Embed Size (px)
Citation preview

301
ROLE OF ADRENERGIC RECEPTORS
IN GLUCOSE-INDUCED INSULINSECRETION IN MAN
EROL CERASI SUAD EFFENDIC
ROLF LUFT
Department of Endocrinology and Metabolism, KarolinskaHospital, Stockholm 60, Sweden
Summary Administration to healthy volunteersof a &bgr;-receptor blocker (propranolol)
in most instances significantly inhibited the insulinresponse to glucose infusion, while &agr;-receptor block-ing (by phentolamine) enhanced the insulin release.The inhibition induced by the &bgr;-blocking agent wastotally or partially overcome by simultaneous adminis-tration of aminophylline. These results indicate that,in man, glucose-induced insulin release is mediated
by adenyl cyclase and, consequently, by the intra-cellular level of cyclic adenosine monophosphate.
INTRODUCTION
A RELATIONSHIP between adrenergic receptors andinsulin release from the pancreas in man was firstshown by Porte et al.1 who showed that the insulin-supressing effect of catecholamines is mediated by thea-adrenergic receptors. However, Porte 2 has saidthat he does not know if adrenergic receptors partici-pate in the physiological stimulation of insulin secre-tion. We have found that insulin release during
hyperglycaemia does involve the adrenergic receptorsystem.
PATIENTS AND METHODS
Tests were done on six healthy volunteers, aged 22-34,with normal intravenous glucose tolerance 3 (k values 1-13-3.85). Plasma-insulin levels were measured during a
glucose-infusion test (G.I.T.) 4 in which a priming dose of500 mg. glucose per kg. body-weight was followed by theconstant infusion, for 60 minutes, of 20 mg. of glucose perkg. per minute. Venous blood-samples for measurementof blood-glucose and plasma-insulin (double-antibodyradioimmunoassay 5) were drawn at 10-minute intervals
during the infusion period and at 20-minute intervals foranother hour. The effect of P-receptor blockade on insulinresponse to glucose infusion was investigated in a secondexperiment by giving 3 mg. propranolol intravenously over5 minutes followed by a constant infusion of 0-08 mg. perminute for 85 minutes. A G.I.T. was started 30 minutesafter the beginning of propranolol administration. Blood-
samples were collected during the half-hour precedingthe G.I.T. The effect of a-receptor blockade was investi-gated by giving a phentolamine infusion (0-5 mg. per
minute) during the half-hour preceding the G.I.T. and
during the glucose infusion. Blood-samples were takenas in the experiments with propranolol. In a fourth seriesof experiments the propranolol/G.I.T. was combined withthe administration of aminophylline. This drug was given30 minutes before the 5 mg. dose of propranolol as a
200 mg. priming injection followed by 200 mg. adminis-tered as a constant infusion for 60 minutes.
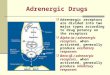
RESULTS (see figure)Neither a nor blockade alone affected basal levels
of blood-glucose and plasma-insulin.
(a) Propranolol (b) Propranolol (c) Phentolamine (d) Aminophylline + propranololBlood-glucose and plasma-insulin response to glucose-infusion test after propranolol, phentolamine, or propranolol plus aminophylline.
Horizontal bars show duration of infusion of: (1) glucose, (2) propranolol (or phentolamine), and (3) aminophylline

302
In four out of six experiments P-receptor blockadeby propranolol significantly inhibited the insulin
response to glucose. In three, this inhibition lastedthroughout the period of increased insulin secretion(a); in one the initial response was preserved (b).
In three out of four tests the a-receptor blockingagent phentolamine enhanced the glucose-inducedrelease of insulin (c).
In all three tests propranolol-induced inhibition ofinsulin release on glucose infusion was partially ortotally overcome by the simultaneous administrationof aminophylline (d). (Aminophylline alone, in theamounts used here, has no enhancing effect on insulinsecretion in healthy individuals. 6)
DISCUSSION
Since {3-receptor blockade inhibited and oc-blockadeenhanced the glucose-induced insulin release, this
implies that the stimulatory action of glucose oninsulin secretion is either mediated through the
&bgr; receptor or is closely related to it. The variabilityin the effects of the blocking agents might be due toindividual differences in the potency of the receptorsor in their sensitivity to the drugs used.7Robinson et al. have suggested that p-adrenergic
receptors are identical with, or closely related to
adenyl cyclase. Since cyclic A.M.P. is a key substancein the secretion of insulin 9 the inhibition of glucose-induced insulin release by blockade may be relatedto a decrease in the formation of cyclic A.M.P. This
assumption is supported by our finding that
aminophylline counteracted the inhibitory effect of
propranolol. Since aminophylline alone, at the dosesused here, does not stimulate insulin release, theinsulin response to glucose in the presence of bothpropranolol and aminophylline could not be the sumof inhibitory and stimulatory actions on insulin release.We suggest that the small doses used here of amino-
phylline, a competitive inhibitor of adenosine-3,5’-monophosphate phosphodiesterase, could influencesignificantly the level of cyclic A.M.P. only when thisnucleotide was formed at a lower rate than normal.Bressler et al.1O suggested that (3-receptor blockers inmice act at a locus beyond adenyl cyclase, but theyused blocker doses 100 times higher than ours, andthe effects may have been unspecific.Our findings suggest that, in man, glucose-induced
insulin release is mediated by adenyl cyclase and,consequently, by the intracellular level of cyclic A.M.P.We thank Mr. A. Roovete, Mrs. Kerstin Waldelof, Mrs.
Christina Thornqvist, Miss Gunnie Sandgren, and Miss AnetteJohansson for valuable assistance. This study was supportedby grants from the Swedish Medical Research Council (B 69-19X-34-05 A) and Knut and Alice Wallenberg’s Foundation.Requests for reprints should be addressed to R. L.
REFERENCES
1. Porte, D. Jr., Graber, A. L., Kuzuya, T., Williams, R. H. J. clin.Invest. 1966, 45, 288.
2. Porte, D. Jr. Archs. intern. Med. 1969, 123, 252.3. Ikkos, D., Luft, R. Acta endocr., Copenh. 1957, 25, 312.4. Cerasi, E., Luft, R. ibid. 1967, 55, 278.5. Hales, C. N., Randle, P. J. Biochem. J. 1963, 88, 137.6. Cerasi, E., Luft, R. Horm. metab. Res. (in the press).7. Östman, J., Efendic, S. Acta med. scand. (in the press).8. Robinson, G. A., Butcher, R. W., Sutherland, E. W. Ann. N.Y.
Acad. Sci. 1967, 139, 703.9. Sussman, K. E., Vaughan, G. D., Timmer, R. F. Diabetes, 1966,
15, 521.10. Bressler, R., Vargas Cordon, M., Brendel, K. Archs intern. Med.
1969, 123, 248.
ACETATE IN THE CORRECTION OF
ACIDOSIS SECONDARY TO DIARRHŒA
RICHARD A. CASH
DAVID R. NALIN
KHONDAKAR M. M. TOHA
ZAHIDUL HUQROBERT A. PHILLIPS
Pakistan-SEATO Cholera Research Laboratory, Institute ofPublic Health, Mohakhali, Dacca 12, East Pakistan
Summary Patients with acute acidosis and de-
hydration due to diarrhœa were treatedwith rapid intravenous infusions of electrolyte solutionscontaining either acetate or bicarbonate, and the rate ofcorrection of arterial pH was monitored. The final pHcorrection was similar with the two types of solutions,demonstrating that acetate-containing solutions are
effective in the treatment of this type of metabolicacidosis.
INTRODUCTION
SOLUTIONS containing either bicarbonate or lactatehave been used widely in the correction of the acidosisof diarrhrea.1-3 Bicarbonate, however, must be auto-claved under a high partial pressure of carbon dioxide,a procedure which makes it difficult to produce largequantities of intravenous solution. Lactate readilysupports the growth of mould, can cause deteriorationof certain types of glassware, and thus has a variableshelf-life. Sodium acetate is easy to autoclave,inexpensive, stable, and has a long shelf-life. This
study was undertaken to determine the efficacy ofintravenous infusions of solutions containing acetateand other electrolytes in the correction of the acidosisand dehydration of cholera and other acute diarrhoealdiseases.
PATIENTS AND METHODS
17 patients were selected from severely dehydratedpatients admitted to our ward with a history of acutediarrhoea. After a brief history and physical examination,an arterial blood-sample and electrocardiogram were
obtained, and intravenous infusion was begun. Arterialblood-samples and electrocardiogram were repeated aftereach litre of replacement therapy and after rehydration wascomplete (as determined by clinical status and plasma sp.gr.). The compositions of the intravenous solutions used inthe different groups is shown in table I.
TABLE I-COMPOSITION OF SOLUTIONS USED (meq./l.)
The bicarbonate solution and acetate-2 were prepared at our laboratory.Acetate-1 (’ Isolyte E McGaw Laboratories, Milledgeville, Georgia)was supplied by the U. S. Agency for International Development.
The blood-samples were analysed for pH, carbon dioxide,electrolytes, hasmatocrit, and plasma sp. gr. The carbon-dioxide content was determined by Van Slyke manometricmethod. Sodium and potassium were determined on aBaird atomic flame photometer; calcium and magnesium ona Perkin-Elmer atomic absorption spectrophotometer, andpH on a Corning 12-B meter.
RESULTS
Of the 17 patients, 9 received a solution containingacetate and 8 received a solution containing bi-