Embed Size (px)
Citation preview
AA
SL
DA
bst
ract
s(± SD) of 8.4 (±8.9) weeks from the time of viral breakthrough. Resistance patterns weredetected in 6 of 8 (75%) patients and all patients had cross-resistance to boceprevir. All 4patients with higher-level resistance patterns were genotype 1a. Both patients who testedsensitive were genotype 1b. Conclusion: Similar to findings in clinical trials, viral break-through with DAA for treatment of chronic HCV infection is associated with genotype 1a,advanced liver fibrosis, and prior null treatment response. Comparable patterns of resistancewere also seen in clinical practice. In our study, however, a significant proportion of patientsexperienced viral breakthrough after completion of the DAA portion of triple therapy. Morefrequent virologic assessments during the PR treatment phase may be useful in a subset of"higher-risk" patients to expedite compliance with stopping rules and decrease unnecessarytreatment burden.Treatment Response of Patients with Viral Breakthrough
*Time between confirmation of viral breakthrough and testing of resistance **Any reductionin dosing of either ribavirin or interferon during treatment course ND = not detectable,defined as a viral load of less than 5 IU per millimeter; vBT = viral breakthrough RBV =ribavirin; IFN = interferon-alfa Higher-level resistance: V36M + R155K, Lower-level resis-tance: A156S, T54S All viral load results are expressed as IU per millimeter.
Sa1041
Triple Therapy Under Real Life Conditions: Telaprevir (TVR) and Boceprevir(BOC) in Combination With Peginterferon-Alfa-2A Plus Ribavirin (P/R) inTreatment Experienced Patients Infected With Chronic Hepatitis C, Genotype1. the PAN StudyGero Moog, Stefan Mauss, Dietrich Hueppe, Ulrich Spengler, Eckart Schott, ChristophEisenbach, Andreas Schober, Renate Heyne, Maria-Christina Jung, Gerlinde Teuber,Margareta Frank Doss, Martin Rössle, Stefan Pape, Marcus Schuchmann, Ulrich Alshuth,Peter Buggisch
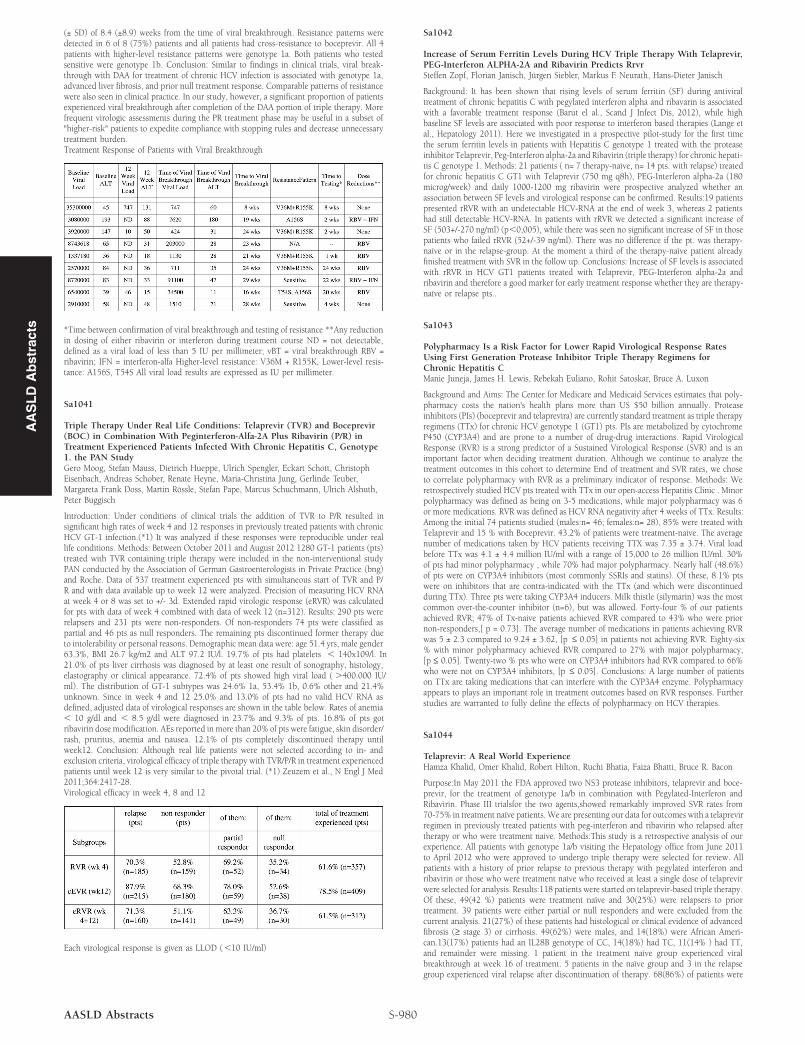
Introduction: Under conditions of clinical trials the addition of TVR to P/R resulted insignificant high rates of week 4 and 12 responses in previously treated patients with chronicHCV GT-1 infection.(*1) It was analyzed if these responses were reproducible under reallife conditions. Methods: Between October 2011 and August 2012 1280 GT-1 patients (pts)treated with TVR containing triple therapy were included in the non-interventional studyPAN conducted by the Association of German Gastroenterologists in Private Practice (bng)and Roche. Data of 537 treatment experienced pts with simultaneous start of TVR and P/R and with data available up to week 12 were analyzed. Precision of measuring HCV RNAat week 4 or 8 was set to +/- 3d. Extended rapid virologic response (eRVR) was calculatedfor pts with data of week 4 combined with data of week 12 (n=312). Results: 290 pts wererelapsers and 231 pts were non-responders. Of non-responders 74 pts were classified aspartial and 46 pts as null responders. The remaining pts discontinued former therapy dueto intolerability or personal reasons. Demographic mean data were: age 51.4 yrs, male gender63.3%, BMI 26.7 kg/m2 and ALT 97.2 IU/l. 19.7% of pts had platelets , 140x109/l. In21.0% of pts liver cirrhosis was diagnosed by at least one result of sonography, histology,elastography or clinical appearance. 72.4% of pts showed high viral load ( .400.000 IU/ml). The distribution of GT-1 subtypes was 24.6% 1a, 53.4% 1b, 0.6% other and 21.4%unknown. Since in week 4 and 12 25.0% and 13.0% of pts had no valid HCV RNA asdefined, adjusted data of virological responses are shown in the table below. Rates of anemia, 10 g/dl and , 8.5 g/dl were diagnosed in 23.7% and 9.3% of pts. 16.8% of pts gotribavirin dose modification. AEs reported in more than 20% of pts were fatigue, skin disorder/rash, pruritus, anemia and nausea. 12.1% of pts completely discontinued therapy untilweek12. Conclusion: Although real life patients were not selected according to in- andexclusion criteria, virological efficacy of triple therapy with TVR/P/R in treatment experiencedpatients until week 12 is very similar to the pivotal trial. (*1) Zeuzem et al., N Engl J Med2011;364:2417-28.Virological efficacy in week 4, 8 and 12
Each virological response is given as LLOD (,10 IU/ml)
S-980AASLD Abstracts
Sa1042
Increase of Serum Ferritin Levels During HCV Triple Therapy With Telaprevir,PEG-Interferon ALPHA-2A and Ribavirin Predicts RrvrSteffen Zopf, Florian Janisch, Jürgen Siebler, Markus F. Neurath, Hans-Dieter Janisch
Background: It has been shown that rising levels of serum ferritin (SF) during antiviraltreatment of chronic hepatitis C with pegylated interferon alpha and ribavarin is associatedwith a favorable treatment response (Barut el al., Scand J Infect Dis, 2012), while highbaseline SF levels are associated with poor response to interferon based therapies (Lange etal., Hepatology 2011). Here we investigated in a prospective pilot-study for the first timethe serum ferritin levels in patients with Hepatitis C genotype 1 treated with the proteaseinhibitor Telaprevir, Peg-Interferon alpha-2a and Ribavirin (triple therapy) for chronic hepati-tis C genotype 1. Methods: 21 patients ( n= 7 therapy-naïve, n= 14 pts. with relapse) treatedfor chronic hepatitis C GT1 with Telaprevir (750 mg q8h), PEG-Interferon alpha-2a (180microg/week) and daily 1000-1200 mg ribavirin were prospective analyzed whether anassociation between SF levels and virological response can be confirmed. Results:19 patientspresented rRVR with an undetectable HCV-RNA at the end of week 3, whereas 2 patientshad still detectable HCV-RNA. In patients with rRVR we detected a significant increase ofSF (503+/-270 ng/ml) (p,0,005), while there was seen no significant increase of SF in thosepatients who failed rRVR (52+/-39 ng/ml). There was no difference if the pt. was therapy-naïve or in the relapse-group. At the moment a third of the therapy-naïve patient alreadyfinished treatment with SVR in the follow up. Conclusions: Increase of SF levels is associatedwith rRVR in HCV GT1 patients treated with Telaprevir, PEG-Interferon alpha-2a andribavirin and therefore a good marker for early treatment response whether they are therapy-naïve or relapse pts..
Sa1043
Polypharmacy Is a Risk Factor for Lower Rapid Virological Response RatesUsing First Generation Protease Inhibitor Triple Therapy Regimens forChronic Hepatitis CManie Juneja, James H. Lewis, Rebekah Euliano, Rohit Satoskar, Bruce A. Luxon
Background and Aims: The Center for Medicare and Medicaid Services estimates that poly-pharmacy costs the nation's health plans more than US $50 billion annually. Proteaseinhibitors (PIs) (boceprevir and telaprevira) are currently standard treatment as triple therapyregimens (TTx) for chronic HCV genotype 1 (GT1) pts. PIs are metabolized by cytochromeP450 (CYP3A4) and are prone to a number of drug-drug interactions. Rapid VirologicalResponse (RVR) is a strong predictor of a Sustained Virological Response (SVR) and is animportant factor when deciding treatment duration. Although we continue to analyze thetreatment outcomes in this cohort to determine End of treatment and SVR rates, we choseto correlate polypharmacy with RVR as a preliminary indicator of response. Methods: Weretrospectively studied HCV pts treated with TTx in our open-access Hepatitis Clinic . Minorpolypharmacy was defined as being on 3-5 medications, while major polypharmacy was 6or more medications. RVR was defined as HCV RNA negativity after 4 weeks of TTx. Results:Among the initial 74 patients studied (males:n= 46; females:n= 28), 85% were treated withTelaprevir and 15 % with Boceprevir. 43.2% of patients were treatment-naive. The averagenumber of medications taken by HCV patients receiving TTX was 7.35 ± 3.74. Viral loadbefore TTx was 4.1 ± 4.4 million IU/ml with a range of 15,000 to 26 million IU/ml. 30%of pts had minor polypharmacy , while 70% had major polypharmacy. Nearly half (48.6%)of pts were on CYP3A4 inhibitors (most commonly SSRIs and statins). Of these, 8.1% ptswere on inhibitors that are contra-indicated with the TTx (and which were discontinuedduring TTx). Three pts were taking CYP3A4 inducers. Milk thistle (silymarin) was the mostcommon over-the-counter inhibitor (n=6), but was allowed. Forty-four % of our patientsachieved RVR; 47% of Tx-naive patients achieved RVR compared to 43% who were priornon-responders,[ p = 0.73]. The average number of medications in patients achieving RVRwas 5 ± 2.3 compared to 9.24 ± 3.62, [p ≤ 0.05] in patients not achieving RVR. Eighty-six% with minor polypharmacy achieved RVR compared to 27% with major polypharmacy,[p ≤ 0.05]. Twenty-two % pts who were on CYP3A4 inhibitors had RVR compared to 66%who were not on CYP3A4 inhibitors, [p ≤ 0.05]. Conclusions: A large number of patientson TTx are taking medications that can interfere with the CYP3A4 enzyme. Polypharmacyappears to plays an important role in treatment outcomes based on RVR responses. Furtherstudies are warranted to fully define the effects of polypharmacy on HCV therapies.
Sa1044
Telaprevir: A Real World ExperienceHamza Khalid, Omer Khalid, Robert Hilton, Ruchi Bhatia, Faiza Bhatti, Bruce R. Bacon
Purpose:In May 2011 the FDA approved two NS3 protease inhibitors, telaprevir and boce-previr, for the treatment of genotype 1a/b in combination with Pegylated-Interferon andRibavirin. Phase III trialsfor the two agents,showed remarkably improved SVR rates from70-75% in treatment naïve patients. We are presenting our data for outcomes with a telaprevirregimen in previously treated patients with peg-interferon and ribavirin who relapsed aftertherapy or who were treatment naive. Methods:This study is a retrospective analysis of ourexperience. All patients with genotype 1a/b visiting the Hepatology office from June 2011to April 2012 who were approved to undergo triple therapy were selected for review. Allpatients with a history of prior relapse to previous therapy with pegylated interferon andribavirin or those who were treatment naïve who received at least a single dose of telaprevirwere selected for analysis. Results:118 patients were started on telaprevir-based triple therapy.Of these, 49(42 %) patients were treatment naïve and 30(25%) were relapsers to priortreatment. 39 patients were either partial or null responders and were excluded from thecurrent analysis. 21(27%) of these patients had histological or clinical evidence of advancedfibrosis (≥ stage 3) or cirrhosis. 49(62%) were males, and 14(18%) were African Ameri-can.13(17%) patients had an IL28B genotype of CC, 14(18%) had TC, 11(14% ) had TT,and remainder were missing. 1 patient in the treatment naïve group experienced viralbreakthrough at week 16 of treatment. 5 patients in the naïve group and 3 in the relapsegroup experienced viral relapse after discontinuation of therapy. 68(86%) of patients were

virus negative by week 4. All patients in both groups achieved HCV RNA levels ≤ 1000 IU/ml by week 12. 44 patients had a significant decrease in hemoglobin levels to ,10 g/dland required transfusion and/or erythropoetin.2 patients discontinued treatment due tosevere anemia. Moderate to severe rash was noted in 19 patients. 6 patients discontinuedtherapy due to severe rash. All others were able to continue treatment with systemic anti-histamines and/or topical steroids.1 patient with cirrhosis decompensated after initiation oftherapy resulting in death. Of the 79 patients, 69(87%) have completed 24 weeks of treatmentand have achieved undetected HCV RNA levels. 64(81%) patients have achieved sustainedviral response at 24weeks of followup. Conclusion:Triple therapywas generally well tolerated.Rash was seen to occur in the majority of patients, requiring treatment and some patientsdiscontinued therapy. Our patients were closely followed by hepatologists with assistancefrom mid-level providers reinforcing adherence to therapy in an algorithmic approach. Ouroutcomes with telaprevir presents a "real-world" experience and are comparable to thoseseen in clinical trials.
Sa1045
Dynamic Changes of Health-Related Quality of Life After Pegylated Interferonand Ribavirin Treatment for Chronic Hepatitis CChi-Yang Chang, Lein-Ray Mo, Chen-Haug Tseng, Yao-Chun Hsu, Jaw-Town Lin
Background: Patients with chronic hepatitis C have lower health-related quality of life(HRQOL) compared to general population. Combination treatment with pegylated interferon(peg-IFN) and ribavirin (RBV) could improve liver function, reduce the viral load, andimprove HRQOL. However, multiple side effects would interfere the HRQOL during treat-ment course and lower adherence of combination therapy. No study has shown the changesof detailed profiles of HRQOL changes along with time. Aim: The aim of this study was toevaluate the effects of peg-IFN and RBV for chronic hepatitis C on the dynamic changes ofHRQOL during the first year of follow-up. Material and Methods: Patients with chronichepatitis C were enrolled for treatment with combined peg-IFN and RBV for 24 or 48 weeksby the recommendation of the Asian Pacific Association for the Study of the Liver (APASAL).The World Health Organization Quality of Life-Brief (WHOQOL-BREF) was administeredbefore the combined treatment with peg-IFN and RBV and 4, 12, 24, and 48 and/or 72weeks after initiation of treatment. Viral load, side effects, haemoglobin, liver functionwere measured at these times. A mixed-effect model was constructed to analyse repeatedmeasurements and determine the relationships between viral load, haemoglobin, othervariables and WHOQOL-BREF scores during follow-up. A reference group with age-, sex-, and municipality-matched healthy subjects will be randomly sampled from the databaseof 2001 National Health Interview Survey. Results: A total of 102 patients were enrolled.Themixed-effect model showed that the physical, psychological and social domains improvedafter combination therapy, with simultaneous reduction in viral load. The reduction of QOLscores was more significant during first 4 weeks. There was a dip in scores of physical andpsychological domains 12 weeks after initiation of treatment, significantly related to reductionof haemoglobin level and side effects such as fatigue and dizziness. All patients graduallyimproved 12 weeks after initiation of treatment to 24 weeks after end of treatment, reachinglevels similar to those of healthy subjects. The reduction of haemoglobin level interferedwith various facets, including energy and fatigue, mobility, activities of daily living, workingcapacity, sexual activity, positive feelings, thinking, learning, memory & concentration, self-esteem, and dependence on medication or treatments. Conclusions: The reduction of viralload associated with improvement of HRQOL. Anemia and other side effects would interfereHRQOL, which decreased during first 12 weeks after initiation of treatment, and improvedagain up to 24 weeks after the end of treatment.
Sa1046
Analysis of Early Treatment Discontinuations in Hepatitis C (HCV) TripleTherapy EraAnastasia Shnitser, Doris H. Chan, Steven Herrine, Jonathan M. Fenkel
Background: The addition of the direct-acting antiviral (DAA) agents boceprevir (B) ortelaprevir (T) to peginterferon (P) and ribavirin (R) provides sustained virologic response(SVR) in approximately 75% of patients with genotype 1 (g1) HCV in phase 3 clinical trials,with low side effect-related treatment discontinuation rates of 10-13% (T) and 2-3% (B).Due to a small percentage of patients with cirrhosis in the registration trials, we hypothesizedthat treatment discontinuation would be more frequent in our practice, which has a highervolume of patients with cirrhosis. Methods: We performed a retrospective chart review ofall patients treated with PRT or PRB triple therapy for g1 HCV at a single clinical-trialsexperienced academic liver transplant center whose regimen was initiated prior June 30,2012. Lab, clinical, and demographic data including viral loads at weeks 4, 12, 24, end oftreatment, and SVR12 were collected. Results: 120 patients initiated triple therapy duringthe study period - 90 (75%) with PRT and 30 (25%) with PRB. Demographics were similarbetween the two treatment regimens with a median age of 56, 40% with cirrhosis and 58.3%with previous treatment failure. Early treatment discontinuation occurred in 56 patients(46.7%). Of these, half were due to on-treatment virologic failure (futility or viral break-through) and half were due to side effects, with no significant differences between patientsreceiving either regimen (Table 1). Treatment discontinuation occurred more often in patientswith cirrhosis (56.3%), though it did not reach statistical significance (OR 1.91, 95% CI0.91 - 3.99, p=0.096). One patient discontinued at week 29 of PRT (SVR12) due to livertransplantation and one patient discontinued at week 12 of PRT (relapse) due to lost insurancecoverage. Overall, 7/56 patients (12.5%) with early discontinuation still achieved SVR12(Table 2) with treatment duration ranging 12-38 weeks. Hepatic decompensation occurredin 5 patients with cirrhosis (10.4%), with none achieving SVR. Two non-cirrhotic patientsdiscontinued secondary to dermatologic side effects (one DRESS syndrome and one intracta-ble pruritus). Five patients, all with cirrhosis, discontinued due to hematologic side effectsuncontrolled by dose reductions, growth factors, and transfusions. There were no mortalities.Conclusion: Early treatment discontinuation was more common in our clinical practice thanreported in clinical trials, and was as likely to be due to side effects as to on-treatmentvirologic failure. More than half of patients with cirrhosis discontinued treatment early.
S-981 AASLD Abstracts
Despite early discontinuation, one in eight patients still achieved SVR12; therefore continuedclinical and laboratory monitoring is recommended in this population.Table 1: Breakdown of Early Terminations
Table 2: SVR12 with Early Termination
Sa1047
The Real Life Experience With the Development and Management of Anemiain the Era of Protease Inhibitors for Chronic Hepatitis C InfectionGurshawn Singh, Danny Issa, Brigette Bevly, Ibrahim A. Hanouneh, Rocio Lopez, NizarN. Zein, Naim Alkhouri
Triple therapy with protease inhibitors, telaprevir and boceprevir, is the new standard oftreatment for hepatitis C virus (HCV) genotype 1 infection. In this study, we investigatedthe natural history of anemia in patients who are treated with triple therapy compared tothose treated with peg-interferon and ribavirin (PEG/RBV) and how the treatment of anemiadiffered in the real-life setting. Methods: Anemia was monitored in 72 consecutive patientstreated with telaprevir- (46) or boceprevir-based triple therapy (26) for at least 16 weeks.These patients were matched to 72 controls with respect to age, sex, race, and fibrosis thatwere treated previously with PEG/RBV. All patients had baseline blood work done beforetreatment and weekly hemoglobin levels. Symptomatic anemia or medically significant dropsin hemoglobin levels were treated by dose reductions of ribavirin (RBV), red blood celltransfusions, epoetin alfa (EPO), or taken off treatment based on the clinician's judgment.Univariable and multivariable logistic regression analyses were performed. Results: The meanage for the study population was 52.1 years, 58.3% were male, 41.4% were treatment naïve,and 30.3% were cirrhotic. The mean baseline hemoglobin was 14.8±1.3 g/dL. Incidence ofgrade 2-4 anemia (hemoglobin , 10g/dL) in patients was 50% for those treated withtelaprevir, 54.2% for those treated with boceprevir, and 23.2% treated with PEG/RBV (p ,0.005). Lowest mean hemoglobin was 10.3±1.8 g/dL, 10.4±1.8 g/dL, and 11.0 for telaprevir,boceprevir, and controls respectively (p,0.061). Hemoglobin nadir was reached betweentreatment weeks 6-10 in all treatment arms (figure 1). Anemia required RBV dose reductionin 60% of those on telaprevir, 57.1% of those on boceprevir, and 17.9% of the controls(p,0.001). Patients who had anemia requiring EPO and/or RBC transfusion was 52.2% fortelaprevir, 50% for boceprevir, and 40.3% for PEG/RBV (p ,0.4), and therefore was notsignificantly different between the three groups. None of the patients had to discontinueHCV therapy due to anemia. Conclusion: Using protease inhibitors to treat patients withhepatitis C does result in more significant anemia when compared to treatment with PEG/RBV alone. However, this can be treated effectively with ribavirin dose reductions ratherthan resorting to red blood cell transfusions or EPO injections.
Figure 1: Hemoglobin levels during hepatitis C treatment for the 3 treatment groups
Sa1048
Treatment Outcomes With Boceprevir Triple Therapy in Black Patients At anUrban Clinic At a Tertiary Care Medical CenterAdrian M. Majid, Luciano Kapelusznik, Eric R. Cox, Samer S. El-Kamary, Bonnie Charon,Judith Myers, Christina Dickson, Yolanda Flores, Robert Knodell, Rohit Talwani
Background: Treatment of chronic HCV infection with boceprevir (BOC)-based triple therapyhas improved sustained virologic response (SVR) rates in both treatment-naïve and previ-ously-treated blacks, but these response rates remain lower than nonblacks. Treatmentefficacy and tolerability of BOC in black patients compared to Caucasians has not beendescribed outside of clinical trials. This study reports outcomes of a black cohort at a largeurban clinic. Methods: We retrospectively identified all patients at our center initiated on
AA
SL
DA
bst
ract
s




























