Embed Size (px)
Citation preview

Clin Plastic Surg 31 (2004) 33–38
Role of radiation therapy for facial skin cancers
Sujay A. Vora, MDa,*, Steven L. Garner, MD, FACSb,c
aDepartment of Radiation Oncology, Mayo Clinic Scottsdale, 13400 E. Shea Blvd., Scottsdale, AZ 85259, USAbDivision of Plastic and Reconstructive Surgery, Stanford University School of Medicine, 300 Pasteur Drive,
Stanford, CA 94305, USAcPrivate Practice, Santa Cruz, CA 95065, USA
There are a number of treatment options for Fractionation is an important radiobiologic prin-
patients who develop skin cancers of the head and
neck, including traditional surgical excision, Mohs’
surgery, cryosurgery, curettage/electrodesiccation, and
radiation therapy. For early lesions, each offers excel-
lent cure rates. Over the past 20 years, radiation
therapy has been used with less frequency, primarily
due to the high control rates reported with Mohs’
surgery, advances in plastic surgery, and physician
preference. Advances in radiation therapy also may
be unknown to physicians in surgical fields. Nonethe-
less, in appropriately selected patients, radiation ther-
apy is a curative option that provides rates of success
similar to those of other treatment options. This article
reviews the radiobiologic principles, radiotherapeutic
techniques, and clinical management of nonmelanoma
skin carcinomas.
Radiobiology
Radiation is a high-energy x-ray that causes cell
death by direct and indirect effects (via formed oxy-
gen-free radicals) on DNA. Due to differences in
cancer and normal tissue tolerances of radiation, can-
cer cells die and normal cells repair from the effects of
radiation. Damage to cancer cells also is dependent on
oxygen status of the tumor, daily radiation dosage
(fraction size), and total dose.
0094-1298/04/$ – see front matter D 2004 Elsevier Inc. All right
doi:10.1016/S0094-1298(03)00119-6
* Corresponding author.
E-mail address: [email protected] (S.A. Vora).
ciple. It was discovered during experiments on ram tes-
ticles in the 1920s. These experiments showed that
rams could not be sterilized with a single dose of ra-
diationwithout excessive skin damage.However, if the
radiation was given in smaller doses over a period of
time, sterilization was possible without skin damage.
The earliest developments of time/dose/fractiona-
tion schedules were derived empirically. Initial
schemes were based on work in 1963 from Von Essen
[1], who examined control rates versus incidence of
skin necrosis. The regimens devised are similar to ones
used today (Tables 1 and 2). Using longer fractiona-
tion schedules, the incidence of serious complications
and poor cosmetic results has decreased markedly.
Radiotherapeutic techniques
Most early lesions are treated with orthovoltage
machines (100–250 kVp) or with linear accelerators
(6–12 MeVelectrons). It is important for the radiation
oncologist to understand the beam characteristics—
particularly the surface dose, radial dose, and depth
dose. The radiation beam can be modified easily by
adjusting the energy of the beam or the size of the
radiation field, and with the use of bolus material that
can mimic skin. Shielding using materials such as
gold, lead, or tungsten is important in the protection
of nearby radiosensitive normal structures such as the
eye or lacrimal gland. Brachytherapy is a less com-
monly used technique that places radiation sources
directly into tumor using catheters that are afterloaded
with radiation sources such as iridium 192. The tumor
s reserved.

Table 1
Time, dose, surface area table for 99% probability of tumor cure
1 cm2 3 cm2 10 cm2 20 cm2 30 cm2 100 cm2
1 treatment (1 d) 2470 2680 2940 3100 3190 3500
2 txs (2 d) 2810 3050 3340 3520 3630 3990
5 txs (5 d) 3310 3600 3940 4150 4280 4670
10 txs (2 wk) 3730 4060 4440 4670 4820 5270
15 txs (3 wk) 3960 4310 4710 4960 5120 5610
20 txs (4 wk) 4130 4480 4910 5160 5330 5830
25 txs (5 wk) 4250 4620 5050 5320 5490 6000
30 txs (6 wk) 4350 4730 5170 5450 5610 6150
Dosages are given in cGy.
Abbreviation: txs, treatments.
Modified from Von Essen CF. A spatial model of time-dose-area relationships in radiation therapy. Radiology 1963;81:881–3.
S.A. Vora, S.L. Garner / Clin Plastic Surg 31 (2004) 33–3834
sites that generally are believed to be suitable are the
lip, lip commissure, and nasal vestibule.
Clinical management
There are many options to treat skin cancers. The
counseling physician should review all treatment
options with the patient along with reasons for his or
her final recommendation. The selection of treatment
modalities is based on a number of selection factors.
There are tumor-related factors such as size, location,
growth pattern, and histology; and patient-related
factors such as patient’s age, medical status, personal
preference, time involved, and cost. In addition, clini-
cian’s preference and referral patterns contribute to
the final recommendation. However, patients with
advanced disease (T4 or involved nodes) require a
combined modality approach.
Primary radiotherapy is an option in the treatment
of most patients with squamous cell carcinomas or
Table 2
Time, dose, surface area table for 3% probability of late skin necr
1 cm2 3 cm2 10 c
1 treatment (1 d) 2860 2400 198
2 txs (2 d) 3750 3150 260
5 txs (5 d) 5380 4520 372
10 txs (2 wk) 7010 5880 485
15 txs (3 wk) 7960 6680 551
20 txs (4 wk) 8180 7270 600
25 txs (5 wk) 8670 7750 640
30 txs (6 wk) 9090 8170 674
Dosages are given in cGy.
Abbreviation: txs, treatments.
Modified from Von Essen CF. A spatial model of time-dose-area re
basal cell carcinomas of the head and neck. Acute ef-
fects during the course of radiation include erythema,
dry desquamation, hyperpigmentation, moist desqua-
mation, and epilation [2]. The degree of reaction
depends on variables such as size of area treated, total
dose, daily dosage, length of treatment course, degree
of patient pigmentation, and medical comorbidity.
Chronic or late effects from radiation include epider-
mal atrophy, telangiectasias, hairless and dry skin,
subcutaneous fibrosis, and hyperpigmentation [2].
Treatment lengths can vary between less than 1 week
to 5 to 7 weeks depending on the size and location of
the tumor and the importance of good cosmetic out-
come. Generally, higher daily dosages will yield more
deleterious effects on the normal tissues, resulting in
an inferior cosmetic outcome.
Advantages to radiation include high rates of local
control; the preservation of adjacent normal tissue; and
the ability to treat areas where it would be difficult to
obtain clear margins without functional or cosmetic
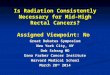
loss, including the nose, lips, eyelids, and ear. Tumors
involving the embryonic fusion planes (H-zone, Fig. 1)
osis
m2 20 cm2 30 cm2 100 cm2
0 1920 1770 1370
0 2320 2180 1800
0 3340 3130 2580
0 4330 4070 3360
0 4930 4610 3820
0 5370 5030 4160
0 5730 5370 4430
0 6030 5640 4670
lationships in radiation therapy. Radiology 1963;81:881–3.

Fig. 1. H-zone of face. Tumors in the shaded area have the
potential for deeper invasion and further radial spread.
S.A. Vora, S.L. Garner / Clin Plastic Surg 31 (2004) 33–38 35
can be treated with wide margins. Wide margins are
necessary because tumors in this location can be more
deeply infiltrative than they appear at the surface.
Radiation is an outpatient procedure that does not
require anesthesia, and may maintain normal tissue
contours better than do surgical techniques. One mis-
conception about radiation is that the cartilage of the
nose and ear tolerates radiation poorly. This miscon-
ception was based on old data that used large fraction
sizes and old technology [3]. The incidence of chon-
droradionecrosis in contemporary radiation practices
is extremely low.
Disadvantages of radiation include some risk of
late-tissue effects of atrophy, pallor, and telangiecta-
sias that can develop months to years after radiation.
This may translate to a loss of cosmetic result. Silver-
man et al [4,5] and Rowe et al [6] studied cosmetic
outcome of basal cell cancer patients 15 years after
radiotherapy/surgery. Between the first and fifteenth
years of follow-up, the percentage of radiation patients
who had either an excellent or good cosmetic result
declined by 20%. This decline was not seen in the
Table 3
Tumor control by size, histology, and presentation
Size Basal cell untreated Basal cell recurrent
<1 cm 64/66 (97%) 22/23 (96%)
1.1–3 cm 71/75 (95%) 27/36 (75%)
3.1–5cm 11/13 (85%) 7/9 (78%)
>5 cm 12/13 (92%) 1/2 (50%)
Not specified 4/4 (100)% 1/1 (100%)
Total 162/171 (95%) 58/71 (82%)
From Lovett RD, et al. External irradiation of epithelial skin
with permission.
surgical patients [4,5]. Therefore, young patients may
find the treatment option of radiation less desirable
than surgery. However, with the use of lower fraction
sizes, these risks of adverse late effects may not
be seen.
Additional disadvantages of radiation include the
inability to examine microscopic margins of tumor to
ensure complete inclusion within the radiation vol-
ume, the potential risk of radiation-induced malig-
nancies (extremely rare event), and the potential to
increase future surgical complication risks if radia-
tion is unsuccessful.
Outcome data
Most of the available data on results of radiation are
based on retrospective studies. Rowe et al [6] reported
long-term recurrence rates in previously untreated
carcinoma (Table 3). Radiation therapy had results
that were similar to those of other non-Mohs’ modali-
ties. Mohs’ surgery had the lowest recurrence rate
(Table 4). Control rates by site are as follows:
Eyelid: High local control rates have been reported
by Royal Marsden Hospital, Princess Margaret
Hospital, Institut Curie, and Massachusetts
General Hospital with local control rates
between 93% and 97% [7,8]. No apparent
differences were seen in squamous cell car-
cinomas versus basal cell carcinomas. Com-
plications included extropion, epiphora, and
conjunctival keratinization.
Nose/ears: High local control rates (91%–97%)
with negligible rates of necrosis have been
reported by a number of institutions [8,9].
The only prospective randomized trial was pub-
lished by Avril et al [10] in 1997. Three hundred and
forty-seven patients with basal cell carcinomas less
Squamous cell untreated Squamous cell recurrent
11/11 (100%) 10/12 (83%)
19/21 (90%) 7/13 (54%)
7/8 (88%) 6/9 (67%)
3/5 (60%) 6/11 (55%)
0/1 (0%) 4/6 (67%)
40/46 (87%) 33/51 (65%)
cancer. Int J Radiat Oncol Biol Phys 1990;19:235–42;

Table 4
Overall outcome data by modality
Recurrence rates
Treatment
modality
Short term
(<5 y)
Long term
(5 y)
Surgical excision 2.8% (157/5560) 10.1% (264/2606)
Curettage/
electrodesiccation
4.7% (173/3664) 7.7% (274/3573)
Radiation therapy 5.3% (318/6072) 8.7% (410/4695)
Cryotherapy 3.7% (90/2462) 7.5% (20/269)
All non-Mohs’ 4.2% (738/17,758) 8.7% (968/11,143)
Mohs’ surgery 1.4% (5/367) 1.0% (73/7670)
Data from Rowe DE, et al. Long-term recurrence rates in
previously untreated carcinoma: implications for patient
follow-up. J Dermatol Surg Oncol 1989;15:315–28.
S.A. Vora, S.L. Garner / Clin Plastic Surg 31 (2004) 33–3836
than 4 cm in size were randomized to radiation therapy
(brachytherapy, contact, or superficial external beam
radiotherapy) or surgical excision (non-Mohs’). At
4 years, the local recurrence rate was 0.7% for surgery
and 7.5% for radiation. Cosmetic result was rated as
‘‘good’’ in 87% surgical patients and 69% of radiation
Fig. 2. (A) An 83-year-old with keratinizing squamous cell carcino
over 4 weeks. (B, C) One-year follow-up photos.
patients. The authors concluded that surgery was
preferred over radiation [10]. There are some concerns,
however, about the variable techniques used in the
radiation arm and the extremely low failure rate seen in
the surgical arm.
One of the larger retrospective reviews of radia-
tion patients was by Lovett et al [11]. They reviewed
339 patients (242 basal cell carcinoma, 97 squamous
cell carcinoma). Their results for both untreated and
recurrent basal cell and squamous cell carcinomas are
shown in Table 3. Control rates were related to tumor
size. Cosmesis was rated based on the amount of
telangectasia, pigmentation change, and skin fibrosis.
Patients were rated ‘‘good to excellent’’ in 92% of
patients. Cosmesis had an inverse relationship to the
primary lesion size, and 5.5% of patients had a
complication that was related to tumor size. Compli-
cations included soft tissue necrosis, bone necrosis,
and cataracts [11].
There are limited data on radiation results for
locally advanced T4 lesions. Lee et al [12] reported
a 67% local control rate on patients previously un-
ma of skin. Using 12 MeV electrons, he received 5000 cGy

S.A. Vora, S.L. Garner / Clin Plastic Surg 31 (2004) 33–38 37
treated and a 41% local control rate for patients with
recurrent disease. When surgery as salvage was added,
the 5-year local control rates were 90% (untreated) and
59% (recurrent). Poor risk factors in this group of
patients included lesions with bone or nerve involve-
ment. Thus, in this group of patients, a combined
approach of surgery and radiation is preferred.
Postoperative radiation therapy
General indications for postoperative radiation
include perineural invasion, lymph node metastasis,
nodal extracapsular extension, positive margins in
patients with squamous cell carcinomas, selected basal
cell carcinoma patients with positive margins, and
selected patients with recurrent skin carcinoma. It is
critical to emphasize that patients with advanced
disease that requires combined modality therapy are
very different than patients who require primary treat-
ment with respect to overall control and complication
rates. When radiation is delivered to an area that has
been surgically managed, there is an increased risk for
wound/flap breakdown and poor healing. However,
in the advanced cases, if radiation is not given, the
risk of tumor relapse or progression is high. The
patient should be counseled with respect to these risks
and benefits.
Perineural invasion is seen more often in squamous
cell carcinomas and recurrent cases than in de novo
basal cell carcinomas. Surgical resection including
nerve generally is combined with postoperative radia-
tion therapy. Radiation fields include the nerve path-
way to the ganglion. Doses vary between 50 and
64 Gy. Even with aggressive surgery and radiation, re-
currence rates still can be as high as 50% [13].
Involvement of two or more lymph nodes or extra-
capsular extension of tumor is an indication for radia-
tion therapy. In these cases, doses vary between 50 and
64 Gy
Postoperative radiation therapy also is recom-
mended for patients with incomplete excision of squa-
mous cell carcinomas in whom re-excision is ill
advised or refused. A recurrence could predispose
the patient to lymph node metastasis and systemic re-
lapse that could be difficult to salvage. Thus, we prefer
to treat these patients once adequate healing of the
primary excision has occurred.
In patients with basal cell carcinomas, it is less clear
who needs immediate postoperative radiation therapy
versus close observation [14]. The relapse rate is
higher without radiation therapy versus immediate
postoperative radiation. However, overall control rates
appear to be identical when salvage treatment with
radiation is included. Thus, if a compliant patient is
willing to have close follow-up in an area that is not
functionally or cosmetically sensitive, observation is a
reasonable option.
Summary
Radiation therapy is one of many modalities that
should be considered and explained to patients with
basal cell carcinomas and squamous cell carcinomas of
the head and neck (Fig. 2). Control rates for appropri-
ately selected patients should exceed 90% and histor-
ically are comparable with most surgical resections.
For locally advanced T4 lesions, a combined modality
approach will give the best chance at local control.
Postoperative radiation therapy is indicated in patients
with advanced lesions, positive margins, lymph node
metastasis, or perineural invasion. We advocate the
discussion of this treatment modality with every such
patient, even if the treating physician does not recom-
mend it. Only then can a patient provide genuine
‘‘informed consent’’ for treatment.
References
[1] VonEssenCF.Aspatialmodelof time-dose-arearelation-
ships in radiation therapy. Radiology 1963;81:881–3.
[2] Aerchambeau JO, et al. Pathophysiology of irradiated
skin and breast. Int J Radiat Oncol Biol Phys 1995;31:
1171–85.
[3] Traenkle H, Mulay D. Further observations on late ra-
diation necrosis following therapy of skin cancer. Arch
Dermatol 1960;81:908–13.
[4] Silverman M, Kopf A, Grin C, Bart R, Levenstein M.
Recurrence rates of treated basal cell carcinomas. Part 1:
overview. J Dermatol Surg Oncol 1991;17:713–8.
[5] Silverman M, Kopf A, Grin C, Bart R, Levenstein M.
Recurrence rates of treated basal cell carcinomas. Part 4:
x-ray therapy. J Dermatol Surg Oncol 1992;18:549–54.
[6] Rowe DE, Carroll RJ, Day Jr CL. Long-term recurrence
rates in previously untreated carcinoma: implications
for patient follow-up. J Dermatol Surg Oncol 1989;15:
315–28.
[7] Fitzpatrick P, et al. Basal and squamous cell carcinoma
of the eyelids and their treatment by radiotherapy. Int J
Radiat Oncol Biol Phys 1984;10:449–54.
[8] Morrison W, Garden AS, Ang KK. Radiation therapy
for nonmelanoma skin carcinomas. Clin Plast Surg
1997;24(4):719–29.
[9] Mazeron J, et al. Radiation therapy of carcinomas of the
skin of nose and nasal vestibule: a report of 1676 cases
by the Groupe Europeen de Curietherapie. Radiother
Oncol 1989;13:165–73.

S.A. Vora, S.L. Garner / Clin Plastic Surg 31 (2004) 33–3838
[10] Avril MF, Auperin A, Margulis A, Gerbaulet A, Duvil-
lard P, Benhamou E, et al. Basal cell carcinoma of the
face: surgery or radiotherapy? Results of a randomized
study. Br J Cancer 1997;76(1):100–6.
[11] Lovett RD, et al. External irradiation of epithelial
skin cancer. Int J Radiat Oncol Biol Phys 1990;19:
235–42.
[12] Lee W, et al. Radical radiotherapy for T4 carcinoma of
the skin of the head and neck: a multivariate analysis.
Head Neck 1993;15:320–4.
[13] Mendenhall W, et al. Carcinoma of the skin of the head
and neck with perineural invasion. Head Neck 1989;
11:301–8.
[14] Pascal RP, et al. Prognosis of ‘‘incompletely excised’’
versus ‘‘completely excised’’ basal cell carcinoma. Plast
Reconstr Surg 1968;41:328.