Copenhagen, Copenhagen, Denmark5Department of Internal Medicine, Hillerød Hospi-tal, University of Copenhagen, Hillerød, Denmark6Section of Biostatistics, Department of PublicHealth, University of Copenhagen, Copenhagen,Denmark
Corresponding author: Thomas Idorn, [email protected].
Received 19 May 2015 and accepted 16 July2015.
Clinical trial reg. no. NCT01394341, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-1025/-/DC1.
© 2015 by the American Diabetes Association.Readersmayuse this article as longas thework isproperly cited, the use is educational and not forprofit, and the work is not altered.
See accompanying article, p. XXX.
Thomas Idorn,1 Filip K. Knop,2,3
Morten B. Jørgensen,1 Tonny Jensen,4
Marsela Resuli,5 Pernille M. Hansen,5
Karl B. Christensen,6 Jens J. Holst,3
Mads Hornum,1 and Bo Feldt-Rasmussen1
Diabetes Care 1
CLIN
CARE/ED
UCATIO
N/N
UTR
ITION/PSYC
HOSO
CIAL
Diabetes Care Publish Ahead of Print, published online August 17, 2015

Diabetic nephropathy is the most com-mon cause of dialysis-dependent end-stage renal disease (ESRD). Forty-fivepercent of U.S. patients with ESRDhave diabetes compared with 23% ofpatients in Denmark (1,2). Several anti-diabetic drugs are cleared renally. Ac-cordingly, only a limited number ofantidiabetic treatment options existfor this group of patients. Currently, in-sulin is the cornerstone of treatment;however, dose reduction may be re-quired due to reduced renal clearanceof circulating insulin (3–5). Hence, therisk of hypoglycemia is high, and un-awareness, often associated with auton-omous neuropathy, frequently furtherimpedes insulin treatment in patientswith ESRD and diabetes (6). The oralantihyperglycemic agents biguanides,a-glucosidase inhibitors, and sodium-glucose cotransporter 2 inhibitors arenot usable in patients with ESRD andtype 2 diabetes (4,5). Some second-generation sulphonylureas and megliti-nides can be used with caution, andthiazolidinediones may be used to treatpatients with ESRD and diabetes withoutcardiac disease (4,5). The dipeptidyl pep-tidase 4 (DPP-4) inhibitors have ex-panded the limited armamentarium;linagliptin can be administered to pa-tients with ESRD without dose reduction(7), and saxagliptin, vildagliptin, and sita-gliptin can be used in reduced doses(8–12). The efficacy of DPP-4 inhibitorsis, however, often inadequate. Glucagon-like peptide-1 (GLP-1) receptor agonistspossess a potent antihyperglycemiceffect with a low risk of hypoglycemia.Nevertheless, these agents have beenless thoroughly investigated and are cur-rently not recommended for patientswith ESRD due to lack of data (13–18).The primary objectives of the currentstudy were to evaluate plasma liraglu-tide concentrations and adverse events(AEs) during treatment in patients withtype 2 diabetes and ESRD. We hypothe-sized that patients with type 2 diabetesand ESRD tolerate treatment with lira-glutide in doses that accord with therecommendations of the EuropeanMedicines Agency (13), without causingsignificant accumulation in plasma.
RESEARCH DESIGN AND METHODS
The protocol has been published previ-ously (19) and a summary is providedbelow.
Trial Design and RegistrationThe studywas conductedas an investigator-initiated, multicenter (three sites), placebo-controlled, double-blinded, parallel group,randomized trial in Denmark. Two groupswere investigated: 1) patients with type 2diabetes and ESRD and 2) patients withtype 2 diabetes and normal kidney func-tion (control group). Participants in bothgroups were randomized to liraglutide orplacebo (1:1). The intervention periodwas 12 weeks and inclusion was contin-ued until 20 participants in each grouphad completed a minimum of 6 weeksof treatment. The Danish MedicinesAgency (EudraCT number 2010-021922-36), the Scientific Ethics Committee ofthe Capital Region of Denmark (H-3-2011-032), and the Danish Data Protec-tion Agency (2007-58-0015) approvedthe study, which was registered atclinicaltrials.gov (NCT01394341) priorto study start. The study was carriedout in compliance with the InternationalConference on Harmonization and goodclinical practice (GCP) guidelines underthe surveillance of the GCP unit at Copen-hagen University Hospital. The study wasconducted in accordance with the latestrevision of the Helsinki Declaration.
Participants and Study SettingsPatients with ESRD were recruitedamong chronic dialysis patients at theDepartments of Nephrology at Rigsho-spitalet and Hillerød Hospital, Denmark,from September 2011 to October 2013.Control subjects were recruited fromthe outpatient clinic at the Departmentof Endocrinology, Rigshospitalet. Eligibilitycriteria for participants in the dialysisgroup were men and women aged 18–85years, chronic hemodialysis or peritonealdialysis treatment, type 2 diabetes diag-nosed at least 3 months prior to screen-ing, and preserved b-cell functionas evaluated by a glucagon test. Inclu-sion criteria in the control group weremen and women aged 18–85 years, nor-mal kidney function (plasma creatinine,105 mmol/L for men and ,90 mmol/Lfor women), type 2 diabetes diagnosed atleast 3 months prior to screening, glycatedhemoglobin (HbA1c).6.5%(.48mmol/mol),and preserved b-cell function.
Experimental DesignParticipants in both groups followed thesame study plan. On an initial screeningday, a 6-min glucagon test was performedfor documentation of preserved b-cell
function. After screening, all included par-ticipants attended nine planned visits: ran-domization (week 0), week 1, week 2,week 4, week 6, week 8, week 10, week12, and follow-up (week 13). At each visit,blood sampling was performed, AEs werereported, glycemic control was assessed,trial medication was dispensed, usedpackages were collected to estimate com-pliance, and doses of antidiabetic drugs,including trial medication, were adjusted.Blood glucosewasmeasured (using a Con-tour glucose meter; Bayer HealthCare,Copenhagen, Denmark) three times daily(fasting in themorning, before dinner, andbefore bedtime) throughout the studyperiod. Participants did not inject trialmedication in the morning prior to thetrial visits, and time since last dose wasregistered at each trial visit. Participantsattended in a fasting state (8 h overnight)for the randomization, week 6, and week12 visits.
InterventionTrial medication was initiated on the dayof randomization in a dosage of 0.6mg s.c.once daily. All participants were requestedto inject the medicine in the abdomen be-forebreakfast.Dependingonglycemic con-trol and side effects, dose was escalatedby up to 0.6 mg per week to a maximumof 1.8 mg. Doses of baseline antidiabeticmedication were individually adjusted inparallel with trial medication according toprespecified treatment goals. To minimizethe risk of hypoglycemia, basal insulin dosewas reduced by 20–50% at randomizationand sulphonylureas were paused, whilemetformin was continued in unchangeddoses.
OutcomesThe primary end point was the dose-corrected trough concentration of liraglu-tide in plasma at the final trial visit (week12). Secondary end points included severeAEs (SAEs), AEs, glycemic control, changein baseline insulin dose, body weight, hy-poglycemic episodes (divided into minor[blood glucose,3.1 mmol/L and no needfor assistance] and major [blood glucose,3.1 mmol/L and requiring assistancefrom third person]), and cardiovascularparameters (heart rate, blood pressure,lipid profile, and prohormone brain natri-uretic peptide [proBNP] concentration inplasma).
Sample SizeThe power calculation was based on theprimary end point. On the basis of previous
2 Liraglutide for Dialysis Patients With Diabetes Diabetes Care

trials with liraglutide, the trough valuewas estimated to be 20,000 pmol/Lduring steady state and the SD was esti-mated to be 8,000 pmol/L in people withnormal kidney function (20,21). Ten com-pleters in each liraglutide treatment armand a significance level of 5% (a = 0.05)would enable us to detect a difference of10,600 pmol/L with a power of 80% (12b = 0.80) using a two-sample Studentt test. Further statistical power was ob-tained by analyzing data from all visitsusing a linear mixed model.
Randomization and BlindingPatients and control subjects were as-signed to receive either liraglutide or pla-cebo according to a computer-generatedrandomization list provided by NovoNordisk A/S (Bagsværd, Denmark). Sim-ple randomization was used consecutivelyin both groups, and an unblinded, impartialperson from Rigshospitalet, was informedin the case of withdrawals or exclusions inorder toensure10 completers in each treat-ment arm. Participants, investigators, andhealthcare staff were blinded for the allo-cated treatment and remained so until lastpatient last visit.
Analyses and Statistical MethodsThe primary end point was reportedbased on a modified per-protocol (PP)analysis, i.e., restricted to participantswho completed a minimum of 6 weeksof interventionwith a compliance.80%of the prescribed trial medication. If thefull intervention period was not com-pleted, the last observation carried for-ward method was applied. Secondaryend points related to efficacy werereported based on data from the PPpopulation, and data related to safetywere reported based on intention-to-treat analyses. We used a linear mixedmodel to address our primary end point.Group, trial visit day, and treatmentdose since last trial visit were used asexplanatory variables, and a modelwith interaction between group and tri-al visit day was applied to model twodifferent trajectories: differences indose-corrected liraglutide concentra-tions between groups and changes indose-corrected liraglutide concentra-tions within groups during the studyperiod. The primary end point wascalculated as the difference in esti-mated, dose-corrected plasma troughliraglutide concentrations between thetwo liraglutide-treated groups at the
final trial visit (week 12). Plasma liraglu-tide concentrations were measuredby a validated liraglutide-specific ELISAmethod at Huntingdon Life Sciences Ltd.(Alconbury, U.K.) as previously de-scribed (22). Distribution of data andhomogeneity of variance were assessedusing graphical evaluation of residualsfrom the linear mixed model. The em-pirical distribution of the liraglutide con-centrations was well approximated by alog-normal distribution, and, hence, lir-aglutide concentrations and treatmentdoses were log transformed prior toanalysis. Otherwise, normally distrib-uted data were evaluated using para-metric testing, and for data that didnot follow a normal distribution or ex-hibited unequal variance, nonparametrictesting was applied. For group compari-sons of categorical data, we used x2 orFisher exact tests, and continuous datawere analyzed with a one-way ANOVAusing Tukey honestly significant differ-ence test as post hoc test. A Poisson re-gression analysis was used for evaluationof AEs, and the placebo-treated controlgroup was used as references. Blood glu-cosemeasurementswere analyzed using alinear mixed effects model, taking the var-iation between participants and the serialcorrelation into account. All tests weretwo tailed, and a P value ,0.05 was con-sidered significant.
RESULTS
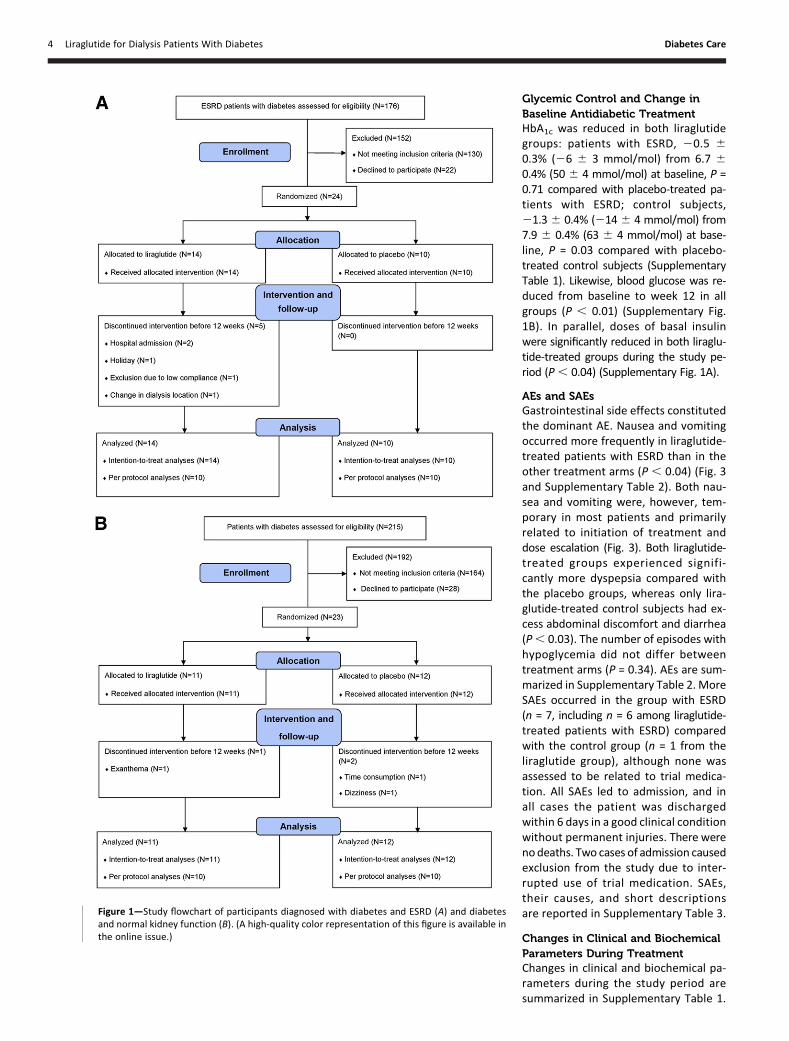
Demographical and Baseline ClinicalDataEligibility was assessed in 176 patientswith ESRD and 215 control subjects; 24patients with ESRD were randomized(14 to liraglutide treatment and 10 toplacebo treatment) and 23 control sub-jects were randomized (11 to liraglutidetreatment and 12 to placebo treat-ment). In both groups, potential studyparticipants were screened based oncomputer-generated lists of patientsregistered with diabetes, without fur-ther specification. Thus, the group ofpatients assessed for eligibility also in-cluded patients with type 1 diabetes. Inthe group with ESRD, the main reasonsfor noneligibility and refusing to partic-ipate were type 1 diabetes, cardiac dis-ease, and time consumption, and in thecontrol group, the main reasons weretype 1 diabetes, ongoing treatment withan incretin-based agent, renal insuffi-ciency, and time consumption. Twenty
participants in each group (10 treatedwith liraglutide and placebo, respectively)completed the study period, with the ex-ception of one patient with ESRD (liraglu-tide group) who dropped out after 8weeks of treatment due to the summerholidays. Figure 1A and B shows studyflowcharts. Groups were matched accord-ing to age, sex, and BMI. Ethnicity, smok-ing, and diabetes historywere comparablebetween groups. The majority of patientswith ESRD and control subjectswere treat-ed with insulin (75 and 70%, respectively;PP population); none of the patients withESRD received metformin compared with80% in the control group. Two patientswith ESRD and one control subject weretreated with sulphonylureas at baseline.The majority of patients with ESRD re-ceived standard medical care for dialysispatients, including erythropoietin, ironsubstitution, vitamins B, C, and D, andphosphate binders. Demographical andbaseline clinical and biochemical data aresummarized in Table 1.
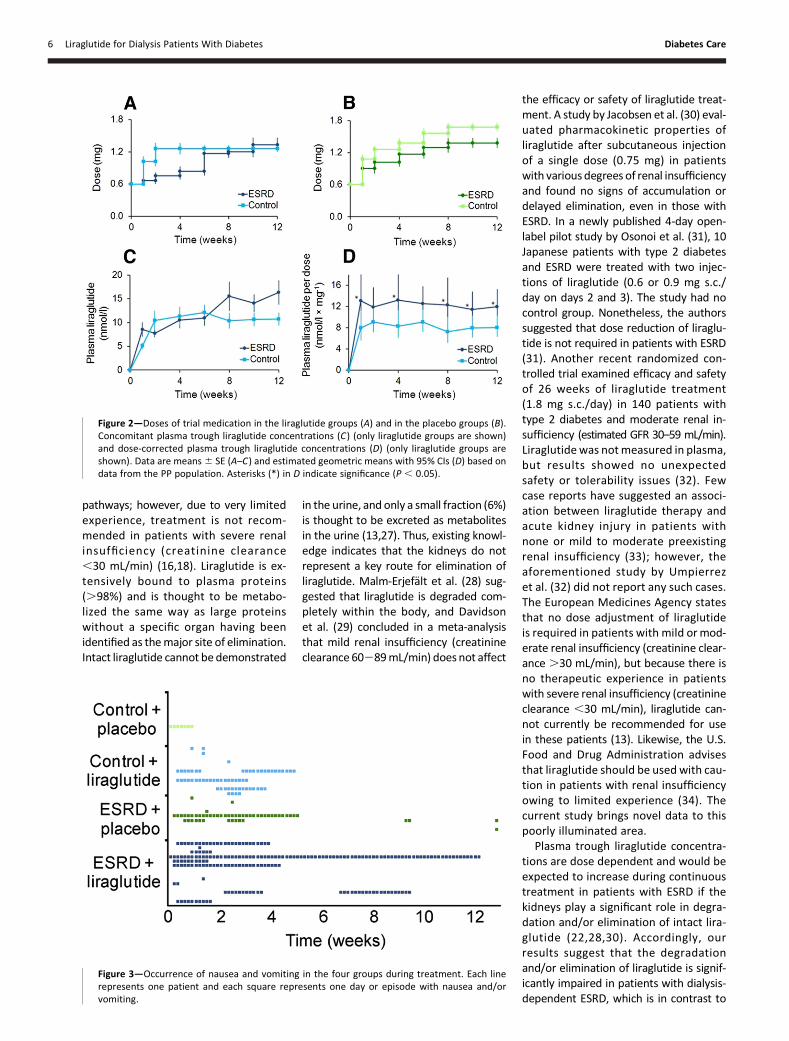
Liraglutide Doses and PlasmaConcentrationsLiraglutide-treated patients with ESRDwere titrated more slowly than liraglu-tide-treated control subjects but endedat comparable doses after 12 weeks(1.33 6 0.13 and 1.26 6 0.06 mg/day,P = 0.61) (Fig. 2A). The dose-correctedplasma trough liraglutide concentrationat the final visit was increased by 49%(95% CI 6–109, P = 0.02) in liraglutide-treated patients with ESRD comparedwith liraglutide-treated control subjects(Fig. 2D). Estimated geometric means ofplasma liraglutide concentrations were11,980 (95% CI 9,379–15,290) and 8,057(6,306–10,290) pmol/L3mg21, respec-tively, at week 12 (Fig. 2D). The dose-corrected plasma trough liraglutideconcentration was increased in the liraglu-tide-treated group with ESRD throughoutthe intervention period compared withthe liraglutide-treated control group. Theincrease ranged from30.4% (29.4 to 87.6)to 70.4% (5.4 to 175.3) at individual trialvisits, and there were no signs of progres-sive accumulation of liraglutide in thegroup with ESRD as evaluated from theslope of the dose-corrected liraglutideconcentration curve, which was similar tothat of the control group (P = 0.78) (Fig.2D). Compliance was high in all four treat-ment arms at all visits (.94.8%), with nodifferences between groups (P = 0.95).
care.diabetesjournals.org Idorn and Associates 3
Glycemic Control and Change inBaseline Antidiabetic TreatmentHbA1c was reduced in both liraglutidegroups: patients with ESRD, 20.5 60.3% (26 6 3 mmol/mol) from 6.7 60.4% (50 6 4 mmol/mol) at baseline, P =0.71 compared with placebo-treated pa-tients with ESRD; control subjects,21.36 0.4% (214 6 4 mmol/mol) from7.9 6 0.4% (63 6 4 mmol/mol) at base-line, P = 0.03 compared with placebo-treated control subjects (SupplementaryTable 1). Likewise, blood glucose was re-duced from baseline to week 12 in allgroups (P , 0.01) (Supplementary Fig.1B). In parallel, doses of basal insulinwere significantly reduced in both liraglu-tide-treated groups during the study pe-riod (P, 0.04) (Supplementary Fig. 1A).
AEs and SAEsGastrointestinal side effects constitutedthe dominant AE. Nausea and vomitingoccurred more frequently in liraglutide-treated patients with ESRD than in theother treatment arms (P , 0.04) (Fig. 3and Supplementary Table 2). Both nau-sea and vomiting were, however, tem-porary in most patients and primarilyrelated to initiation of treatment anddose escalation (Fig. 3). Both liraglutide-treated groups experienced signifi-cantly more dyspepsia compared withthe placebo groups, whereas only lira-glutide-treated control subjects had ex-cess abdominal discomfort and diarrhea(P, 0.03). The number of episodes withhypoglycemia did not differ betweentreatment arms (P = 0.34). AEs are sum-marized in Supplementary Table 2. MoreSAEs occurred in the group with ESRD(n = 7, including n = 6 among liraglutide-treated patients with ESRD) comparedwith the control group (n = 1 from theliraglutide group), although none wasassessed to be related to trial medica-tion. All SAEs led to admission, and inall cases the patient was dischargedwithin 6 days in a good clinical conditionwithout permanent injuries. There werenodeaths. Two cases of admission causedexclusion from the study due to inter-rupted use of trial medication. SAEs,their causes, and short descriptionsare reported in Supplementary Table 3.
Changes in Clinical and BiochemicalParameters During TreatmentChanges in clinical and biochemical pa-rameters during the study period aresummarized in Supplementary Table 1.
Figure 1—Study flowchart of participants diagnosed with diabetes and ESRD (A) and diabetesand normal kidney function (B). (A high-quality color representation of this figure is available inthe online issue.)
4 Liraglutide for Dialysis Patients With Diabetes Diabetes Care
Liraglutide treatment caused weightloss in the control group (from 89.5 63.7 to 86.6 6 3.5 kg, P = 0.03), whereasweight was reduced insignificantly inthe group with ESRD (from 91.1 6 4.9to 88.7 6 5.2 kg, P = 0.22). Pulse rateincreased 6.96 2.4 min21 in liraglutide-treated patients with ESRD from 69.962.9 min21 at randomization (P , 0.01when compared with the placebo group)and 5.56 2.3min21 in liraglutide-treatedcontrol subjects from 77.8 6 3.8 min21
at randomization (P = 0.35). Liraglutidetreatment changed neither systolic nordiastolic blood pressure significantly inthe two groups (P. 0.33). The majorityof biochemical markers were not af-fected by liraglutide treatment. ProBNPwas significantly reduced in the groupwith ESRD treated with liraglutide, whichwas not the case in the liraglutide-treatedcontrol group. However, significant re-ductions in total LDL and HDL cholesterolwere observed only in the control group.
None of the clinical and biochemicalchanges observed during interventiondiffered between liraglutide-treated pa-tients with ESRD and liraglutide-treatedcontrol subjects (P . 0.10). Changes inclinical and biochemical parameters aresummarized in Supplementary Table 1.
CONCLUSIONS
In this investigator-initiated, multicen-ter, placebo-controlled, double-blinded,parallel group, randomized trial, wefound that 1) dose-corrected liraglutideconcentration was significantly increasedin patients with type 2 diabetes andESRD throughout 12 weeks of liraglutidetreatment as compared with patientswith type 2 diabetes and normal kidneyfunction, 2) progressive accumulation ofliraglutide did not occur in patients withESRD during treatment, 3) liraglutidetreatment allowed significant reductionin basal insulin doses in insulin-treatedpatients with type 2 diabetes and ESRD
without causing deterioration of glycemiccontrol, and 4) patients with ESRD seemedmoreprone to liraglutide’s gastrointestinalside effects than patients with type 2 di-abetes with normal kidney function.
Few studies have examined safetyand efficacy of GLP-1 receptor agonistsin the setting of renal insufficiency. FiveGLP-1 receptor agonists are approvedby the European Medicines Agency totreat type 2 diabetes: exenatide (twice-daily and once-weekly formulations),lixisenatide, albiglutide, dulaglutide,and liraglutide (13–18). Exenatide andlixisenatide are primarily eliminated byglomerular filtration and subsequentproteolytic degradation in the tubules;therefore, in the currently recommendeddoses, they are unsuitable for patientswith advanced stages of renal insuffi-ciency (11,12,14,15,17,23–26). Albiglu-tide and dulaglutide are thought to bedegraded in vivo by ubiquitous proteolyticenzymes and general protein catabolism
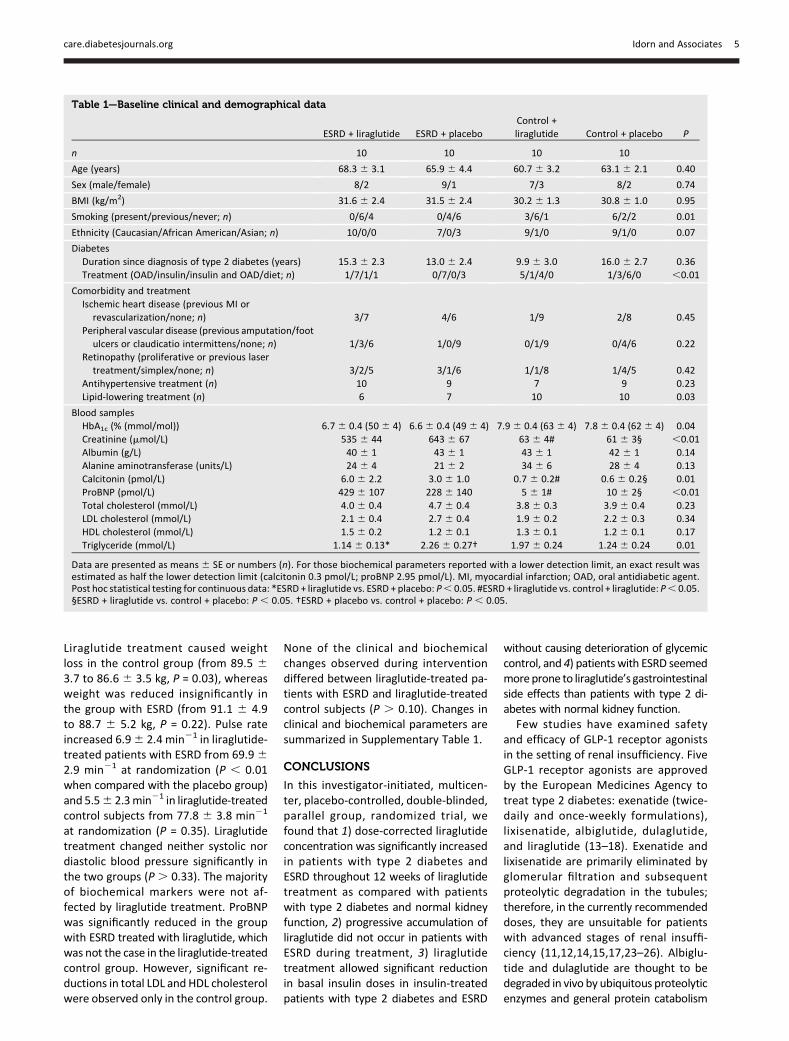
Table 1—Baseline clinical and demographical data
ESRD + liraglutide ESRD + placeboControl +liraglutide Control + placebo P
n 10 10 10 10
Age (years) 68.3 6 3.1 65.9 6 4.4 60.7 6 3.2 63.1 6 2.1 0.40
Sex (male/female) 8/2 9/1 7/3 8/2 0.74
BMI (kg/m2) 31.6 6 2.4 31.5 6 2.4 30.2 6 1.3 30.8 6 1.0 0.95
Smoking (present/previous/never; n) 0/6/4 0/4/6 3/6/1 6/2/2 0.01
Ethnicity (Caucasian/African American/Asian; n) 10/0/0 7/0/3 9/1/0 9/1/0 0.07
DiabetesDuration since diagnosis of type 2 diabetes (years) 15.3 6 2.3 13.0 6 2.4 9.9 6 3.0 16.0 6 2.7 0.36Treatment (OAD/insulin/insulin and OAD/diet; n) 1/7/1/1 0/7/0/3 5/1/4/0 1/3/6/0 ,0.01
Comorbidity and treatmentIschemic heart disease (previous MI or
revascularization/none; n) 3/7 4/6 1/9 2/8 0.45Peripheral vascular disease (previous amputation/foot
ulcers or claudicatio intermittens/none; n) 1/3/6 1/0/9 0/1/9 0/4/6 0.22Retinopathy (proliferative or previous laser
treatment/simplex/none; n) 3/2/5 3/1/6 1/1/8 1/4/5 0.42Antihypertensive treatment (n) 10 9 7 9 0.23Lipid-lowering treatment (n) 6 7 10 10 0.03
Blood samplesHbA1c (% (mmol/mol)) 6.76 0.4 (506 4) 6.66 0.4 (496 4) 7.96 0.4 (636 4) 7.86 0.4 (626 4) 0.04Creatinine (mmol/L) 535 6 44 643 6 67 63 6 4# 61 6 3§ ,0.01Albumin (g/L) 40 6 1 43 6 1 43 6 1 42 6 1 0.14Alanine aminotransferase (units/L) 24 6 4 21 6 2 34 6 6 28 6 4 0.13Calcitonin (pmol/L) 6.0 6 2.2 3.0 6 1.0 0.7 6 0.2# 0.6 6 0.2§ 0.01ProBNP (pmol/L) 429 6 107 228 6 140 5 6 1# 10 6 2§ ,0.01Total cholesterol (mmol/L) 4.0 6 0.4 4.7 6 0.4 3.8 6 0.3 3.9 6 0.4 0.23LDL cholesterol (mmol/L) 2.1 6 0.4 2.7 6 0.4 1.9 6 0.2 2.2 6 0.3 0.34HDL cholesterol (mmol/L) 1.5 6 0.2 1.2 6 0.1 1.3 6 0.1 1.2 6 0.1 0.17Triglyceride (mmol/L) 1.14 6 0.13* 2.26 6 0.27† 1.97 6 0.24 1.24 6 0.24 0.01
Data are presented as means6 SE or numbers (n). For those biochemical parameters reported with a lower detection limit, an exact result wasestimated as half the lower detection limit (calcitonin 0.3 pmol/L; proBNP 2.95 pmol/L). MI, myocardial infarction; OAD, oral antidiabetic agent.Post hoc statistical testing for continuous data: *ESRD + liraglutide vs. ESRD + placebo: P, 0.05. #ESRD + liraglutide vs. control + liraglutide: P, 0.05.§ESRD + liraglutide vs. control + placebo: P , 0.05. †ESRD + placebo vs. control + placebo: P , 0.05.
care.diabetesjournals.org Idorn and Associates 5
pathways; however, due to very limitedexperience, treatment is not recom-mended in patients with severe renalinsufficiency (creatinine clearance,30 mL/min) (16,18). Liraglutide is ex-tensively bound to plasma proteins(.98%) and is thought to be metabo-lized the same way as large proteinswithout a specific organ having beenidentified as themajor site of elimination.Intact liraglutide cannot be demonstrated
in the urine, and only a small fraction (6%)is thought to be excreted as metabolitesin the urine (13,27). Thus, existing knowl-edge indicates that the kidneys do notrepresent a key route for elimination ofliraglutide. Malm-Erjefalt et al. (28) sug-gested that liraglutide is degraded com-pletely within the body, and Davidsonet al. (29) concluded in a meta-analysisthat mild renal insufficiency (creatinineclearance 60289mL/min) does not affect
the efficacy or safety of liraglutide treat-ment. A study by Jacobsen et al. (30) eval-uated pharmacokinetic properties ofliraglutide after subcutaneous injectionof a single dose (0.75 mg) in patientswith various degrees of renal insufficiencyand found no signs of accumulation ordelayed elimination, even in those withESRD. In a newly published 4-day open-label pilot study by Osonoi et al. (31), 10Japanese patients with type 2 diabetesand ESRD were treated with two injec-tions of liraglutide (0.6 or 0.9 mg s.c./day on days 2 and 3). The study had nocontrol group. Nonetheless, the authorssuggested that dose reduction of liraglu-tide is not required in patients with ESRD(31). Another recent randomized con-trolled trial examined efficacy and safetyof 26 weeks of liraglutide treatment(1.8 mg s.c./day) in 140 patients withtype 2 diabetes and moderate renal in-sufficiency (estimated GFR 30–59 mL/min).Liraglutide was notmeasured in plasma,but results showed no unexpectedsafety or tolerability issues (32). Fewcase reports have suggested an associ-ation between liraglutide therapy andacute kidney injury in patients withnone or mild to moderate preexistingrenal insufficiency (33); however, theaforementioned study by Umpierrezet al. (32) did not report any such cases.The European Medicines Agency statesthat no dose adjustment of liraglutideis required in patients with mild ormod-erate renal insufficiency (creatinine clear-ance .30 mL/min), but because there isno therapeutic experience in patientswith severe renal insufficiency (creatinineclearance ,30 mL/min), liraglutide can-not currently be recommended for usein these patients (13). Likewise, the U.S.Food and Drug Administration advisesthat liraglutide should be used with cau-tion in patients with renal insufficiencyowing to limited experience (34). Thecurrent study brings novel data to thispoorly illuminated area.
Plasma trough liraglutide concentra-tions are dose dependent and would beexpected to increase during continuoustreatment in patients with ESRD if thekidneys play a significant role in degra-dation and/or elimination of intact lira-glutide (22,28,30). Accordingly, ourresults suggest that the degradationand/or elimination of liraglutide is signif-icantly impaired in patients with dialysis-dependent ESRD, which is in contrast to
Figure 2—Doses of trial medication in the liraglutide groups (A) and in the placebo groups (B).Concomitant plasma trough liraglutide concentrations (C) (only liraglutide groups are shown)and dose-corrected plasma trough liraglutide concentrations (D) (only liraglutide groups areshown). Data are means6 SE (A–C) and estimated geometric means with 95% CIs (D) based ondata from the PP population. Asterisks (*) in D indicate significance (P , 0.05).
Figure 3—Occurrence of nausea and vomiting in the four groups during treatment. Each linerepresents one patient and each square represents one day or episode with nausea and/orvomiting.
6 Liraglutide for Dialysis Patients With Diabetes Diabetes Care

the aforementioned studies (13,28,30).Nonetheless, we did not observe progres-sive accumulation in the group with ESRDduring treatment (Fig. 2D), indicating thatthe kidneys are not exclusively responsi-ble for elimination and/or degradation ofliraglutide. Our findings suggest thatdoses should be reduced if liraglutidetreatment is considered for those withsevere renal insufficiency. Further studiesare needed to confirm this.Plasma liraglutide concentrations cor-
relate with the frequency and intensityof AEs related to treatment with liraglu-tide (22), and elderly patients and pa-tients with mild renal impairment areknown to be more prone to its gastroin-testinal side effects (13). These factsmight explain the increased incidencesof nausea and vomiting occurring in theliraglutide-treated group with ESRD inour study. Nausea and vomiting weregenerally temporary phenomena re-lated to initiation of treatment anddose escalation, and few patients expe-rienced these side effects in the secondhalf of the treatment period. Therefore,it is likely that dose reduction and slowdose escalation will reduce occurrenceand duration of these side effects.The safety profile was overall good in
the group with ESRD. The SAEs were inexcess in the liraglutide-treated part ofthe group with ESRD; however, nonewas considered related to liraglutidetreatment, and in all cases of admission,the patients were discharged in a goodclinical condition within 6 days withoutpermanent disabilities. Only few casesof hypoglycemia were observed (all mi-nor) despite combination with insulin inseveral patients. We observed an excessnumber of withdrawals and exclusionsin the liraglutide-treated part of thegroup with ESRD (n = 5); however, withthe exception of one patient, who wasexcluded due to low compliance, noneof these was assessed to be caused byliraglutide treatment. Liraglutide-treatedpatients with ESRD and control sub-jects expectedly lost weight duringtreatment with no difference betweengroups (P = 0.39) (35). We observed nocases of severe dehydration, even inthose with the most gastrointestinalside effects, i.e., the weight losses ob-served were not assessed to be due todehydration. We reported two SAEs dueto clotted arteriovenous fistulas; neitherpatient was clinically dehydrated and
both were above their ideal “dry weight”at admission.
A high BMI is associated with lowermortality in patients with ESRD includ-ing the range of obesity ($30 kg/m2),the so-called obesity paradox (36–38).Moreover, weight loss at any BMI isassociated with increased mortalityamong patients receiving maintenancedialysis (39). Even though the aforemen-tioned studies were only observationaland did not specifically examine patientswith ESRD and type 2 diabetes duringintervention, individual evaluation ofan acceptable weight loss must be per-formed prior to initiation of liraglutidetreatment in patients with ESRD.
The study was not powered to con-clude on most of our secondary endpoints. Nevertheless, data on HbA1c,blood glucose, and change in doses ofbaseline antidiabetic treatment suggestthat the blood glucose–lowering effectof liraglutide is not impeded by severeuremia. Earlier studies by our group in-dicated that endogenous GLP-1 mighthave a reduced b-cell stimulatory effectin patients with ESRD (40,41), but thepresent results suggest that high plasmalevels of a GLP-1 receptor agonist cancircumvent this. Further studies testingthe efficacy of liraglutide in patients withadvanced stages of renal insufficiency arewarranted.
Our study has several limitations. Thestudy population was relatively small,which allows us to draw statistically sup-ported conclusions only on our primaryend point. Likewise, evaluation of po-tential severe, rare AEs, e.g., pancreati-tis (11), requires larger-scale studieswith longer follow-up. The primaryend point in our study is nonclinical;however, it is strictly objective and,therefore, representative of the popula-tion with ESRD, although our patientsrepresent a selected part of the popula-tion with diabetes and ESRD withthe least comorbidity. Gastrointestinalsymptoms, including nausea and occa-sionally vomiting, occur frequently inthe population with ESRD in general(Fig. 3). This impedes evaluation ofgastrointestinal side effects related toliraglutide to some extent. However, in-clusion of a placebo arm in the groupwith ESRD facilitated differentiation.Hemodialysis patients were examinedimmediately prior to a dialysis session,i.e., often with excess body fluid. This
affects weight and blood pressure meas-urements and complicates the evaluationof liraglutide-induced weight loss andchange in blood pressure.
In conclusion, our data suggest thatcontinuous liraglutide treatment is ap-plicable in patients with type 2 diabetesand ESRD, although larger-scale studiesare needed to confirm this. Dose reduc-tion and prolongation of the titrationperiod may be advisable to reduce nau-sea and vomiting, which occurred morefrequently in patients with ESRD. FewSAEs were reported, all seemingly unre-lated to liraglutide treatment. Glycemiccontrol did not deteriorate during lira-glutide treatment in the group withESRD, despite a significant reduction inbasal insulin doses. We observed a non-significant weight loss in the group withESRD, which may be an untoward effectin some dialysis patients.
Acknowledgments. The authors thank studynursesHelleCorinthandTanjaOlsen(Rigshospitalet,University of Copenhagen) for their skillfulworkand laboratory technician Andreas Haltorp(Rigshospitalet, University of Copenhagen) forbeing responsible for randomization throughoutthe study.Duality of Interest. This study was funded byNovo Nordisk. T.I. and B.F.-R. have receivedlecture fees and research support from NovoNordisk. F.K.K. has received research supportfrom Sanofi and is a member of the advisoryboards and has received lecture fees fromAstraZeneca, Eli Lilly and Company, ZealandPharma, Fractyl Laboratories, Novo Nordisk,and Sanofi. M.B.J. has received research supportfrom Novo Nordisk. T.J. holds shares in NovoNordisk A/S. J.J.H. has received grants fromNovartis and Merck Sharp & Dohme. J.J.H. is amember of the advisory boards and has con-sulted for GlaxoSmithKline, Zealand Pharma,AstraZeneca, Novo Nordisk, Intarcia Therapeu-tics, Hanmi Pharmaceutical, Sanofi, and MerckSharp & Dohme. None of the authors’ spouses,partners, or children has financial relationshipsthat could appear to have influenced the sub-mitted work. None of the authors has nonfinan-cial interests that could appear to haveinfluenced the submittedwork. No other poten-tial conflicts of interest relevant to this articlewere reported.
NovoNordiskdidnotparticipate in thewritingof the protocol; collection, analysis and inter-pretation of data; writing of the manuscript; ordecision to submit the article for publication.AuthorContributions. T.I. designed the study;wrote the study protocol; screened, recruited,and treated all study participants; performeddata analyses and statistical calculations; andwrote the initial draft of the manuscript. F.K.K.,J.J.H., M.H., and B.F.-R. designed the study.M.B.J.screened, recruited, and treated all study partic-ipants andperformeddataanalysesand statisticalcalculations. T.J. designed the studyand screened,
care.diabetesjournals.org Idorn and Associates 7

recruited, and treated all study participants. M.R.and P.M.H. screened, recruited, and treated allstudy participants. K.B.C. designed the study andperformed data analyses and statistical calcula-tions.Allauthorscontributedtothe interpretationof the data and the revision of the paper andapproved the final version of the manuscript. Thestudy data are the property of T.I., B.F.-R., andRigshospitalet.T.I.andB.F.-R.aretheguarantorsofthisworkand,assuch,hadfullaccess toall thedatainthestudyandtakeresponsibility for the integrityof the data and the accuracy of the data analysis.Prior Presentation. Parts of this study werepresented in abstract form and as a poster at the50th European Association for the Study ofDiabetes Annual Meeting, Vienna, Austria, 15–19 September 2014.
References1. U.S. Renal Data System. USRDS 2013 AnnualData Report: Atlas of Chronic Kidney Diseaseand End-Stage Renal Disease in the UnitedStates. Bethesda, MD, National Institutes ofHealth, National Institute of Diabetes and Diges-tive and Kidney Diseases, 2013, 1.218.ii2. Danish Society of Nephrology. Danish Ne-phrology Registry Annual Report 2013. Availablefrom http://www.nephrology.dk/Publikationer/Landsregister/%C3%85rsrapport%202013.pdf.Accessed 15 March 2015 [in Danish]3. Duckworth WC, Bennett RG, Hamel FG. In-sulin degradation: progress and potential. En-docr Rev 1998;19:608–6244. Rocco MV, Berns JS; National Kidney Foun-dation. KDOQI Clinical Practice Guideline for Di-abetes and CKD: 2012 Update. Am J Kidney Dis2012;60:850–8865. Williams ME, Garg R. Glycemic managementin ESRD and earlier stages of CKD. Am J KidneyDis 2014;63(Suppl. 2):S22–S386. Brouns R, De Deyn PP. Neurological compli-cations in renal failure: a review. Clin NeurolNeurosurg 2004;107:1–167. Graefe-Mody U, Friedrich C, Port A, et al. Ef-fect of renal impairment on the pharmacokineticsof the dipeptidyl peptidase-4 inhibitor linagliptin(*). Diabetes Obes Metab 2011;13:939–9468. Arjona Ferreira JC, Corry D, Mogensen CE,et al. Efficacy and safety of sitagliptin in patientswith type 2 diabetes and ESRD receiving dialysis:a 54-week randomized trial. Am J Kidney Dis2013;61:579–5879. Boulton DW, Li L, Frevert EU, et al. Influenceof renal or hepatic impairment on the pharma-cokinetics of saxagliptin. Clin Pharmacokinet2011;50:253–26510. Kothny W, Shao Q, Groop PH, LukashevichV. One-year safety, tolerability and efficacy ofvildagliptin in patients with type 2 diabetes andmoderate or severe renal impairment. DiabetesObes Metab 2012;14:1032–103911. Nakata H, Sugitani S, Yamaji S, et al. Pancre-atitis with pancreatic tail swelling associated withincretin-based therapies detected radiologically intwo cases of diabetic patients with end-stage re-nal disease. Intern Med 2012;51:3045–304912. Scheen AJ. Pharmacokinetics and clinicaluse of incretin-based therapies in patientswith chronic kidney disease and type 2 diabetes.Clin Pharmacokinet 2015;54:1–21
13. European Medicines Agency. Annex I, sum-mary of roduct characteristics (Victoza). Availablefrom http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/001026/WC500050017.pdf. Accessed 27Februrary 201514. European Medicines Agency. Annex I, sum-mary of product characteristics (Byetta). Availablefrom http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000698/WC500051845.pdf. Accessed 26January 201515. European Medicines Agency. Annex I, sum-mary of product characteristics (Lyxumia).Available from http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002445/WC500140401.pdf.Accessed 26 January 201516. European Medicines Agency. Annex I, sum-mary of product characteristics (Eperzan). Availablefrom http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002735/WC500165117.pdf. Accessed 26January 201517. EuropeanMedicines Agency. Annex 1, sum-mary of product characteristics (Bydureon).Available from http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002020/WC500108241.pdf.Accessed 26 January 201518. European Medicines Agency. Annex I, sum-mary of product characteristics (Trulicity). Availablefrom http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002825/WC500179470.pdf. Accessed 26January 201519. Idorn T, Knop FK, Jørgensen M, et al. Safetyand efficacy of liraglutide in patients with type 2diabetes and end-stage renal disease: protocolfor an investigator-initiated prospective, rando-mised, placebo-controlled, double-blinded, par-allel intervention study. BMJ Open 2013;3:e00276420. Chatterjee DJ, Khutoryansky N, ZdravkovicM, Sprenger CR, Litwin JS. Absence of QTc pro-longation in a thorough QT study with subcuta-neous liraglutide, a once-daily human GLP-1analog for treatment of type 2 diabetes. J ClinPharmacol 2009;49:1353–136221. Morrow L, Hompesch M, Guthrie H, ChangD, Chatterjee DJ. Co-administration of liraglu-tide with insulin detemir demonstrates additivepharmacodynamic effects with no pharmacoki-netic interaction. Diabetes Obes Metab 2011;13:75–8022. Agersø H, Jensen LB, Elbrønd B, Rolan P,Zdravkovic M. The pharmacokinetics, pharma-codynamics, safety and tolerability of NN2211, anew long-acting GLP-1 derivative, in healthymen. Diabetologia 2002;45:195–20223. Christensen M, Knop FK, Vilsbøll T, Holst JJ.Lixisenatide for type 2 diabetes mellitus. ExpertOpin Investig Drugs 2011;20:549–55724. Linnebjerg H, Kothare PA, Park S, et al. Effectof renal impairment on the pharmacokinetics ofexenatide. Br J Clin Pharmacol 2007;64:317–32725. Liu Y-H, Ruus P. Pharmacokinetics andsafety of the GLP-1 agonist AVE0010 in patientswith renal impairment (Abstract). Diabetes2009;59(Suppl. 1):A149–A150
26. Filippatos TD, ElisafMS. Effects of glucagon-like peptide-1 receptor agonists on renal func-tion. World J Diabetes 2013;4:190–20127. Neumiller JJ. Differential chemistry (struc-ture), mechanism of action, and pharmacologyof GLP-1 receptor agonists and DPP-4 inhibitors.J Am Pharm Assoc (2003) 2009;49(Suppl. 1):S16–S2928. Malm-Erjefalt M, Bjørnsdottir I, Vanggaard J,et al. Metabolism and excretion of the once-dailyhuman glucagon-like peptide-1 analog liraglutide inhealthy male subjects and its in vitro degradationby dipeptidyl peptidase IV and neutral endopepti-dase. Drug Metab Dispos 2010;38:1944–195329. Davidson JA, Brett J, Falahati A, Scott D. Mildrenal impairment and the efficacy and safety ofliraglutide. Endocr Pract 2011;17:345–35530. Jacobsen LV, Hindsberger C, Robson R,Zdravkovic M. Effect of renal impairment onthe pharmacokinetics of the GLP-1 analogue lir-aglutide. Br J Clin Pharmacol 2009;68:898–90531. Osonoi T, Saito M, Tamasawa A, et al. Effectof hemodialysis on plasma glucose profile andplasma level of liraglutide in patients with type 2diabetes mellitus and end-stage renal disease:a pilot study. PLoS One 2014;9:e11346832. Umpierrez G, Atkin S, Bain S, et al. Efficacyand safety of liraglutide versus placebo in sub-jects with type 2 diabetes and moderate renalimpairment (LIRA-RENAL): a randomised trial.Diabetologia 2014;57:S8433. Kaakeh Y, Kanjee S, Boone K, Sutton J.Liraglutide-induced acute kidney injury. Pharma-cotherapy 2012;32:e7–e1134. U.S. Food and Drug Administration. Highlightsof prescribing information. Available from http://www.accessdata.fda.gov/drugsatfda_docs/label/2013/022341s020lbl.pdf. Accessed 26 January201535. Astrup A, Rossner S, Van Gaal L, et al.;NN8022-1807 Study Group. Effects of liraglutidein the treatment of obesity: a randomised,double-blind, placebo-controlled study. Lancet2009;374:1606–161636. Kalantar-Zadeh K, Abbott KC, SalahudeenAK, Kilpatrick RD, Horwich TB. Survival advan-tages of obesity in dialysis patients. Am J ClinNutr 2005;81:543–55437. Yen TH, Lin JL, Lin-Tan DT, Hsu CW. Associ-ation between bodymass andmortality inmain-tenance hemodialysis patients. Ther Apher Dial2010;14:400–40838. Kalantar-Zadeh K, Kopple JD. Obesity paradoxin patients on maintenance dialysis. ContribNephrol 2006;151:57–6939. Kalantar-Zadeh K, Streja E, Kovesdy CP,et al. The obesity paradox and mortality associ-ated with surrogates of body size and musclemass in patients receiving hemodialysis. MayoClin Proc 2010;85:991–100140. Idorn T, Knop FK, Jørgensen M, Holst JJ,Hornum M, Feldt-Rasmussen B. Gastrointesti-nal factors contribute to glucometabolic distur-bances in nondiabetic patients with end-stagerenal disease. Kidney Int 2013;83:915–92341. Idorn T, Knop FK, Jørgensen M, Holst JJ,Hornum M, Feldt-Rasmussen B. Postprandial re-sponses of incretin and pancreatic hormones innon-diabetic patients with end-stage renal dis-ease. Nephrol Dial Transplant 2014;29:119–127
8 Liraglutide for Dialysis Patients With Diabetes Diabetes Care


![Liraglutide for the treatment of diabetes mellitus in Japan...blood glucose (area under the curve [AUC] glucose, 0–24h /24) in patients receiving liraglutide was 20% lower in the](https://img.dokumen.tips/doc/110x75/5f9549b2f923ea510e621f77/liraglutide-for-the-treatment-of-diabetes-mellitus-in-japan-blood-glucose-area.jpg)


























