Embed Size (px)
Citation preview
Right Ventricular Metastatic Melanoma 27 Years After Resection of the Primary Tumor
SETH M. MINDELL, MD, ALLAN W. CHERNICK, MD, MARCUS H. SUGARMAN, MD, RICHARD M. ZIRKIN, MD, AND ROBERT E. BLOOM, MD
This article is a case report of a 65-year-old white woman with a history of malignant melanoma, resected from her back in 1959. She presented 27 years later with right-sided heart failure and metastatic melanoma to her right ventricle. To the authors’ knowledge, a large ventricular mass as the sole site of disease recurrence has not been described previously.
Cancer 63:1237-1239, 1989.
NTRAVENTRICULAR masses are quite rare. Primary and I metastatic malignancies, benign tumors, and thrombi are possible etiologies. Angiosarcomas, rhabdomyosar- comas, and fibrosarcomas are the most common primary malignant tumors of the heart.’ Myxomas and lipomas are the most frequently occumng benign tumors.’ In pa- tients with malignancies, cardiac metastases are found in 1.5% to 21% of autopsies.2 Carcinoma of the lung and breast are the most common source of cardiac metastases due to their high prevalence rate.2q3 Malignant melanoma, leukemia, and lymphoma have a disproportionately high rate of cardiac inv~lvement .~ .~ We report a patient with a history of a malignant melanoma who presents 27 years later with a right ventricular mass.
Case Report
A 65-year-old white woman presented with a 2-month history of exertional dyspnea, fatigue, and pedal edema. She had no previous history of heart disease. Twenty-seven years earlier a malignant melanoma “without evidence of deep invasion” had been excised from her back.
On examination the blood pressure was 130/70 mmHg, the pulse was 80 bpm, and the respirations were 16. Careful fun- doscopic exam was normal. There was marked jugular venous distension with prominent A and V waves. The lungs were clear. A left parasternal heave was palpable. There was a right-sided S4 gallop. A grade III/VI pansystolic murmur, which increased with inspiration, was heard at the lower left sternal border. A soft I/IV high-frequency diastolic murmur was also heard near the lower left sternal border. The liver was palpable 3 cm below
From the Departments of Internal Medicine and Pathology, Sinai Hospital of Detroit, Detroit, Michigan.
The authors thank Gordon K. Danielson, MD, of the Department of Cardiothoracic Surgery at Mayo Clinic, Nena Apt, LPN, Demetrea Wat- son, and Susan Palmer-Abu-Zahra.
Address for reprints: Seth M. Mindell, MD, Sinai Hospital of Detroit, 6767 West Outer Drive, Detroit, MI 48235.
Accepted for publication August 22, 1988.
the right costal margin and was highly pulsatile. Mild pedal edema was present. Examination of the skin failed to reveal any abnormal areas of hyperpigmentation.
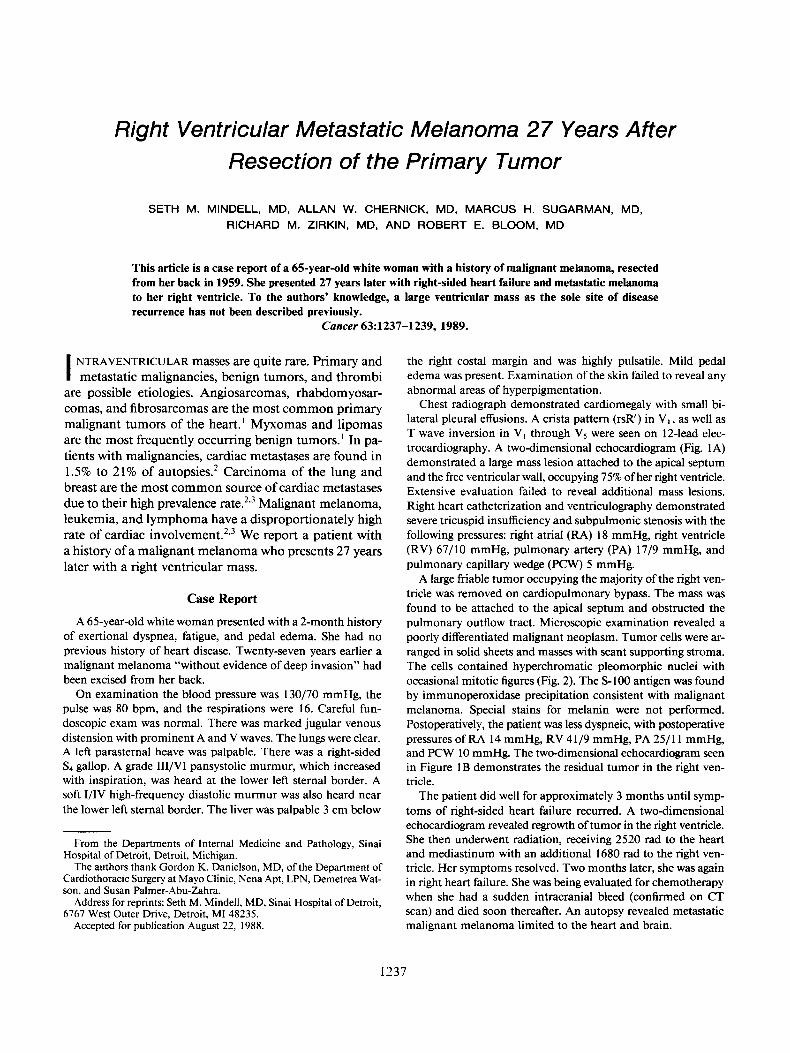
Chest radiograph demonstrated cardiomegaly with small bi- lateral pleural effusions. A crista pattern (rsR‘) in Vl , as well as T wave inversion in V, through V5 were seen on 12-lead elec- trocardiography. A two-dimensional echocardiogram (Fig. 1 A) demonstrated a large mass lesion attached to the apical septum and the free ventricular wall, occupying 75% of her right ventricle. Extensive evaluation failed to reveal additional mass lesions. Right heart catheterization and ventriculography demonstrated severe tricuspid insufficiency and subpulmonic stenosis with the following pressures: right atrial (RA) 18 mmHg, right ventricle (RV) 67/10 mmHg, pulmonary artery (PA) 17/9 mmHg, and pulmonary capillary wedge (PCW) 5 mmHg.
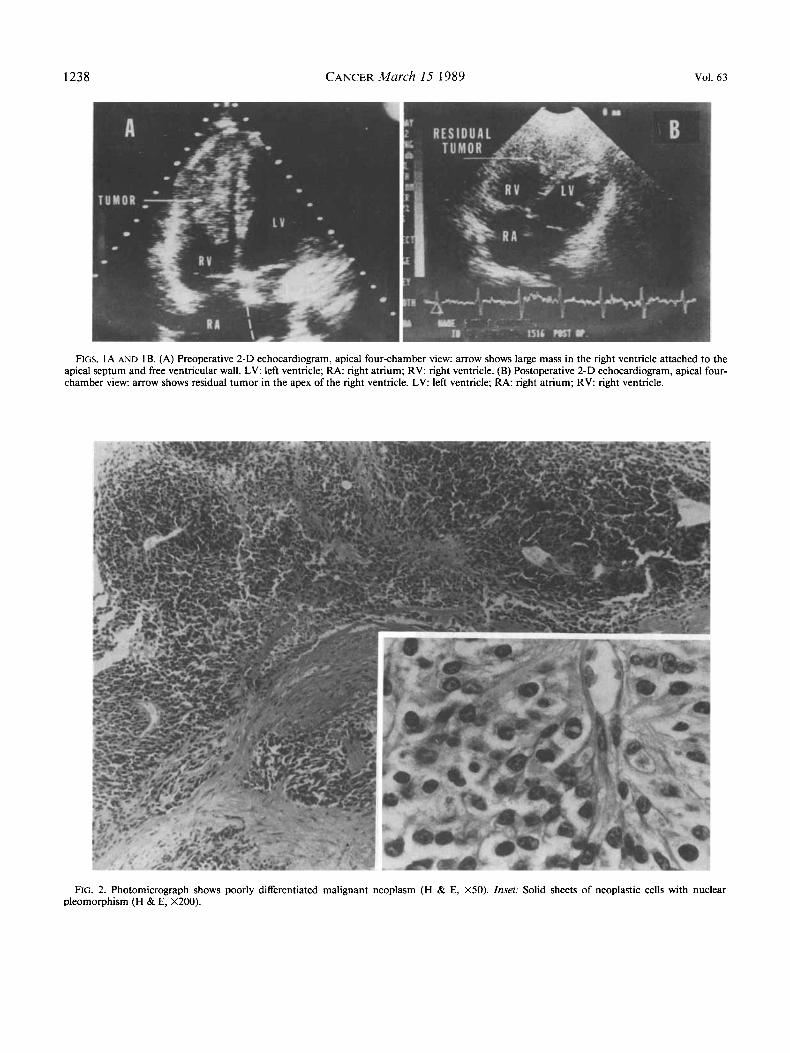
A large friable tumor occupying the majority of the right ven- tricle was removed on cardiopulmonary bypass. The mass was found to be attached to the apical septum and obstructed the pulmonary outflow tract. Microscopic examination revealed a poorly differentiated malignant neoplasm. Tumor cells were ar- ranged in solid sheets and masses with scant supporting stroma. The cells contained hyperchromatic pleomorphic nuclei with occasional mitotic figures (Fig. 2). The S-100 antigen was found by immunoperoxidase precipitation consistent with malignant melanoma. Special stains for melanin were not performed. Postoperatively, the patient was less dyspneic, with postoperative pressures of RA 14 mmHg, RV 4 1 /9 mmHg, PA 25/ 1 1 mmHg, and PCW 10 mmHg. The two-dimensional echocardiogram seen in Figure IB demonstrates the residual tumor in the right ven- tricle.
The patient did well for approximately 3 months until symp- toms of right-sided heart failure recurred. A two-dimensional echocardiogram revealed regrowth of tumor in the right ventricle. She then underwent radiation, receiving 2520 rad to the heart and mediastinum with an additional 1680 rad to the right ven- tricle. Her symptoms resolved. Two months later, she was again in right heart failure. She was being evaluated for chemotherapy when she had a sudden intracranial bleed (confirmed on CT scan) and died soon thereafter. An autopsy revealed metastatic malignant melanoma limited to the heart and brain.
1237
1238 CANCER March 15 1989 Vol. 63
FIGS. 1A AND IB. (A) Preoperative 2-D echocardiogram, apical four-chamber view: arrow shows large mass in the right ventricle attached to the apical septum and free ventricular wall. LV: left ventricle; RA: right atrium; R V right ventricle. (B) Postoperative 2-D echocardiogram, apical four- chamber view: arrow shows residual tumor in the apex of the right ventricle. LV: left ventricle; RA: right atrium; RV: right ventricle.
FIG. 2. Photomicrograph shows poorly differentiated malignant neoplasm (H & E, X50). Inset: Solid sheets of neoplastic cells with nuclear pleomorphism (H & E, X200).

No. 6 RIGHT VENTRICULAR MELANOMA - Mindell et al. 1239
Discussion
Metastatic melanoma to the heart has been well de- Glancy and Roberts2 reported 45 cases of car-
diac metastases from melanoma at the time of widespread systemic relapse. To our knowledge, a large ventricular mass as the sole site of disease recurrence has not been described. It has been that tumors of inter- mediate thickness, 1.70 mm to 3.64 mm, are most likely to be associated with delayed metastases. Unfortunately, the original slide was not available for review. The pa- thology report, however, stated that “there was no evi- dence of deep invasion.”
Malignant melanoma is a tumor which may have a bizarre natural history and unpredictable course. This re- port reemphasizes that prior excision of malignant mel- anoma, regardless of how remote in time, can never be considered irrelevant when evaluating a cardiac mass.
REFERENCES
1. Colucci WS, Braunwald E. In: Braunwald Heart Disease: A Text- book of Cardiovascular Medicine, ed. 3. Philadelphia: WB Saunders,
2. Glancy DL, Roberts WC. The heart in malignant melanoma: A study of 70 autopsy cases. Am J Cardiol 1968; 21:555-57 1.
3. Waller BF, Gottdiener JS, Virmani R, Roberts WC. The “charcoal heart” melanoma to the cor. Chest 1980; 77:671-676.
4. Koh HK, Sober AJ, Fitzpatrick TB. Late recurrence (beyond 10 years) of cutaneous malignant melanoma. JAMA 1984; 25 1: 1859-1862.
5. Hanley PC, Shub C, Seward JB, Wold LE. Intracavitary cardiac melanoma diagnosed by endomyocardial left ventricular biopsy. Chest
6. Thomas JH, Panoussopoulos DG, Jewel1 WR, Pierce GE. Tricuspid stenosis secondary to metastatic melanoma. Cancer 1977; 39: 1732-1737.
7. Kutalek SP, Panidis IP, Kotler MN, Mintz GS, Carver J, Ross JJ. Metastatic tumors of the heart detected by two-dimensional echocardi- ography. Am Heart J 1985; 109:343-349.
8. Day CL Jr, Mihm MC, Sober AJ ef al. Predictors of late deaths among patients with clinical Stage 1 melanoma who have not had bony or visceral metastases within the first 5 years after diagnosis. JAm Acad Dermatol 1983; 8:864-868.
1988; 1470- 1483.
1983; 84:195-198.


















![Liver resection for metastatic colorectal cancer - [email protected]](https://img.dokumen.tips/doc/110x75/620633768c2f7b1730055cf8/liver-resection-for-metastatic-colorectal-cancer-emailprotected.jpg)







