Embed Size (px)
Citation preview

Routine Coronary Arteriography Before Abdominal Aortic Aneurysm Repair
Murat Bayazit, MD, M. Kamil G51, MD, Bektas Battaloglu, MD, Hilmi Tokmakoglu, MD, Oguz Tasdemir, MD, Kemal Bayazit, MD, Ankara, Turkey
BACKGROUND: AS cardiac complications constb tute the principal cause of early and late morbid- ity and mortality after the surgical treatment of abdominal aortic aneurysm (AAA), a prospective study was planned to evaluate the effects of revascularization of coronary arteries on sur- vival after AAA repair during early and long-term follow-up periods.
PATIENTS AND METHODS: A total of 125 patients un- derwent elective repair of AAA between 1986 and 1994. Coronary arteriography was performed in all cases. All cases with critical left anterior de- scending artery (LAD) lesions underwent a coro- nary artery bypass operation either simultane- ously or shortly before AAA repair. In addition, percutaneous transluminal coronary angioplasty (PTCA) was performed for symptomatic and criti- cal stenosis of arteries other than the LADs, or if noncritical but symptomatic stenosis of the LADs existed. Early and late follow-up data were obtained for all cases, and late-term cumulative survival rates were Calculated.
RESULTS: Coronary artery lesions were found in 66 (53%) cases. In 24 cases, AAA repairs were performed 2.3 (mean) months after coronary artery bypass grafting (CABG), whereas in 4 cases both procedures were performed simulta- neously. PTCA was performed in 4 cases 3 to 4 days prior to the abdominal surgery. Even though the coronary artery lesions were found inoperable in 7 cases, these patients underwent repair of AAA because of rapidly expanding and painful aneurysms, Early mortality rate was 4% (5 cases), in which 3 of these were from the group inoperable for CABG. A mean follow-up of 3.17 years (3 to 87 months) was achieved for all discharged patients. Cumulative survival rates for 6 months and 1, 2, 3, and 6 years were 99%, 99%, 95%, 93%, and 89%, respectively.
CONCLUSIONS: The results of this study empha- size the importance of coronary artery revascu-
From T0rkiye Y0ksek Ihtisas Hastanesi, Cardiovascular Surgery Clinic, Ankara, Turkey.
Requests for reprints should be addressed to Murat Bayazit, MD, TQrkiye Y0ksek Ihtisas Hastanesi, Kalp ve Damar Cerrahisi Klinigi, Sihhiyi 06100, Ankara, Turkey.
Manuscript submitted February 28, 1994 and accepted in re- vised form August 26, 1994.
larization for early, and especially for late, sur- vival after AAA repair. Am J Surg. 1995;170: 246-250.
I n the last 2 decades, surgery for abdominal aortic aneuwsms (AAA) has been performed with reasonably low mortality and morbidity rates. Although technical
improvements offer a safe surgical procedure for patients, cardiac complications constitute the principal cause of mor- bidity and mortality in the early and late postoperative pe- riods, 15 For this reason, cardiovascular assessment is conse- quently an important part of the presurgical evaluation before elective aortic aneurysm repair, but there is a con- tinuing controversy concerning the best methods to evalu- ate the associated cardiac conditions. While some authors suggest routine preoperative coronary angiography, others in- sist on the noninvasive evaluation of the heart with meth- ods such as two-dimensional echocardiography, thallium scanning, or single photon emission Computed tomographi¢ (SPECT) thallium imaging. 6"1°
In the past 8 years, routine coronary angiography has been performed for all the elective cases of AAA in our clinic. This study was planned in !985 for prospective evaluation of this method and the effects of coronary revascularization on long-term survival.
P A T I E N T S A N D M E T H O D S Patient Population
A total of 145 patients with infrarenal or juxtarenal AAA were operated on in our cardiovascular surgery clinic be- tween 1986 and 1994. Of these, 20 repairs of ruptured aneurysms, which were performed on an emergency basis without coronary arteriography, were excluded from the study. The remaining 125 (nonruptured) infrarenal or juxtarenal AAAs were evaluated in a prospective manner. Twenty-one patients (17 %) were women, and the mean age was 64.4 years (standard deviation [SD] 13.2, range 38 to 83). Mean diameter of the abdominal aorta was 5.8 cm (SD 1.3, range 4 to 16). Only 39 of the patients (31%) were symptomatic. The diagnosis was usually suggested by palpa- tion of the pulsatile abdominal mass during a physical ex- amination for routine control or for some other complaint that was not related to AAA. In 114 cases, the diagnosis was made by ultrasonographic examination of the abdomen. In the remaining cases, accurate diagnosis was made using abdominal computerized tomography. At least i operative risk factor was found in 110 of the cases (88%). Patient char- acteristics and concomitant risk factors are listed in Table I. The most frequent operative risk factors were coronary artery disease and hypertension. None of the clinical scoring sys-
246 THE AMERICAN JOURNAL OF SURGERY * VOLUME 170 SEPTEMBER 1995

CORONARY ARTERIOGRAPHY BEFOREAAA REPAIWBAYAZIT ET AL
terns were applied to any of the cases, since they all under- went routine coronary arteriography.
Preoperative Routine Coronary Arteriography Coronary arteriographies and left ventriculographies were
done prior m all elective surgery for AAA. Coronary arte- riography revealed normal coronary arteries in 59 patients (47%). Critical lesions of the left anterior descending artery (LAD) with stenosis >70% narrowing of the lumen was defined as severe coronary artery disease, whether it was accompanied with other vessel diseases or not. Double- or single-vessel disease of the dominant arteries with signifi- cant narrowing lesions, without coexisting critical LAD le- sions, were defined as moderate coronary artery disease. Mild coronary artery disease was defined as noncritical le- sions of all 3 arteries. Lesions of the LAD that were criti- cal (stenosis >70%) were accepted as the only solid indi- cation for coronary artery surgery. Results of the coronary arteriographies are given in Table I!. Although 66 patients had coronary artery lesions, for 35 (53%) of these there was no laboratory, electrocardiographic (ECG), or historic evi- dence of coronary artery disease. ECG evidence of chronic myocardial infarction was present in 18 patients (14%), of which 6 lesions were located inferiorly, 4 were located an- teriorly, and 8 were located anterolaterally. A history of my- ocardial infarction was present only in 14 of the cases with ECG evidence of prior myocardial infarction. History of con- gestive heart failure was present in 3 cases in the inoperable coronary artery disease group and in 1 of the cases with op- erable coronary artery disease.
Four patients who had mild-to-moderate coronary artery lesions underwent percutaneous transluminal coronary an- gioplasty (PTCA). Surgical revascularization of the heart was indicated in 28 patients because of the critical condi- tion of the LAD. In 4 patients who were found to be unfit for elective separate repair because of painful or rapidly ex- panding aneurysms, coronary artery bypass grafting (CABG) and AAA repair were performed simultaneously. In the other 24 patients, the time from CABG to AAA was a mean of 2.3 months. Seven patients who had severe but inoperable coronary artery disease (2- or 3-vessel disease with critical LAD [>70% stenosis] lesion and global ejection fraction of the heart < 15 %) with severely impaired left ventricular func- tion underwent only AAA repair. In the last 2 cases of the inoperable coronary artery disease in patients with poorly functioning ventricles, an intra-aortic balloon was inserted after placement of the abdominal graft. Intra-aortic counter pulsation continued for 72 hours in these 2 cases.
Operative Technique In the perioperative period, all patients underwent radial
artery blood pressure, ECG, pulmonary artery pressure (Swan- Ganz catheter), central venous pressure, and urine output monitoring. This monitoring continued for 48 hours postop- eratively for optimal electrolyte and fluid balance and for other medications. A subumbilical transverse laparotomy in- cision was used. In 112 cases, the proximal aorta was clamped inferior to the renal arteries. An intra-aortic balloon occluder was used in 5 juxtarenal cases. In 8 cases the proximal aorta had robe controlled with suprarenal clamps. Bifurcated wo-
TABLE I Patient Characteristics and Associated Conditions
Number of patients 125 Sex
Male 21 (17%) Female 104 (83%)
Mean age + SD (y) 64.4 _+ 13.2 Range 38-83
Symptomatic AAA 39 (31%) Asymptomatic AAA 86 (69%) Mean aneurysm diameter (cm) 5.8
Range 4-16 Coronary artery disease 66 (53%) Hypertension 63 (50%) Chronic obstructive pulmonary disease 44 (35%) Cerebrovascular disease 5 (4%) Chronic renal failure 15 (12%) Diabetes mellitus 19 (15%) Peripheral vascular disease 22 (18%) Inflammatory AAA 7 (6%) Juxtarenal AAA 13 (10%)
Data reported as number of patients (%) unless otherwise indicated. SD = standard deviation; AAA = abdominal aortic aneurysm,
TABLE II Results of Coronary Arteriographies in Patients With
Abdominal Aortic Aneurysm
No. of Result Cases PTCA CABG
Normal coronary arteries 59 (47%) - - Mild to moderate coronary 31 (25%) 4* -
artery lesions Severe operable coronary 28 (22%) - 28 t
artery lesions Inoperable coronary 7 (6%) - -
artery disease
*procedures were performed 2 or 3 days before surgery for AAA. tin 4 cases CABG was performed simultaneously with AAA repair. In the remaining 24 cases, CABG was perfomed a mean of 2.3 months before AAA repair. PTCA = percutaneous transluminal coronary angioplasty; CABG -: coro- nary artery bypass grafting; AAA = abdominal aortic aneurysm.
ven Dacron (Dupont Dacron, Wilmington, Delaware) grafts and, recently, sealed knitted Dacron grafts were used in 74 (59%) cases, and in 51 cases (41%), tube grafts were used.
Concomitant surgical procedures are shown in Table III. .In the cases of simultaneous CABG and AAA repair, CABG was completed first; after the release of the proximal aortic cross-clamp, the abdominal aorta was clamped and AAA re- pair was performed under cardiopulmonary bypass. After completion of the aneurysm repair, cardiopulmonary bypass was discontinued and the mediastinum was closed before the laparotomy incision was made.
Nephrectomies were performed in 2 patients who had uni- lateral afunctional kidneys and suffered from chronic hyper- tension. In 3 other cases, aortorenal saphenous bypasses were performed. In 3 cases in which the pressure of the inferior mesenteric artery was <30 mm Hg, this artery was reim- planted to the aortic graft. Iatrogenic rupture was the rea- son for splenectomies in 4 cases. Femoropopliteal saphenous
THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 SEPTEMBER 1995 247

CORONARY ARTERIOGRAPHY BEFORE AAA REPAIWBAYAZIT ET A L I
TABLE III Concomitant Operations With
125 Elective Aortic Aneurysm Repairs Procedure No. of Cases Coronary artery bypass 4 Nephrectomy 2 Aortorenal saphenous bypass 3 Reimpiantation of inferior mesenteric artery to graft 3 Femoropopliteal saphenous bypass 2 Cholecystectomy 4 Splenectomy 4 Femoral embolectomy 6 Horseshoe kidney 1 Total 29
TABLE IV Early Postoperative Complications in 125 Elective Aortic Aneurysm Repairs
Complication No. of Cases Lung complications 10 Bleeding 4 Early graft occlusion 3 Hemodialysis 3 Extrasystole (minor) 3 Infection at incision site 1 Ischemic colon 1 Hematuria 1
bypasses were performed in 2 cases, because of hemody- namically significant femoral artery lesions. An experienced urologist was consulted for 1 patient with horseshoe kidney. The hilus and the isthmus of the kidney were dissected first, and then AAA repair was performed.
R E S U L T S Early and late postoperative follow-up data were obtained
for all patients. Early mortality rate (including the first 30 postoperative days) was 4% with 5 deaths. Of these 5 cases, 3 were classified inoperable for CABG. One of these deaths was due to excessive postoperative bleeding. Two other pa- tients died of cardiac events (myocardial infarction and in- tractable ventricular fibrillation). Of the patients who were operated on for coronary artery lesions and AAA simultane- ously, 2 died because of low cardiac output and congestive heart failure. The last 2 cases in the inoperable coronary artery disease group, who had intra-aortic balloons placed, survived the operation and had art uneventful postoperative period, A logistic or linear regression analysis for early postoperative death with preoperative risk factors was not done because early postoperative deaths had cardiac reasons in 4 of 5 cases, and all patients had severe coronary artery lesions that either needed coronary artery surgery or were inoperable for CABG.
Excluding the 5 deaths, there was no form of perioperative myocardial ischemia or major arrhythmia. Hemodialysis had to be performed in the early postoperative period 4 to 5 times in 3 patients who had chronic renal failure and preoperative blood creatinine levels >2 mg/dL. In 8 patients who had mild renal failure preoperatively, renal functions returned to nor- mal in the early postoperative period. Three patients who had compensated chronic renal failure preoperatively were
120
100'
8 o
,~ 60
"~ 40,
20'
0
100 99 99 " ~ 9 3 93 93
- - - - - . . ~ 8 9 89
I I I I I I I I I
0,1 ~ ,,~ tO ~ I ~. ¢O
Fo l low-Up T i m e
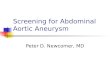
Figure. Cumulative long-term survival rates for 120 patients who underwent elective repair of an abdominal aortic aneurysm between 1986 and 1994 and survived at least 1 month after surgery (5 patients died within 1 month of surgery), Coronary arteriography was performed in all cases,
discharged with the same renal status. Early postoperative morbidity is shown in Table IV. C01onoscopy had to be per- formed on the 45th day after surgery in 1 case because of continuing diarrhea. Mucosal ischemia was found and left hemicolectomy was performed.
Late follow-up data were obtained in all of those who sur- vived the hospitalization period. The mean follow-up period was 3.17 years (1.23 y/patient, 3 to 87 months). During this
follow-up, 6 patients died (at 6, 13, 21, 22, 34, and 63 months after surgery). Two of the patients died in other medical cen- ters from cerebrovascular events. Three late deaths, reported as "sudden" by the patient's families, occurred outside the hos- pital and were accepted as cardiac deaths. The patient who died 13 months after surgery had received CABG. The re- maining patient died 34 months after surgery because of a lung malignancy that was diagnosed 9 months postopera- tively. Cumulative long-term survival rates are presented in the Figure.
C O M M E N T S In the 1970s, an understanding of the pathophysiology of
declamping shock encouraged the use of invasive monitor- ing of postoperative fluid administration, ira3 which in turn decreased the mortality of AAA repair to rates below 6%. Many investigators proved that myocardial infarction was the main contributing factor in this mortality figure. 15 In the 1980s, many noninvasive methods were investigated and some clinical scoring systems were developed for further eval- uation and early detection of cardiac risk factors. However, when the patient group under evaluation is known to have a high prevalence of underlying apparent or silent coronary artery disease, such as patients undergoing abdominal aorta repair or peripheral vascular surgery, a very low-risk group cannot be identified by clinical markers alone. 14'15 Unfortun- ately, these clinical scoring systems did not help very much
248 THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 SEPTEMBER 1995

CORONARY ARTERIOGRAPHY BEFORE AAA REPAIR/BAYAZIT ET AL
in predicting the cardiac death risk after A A A repair, and these scores of cardiac status did not correlate with the inci- dence of perioperative cardiac events. 16"22
The use of dipyridamole-thallium tests has gained wide- spread acceptance. False-positive results and the lower-than- expected sensitivity still present major problems with this test. In a recent study, angina and the presence of fixed thal- lium defects after exercise were independent predictors of
cardiac risk in patients undergoing elective surgery. 1° Two-dimensional echocardiography did not have any value
beyond suggesting ischemic myocardium and was not a re- liable predictor of forthcoming cardiac events. Although this imaging can provide some information on functional cardiac status, it cannot predict myocardial behavior on exposure to a physical burden such as cross-clamping of the aorta.
It has been demonstrated that coronary artery revascular- ization lowers the risk of acute cardiac events in panents with coronary artery disease undergoing separate major sur- gical procedures. 23'24 For patients with coronary artery dis- ease and AAA, two different approaches were adopted in the past. The most common course was for myocardial revas- cularization to be undertaken first, followed at a later date by elective A A A repair. This was our approach for patients who can be satisfactorily revascularized and who have rea- sonably good left ventricular function. Alternatively, some clinicians adopted a one-stage procedure consisting of my- ocardial revascularization followed by discontinuation of car- diopulmonary bypass, and then aneurysm repair, during the same operation. 24 In cases with coronary artery disease, cross- clamping the aorta causes elevation of left atrial pressure and subendocardial ischemia. Cardiac output is maintained at the expense of increased filling pressures. Increased filling pressures must be countered with peripheral vasodilators, and the benefit may be the reversal of subendocardial ischemia. This brings us to the idea of performing the abdominal aor- tic repair under cardiopulmonary bypass, after coronary artery revascularization--an idea which is also supported by the works of Westaby et a125 in a recently published report.
A thorough review of the literature on A A A reveals that coronary artery disease is the leading cause of early and late mortality. Although early mortatily rates do not differ among the centers that perform routine or selective coronary arteri- ography, there is a consensus that coronary artery revascu- larization should be performed if extensive myocardial is- chemia is demonstrated and the anatomic findings suggest that revascularization may prolong survival. 1'15'26 The only way to show the degree of myocardial ischemia and accurate anatomic findings is by coronary arteriography. This is an ex- pensive, invasive test that requires patient hospitalization in many centers. However, it could be performed with very low mortality and morbidity with only overnight hospitalization of the patient, including time spent in the cardiology clinic (in our hospital). Long-term life expectancy is the most valu- able thing exceeding the offset of cost. Even though some physicians remain unconvinced that coronary artery revas- cularization will improve long-term survival, we believe that it is justifiable, since the prophylactic coronary artery revas- cularization tested in this prospective study was found to be beneficial. Because coronary arteriography is the only way to detect silent ischemic myocardium, we recommend that rou-
tine coronary arterial screening be done with the so-called invasive method of coronary arteriography, and that patients with extensive ischemia should undergo coronary artery revascularization prior to abdominal aortic surgery.
In conclusion, it was shown in our series that coronary artery revascularization may extend long-term survival after surgical repair of abdominal aortic aneurysms, and that coro- nary artery disease could most accurately be diagnosed with coronary angiography.
The conundrum of which critical degenerative vascular lesion comes first continues to plague clinical surgeons. The regular use of coronary arteriography prior to abdominal aneurysm replace. ment allowed this surNcal group to achieve creditable results and provide both short- and long-term follow-up data that will help many of us with a frequent and disconcerting judgment call.
REFERENCES 1. Golden MA, Whittemore AD, Donaldson MC, Mannick JA. Selective evaluation and management of coronary artery disease in patients undergoing repair of abdominal aortic aneurysms: a 16 year experience. Ann Surg. 1990;212:415-420. 2. Whittemore AD, Clowes AW, Hechtman H, Mannick JA. Aortic aneurysm repair. Ann Surg. 1980;192:414-421. 3. Young AE, Sanberg GW, Couch NP. The reduction of mortality of abdominal aortic aneurysm resection. Am J Surg. 1977;134:585-590. 4. Volpetti G, Barker CF, Berkowitz HD, Roberts B. A twenty-two year review of elective resection of abdominal aortic aneurysms. Surg Gynecol Obstet. 1976;142:321-324. 5. Crawford ES, Palamara AE, Saleh SA, Roehm JOE Aortic aneurysm: current status of surgical treatment. Surg Clin North Am. 1979;59:597~536. 6. Boucher CA, Brewster DC, Darling RC, et al. Determination of cardiac risk by dipyridamole-thallium imaging before peripheral vas- cular surgery. NEJM. 1985;312:389-394. 7. Brewster DC, Okada RD, Strauss W, et al. Selection of patients for preoperative coronary angiography, use of dipyridamole-stress-thallium myocardial imaging. J Vasc Surg. 1985;2:504-5 i0. 8. McEnroe CS, O'Donnell TFJr, Yeager A, et al. Comparison of ejec- tion fraction and Goldman risk factor analysis to dipyridamole-thal- lium 201 studies in the evaluation of cardiac morbidity after aortic aneurysm surgery. J Vasc Surg. 1990;11:497404. 9. Chae SC, Heo J, Iskandrian AS, et al. Identification of extensive coronary artery disease in women by exercise single photon emission computed tomographic (SPECT) thallium imaging. J Am Coll Cardiol. 1993;21:1305-1311. 10. McFalls EO, Doliszny K, Grund F, et al. Angina and persistent ex- ercise thallium defects: Independent risk factors In elective vascular surgery. J Am Coll Cardiol. 1993;21:1347-1352. 1 I. Cohn LH, Powell MR, Seidlitz L, et al. Fluid requirements and shifts after reconstruction of the aorta. AmJ Surg. 1970;120:182-186. 12. Grindlinger GA, Vegas AM, Manny J, et al. Volume loading and vasodilators in abdominal aortic aneurysmectomy. Am J Surg. 1980; 139:480-486. 13. Bush HL, LoGeffo FW, Weisel RD, et al. Assessment of myocar- dial performances and optimal volume loading during elective ab- dominal aortic resection. Arch Surg. 1977;112:1301-1305. 14. Wong T, Detsky AS. Perioperative cardiac risk assessment for pa- tients having peripheral vascular surgery. Ann Intern Med. 1992;116: 743-753. 15. Massie BM, Mangano DT. Assessment of perioperative risk: have we put the cart before the horse? J Am Coll Cardiol. 1993;21: 1353-1356. Editorial comment. 16. Lette FJ, Waters D, Lassande J, et al. Postoperative myocardial in- farction and cardiac death. Ann Surg. 1990;211:84-90.
THE AMERICAN JOURNAL OF SURGERY ® vOLUME 170 SEPTEMBER 1995 249

CORONARY ARTERIOGRAPHY BEFORE AAA REPAIR/BAYAZIT ET AL ]
17. Goldraan L, Caldera DL, Nussman SR, et al. Multifactorial index of cardiac risk in non-cardiac surgical procedures. NEJM. 1977;297: 845-850. 18. Cooperman M, Pflug B, Martin EW Jr., Evans WE. Cardiovascular risk factors in patients with peripheral vascular disease. Surgery. 1978; 84:505-509. 19. Drips RD, Lamont A, Eckm~hoff JE. The role of anesthesia in sur- gical mortality. JAMA. 1961;178:261-266. 20. Detsky AS, Abrams HB, Forbath N, et al. Cardiac assessment of patients undergoing noncardiac surgery: a multifactorial risk index. Arch Intern Med. 1986;146:2131-2134. 21. Eagle KA, Singer DE, Brewster DC, et at. Dipyridamole-thallium scanning in patients undergoing vascular surgery. JAMA. 1987;257: 2185-2189.
22. McPhail N, Calvin JE, Shariatmadar A, et al. The use of preop- erative exercise testing to predict cardiac complications after arterial reconstruction. J Vasc Surg. 1988;7:60-68. 23. McCann RL, Wolfe WG. Resection of abdominal aortic aneurysra in patients with low ejection fractions. J Vasc Surg. 1989;10:240-244. 24. Reul GJ Jr, Cooley DA, Duncan JM, et al. The effect of coronary bypass on the outcome of peripheral vascular operations in 1093 pa- tients. J Vaac Surg. 1986;3~788-798. 25. Westaby S, Parry A, Grebenik CR, et al. Combined cardiac and abdominal aortic aneurysm operations: the dual operation on car- diopulmonary bypass. Thorac Cardiovasc Surg. 1992;104:990-995. 26. Gouny P, Bertrans M, Coriat P, Kieffer E. Perioperative cardiac complications of surgical repair or inftarenal aortic aneurysms. Ann Vasc Surg. 1989;3:328-334.
250 THE AMERICAN JOURNAL OF SURGERY ® VOLUME 170 SEPTEMBER 1995