Embed Size (px)
Citation preview
Ruptured Abdominal Aortic Aneurysm: DoesTrauma Center Designation Affect Outcome?
Farida Bounoua,1 Rob Schuster,1 Prabhjot Grewal,1 Kenneth Waxman,1
and Paul Cisek,2 Santa Barbara, California
Ruptured abdominal aortic aneurysm (RAAA) continues to be a major cause of mortality in theUnited States. Rapid diagnosis and uncomplicated surgical repair remain paramount to improv-ing survival in this population. We proposed that the addition of an organized trauma service andsubsequent improved management of critically ill patients who present with RAAA would posi-tively impact overall mortality. A retrospective analysis was performed on all patients treatedfor RAAA at Santa Barbara Cottage Hospital for the years 1985-2004. Patients treated beforelevel II trauma center designation (1985-1999) were compared to those treated after the traumacenter was instituted. A total of 76 patients were included in this analysis. The two groups weresimilar with regard to demographics. However, significant decreases in transport time from theemergency department to the operating room and overall 30-day mortality were seen in patientsafter the trauma center designation. This designation also led to an increase in the number ofcases performed per year, centralizing the treatment for these critically ill patients. Institutionof a well-prepared and organized service, such as trauma, improved the outcome for patientstreated with RAAA, with a particular benefit in the unstable patient.
INTRODUCTION
Ruptured abdominal aortic aneurysm (RAAA) con-
tinues to be a major cause of mortality in the United
States. RAAA currently ranks fifteenth among all
causes of death for men in the United States each
year.1 Expedient diagnosis and uncomplicated sur-
gical repair remain of paramount importance to im-
proving the chances of survival in this population.
However, even with advances in surgical and perio-
perative care, RAAA is associated with a mortality
rate of 45-58% and an overall mortality of 75-
90%, including prehospital deaths. These dismal
Presented at the 23rd Annual Meeting of the Southern CaliforniaVascular Surgical Society, La Quinta, CA, May 13-15, 2005.
1Department of Surgery Santa Barbara Cottage Hospital, SantaBarbara, CA, USA.
2Department of Vascular Surgery, Sansum Santa Barbara MedicalFoundation Clinic, Santa Barbara, CA, USA.
Correspondence to: Paul Cisek, MD, Sansum Santa Barbara Clinic,317 West Pueblo Street, Santa Barbara, CA 93105, USA, E-mail:[email protected]
Ann Vasc Surg 2007; 21: 133-136DOI: 10.1016/j.avsg.2007.01.003� Annals of Vascular Surgery Inc.Published online: March 9, 2007
mortality rates have not significantly improved in
the past 20 years.1-5 Many factors have been dis-
cussed in the literature with regard to predicting
mortality in patients with RAAA. These factors in-
clude blood pressure, hemoglobin level, creatinine
level, blood transfusion requirement, temperature,
cardiac arrest, acidosis, age, and female gender.6-8
Certainly, all physicians treating RAAA agree that
these patients need operative intervention as
quickly as possible since delays in transport to the
operating room are associated with increased
mortality.9 This often requires an organized team
approach with designated operating rooms and staff
for support.
Santa Barbara Cottage Hospital is a 350-bed com-
munity teaching hospital. In 1999 the hospital was
first designated as a level II trauma center by the
American College of Surgeons. In order to achieve
and maintain this designation, a dedicated trauma
team consisting of a surgeon, resident physician
staff, anesthesiology, neurosurgery, orthopedics,
on-call nurses, and ancillary staff must be well pre-
pared to rapidly assess and treat critically ill patients.
Although not specifically designed to treat vascular
emergencies, this team remains equipped to handle
all surgical emergencies.
133
134 Bounoua et al. Annals of Vascular Surgery
We proposed that the addition of this organized
trauma service and subsequent improved manage-
ment would positively impact overall mortality for
patients presenting with RAAA.
METHODS
A retrospective analysis was performed for all pa-
tients treated for RAAA at Santa Barbara Cottage
Hospital between February 1985 and December
2004. All patients refusing surgical intervention
were excluded. After institutional review board
approval, all patient charts were reviewed based
on Current Procedural Terminology (CPT) codes
for ruptured infrarenal AAAs. Demographic and
preoperative factors recorded included age, sex, co-
morbidities, blood pressure, and transport time from
the emergency department to the operating room.
In addition, intraoperative and postoperative data
were gathered. Primary outcome was 30-day
mortality.
The patients were stratified into two groups:
those treated from 1985 to 1999 before the level II
trauma center designation (group I) and those
treated after the designation (group II). The patients
were further evaluated with respect to hemody-
namic status on arrival as stable versus unstable.
Unstable patients were defined as those with a re-
corded systolic blood pressure of<90 mm Hg on pre-
sentation to the emergency room. In addition,
distance traveled to the hospital was recorded.
Data were analyzed using GraphPad� (GraphPad,
San Diego, CA) software. Groups were compared
using Student’s two-tailed t-test. Statistical signifi-
cance was achieved at P < 0.05.
RESULTS
A total of 100 patients were treated at our institution
for RAAA from 1985 to 2004. Twenty-four patients
refused treatment, and all expired. The remaining
76 patients underwent open repair of RAAA and
are the focus of this report.
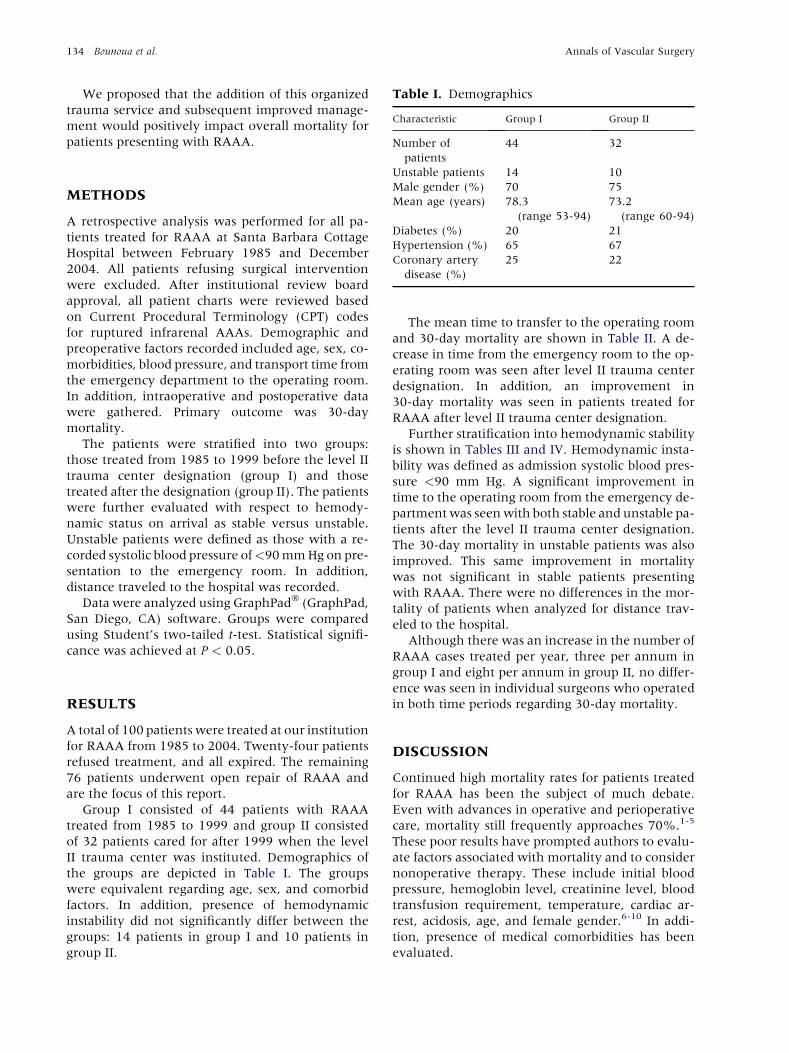
Group I consisted of 44 patients with RAAA
treated from 1985 to 1999 and group II consisted
of 32 patients cared for after 1999 when the level
II trauma center was instituted. Demographics of
the groups are depicted in Table I. The groups
were equivalent regarding age, sex, and comorbid
factors. In addition, presence of hemodynamic
instability did not significantly differ between the
groups: 14 patients in group I and 10 patients in
group II.
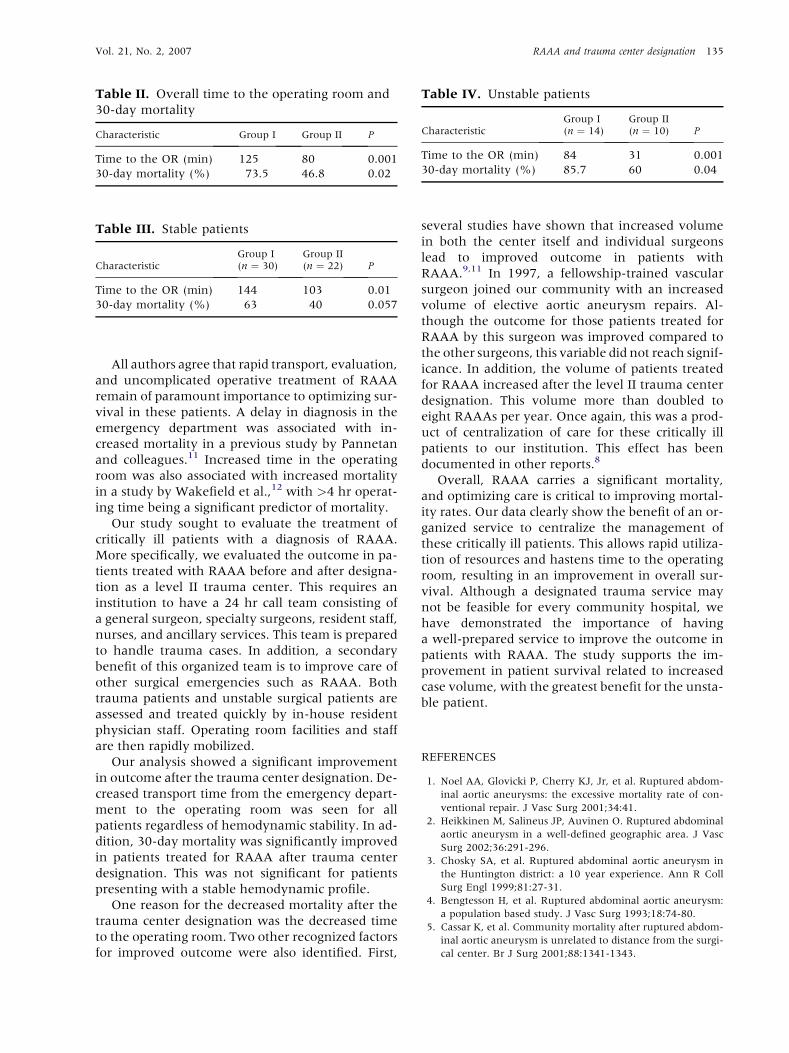
The mean time to transfer to the operating room
and 30-day mortality are shown in Table II. A de-
crease in time from the emergency room to the op-
erating room was seen after level II trauma center
designation. In addition, an improvement in
30-day mortality was seen in patients treated for
RAAA after level II trauma center designation.
Further stratification into hemodynamic stability
is shown in Tables III and IV. Hemodynamic insta-
bility was defined as admission systolic blood pres-
sure <90 mm Hg. A significant improvement in
time to the operating room from the emergency de-
partment was seen with both stable and unstable pa-
tients after the level II trauma center designation.
The 30-day mortality in unstable patients was also
improved. This same improvement in mortality
was not significant in stable patients presenting
with RAAA. There were no differences in the mor-
tality of patients when analyzed for distance trav-
eled to the hospital.
Although there was an increase in the number of
RAAA cases treated per year, three per annum in
group I and eight per annum in group II, no differ-
ence was seen in individual surgeons who operated
in both time periods regarding 30-day mortality.
DISCUSSION
Continued high mortality rates for patients treated
for RAAA has been the subject of much debate.
Even with advances in operative and perioperative
care, mortality still frequently approaches 70%.1-5
These poor results have prompted authors to evalu-
ate factors associated with mortality and to consider
nonoperative therapy. These include initial blood
pressure, hemoglobin level, creatinine level, blood
transfusion requirement, temperature, cardiac ar-
rest, acidosis, age, and female gender.6-10 In addi-
tion, presence of medical comorbidities has been
evaluated.
Table I. Demographics
Characteristic Group I Group II
Number of
patients
44 32
Unstable patients 14 10
Male gender (%) 70 75
Mean age (years) 78.3
(range 53-94)
73.2
(range 60-94)
Diabetes (%) 20 21
Hypertension (%) 65 67
Coronary artery
disease (%)
25 22
Vol. 21, No. 2, 2007 RAAA and trauma center designation 135
All authors agree that rapid transport, evaluation,
and uncomplicated operative treatment of RAAA
remain of paramount importance to optimizing sur-
vival in these patients. A delay in diagnosis in the
emergency department was associated with in-
creased mortality in a previous study by Pannetan
and colleagues.11 Increased time in the operating
room was also associated with increased mortality
in a study by Wakefield et al.,12 with >4 hr operat-
ing time being a significant predictor of mortality.
Our study sought to evaluate the treatment of
critically ill patients with a diagnosis of RAAA.
More specifically, we evaluated the outcome in pa-
tients treated with RAAA before and after designa-
tion as a level II trauma center. This requires an
institution to have a 24 hr call team consisting of
a general surgeon, specialty surgeons, resident staff,
nurses, and ancillary services. This team is prepared
to handle trauma cases. In addition, a secondary
benefit of this organized team is to improve care of
other surgical emergencies such as RAAA. Both
trauma patients and unstable surgical patients are
assessed and treated quickly by in-house resident
physician staff. Operating room facilities and staff
are then rapidly mobilized.
Our analysis showed a significant improvement
in outcome after the trauma center designation. De-
creased transport time from the emergency depart-
ment to the operating room was seen for all
patients regardless of hemodynamic stability. In ad-
dition, 30-day mortality was significantly improved
in patients treated for RAAA after trauma center
designation. This was not significant for patients
presenting with a stable hemodynamic profile.
One reason for the decreased mortality after the
trauma center designation was the decreased time
to the operating room. Two other recognized factors
for improved outcome were also identified. First,
Table II. Overall time to the operating room and
30-day mortality
Characteristic Group I Group II P
Time to the OR (min) 125 80 0.001
30-day mortality (%) 73.5 46.8 0.02
Table III. Stable patients
CharacteristicGroup I(n ¼ 30)
Group II(n ¼ 22) P
Time to the OR (min) 144 103 0.01
30-day mortality (%) 63 40 0.057
several studies have shown that increased volume
in both the center itself and individual surgeons
lead to improved outcome in patients with
RAAA.9,11 In 1997, a fellowship-trained vascular
surgeon joined our community with an increased
volume of elective aortic aneurysm repairs. Al-
though the outcome for those patients treated for
RAAA by this surgeon was improved compared to
the other surgeons, this variable did not reach signif-
icance. In addition, the volume of patients treated
for RAAA increased after the level II trauma center
designation. This volume more than doubled to
eight RAAAs per year. Once again, this was a prod-
uct of centralization of care for these critically ill
patients to our institution. This effect has been
documented in other reports.8
Overall, RAAA carries a significant mortality,
and optimizing care is critical to improving mortal-
ity rates. Our data clearly show the benefit of an or-
ganized service to centralize the management of
these critically ill patients. This allows rapid utiliza-
tion of resources and hastens time to the operating
room, resulting in an improvement in overall sur-
vival. Although a designated trauma service may
not be feasible for every community hospital, we
have demonstrated the importance of having
a well-prepared service to improve the outcome in
patients with RAAA. The study supports the im-
provement in patient survival related to increased
case volume, with the greatest benefit for the unsta-
ble patient.
REFERENCES
1. Noel AA, Glovicki P, Cherry KJ, Jr, et al. Ruptured abdom-
inal aortic aneurysms: the excessive mortality rate of con-
ventional repair. J Vasc Surg 2001;34:41.
2. Heikkinen M, Salineus JP, Auvinen O. Ruptured abdominal
aortic aneurysm in a well-defined geographic area. J Vasc
Surg 2002;36:291-296.
3. Chosky SA, et al. Ruptured abdominal aortic aneurysm in
the Huntington district: a 10 year experience. Ann R Coll
Surg Engl 1999;81:27-31.
4. Bengtesson H, et al. Ruptured abdominal aortic aneurysm:
a population based study. J Vasc Surg 1993;18:74-80.
5. Cassar K, et al. Community mortality after ruptured abdom-
inal aortic aneurysm is unrelated to distance from the surgi-
cal center. Br J Surg 2001;88:1341-1343.
Table IV. Unstable patients
CharacteristicGroup I(n ¼ 14)
Group II(n ¼ 10) P
Time to the OR (min) 84 31 0.001
30-day mortality (%) 85.7 60 0.04

136 Bounoua et al. Annals of Vascular Surgery
6. Previti FW, et al. The ruptured abdominal aortic aneurysm in
a community hospital: a 5 year study. Am Surg 1992;58:
488-501.
7. Basnyat PS, et al. Mortality from ruptured abdominal aortic
aneurysm in Wales. Br J Surg 1999;86:765-770.
8. Dueck DA. Survival after ruptured abdominal aortic aneu-
rysm: effect of patient, surgeon and hospital factors.
J Vasc Surg 2004;39:1253-1260.
9. Han SS, Huang RR. Results of 101 ruptured abdominal aortic
aneurysm repairs from a single surgical practice. Arch Surg
2003;138:898-901.
10. Johansen K, et al. Ruptured abdominal aortic aneurysm:
the Harborview experience. J Vasc Surg 1991;13:
240-247.
11. Pannetan JM, Lassorde J, Laurendeau F. Ruptured abdomi-
nal aortic aneurysm: impact of comorbidity and postopera-
tive complications on outcome. Ann Vasc Surg 1995;9:
535-541.
12. Wakefield TW, Whitehouse WM, Jr, Wu SC, et al. Ab-
dominal aortic aneurysm rupture: statistic of factors af-
fecting outcome of surgical treatment. Surgery 1982;91:
586-596.





























