Embed Size (px)
Citation preview

Role of Helicobacter pylori Gastritis in Gastric Atrophy,Intestinal Metaplasia, and Gastric NeoplasiaVINCENT C. SMITH1 AND ROBERT M. GENTA1–3*1Department of Pathology, Veterans Affairs Medical Center and Baylor College of Medicine, Houston, Texas 770302Department of Medicine, Veterans Affairs Medical Center and Baylor College of Medicine, Houston, Texas 770303Department of Microbiology and Immunology, Veterans Affairs Medical Center and Baylor College of Medicine,Houston, Texas 77030
ABSTRACT Helicobacter pylori is the major cause of chronic gastritis worldwide. With an esti-mated rate of infection of over one half of the world’s population, it is responsible for extensive morbidityand mortality. Infection with this organism does not appear to spontaneously resolve. Instead it reachesa chronic stage from which a number of outcomes are possible. This article reviews those outcomes thathave been linked to H. pylori and explores the pathogenesis while attempting to resolve the discrepantpaths infection can take. The associations include duodenal and gastric ulcers and the majority ofgastric lymphomas of B-cell type derived from the mucosa-associated lymphoid tissue (MALT). Chronicgastritis has also been shown to evolve into atrophy with intestinal metaplasia in certain populations.This change in the gastric epithelium has been linked with an increased risk of gastric adenocarci-noma. Microsc. Res. Tech. 48:313–320, 2000. Published 2000 Wiley-Liss, Inc.†
INTRODUCTIONHelicobacter pylori is a species of bacteria that was
first linked to gastric disease more than a decade ago(Marshall et al., 1985). Prior to its discovery, stress anddiet were considered to be the main etiologies of pepticulcer disease. The initial publications by Warren andMarshall stimulated an unprecedented worldwide de-bate on the significance of this newly rediscovered gas-tric infection. While several prominent gastroenterol-ogists and microbiologists expressed opinions so force-ful and widely divergent that at times they appearedtinged by an almost religious fervor, others tackled theissue with scientific rigor and set up studies designedto confirm or refute the hypothesis put forward byWarren and Marshall. Within less than a decade it wasdemonstrated that H. pylori was the main cause ofchronic gastritis worldwide, with more than half of theworld population infected. A number of conditions pre-viously associated with chronic gastritis were then rec-ognized to be ultimately related to H. pylori infection,including virtually all cases of duodenal ulcers and themajority of gastric ulcers, gastric cancer, and, morerecently, primary gastric B-cell lymphomas arisingfrom mucosa-associated lymphoid tissue (Correa, 1995;Isaacson, 1994a; Marshall, 1995).
EPIDEMIOLOGYAs mentioned above, H. pylori infection is highly
prevalent worldwide (Pisani et al., 1997). Some devel-oping countries have rates of infection approaching90%, while in industrialized nations of Western Eu-rope, North America, and Oceania the infection ratesmay be as low as 30% (Bergenzaun et al., 1996; Hol-combe et al., 1992; Mitchell et al., 1992; Queiroz et al.,1991). In these countries, the prevalence of H. pylori incertain groups of non-underpriviledged children are aslow as 1%. Several studies have shown a link betweensocioeconomic status to explain the differences in theprevalence of infection in different groups within the
same geographical region (Anonymous,1993; Grahamet al., 1991). As sanitary conditions improve in a coun-try, rates of infection have been shown to decline.Other demographic factors include sex, with slightlyhigher rates of infection in males (Replogle et al.,1995), and possible genetic roles, which have been ex-plored in twin studies (Malaty et al., 1994).
These infection rates represent approximately 3 bil-lion people currently harboring H. pylori, but they donot reflect the level of morbidity and mortality result-ing from this infection. Most individuals remainasymptomatic throughout their life, although biopsystudies have revealed that histological evidence of gas-tritis is present in virtually every infected subject, ir-respective of the presence or absence of symptoms(Dooley et al., 1989). H. pylori has been linked to mostcases of peptic ulcers, which include both gastric andduodenal ulcers. Serologic studies attribute at least300,000 cases of gastric adenocarcinoma per year to theorganism (Forman, 1995). Gastric adenocarcinoma, adisease with a high mortality, represents the mostnefarious outcome of infection. The 300,000 cases peryear represent approximately one third of the worlds’total. Although it is clear from these figures that only asmall percentage of those infected will develop gastriccancer as a consequence of having H. pylori, one mustconsider that gastric adenocarcinoma still remains thesecond leading cause of cancer death worldwide. Theglobal eradication of H. pylori, advocated by some,might contribute to a considerable decline in the inci-dence of this tumor (Pisani et al., 1997). Other out-comes, such as peptic ulcers, are much more common.With a lifetime incidence of 2–5%, several hundredmillion people will suffer from ulcer disease. The mor-
*Correspondence to: Robert M. Genta, M.D., Pathology 113, VAMC, 2002Holcombe Blvd., Houston, TX 77030.
E-mail: [email protected] 30 March 1999; accepted in revised form 9 September 1999
MICROSCOPY RESEARCH AND TECHNIQUE 48:313–320 (2000)
Published 2000 WILEY-LISS, INC. †This article is a USGovernment work and, as such, is in the public domain in theUnited States of America.

tality rate is much lower than that of gastric adenocar-cinoma, but with a much higher prevalence, approxi-mately 200,000 people per year will die of complica-tions related to gastro-duodenal ulcers (Parsonnet,1998). These two examples of H. pylori-associated dis-eases illustrate the worldwide scale of the problemsassociated with this organism. The etiological role nowattributed to H. pylori in the causation of these condi-tion may become better defined as continuing ongoingstudies reveal an even stronger link to these and per-haps other outcomes. Also, these figures do not reflectthe impact of other associations, including a possiblelink to common dyspepsia (Talley, 1996; Veldhuyzen,1997) and a proven role in the more rare, yet eminentlypreventable and curable, primary gastric lymphomas(Wotherspoon et al., 1993).
Normal Gastric MucosaInfection with H. pylori causes characteristic
changes in the gastric epithelium. To appreciate thesechanges a good understanding of the normal gastrichistology is necessary (Owen, 1986). The stomach con-tains two major types of epithelial lining. The antralmucosa and the mucosa of the cardia consist almostexclusively of mucus-secreting cells lining both surfaceand glands. Glands open to the surface through pits (orfovoeolae), which in these locations occupy approxi-mately one half of the mucosa thickness. The acid-secreting mucosa of the corpus (also called oxyntic mu-cosa and, particularly in North America, fundic mu-cosa) contains the same mucus cells lining the surface,but differs in its glandular structure. Here the glands,termed oxyntic, are tightly packed, tubular, and linedby parietal and chief cells along with the mucus cells.The pits occupy less than one third of the thickness ofthe oxyntic mucosa. Within the lamina propria of thenormal gastric mucosa of either type, only a few scat-tered lymphocytes and plasma cells reside, and no lym-phoid follicles are present (Genta et al., 1993). A smallamount of extra-cellular matrix separates the antraland cardiac mucous glands from one another, whereasoxyntic glands are in close contact with one another.
Acute GastritisThe initial phases of H. pylori infection are believed
to elicit an acute inflammatory response often referredto as acute gastritis. Significant clinical manifestationsare uncommonly associated with this histopathologicalentity, and when they are they tend to be of shortduration and, therefore, patients rarely undergo endo-scopic procedures at this time. As a consequence, infor-mation on the histopathological aspects of recent H.pylori infection has been gathered mainly from reportsof human ingestion studies in volunteers (Marshall etal., 1985; Morris and Nicholson, 1987), and rare docu-mented spontaneous occurrences (Frommer et al.,1988). In infected patients, H. pylori organisms arefound singly or grouped along the surface epithelium.They can be seen directly adhering to the cells or inacellular mucus strands. In acute infection, as well asin the chronic phase, bacteria are only rarely seen inthe deeper portions of the lumina of mucus or oxynticglands. Through this close interaction, the organismsare believed to exert a direct effect on the surface cells.The first step in this process of cellular injury is adher-
ence of the organisms to the epithelial cells. This hasbeen shown to alter the host cell cytoskeleton by cre-ating an adherence pedestal (Smoot et al., 1993). Oncea link between the bacteria and the specific epithelialcell has been established, transfer of various moleculesoccurs. These include bacterial enzymes, which have atoxic effect by degrading the protective mucus layer inthe stomach. Lipase and protease have been shown toperform this function, while urease releases ammonia,which possibly affects epithelial cell division (Smoot,1997). Besides enzymes, researchers have isolated H.pylori toxins that also affect epithelial cells. The firsthas been termed vacuolating toxin (Vac A) because ofits effects on cell cultures. The cytotoxin-associatedgene (now better know as a group of genes forming thecag A pathogenicity island) also yields a toxic protein,known as Cag A. This gene expression, which is notpresent in all H. pylori strains, has been linked withgreater inflammatory responses, and higher risk forpeptic ulcer disease and gastric adenocarcinoma (Bla-ser, 1996). Other direct effects may involve alterationof the normal apoptotic paterns of epithelial cells. Sev-eral studies have suggested that the organisms makethe epithelium more sensitive to oxidation injury ordecrease the nascent enzymes functioning to scavengeoxygen radicals (Mannick et al., 1996; Moss et al.,1996).
As gastric epithelial cells are injured by contact withH. pylori they become activated and release a variety ofcytokines. These chemical mediators, which activateinflammatory and immune processes, include tumornecrosis factor a, interferon g, and interleukins 1,6,and 8 (Genta, 1997). The complex cascade leads to anacute inflammatory infiltrate consisting of neutrophilicpolymorphonuclear leukocytes invading the gastric ep-ithelium. These are the major inflammatory cellspresent in the acute phase of gastritis, which has beenarbitrarily defined as the first 6 months after infection(Dixon et al., 1996). Acute gastritis eventually evolvesinto chronic active gastritis, which is believed to persistindefinitely in most infected subjects; only rare cases ofspontaneous resolution have been convincingly docu-mented.
Chronic GastritisThe appearance of gastric mucosa chronically in-
fected with H. pylori is quite characteristic. In additionto the presence of organisms, the columnar cells of thesurface epithelium undergo mucus depletion and takea cuboidal appearance (Fig. 1), which may give theepithelium a “flat” appearance. Individual cells mayseem as they have disappeared (“cell drop out”) leavinggaps that sometimes contain bacteria (Fig. 2). Micro-erosions and the formation of cellular tufts may alsooccur (Fig. 1, center), in some patients so prominent tosuggest that these microscopic lesions could be theprecursors of gastric ulcers (Genta, 1992; Hui et al.,1992).
These epithelial changes are seen in the large ma-jority of infected patients, and their presence shouldalert pathologists about the need to search for H. py-lori, even if no organisms are immediately apparent onthe injured epithelium.
The chronic inflammatory infiltrate associated withinfection is characteristic as well. Neutrophils are the
314 V.C. SMITH AND R.M. GENTA

most prominent cells in the surface and, less com-monly, in the glandular epithelium. In the lamina pro-pria, neutrophils are mixed with lymphocytes andplasma cells. This mixed, mostly mononuclear infil-trate can become quite dense and obscure and evenseparate the normally closely arranged gastric glands(Fig. 3). In most infected subjects in industrializednations the antral mucosa typically shows a moreprominent infiltrate, with formation of lymphoid folli-cles with germinal centers, a topographic distributiondefined in the Sydney System as “antrum-predominantgastritis” (Dixon et al., 1996). In the corpus of thesesubjects, the corpus is often minimally affected by theinflammation. When inflammation is present, it is of-ten in the form of a band of mild edema and chronicinflammation that separates the surface epitheliumfrom the underlying glands. This pattern, depicted inFigure 4, has been referred to as “superficial gastritis.”In socioeconomically deprived populations in the de-veloping world, the inflammation tends to be almostequally distributed throughout the entire stomach.This type of gastritis, frequently characterized by de-
velopment of atrophy and intestinal metaplasia, isknown as “pangastritis.” Although these patterns ofinflammation are most commonly the consequence ofH. pylori infection, in some cases bacteria are not iden-tified even when the biopsy specimens are stained withappropriate special stains. Sampling error is the mostfrequent cause of this scenario, but some patients dohave a type of focal H. pylori-negative chronic activegastritis. While in many of these individuals the originof H. pylori-negative chronic active gastritis is neverelucidated, some patients either have or will developclinically manifest Crohn’s disease (Meining et al.,1997).
Intestinal MetaplasiaIntestinal metaplasia is the replacement of glandu-
lar or foveolar epithelium by an intestinal-type epithe-lium (Figs. 5 and 6). This is the commonest type ofmetaplasia found in the stomach, although some indi-viduals with chronic gastritis in the corpus developchanges in the oxyntic mucosa known with the confus-ing name of “pseudopyloric” metaplasia. The metaplas-
Fig. 1. In many cases of chronic activegastritis, Helicobacter pylori form an almostcontinuous border on the surface and in theintercellular spaces of the gastric surface ep-ithelium. The epithelium is depleted of mu-cin, irregular, and several missing cells(“drop-out cells”) and cellular tufts can benoted. The lamina propria contains numer-ous mononuclear and polymorphonuclearcells.
Fig. 2. High-power photomicrograph of theinfected gastric epithelium showing details ofadherent bacteria (arrows at right and left) andthe space left by a drop-out cell, now containingnumerous organisms (center arrow).
315HELICOBACTER PYLORI IN GASTRIC PATHOLOGY

tic epithelium consists of various proportions of gobletcells and absorptive cells. Goblet cells are modifiedepithelial cells that secrete mucus. They are normallyfound throughout the gastrointestinal tract distally tothe pylorus, but not in the stomach. Although manytheories have been proposed, neither the histogenesisnor the initial impetus for intestinal metaplasia arecurrently understood. Epidemiological studies haveshown that significant amounts of intestinal metapla-sia are very rarely found in individuals who have neverbeen infected with H. pylori, and it is therefore widelybelieved to represent one of the possible outcomes ofchronic infection (Rugge et al., 1993). The prevalence ofintestinal metaplasia in biopsy specimens obtainedfrom unselected infected subjects populations rangesbetween 10 and 60% (Genta et al., 1995).
Metaplastic changes can vary from the so-called“complete” (metaplastic cells are morphologically iden-tical to the enterocytes of the small intestine, with abrush border of microvilli) to a spectrum of “incom-plete” types (also known as colonic types, in which cellslack a brush border and sulfated mucins may be de-tected both in absorptive and goblet cells). It has beennoted that H. pylori organisms are not usually seenoverlying the metaplastic epithelium (Dixon, 1991).Acidic mucus produced by the goblet cells was assumedto form an inhospitable microenvironment for the or-ganism, and teleological speculation suggested thatthis metaplasia represented a response of the gastricmucosa aimed at the elimination of H. pylori (Tsutsumiet al., 1984). Recent work based on cases in whichorganisms do adhere to metaplastic epithelium of theincomplete type (Genta et al., 1996; Ota et al., 1998),
led to the speculation that incomplete metaplasia mayrepresent a hybrid phenotype in which there is stillexpression of surface molecules to which H. pylori mayadhere. Complete intestinal metaplasia is a phenotypethat does not express the site for H. pylori adherence,and thus no organisms are seen attached to this epi-thelium.
The frequent association between intestinal meta-plasia and mucosal atrophy, and the association ofthese two features with the development of gastricadenocarcinoma make the detection of intestinal meta-plasia in a gastric biopsy specimen a particularly im-portant finding to report. However, the amount ofmetaplasia that reaches significance remains highlycontroversial, and pathologists continue to strugglewith such questions as whether a minute patch ofgoblet cells in the antrum is a real predictor of gastriccancer. If not, how much metaplasia and atrophy areneeded to diagnose “atrophic gastritis”? Only popula-tion-based large prospective patho-epidemiologicalstudies can provide an answer to these issues.
AtrophyAtrophy of the gastric epithelium has been defined as
“loss of glands.” However, we have recently proposed toredefine gastric mucosal atrophy as the “loss of appro-priate glands” to emphasize that, after the glands thatare normally present in an area of the stomach disap-pear, they may either be replaced by extracellular ma-trix (usually fibrous tissue similar to a scar) or by othertypes of glands (e.g., intestinal or pyloric metaplasia)In the past, when gastrectomies were commonly per-formed for duodenal and gastric ulcers, it was noticedthat many specimens contained patches of atrophicand metaplastic epithelium, frequently located alongthe lesser curvature of the stomach. This condition wastermed “multifocal atrophic gastritis.” Studies per-formed before the discovery of H. pylori noted thatpopulations with high rates of atrophic gastritis alsohad high rates of gastric cancer (Correa et al., 1976).This discovery led to the formulation of the now widelyaccepted hypothesis of a multi-step sequence thatstarts with gastritis and, through atrophy, metaplasia,and dysplasia eventually leads to gastric cancer . To-day, gastrectomies are rare specimens for the patholo-gist. Endoscopy and biopsy have become the mainstayof diagnosis for gastric lesions. Obviously, with only asmall portion of the stomach to analyze, a pathologist isat a disadvantage in diagnosing multifocal atrophicgastritis. Because of this difficulty, grading systemshave been generated to maximize pathologists’ abilityto make reasonable topographic inferences from a set ofbiopsy specimens, and also to increase interobserveragreement among pathologists. The Updated SydneySystem (Dixon et al., 1996) proposed a set of visualanalogue diagrams (originally conceived by TuomoKarttunen of the University of Oulu, Finalnd) to helpgrade several features of gastritis, including the inten-sity of inflammation, the extension of intestinal meta-plasia, and the severity of atrophy.
Even with these recommendations, a satisfactorylevel of agreement between pathologists has not beenreached yet by pathologists for the evaluation of atro-phy (el-Zimaity et al., 1996; Offerhaus et al., 1999), andan international group of gastric pathologists is still
Fig. 3. Gastric corpus with severe chronic active inflammation inthe interglandular spaces and the lower portions of the mucosa. Thishistological picture is characteristically seen in atrophic or pre-atro-phic gastritis associated with H. pylori, but may occasionally be seenin the patchy active gastritis due to Crohn’s disease.
316 V.C. SMITH AND R.M. GENTA

engaged in a quest for the best definition and the bestway to reliably diagnose atrophy and atrophic gastritis.As of now, many confusing and even conflicting termsare still used. For example, in the evaluation of atrophyin non-metaplastic gastric biopsy specimens, confusionhas stemmed from the fact that the glandular compo-nent of the mucosa may be replaced either by fibroblas-tic proliferation with extracellular matrix (fibrosis), asdepicted in Figure 7A, or by inflammatory cells, whichmay separate, obscure, or, in fact, replace glands (Fig.7B). Both scenarios cause the microscopic appearance ofdecreased gland tissue and both have been shown to
decrease acid secretion (Sipponen et al., 1996). Thus, bothtypes of glandular loss, true loss and apparent loss byseparation of glands by inflammatory cells, have func-tional repercussions and, therefore, there may be a justi-fication for applying the term atrophy in both cases.
A stricter definition of atrophy may have relevance,however. Although this is not known with certainty,the two scenarios above may differ in reversibility.When fibrosis or intestinal metaplasia has replacedglands, eradication of H. pylori infection would seemunlikely to restore the normal gastric epithelium. Incontrast, when atrophy is used to describe a decrease in
Fig. 4. Typical superficial gastritis in the gastriccorpus. Inflammation and mild edema form a sub-epithelial band that does not exceed in depth thelength of the fovoeolae.
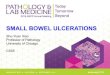
Fig. 5. Schematic representation of the genesis of intestinal meta-plasia. The normal epithelium (N), which consists of regularly ar-ranged columnar cells, is damaged (D) by H. pylori infection and thecells lose mucin, become shorter, and may even undergo rapid necro-sis and excess apoptosis, resulting in an irregular surface. The dam-aged epithelium is replaced by a new metaplastic one (IM), containingboth goblet and absorptive cells. The change affects also the laminapropria (LP), which undergoes a number of yet undefined structuralrearrangements likely to provide a microenvironment suited to theintestinal-type epithelium resting on it.
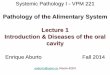
Fig. 6. Full-thickens replacement of oxyntic mucosa by intestinalmetaplasia. In such a case, metaplasia is equivalent to atrophy, sinceall original slides of that portion of the gastric mucosa have beenreplaced by other, non-appropriate intestinal-type structures.
317HELICOBACTER PYLORI IN GASTRIC PATHOLOGY

glands due to inflammation, treatment results in re-gression of the inflammatory infiltrate and an eventualreturn to the normal gastric architecture (Genta,1996). A second major reason to define gastric atrophymore strictly is the implication for neoplastic transfor-mation (Sipponen, 1989; Sipponen and Kimura, 1994).Atrophy has been reported to confer up to a 10-foldincreased risk for gastric adenocarcinoma (Parsonnet
et al., 1991). However, there are suggestions that onlymetaplastic atrophy is a definite precursor of gastricadenocarcinoma (Correa, 1995).
The role of H. pylori in the induction of gastric atro-phy is probably related to the damage inflicted uponthe mucosa by the inflammatory responses to the in-fection. However, this damage alone is not the solecause of atrophy, because a large proportion of chron-
Fig. 7. A: Oxyntic mucosa with moderate loss of glands and sig-nificant replacement by fibrous tissue. B: A dense inflammatory in-filtrate causes the appearance of a severe loss of glands in the oxynticmucosa. Although both these changes, if diffuse, could cause func-
tional atrophy with reduced acid production, consensus has not yetformed as to whether both these patterns constitute histological at-rophy.
318 V.C. SMITH AND R.M. GENTA

ically infected individuals seem to undergo a continu-ous process of inflammatory damage and repair andregeneration of the glands, with the result that nosignificant loss of glands ever occurs. This pattern iscalled “non-atrophic gastritis,” and is the most preva-lent type of gastritis in the industrialized countries ofWestern Europe and North America. When fibrosis andmetaplasia replace glands a permanent loss may re-sult, and “atrophic gastritis” is produced (Genta, 1997).This latter pattern, common in developing countries, isprobably induced by the combined effects of H. pyloriinfection and other factors that may damage the gas-tric mucosa, such as other infections in early childhood,or food products such as salt. The lack of vitamins(particularly ascorbic acid) caused by the absence offresh fruits and vegetables in the diet may furtherhamper mucosal regeneration and contribute to thegenesis of atrophic gastritis.
CancerAlthough gastric cancer rates have declined, as late
as 1980 this malignancy was still responsible for themost deaths from any neoplastic disease worldwide(Parkin et al., 1988), and in 1990 it remained the sec-ond most common malignant tumor (Parkin et al.,1999). In the United States the current incidence isabout 16 cases per 100,000 people (Silverberg et al.,1990). In Japan it is still the most common malignantdiagnosis with a rate of 80 cases per 100,000 per year.Prior to the discovery of H. pylori as the major cause ofchronic gastritis and its progression to atrophic gastri-tis, it was known that this latter pattern was associ-ated with the intestinal type of gastric adenocarcinoma(Correa et al., 1976). With proof that H. pylori is thecatalyst to this progression, the World Health Organi-zation classified the organism as a group 1 carcinogenin 1994 (Moller et al., 1995). The exact mechanism forthis transformation is unknown. Why, with over 50% ofthe world’s population infected, does less than 3% de-velop cancer? And why is the risk for gastric cancer sodifferent in different areas of the world? These ques-tions are the focus of many studies that look into dif-ferent strains of the organism (Figura, 1996), differentages at which infection is acquired, and antibiotictreatment as a possible prevention of gastric cancer(Parsonnet et al., 1996). The most common hypothesisviews H. pylori as the agent leading to gastritis andeventual atrophy over several decades. Differences inthe extent of the inflammation and atrophy with intes-tinal metaplasia are thought to confer different risks ofcancer. Other factors such as the presence of the cagAgene in the organism (Blaser, 1996), or increased oxy-gen radicals in the epithelium may promote mutationand carcinogenesis (Goldstone et al., 1996).
As has been alluded to, not all gastric cancers arepathogenetically linked to H. pylori. Only adenocarci-noma of the antrum and corpus (usually collectivelyreferred to as distal gastric cancer) has a clear associ-ation with H. pylori-induced metaplastic atrophic gas-tritis; a further indirect proof of this association isprovided by the decreasing incidence of gastric cancerin populations in which the prevalence of H. pylori hasbeen decreasing. In contrast, in those same populationsthe incidence of adenocarcinoma of the gastro-esopha-geal junction cardia has been increasing in the last
several decades . For example, carcinoma of the cardiaregion now accounts for approximately one third of allgastric cancers in the United States (Antonioli andGoldman, 1982). Most of these tumors are believed tobe pathogenetically related to carcinomas arising inBarrett’s mucosa and not H. pylori (Dolan et al., 1999;Wijnhoven et al., 1999). It has been hypothesized thatthe decreased prevalence of corpus atrophy that hasaccompanied the decrease in H. pylori infection is re-sponsible for the increased acid production that leadsto Barrett’s esophagus (Labenz et al., 1997). In thismodel, H. pylori, the cause of gastritis, gastric cancerand primary gastric B-cell lymphomas, is portrayed asan unlikely defender of the cardia (Blaser, 1999).
A term often used when discussing neoplasms of thestomach is “early gastric cancer.” These tumors are theearliest stages of common advanced gastric cancers.Early gastric cancers are frequently detected in Japan,where extensive endoscopy screening programs havebeen implemented for several years. In such an epidemi-ological context, this effort results in the effective cure ofa large percentage of gastric tumors detected at a curablestage (Eckardt, 1993). A similar approach of widespreadendoscopic screening is not believed to be cost-effective inEurope and North America, because of the relatively lowincidence of gastric cancer in these areas.
The global eradication of H. pylori infection is be-lieved by many to be the most viable approach to de-crease mortality from gastric cancer worldwide. How-ever, until some large prospective studies currentlyunderway in Japan and China yield convincing positiveresults, skeptics will continue to regard global eradica-tion plans as fanciful and perhaps dangerous attemptsto modify the course of the joint evolution of humansand their microorganisms.
MALT LymphomaAs discussed above, H. pylori infection elicits the
development of lymphoid follicles in the gastric mu-cosa. In some infected individuals this lymphoid re-sponse may take a predominantly monoclonal differen-tiation and low-grade B cell lymphomas known asMALT lymphomas arise (Isaacson, 1994a). The patho-genesis of these neoplasms and the exciting therapeu-tic possibilities opened by the discovery of an infection-promoted tumor are discussed elsewhere in this issue.
REFERENCESAnonymous. 1993. Epidemiology of, and risk factors for Helicobacter
pylori infection among 3194 asymptomatic subjects in 17 popula-tions. The EUROGAST Study Group. Gut 34:1672–1676.
Antonioli DA, Goldman H. 1982. Changes in the location and type ofgastric adenocarcinoma. Cancer 50:775–781.
Bergenzaun P, Kristinsson KG, Thjodleifsson B, Sigvaldadottir E,Molstad S, Held M and Wadstrom T 1996. Seroprevalence of Heli-cobacter pylori in south Sweden and Iceland. Scand J Gastroenterol31:1157–1161.
Blaser MJ. 1996. Role of vacA and the cagA locus of Helicobacterpylori in human disease. Aliment Pharmacol Ther 10(Suppl 1):73–77.
Blaser MJ. 1999. Hypothesis: the changing relationships of Helico-bacter pylori and humans: implications for health and disease.J Infect Dis 179:1523–1530.
Correa P. 1995. Helicobacter pylori and gastric carcinogenesis. Am JSurg Pathol 19(Suppl 1):S37–43
Correa P, Cuello C, Duque E, Burbano LC, Garcia FT, Bolanos O,Brown C, Haenszel W. 1976. Gastric cancer in Colombia. III. Nat-ural history of precursor lesions. J Natl Cancer Inst 57:1027–1035.
Dixon MF. 1991. Helicobacter pylori and peptic ulceration: his-topathological aspects. J Gastroenterol Hepatol 6:125–130.
319HELICOBACTER PYLORI IN GASTRIC PATHOLOGY

Dixon MF, Genta RM, Yardley JH, Correa P. 1996. Classification andgrading of gastritis. The updated Sydney System. InternationalWorkshop on the Histopathology of Gastritis Houston 1994. Am JSurg Pathol 20:1161–1181.
Dolan K, Sutton R, Walker SJ, Morris AI, Campbell F, Williams EM.1999. New classification of oesophageal and gastric carcinomasderived from changing patterns in epidemiology. Br J Cancer 80:834–842.
Dooley CP, Cohen H, Fitzgibbons PL, Bauer M, Appleman MD, Perez-Perez GI, Blaser MJ. 1989. Prevalence of Helicobacter pylori infec-tion and histologic gastritis in asymptomatic persons. N Engl J Med321:1562–1566.
Eckardt VF. 1993. Early detection of gastrointestinal malignancies:what is new?. Bildgebung 60(Suppl 1):13–15.
el-Zimaity HM, Graham DY, al-Assi MT, Malaty H, Karttunen TJ,Graham DP, Huberman RM, Genta RM. 1996. Interobserver vari-ation in the histopathological assessment of Helicobacter pylorigastritis. Hum Pathol 27:35–41.
Figura N. 1996. Helicobacter pylori exotoxins and gastroduodenaldiseases associated with cytotoxic strain infection. Aliment Phar-macol Ther 10(Suppl 1):79–96.
Forman D. 1995. The prevalence of Helicobacter pylori infection ingastric cancer. Aliment.Pharmacol.Ther. 9 Suppl 2:71–76.
Frommer DJ, Carrick J, Lee A, Hazell SL. 1988. Acute presentation ofCampylobacter pylori gastritis. Am J Gastroenterol 83:1168–1171.
Genta RM. 1992. Counting angels and bacteria. The quest for aunifying theory of ulcerogenesis. Am J Clin Pathol 98:549–551.
Genta RM. 1995. Helicobacter pylori as a promoter of intestinal meta-plasia and gastric cancer: an alluring hypothesis in search of evi-dence. Eur J Gastroenterol Hepatol 7(Suppl 1):S25–30.
Genta RM. 1996. Recognizing atrophy: another step toward a classi-fication of gastritis. Am J Surg Pathol 20(Suppl 1):S23–S30.
Genta RM. 1997. The immunobiology of Helicobacter pylori gastritis.Semin Gastrointest Dis 8:2–11.
Genta RM, Hamner HW, Graham DY. 1993. Gastric lymphoid folliclesin Helicobacter pylori infection: frequency, distribution, response totriple therapy. Hum Pathol 24:577–583.
Genta RM, Gurer IE, Graham DY. 1995. Geographical pathology ofHelicobacter pylori infection: is there more than one gastritis? AnnMed 27:595–599.
Genta RM, Gurer IE, Graham DY, Krishnan B, Segura AM, GutierrezO, Kim JG, Burchette JLJ. 1996. Adherence of Helicobacter pylorito areas of incomplete intestinal metaplasia in the gastric mucosa.Gastroenterology 111:1206–1211.
Goldstone AR, Quirke P, Dixon MF. 1996. Helicobacter pylori infec-tion and gastric cancer. J Pathol 179:129–137.
Graham DY, Malaty HM, Evans DG, Evans DJ.J, Klein PD, Adam E.1991. Epidemiology of Helicobacter pylori in an asymptomatic pop-ulation in the United States. Effect of age, race , socioeconomicstatus. Gastroenterology 100:1495–1501.
Holcombe C, Omotara BA, Eldridge J, Jones DM. 1992. H. pylori, themost common bacterial infection in Africa: a random serologicalstudy. Am J Gastroenterol 87:28–30.
Hui PK, Chan WY, Cheung PS, Chan JK, Ng CS. 1992. Pathologicchanges of gastric mucosa colonized by Helicobacter pylori. HumPathol 23:548–556.
Isaacson PG. 1994a. Gastric lymphoma and Helicobacter pylori.N Engl J Med 330:1310–1311.
Isaacson PG. 1994b. Gastrointestinal lymphoma. Hum Pathol 25:1020–1029.
Labenz J, Blum AL, Bayerdorffer E, Meining A, Stolte M, Borsch G.1997. Curing Helicobacter pylori infection in patients with duode-nal ulcer may provoke reflux esophagitis. Gastroenterology 112:1442–1447.
Malaty HM, Engstrand L, Pedersen NL, Graham DY. 1994. Helico-bacter pylori infection: genetic and environmental influences. Astudy of twins. Ann Intern Med 120:982–986.
Mannick EE, Bravo LE, Zarama G, Realpe JL, Zhang XJ, Ruiz B,Fontham ET, Mera R, Miller MJ, Correa P. 1996. Inducible nitricoxide synthase, nitrotyrosine, apoptosis in Helicobacter pylorigastritis: effect of antibiotics and antioxidants. Cancer Res 56:3238–3243.
Marshall BJ. 1995. The 1995 Albert Lasker Medical Research Award.Helicobacter pylori. The etiologic agent for peptic ulcer. JAMA274:1064–1066.
Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. 1985. Attemptto fullfil Koch’s postulates for pyloric Campylobacter. Med J Aust142:436–439.
Meining A, Bayerdorffer E, Bastlein E, Raudis N, Thiede C, Cyrus B,Kramer W, Klann H, Labenz J, Stolte M. 1997. Focal inflammatory
infiltrations in gastric biopsy specimens are suggestive of Crohn’sdisease. Crohn’s Disease Study Group Germany. Scand J Gastro-enterol 32:813–818.
Mitchell HM, Li YY, Hu PJ, Liu Q, Chen M, Du GG, Wang ZJ, Lee A,Hazell SL. 1992. Epidemiology of Helicobacter pylori in southernChina: identification of early childhood as the critical period foracquisition. J Infect Dis 166:149–153.
Moller H, Heseltine E, Vainio H. 1995. Working group report onschistosomes, liver flukes and Helicobacter pylori. Int J Cancer60:587–589.
Morris A, Nicholson G. 1987. Ingestion of Campylobacter pyloridiscauses gastritis and raised fasting gastric pH. Am J Gastroenterol82:192–199.
Moss SF, Calam J, Agarwal B, Wang S, Holt PR. 1996. Induction ofgastric epithelial apoptosis by Helicobacter pylori. Gut 38:498–501.
Offerhaus GJ, Price AB, Haot J, Ten Kate FJ, Sipponen P, Fiocca R,Stolte M, Dixon MF. 1999. Observer agreement on the grading ofgastric atrophy. Histopathology 34:320–325.
Ota H, Katsuyama T, Nakajima S, el-Zimaity H, Kim JG, GrahamDY, Genta RM. 1998. Intestinal metaplasia with adherent Helico-bacter pylori: a hybrid epithelium with both gastric and intestinalfeatures. Hum Pathol 29:846–850.
Owen DA. 1986. Normal histology of the stomach. Am J Surg Pathol10:48–61.
Parkin DM, Laara E, Muir CS. 1988. Estimates of the worldwidefrequency of sixteen major cancers in 1980. Int J Cancer 41:184–197.
Parkin DM, Pisani P, Ferlay J. 1999. Estimates of the worldwideincidence of 25 major cancers in 1990. Int J Cancer 80:827–841.
Parsonnet J. 1998. Helicobacter pylori: the size of the problem. Gut43(Suppl 1):S6–S9.
Parsonnet J, Friedman GD, Vandersteen DP, Chang Y, Vogelman JH,Orentreich N, Sibley RK. 1991. Helicobacter pylori infection and therisk of gastric carcinoma . N Engl J Med 325:1127–1131.
Parsonnet J, Harris RA, Hack HM, Owens DK. 1996. Modelling cost-effectiveness of Helicobacter pylori screening to prevent gastriccancer: a mandate for clinical trials . Lancet 348:150–154.
Pisani P, Parkin DM, Munoz N, Ferlay J. 1997. Cancer and infection:estimates of the attributable fraction in 1990. Cancer EpidemiolBiomarkers Prev 6:387–400.
Queiroz DM, Rocha GA, Mendes EN, Carvalho AS, Barbosa AJ, Ol-iveira CA, Lima GFJ. 1991. Differences in distribution and severityof Helicobacter pylori gastritis in children and adults with duodenalulcer disease. J Pediatr Gastroenterol Nutr 12:178–181.
Replogle ML, Glaser SL, Hiatt RA, Parsonnet J. 1995. Biologic sex asa risk factor for Helicobacter pylori infection in healthy youngadults. Am J Epidemiol 142:856–863.
Rugge M, Di Mario F, Cassaro M, Baffa R, Farinati F, Rubio JJ, NinfoV. 1993. Pathology of the gastric antrum and body associated withHelicobacter pylori infection in non-ulcerous patients: is the bacte-rium a promoter of intestinal metaplasia? Histopathology 22:9–15.
Silverberg E, Boring CC, Squires TS. 1990. Cancer Statistics, CACancer J Clin 40:9–26.
Sipponen P. 1989. Atrophic gastritis as a premalignant condition. AnnMed 21:287–290.
Sipponen P, Kimura K. 1994. Intestinal metaplasia, atrophic gastritisand stomach cancer: trends over time. Eur J Gastroenterol Hepatol6(Suppl 1):S79–S83.
Sipponen P, Hyvarinen H, Siurala M. 1996. H. pylori corpus gastritis:relation to acid output. J Physiol Pharmacol 47:151–159.
Smoot DT. 1997. How does Helicobacter pylori cause mucosal dam-age? Direct mechanisms. Gastroenterology 113 S31–S34
Smoot DT, Resau JH, Naab T, Desbordes BC, Gilliam T, Bull-HenryK, Curry SB, Nidiry J, Sewchand J, Mills-Robertson K. 1993. Ad-herence of Helicobacter pylori to cultured human gastric epithelialcells. Infect Immun 61:350–355.
Talley NJ. 1996. Helicobacter pylori and non-ulcer dyspepsia. Scand JGastroenterol Suppl 220:19–22.
Tsutsumi Y, Nagura H, Watanabe K. 1984. Immune aspects of intes-tinal metaplasia of the stomach: an immunohistochemical study.Virchows Arch A Pathol Anat Histopathol 403:345–359.
Veldhuyzen vZS. 1997. The role of Helicobacter pylori infection in non-ulcer dyspepsia. Aliment Pharmacol Ther11(Suppl 1):63–9, 63–69.
Wijnhoven BP, Siersema PD, Hop WC, van Dekken H, Tilanus HW.1999. Adenocarcinomas of the distal oesophagus and gastric cardiaare one clinical entity.Rotterdam Oesophageal Tumour StudyGroup. Br J Surg 86:529–535.
Wotherspoon AC, Doglioni C, Diss TC, Pan L, Moschini A, De Boni M,Isaacson PG. 1993. Regression of primary low-grade B-cell gastriclymphoma of mucosa-associated lymphoid tissue type after eradi-cation of Helicobacter pylori. Lancet 342:575–577.
320 V.C. SMITH AND R.M. GENTA