Embed Size (px)
Citation preview

4993
Key Words: 5-fluorouracil, Gastrointestinal mucositis, Rifaximin.
Introduction
Oral and gastrointestinal chemotherapy-indu-ced mucositis represents a common challenge for an oncologist, as this complication frequently requires chemotherapy dose reduction and sub-sequently decreases its’ efficacy. After cytotoxic drugs, gastrointestinal mucositis is most promi-nent in the small intestine, but it also occurs in the esophagus, stomach, and large intestine1.
The interplay between the gut tissues, the im-mune system and the microbiota is profoundly unbalanced by the chemotherapy that acts on all these components2,3. The cytotoxic drugs cause DNA damage and cell death directly and throu-gh the generation of reactive oxygen species. At the same time, transcription factors, like tran-scription factor nuclear factor kappa B (NF-kB) are activated and subsequently proinflammatory cytokine genes are up-regulated, leading to apop-tosis2,3. The antimetabolite 5-fluorouracil (5-FU) was associated with changes in the intestinal mi-crobiota in rats4,5. Complex interactions between the immune system and the altered intestinal mi-crobiota are responsible for degenerative and in-flammatory mucosal lesions. The gut microbiota plays a key role in this phase through the activa-tion of Toll-like receptor (TLR) signaling, espe-cially TLR2, TLR4 and TLR5. Once activated by intestinal microbiota, TLRs can also up-regula-te NFκB through complex signaling pathways6, further compounding the inflammatory response
Abstract. – OBJECTIVE: This study assessed the protective potential of rifaximin in 5-fluoro-uracil (5-FU) induced intestinal mucositis in the Wistar rats’.
MATERIALS AND METHODS: Twenty-nine Wistar rats were divided into 4 interventional groups of 6 animals (A, B, C and F) and one con-trol group (M) of 5 animals. Groups A, B and C received for three days consecutively rifaximin orally: 50 mg/kg (group A), 100 mg/kg (group B) and 200 mg/kg (group C). In the fourth day, 500 mg/kg of 5-FU was administered intraperitone-ally to the groups A, B, C and F. A semi-quan-titative histological assessment for duodenum, jejunum and colon were obtained by rating 11 histological characteristics of mucositis from 0 (normal) to 3 (severe). Semi-quantitative grades were a measure for TLR4 immunopositive cells. Statistical comparisons used - U Test, with a Bonferroni correction for alpha (p ≤ 0.016).
RESULTS: In the group F the most affected areas were the jejunum (median histological score 25) and the duodenum (median histologi-cal score 22). The assessment of duodenum his-tological lesions depicted significant difference between F and B groups (U = 1.5, p = 0.007) and between F and C groups (U = 0, p = 0.003). Grad-ed microscopic degenerative lesions on jeju-num were significantly different between F and C groups (U = 0, p = 0.004). Graded TLR4 immu-nopositive cells in the jejunum surface epitheli-um was significantly different between groups F and C (U = 2.5, p = 0.006). In the colonic muco-sa, significantly differences were noted on mi-croscopic degenerative lesions between F and A groups (U = 0, p = 0.004) and between F and C groups (U = 0, p = 0.004).
CONCLUSIONS: Pretreatment with 200 mg/kg of rifaximin for 3 consecutive days proved effi-cient in preventing intestinal mucosal degenera-tive lesions induced by 5-FU.
European Review for Medical and Pharmacological Sciences 2016; 20: 4993-5001
L. CIOBANU1,2, M. TANTAU1,2, S. VALEAN1,3, A. PARAU2, I. BEDECEAN4, R. MÎRLENEANU5, C. BERCE1, C. CATOI5, M. TAULESCU5
1University of Medicine and Pharmacy Iuliu Hatieganu, Cluj-Napoca, Romania2Regional Institute of Gastroenterology and Hepatology, Cluj-Napoca, Romania31st Medical Clinic Cluj-Napoca, Romania4Pathophysiology Department, Faculty of Veterinary Medicine, University of Agricultural Sciences and Veterinary Medicine, Cluj-Napoca, Romania5Pathology Department, Faculty of Veterinary Medicine, University of Agricultural Sciences and Veterinary Medicine, Cluj-Napoca, Romania
Corresponding Author: Lidia Ciobanu, MD; e-mail: [email protected]
Rifaximin modulates 5-fluorouracil-induced gastrointestinal mucositis in rats

L. Ciobanu, M. Tantau, S. Valean, A. Parau, I. Bedecean, R. Mîrleneanu, C. Berce, C. Catoi, M. Taulescu
4994
through the generation and amplification of the tu-mor necrosis factor (TNF)-α, interleukin-1β (IL-1β), and interleukin-6 (IL-6)2. 5-Fluorouracil also significantly decreases the mucin at the jejunal and colon ic mucosa levels7.
Recent reports suggested that probiotics could modulate the microbiota and decrease the severity of chemotherapy-induced mucositis8-11.
Rifaximin, a non-absorbable oral antibiotic that acts locally in the gastrointestinal tract with minimal systemic adverse effects, may have beneficial ef-fects in decreasing the severity of chemotherapy-in-duced mucositis, by modulating the microbiota. In vitro studies found that rifaximin possessed activity against Lactobacillus spp., Staphylococcus spp., En-terococcus spp., Bacillus cereus, Moraxella catar-rhalis, Haemophilus influenzae12.
This study was designed to assess the potential of rifaximin to protect against 5-FU-induced gastroin-testinal mucositis in the Wistar rats’ intestine.
Materials and Methods
Animals and Study Design Twenty-nine adults, male and female Wistar
rats, with an average weight of 300 g were used for in the experiment, conducted in the licensed animal house facility of the Faculty of Veteri-nary Medicine from Cluj-Napoca (Romania). The experiments were approved by the Institutional Animal Ethics Committee, being in accordance with Romanian laws. The animals were divided into 4 interventional groups of 6 animals (named A, B, C and F) and one control group (M) with 5 Wistar rats.
Groups A, B and C received rifaximin orally for three days consecutively: 50 mg/kg in group A, 100 mg/kg in group B and 200 mg/kg in group C. Group F and M received the vehicle. The an-tibiotics were given by oral gavage and after two hours the animals were allowed to eat. In the four-th day, 500 mg/kg of 5-FU was administered in-traperitoneally to the groups A, B, C and F. The M group received the vehicle. After 24 hours, the animals were sacrificed by deep ether anesthesia. The intestinal tissue samples were collected from the proximal part of the duodenum, distal part of the jejunum and the middle part of the colon.
Histological AssessmentFor the histological examination, the samples
were fixed in 10 % phosphate-buffered formalin (pH 7.0) for 24 hours, routinely processed, em-
bedded in paraffin wax, cut into 3-4 micrometers (μm) sections and stained with hematoxylin and eosin (H&E) and Periodic Acid Schiff (PAS). Samples were examined using an Olympus Bx51 microscope. The photomicrographs were taken using an Olympus SP 350 digital camera and Cel-l^B basic imaging software (Olympus Corpora-tion, Tokyo, Japan).
The sections were evaluated for the degree of mucositis using a method described previously by Horvath et al13. A semi-quantitative histological as-sessment for each intestinal segment (duodenum, jejunum, and colon) was obtained by rating 11 hi-stological characteristics of mucositis from 0 (nor-mal) to 3 (severe). The criteria used were: villous fusion and stunting (atrophy), disruption of brush border and surface enterocytes, reduction in goblet cells number, reduction in numbers of mitotic figu-res, crypt loss/architectural disruption, disruption or distortion of crypt cells, crypt abscess formation, infiltration of polymorphonuclear cells, infiltration of lymphocytes, dilatation of lymphatics and ca-pillaries, thickening and edema of the submucosal and muscularis externa layers. The pathologist was experienced in the assessment of the gastrointestinal pathology and utilized the normal rat intestinal tis-sue as a baseline reference to grade each of the 11 histological criteria.
For the immunohistochemical method, the sections were prepared from the same blocks as the H&E-stained slides. The sections were incubated at 37°C for 12 hours and were processed using au-tomatic platform Leica BOND-MAX. The primary antibody rabbit polyclonal anti-TLR4, (ab13556, Abcam, Cambridge, UK) was diluted in 1% PBS-BSA (bovine serum albumin) at 1: 1000. The Bond Polymer Refine Detection kit (DS9800, No-vocastra) containing peroxide block, post-primary, polymer reagent, DAB chromogen and hematoxylin counterstain were used. The negative controls for each sample were prepared by replacing the primary antibody with mouse IgG1 Negative Control (Code X0931, Dako, Glostrup, Denmark).
Immunopositivity for TLR4 was evaluated by a pathologist (MT) separately for mucosal epithe-lium, glandular epithelium, and lamina propria14 and graded microscopically as follows: 0 – the same as background, 0.5 – close to background, 1 – well marked positivity, 1.5 focally enhanced, 2 – strong positivity, 2.5 – very strong positivity 15.
Statistical Analysis The histological and immunohistochemistry
scoring results were expressed as median IQR (in-
Rifaximin and 5-fluorouracil induced gastrointestinal mucositis
4995
terquartile range) and the results for villous height as mean ± standard deviation. One way ANOVA test was used to compare the means of jejunum and duodenal villous height. The independent groups were analyzed using the Kruskal-Wallis test, Mann-Whitney U-test or Student’s t-test. If Kruskal-Wallis test led to significant results (re-garding the applied semi-quantitative grades on studied groups) a Bonferroni correction for alpha was applied on Mann-Whitney U test, exact p va-lues ≤ 0.016 being considered statistically signi-ficant. For the statistical analysis, R environment for statistical computing and graphics, version 3.2.0 was used.
Results
Histological ScoresIn the control group, no important lesions were
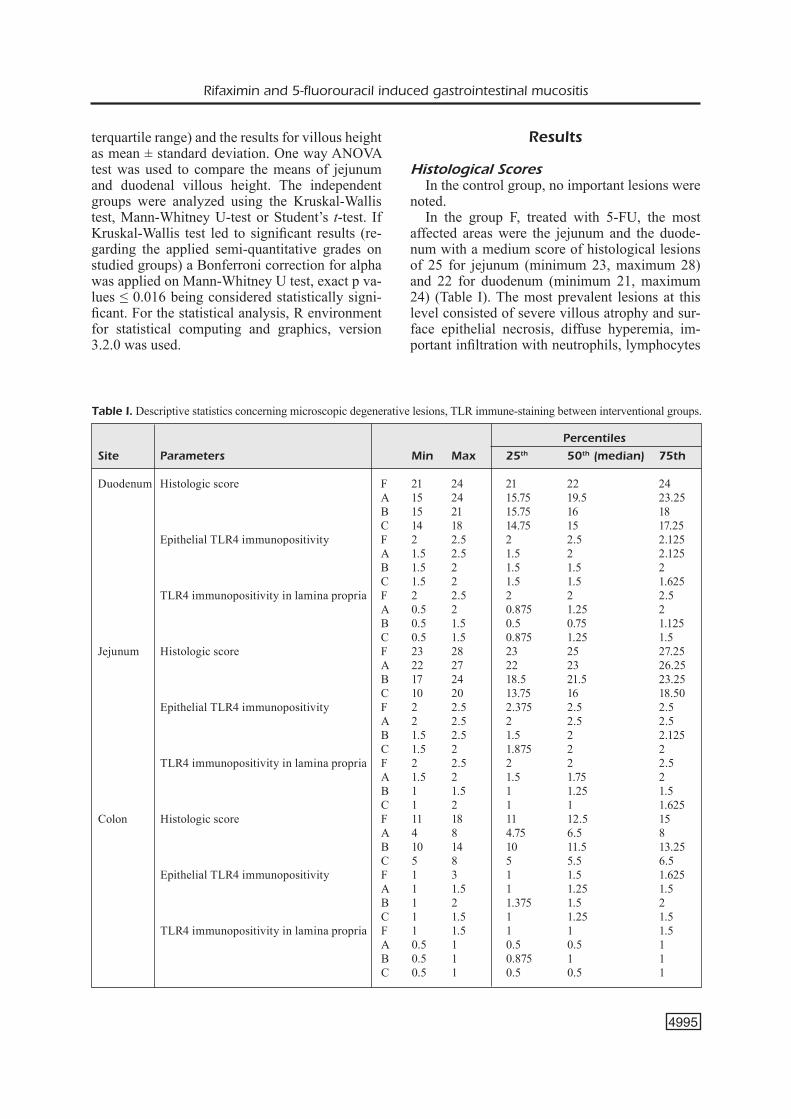
noted.In the group F, treated with 5-FU, the most
affected areas were the jejunum and the duode-num with a medium score of histological lesions of 25 for jejunum (minimum 23, maximum 28) and 22 for duodenum (minimum 21, maximum 24) (Table I). The most prevalent lesions at this level consisted of severe villous atrophy and sur-face epithelial necrosis, diffuse hyperemia, im-portant infiltration with neutrophils, lymphocytes
Table I. Descriptive statistics concerning microscopic degenerative lesions, TLR immune-staining between interventional groups.
Percentiles
Site Parameters Min Max 25th 50th (median) 75th
Duodenum Histologic score F 21 24 21 22 24 A 15 24 15.75 19.5 23.25 B 15 21 15.75 16 18 C 14 18 14.75 15 17.25 Epithelial TLR4 immunopositivity F 2 2.5 2 2.5 2.125 A 1.5 2.5 1.5 2 2.125 B 1.5 2 1.5 1.5 2 C 1.5 2 1.5 1.5 1.625 TLR4 immunopositivity in lamina propria F 2 2.5 2 2 2.5 A 0.5 2 0.875 1.25 2 B 0.5 1.5 0.5 0.75 1.125 C 0.5 1.5 0.875 1.25 1.5Jejunum Histologic score F 23 28 23 25 27.25 A 22 27 22 23 26.25 B 17 24 18.5 21.5 23.25 C 10 20 13.75 16 18.50 Epithelial TLR4 immunopositivity F 2 2.5 2.375 2.5 2.5 A 2 2.5 2 2.5 2.5 B 1.5 2.5 1.5 2 2.125 C 1.5 2 1.875 2 2 TLR4 immunopositivity in lamina propria F 2 2.5 2 2 2.5 A 1.5 2 1.5 1.75 2 B 1 1.5 1 1.25 1.5 C 1 2 1 1 1.625Colon Histologic score F 11 18 11 12.5 15 A 4 8 4.75 6.5 8 B 10 14 10 11.5 13.25 C 5 8 5 5.5 6.5 Epithelial TLR4 immunopositivity F 1 3 1 1.5 1.625 A 1 1.5 1 1.25 1.5 B 1 2 1.375 1.5 2 C 1 1.5 1 1.25 1.5 TLR4 immunopositivity in lamina propria F 1 1.5 1 1 1.5 A 0.5 1 0.5 0.5 1 B 0.5 1 0.875 1 1 C 0.5 1 0.5 0.5 1

L. Ciobanu, M. Tantau, S. Valean, A. Parau, I. Bedecean, R. Mîrleneanu, C. Berce, C. Catoi, M. Taulescu
4996
and macrophages, crypt architectural disruption with crypt abscesses formation (Figure 1 D-D1, J-J1). The cellular turnover was reduced, many fields lacking epithelial cells division. On the co-lonic mucosa, the degenerative lesions were mild and moderate, with the medium histological score 12.5 (minimum 11, maximum 18). Mild subepi-thelial edema, mild infiltration with neutrophils and lymphocytes within lamina propria and redu-ced cellular turnover were identified in the colonic mucosa (Figure 1 C-C1). The number and distri-bution of the PAS-positive Goblet cells were si-gnificantly reduced, mainly at the duodenum and jejunum levels (Figure 1 D2, J2 and C2).
In the group F, diffuse and intense TLR4 stai-ning was noted on epithelial surface and lamina propria of the duodenum and jejunum (Table I). The intensity of TLR4 staining was moderate on the epithelial surface and lamina propria of the co-lon (Figure 1 D3, J3 and C3).
The assessment of histological lesions in the duodenum of groups A, B and C depicted gradua-ted less severe lesions. In group C, the histologi-
cal changes were minor, characterized by mild to moderate attenuation of the mucosal height, fusion of the intestinal villi and moderate infiltration of the lamina propria with lymphocytes, macropha-ges, neutrophils and eosinophils (Figure 2 D-D1). The Goblet cells were uniformly distributed in the overlying epithelium in contrast to crypts and inte-stinal glands (Figure 2 D2). The immunopositivity for TLR4 on the duodenal epithelial surface and lamina propria in the groups treated with rifaximin depicted graduated lesser staining. In the group C, the mucosa of the duodenum showed a weak and multi-focal TLR4 immunoreactivity, mainly re-stricted to the overlying epithelium and superficial crypts (Figure 2 D3). One-way ANOVA test reve-aled significant difference regarding means duode-num villous height (F = 9.004, p < 0.001) between controls and groups receiving 5-FU, but no stati-stical difference between interventional groups (Fi-gure 3). The median mitotic index was significant-ly decreased in all groups receiving 5-FU (group A 0.18 ± 0.13, group B 0.12 ± 0.12, group C 0.23 ± 0.05, group D 0.18 ± 0.13) compared with con-
Figure 1. Microscopical findings of intestinal mucosa from experimental Wistar rats exposed to 5-fluorouracil-induced intesti-nal mucositis, group F. D – Duodenum, J - Jejunum, C - Colon. Images D-D1, J-J1, C-C1 corresponds to histological features of intestinal mucositis at the duodenal, jejunal and colonic levels in group C, hematoxylin and eosin staining. In PAS stained sec-tions (D2, J2, C2), marked reduction in goblet cell number over the villi and crypts was noticed (arrows), Periodic Acid Schiff (PAS) stain. Images D3, J3, C3 depict TLR4 immunoreactivity on the intestinal mucosa. Note a strong and diffuse immunostain-ing of TLR4 in the epithelial component and lamina propria of the intestinal mucosa of duodenum and jejunum.

Rifaximin and 5-fluorouracil induced gastrointestinal mucositis
4997
trol group (8.55 ± 0.83) (<0.001 {0.997/0.999/1/<0.001/0.978/0.997/<0.001/0.999/<0.001/<0.001}). Statistical analysis of graded microscopic degene-rative lesions depicted on the duodenum found no significant difference between F and A groups (U = 10, p = 0.188, - Mann-Whitney U test), but signifi-cant differences between F and B groups (U = 1.5, p = 0.007, - Mann-Whitney U test) and between F and C groups (U = 0, p = 0.003, - Mann-Whi-tney U test). Graded TLR4 immunopositivity on the surface epithelium of the duodenum was not significantly different between F and A groups (U = 7, p = 0.057, Mann-Whitney U test). Significant differences for graded TLR4 immunopositivity on the surface epithelium of the duodenum was no-ted comparing group F with group B (U = 2, p = 0.007, - Mann-Whitney U test) and group C (U = 1, p = 0.004, - Mann-Whitney U test). Statistical analysis for graded TLR4 expression on the lamina propria of the duodenum found significant diffe-rence between groups F and A (U = 4, p = 0.016, - Mann-Whitney U test), groups F and B (U = 2, p = 0.007, - U test) and groups F and C (U = 1, p = 0.004, - Mann-Whitney U test).
The assessment of histological lesions in the jejunum of groups A, B and C depicted gradua-ted less severe lesions. In group C, the jejunal mucosa presented mild reduction of villous hei-ght, minor cryptal distortion, mild upper villous degeneration and necrosis, moderate infiltration of lamina propria with lymphocytes, macropha-ges and scattered neutrophils and eosinophils (Figure 2 J-J1). In group C, the Goblet cells cor-responding to the jejunal mucosa were diffusely distributed, particularly in the upper third portion of the jejunal mucosa (Figure 2 J2). In all groups treated with rifaximin, the TLR4 immunoreacti-vity was gradually decreased on epithelial surfa-ce and lamina propria of jejunal mucosa, compa-red with group F. In the group C, small patches of TLR4 immunopositive cells were randomly present in the superficial area of the intestinal mucosa (Figure 2 J3). The one-way ANOVA test revealed significant difference regarding means jejunum villous height (F = 14.182, p < 0.001) between controls and group F (p < 0.001) and between groups F and C (p = 0.003) (Figure 4). The median mitotic index was significantly de-
Figure 2. Microscopical findings of intestinal mucosa from experimental Wistar rats exposed orally to 200 mg/kg rifaximin for three consecutive days and to 5-FU in the fourth day, group C. D – Duodenum, J - Jejunum, C - Colon. Images D-D1, J-J1, C-C1 depict histological features of attenuated intestinal mucositis at the duodenal (D-D1), jejunal (J-J1) and colonic (C-C1) levels, hematoxylin and eosin stain. Images D2, J2, C2 revealed the distribution of PAS positive Goblet cells (arrow) in the in-testinal mucosa, Periodic Acid-Schiff (PAS) stain. Images D3, J3, C3 correspond to the TLR4 immunopositive cells at different levels of the rat intestinal mucosa. Note the weak immunoreaction of the intestinal mucosa of duodenum and jejunum (arrows).

L. Ciobanu, M. Tantau, S. Valean, A. Parau, I. Bedecean, R. Mîrleneanu, C. Berce, C. Catoi, M. Taulescu
4998
creased in all groups receiving 5-FU (group A 0.08 ± 0.08, group B 0.05 ± 0.05, group C 0.12 ± 0.15, group D 0.05 ± 0.08) compared with con-trol group (10.03 ± 0.72) (< 0.001 {1/1/1/<0.001/0.995/1/<0.001/0.995/< 0.001/< 0.001}). The statistical analysis of graded microscopic dege-nerative lesions of the jejunum depicted no si-gnificant differences between F and A groups (U = 10, p = 0.191, Mann-Whitney U test), and F and B groups (U = 4.5, p = 0.027, Mann-Whit-ney U test), but significant differences between F and C groups (U = 0, p = 0.004, Mann-Whit-ney U test). Graded TLR4 immunopositivity on the epithelial lining of jejunum was not signifi-cantly different between F and A groups (U = 15, p = 0.523, Mann-Whitney U test) and F and B groups (U = 5, p = 0.023, Mann-Whitney U test). A significant difference was noted comparing graded TLR4 immunopositivity of the epithelial surface of the jejunum between groups F and C (U = 2.5, p = 0.006, Mann-Whitney U test). The statistical analysis for graded TLR4 expression on the lamina propria of the jejunum found no significant difference between F and A groups (U = 6, p = 0.030, Mann-Whitney U test), but signi-ficant differences between F and B groups (U = 0, p = 0.003, Mann-Whitney U test) and F and C groups (U = 2, p = 0.007, Mann-Whitney U test).
The assessment of histological lesions in the colonic mucosa of groups pretreated with rifa-
ximin found mild lesions in groups A and C and moderate lesions in group B. (Table I). Hydro-pic degeneration and attenuation of overlying colonic epithelium, mild edema and scant in-flammatory cells within superficial lamina pro-pria were identified in group C (Figure 2 C-C1). The Goblet cells were diffusely and uniformly distributed in the colonic mucosa (Figure 2 C2). In groups C the colonic mucosa showed a weak and patch immunopositivity for TLR4 (Figure 2 C3). Statistical analysis of graded microsco-pic degenerative lesions on the colonic mucosa found no significant difference between groups F and B (U = 11.5, p = 0.291, Mann-Whitney U test), but significant difference between F and A groups (U = 0, p = 0.004, Mann-Whitney U test) and between F and C groups (U = 0, p = 0.004, Mann-Whitney U test). Graded TLR4 immuno-positivity on the colonic surface epithelium was not significant different between F and A groups (U = 13.5, p = 0.423, Mann-Whitney U test), F and B groups (U = 13.5, p = 0.434, Mann-Whi-tney U test) and groups F and C (U = 13.5, p = 0.423, Mann-Whitney U test). Statistical analy-sis for graded TLR4 expression on lamina pro-pria of the colon found no significant difference between F and B groups (U = 10, p = 0.092, Mann-Whitney U test), but significant differen-ce between F and A groups (U = 4, p = 0.014, Mann-Whitney U test) and F and C groups (U = 4, p = 0.014, Mann-Whitney U test).
Figure 3. Duodenum villous height comparison between groups.
Figure 4. Jejunum villous height comparison between groups.

Rifaximin and 5-fluorouracil induced gastrointestinal mucositis
4999
Discussion
After 5-FU administration, gastrointestinal mu-cositis is most prominent in the small intestine but it also occurs in the large intestine1. Our experi-mental model depicted severe histological lesions at jejunum and duodenal level in animals exposed to 5-FU; moderate lesions were present on colo-nic mucosa in animals exposed to 5-FU. As severe lesions were depicted in sites where the gut bacte-rial load is lower, the interplay between mucosal barrier, microbiota and immune system might be disrupted differently by 5 FU throughout the inte-stine. A higher ratio of proapoptotic to antiapop-totic genes in the small intestine than in the large intestine correlated with rapid changes in gene expression following chemotherapy might par-tially explain these differences1,16. Administration of 5-FU was associated with changes in the inte-stinal microbiota at different sites of the gut4,5. A study by von Bultzingslowen et al4 demonstrated that 5-FU administration (6 × 50 mg/kg) in Lewis rats caused an increase in the number of faculta-tive anaerobes in the large intestine. A later study by Stringer et al5 showed no significant findings; however, peaks were observed following 5-FU administration (150 mg/kg, single dose) in E. coli at 48 h, Clostridium spp. at multiple time points, and Staphylococcus spp. at 24 h. Decreases were observed in Lactobacillus spp. at 24 h and Ente-rococcus spp. at 2 h – 48 h following treatment5. The role of microbiota in gastrointestinal muco-sitis pathogenesis was argued by the studies that proved the beneficial role of probiotics8,17. Yeung et al9 demonstrated that Lactobacillus casei va-riety rhamnosus or Lactobacillus acidophilus and Bifidobacterium bifidum ameliorated chemothe-rapy-induced intestinal mucositis in a mouse mo-del. Lactobacillus acidophilus also improved the inflammatory and functional aspects of intestinal mucositis induced by 5-FU11. Conflicting resul-ts were reported about Saccharomyces boulardii regarding the inflammation and dysfunction cor-responding to the 5-FU-induced gastrointestinal mucositis18,19.
This experimental study proposed a different approach for microbiota modulation, by using ri-faximin, a non-absorbable derivative of rifamycin that proved an effective antibiotic by inhibiting bacterial ribonucleic acid synthesis. In vitro and in vivo studies found that rifaximin possessed activity against many enteric pathogens Aeromo-nas, Campylobacter, Clostridium, enteroaggrega-tive Escherichia coli, enterohemorrhagic E. coli,
enteroinvasive E. coli, Plesiomonas shigelloides, Salmonella, Shigella spp., Serratia spp. and Vi-brio spp.20. An antiinflammatory effect of rifaxi-min on the intestinal mucosa was also documen-ted in previous studies, mostly related to irritable bowel syndrome21. The clinical use of rifaximin was documented in traveler’s diarrhea22 hepatic encephalopathy23, irritable bowel syndrome with diarrhea24. Other beneficial effects were proven in inflammatory bowel disease25, in preventing recurrence of acute diverticulitis26 and in an expe-rimental model of NSAIDs enteropathy27.
To our knowledge, this is the first reported stu-dy that investigated the different doses of rifaxi-min in preventing enteric lesions induced by 5-FU in Wistar rats.
In our experimental model the oral administra-tion of rifaximin for three consecutive days, prior to 5-FU administration, proved efficient in limi-ting the small bowel lesions. This effect seemed dose dependent at different sites of the gut.
Rifaximin administered orally in a dose of 50 mg/kg for three days had little effects on seve-re lesions induced by 5-FU in the duodenal and jejunal mucosa. But at this dose rifaximin proved significant efficiency in limiting the moderate co-lonic lesions induced by 5-FU and also in redu-cing the immunopositivity of TLR4 on the lamina propria of the colon.
Three doses of 100 mg/kg of rifaximin signifi-cantly reduced the degree of mucositis lesions in duodenum and also the extent of immunopositivi-ty of TLR4 on epithelial cells and lamina propria. This dose also reduced the severity of the lesions in the jejunum, but had little influence of colonic mucosa lesions.
A higher dose of rifaximin: 200 mg/kg daily for three consecutive days significantly decreased the severity of the lesions in the duodenum, jejunum and colon and the immunoreactivity for TLR 4 on epithelial surface and in lamina propria.
A limit of our study consists in the lack of analysis of the effect of rifaximin on bacterial population at different levels of the intestine. Based on previous experimental rat studies, rifaximin administration reduced at the di-stal part of the ileum tha bacterial load of the Clostridiaceae, Erysipelotrichaceae, and Pep-tostreptococcaceae and striking increased the Lactobacillaceae (identified as Lactobacillus spp.). Furthermore, a marked reduction in the number of segmented filamentous bacteria was reported. 21. These changes in microbial com-munities may contribute to the antiinflamma-

L. Ciobanu, M. Tantau, S. Valean, A. Parau, I. Bedecean, R. Mîrleneanu, C. Berce, C. Catoi, M. Taulescu
5000
tory effects of rifaximin on the intestinal mu-cosa21. In our study, the effect on inflammation was assessed throughout immunopositivity for TLR4 on epithelial surface and lamina propria on the duodenum, jejunum, and colon. The de-creased in immunoreactivity for TLR4 accom-panied the reduction of the histological scores. The intestinal microbiota may play a key role in intestinal mucositis by the activation of TLR signaling, especially TLR2, TLR4 and TLR5. Once activated by intestinal microbiota, TLRs can also up-regulate NFκB through complex signaling pathways6, further compounding the inflammatory response through the generation and amplification of TNF-α, IL-1β, and IL-62.
Different doses of rifaximin proved efficient in limiting the effects of 5-FU at different sites of the intestinal tract in our study. This observation mi-ght be related to the different bioavailability of ri-faximin throughout the gut. In vitro studies shown that the solubility of rifaximin is 70- to 120-fold greater in bile acids and rifaximin exhibits con-centration dependent antibiotic effect in bile28. Rifaximin is more active in upper gastrointestinal tract because of the increased bioavailability in the small intestine compared to the aqueous me-dium of the colon28. The different degree of le-sions induced by 5-FU: severe on duodenum and jejunum site and moderate on colonic mucosa mi-ght partially explain the results.
In our study, 200 mg/kg of rifaximin for three consecutive days administered orally proved effi-cient in limiting severe lesions induced by 5-FU on the small intestine and moderate lesions indu-ced by 5-FU on the large intestine. Interestingly 50 mg/kg of rifaximin had similar effects on colo-nic lesions induced by chemotherapy, but not 100 mg/kg. On the colon, the decrease of histological lesions in groups receiving 50 mg/kg or 200 mg/kg rifaximin was accompanied by the reduction of TLR4 immunopositivity on the lamina propria. The immunopositivity for TLR4 on surface colo-nic epithelium was similar in all groups receiving 5-FU (A, B, C and F), suggesting that 5-FU might induce the expression of TLR4 on colonic surfa-ce epithelial cells independent of the microbiota composition.
Conclusions
The most severe histological lesions indu-ced by 5 FU were depicted in the jejeunal and duodenal mucosa. Pretreatment with 200 mg/kg
of rifaximin for three consecutive days proved efficient in preventing degenerative mucosal le-sions induced by 5-FU in the duodenum, jeju-num and colon.
AcknowledgementsThis work was supported by the Partnership in Priority Areas Programme-PNII, developed with the support of MEN-UE-FISCDI (Project No.154 [PN-II-PT- PCCA- 2013-4-0743].
Conflict of InterestsThe Authors declare that they have no conflict of interests.
References
1) SoniS ST, ElTing lS, KEEfE D, PETErSon DE, SchubErT M, hauEr-JEnSEn M, bEKElE bn, rabEr-DurlachEr J, DonnElly JP, rubEnSTEin Eb. Perspectives on cancer therapy-induced mucosal injury: pathogenesis, measurement, epidemiology, and consequences for patients. Cancer 2004; 100: 1995-2025.
2) SoniS ST. The pathobiology of mucositis. Nat Rev Cancer 2004; 4: 277-284.
3) STringEr aM. Interaction between host cells and microbes in chemotherapy-induced mucositis. Nutrients 2013; 5: 1488-1499
4) Von bulTzingSlowEn i, aDlErbErTh i, wolD aE, Dah-lEn g, JonTEll M. Oral and intestinal microflora in 5-fluorouracil treated rats, translocation to cervi-cal and mesenteric lymph nodes and effects of probiotic bacteria. Oral Microbiol Immunol 2003; 18: 278-284.
5) STringEr aM, gibSon rJ, logan rM, bowEn JM, yEoh aS, haMilTon J, KEEfE DM. Gastrointestinal microflora and mucins may play a critical role in the development of 5-fluorouracil-induced gastrointestinal mucositis. Exp Biol Med (Maywood) 2009; 234: 430-441.
6) cario, E. Bacterial interactions with cells of the intestinal mucosa: Toll-like receptors and NOD2. Gut 2005; 54: 1182-1193.
7) SaEguSa y, ichiKawa T, iwai T, goSo y, oKayaSu i., iKE-zawa T, ShiKaMa n, SaigEnJi K, iShihara K. Changes in the mucus barrier of the rat during 5-fluorou-racil-induced gastrointestinal mucositis. Scand J Gastroenterol 2008; 43: 59-65.
8) PriScianDaro lD, gEiEr MS, buTlEr rn, cuMMinS ag, howarTh gS. Evidence supporting the use of pro-biotics for the prevention and treatment of che-motherapy-induced intestinal mucositis. Crit Rev Food Sci Nutr 2011; 51: 239-247.
9) yEung cy, chan wT, Jiang cb, chEng Ml, liu cy, chang Sw, chiang chiau JS, lEE hc. Amelioration of chemotherapy-induced intestinal mucositis by orally administered probiotics in a mouse model. PLoS One 2015; 10: e0138746.
10) yuan KT, yu hl, fEng wD, chong P, yang T, XuE cl, yu M, Shi hP. Bifidobacterium infantis has a beneficial

Rifaximin and 5-fluorouracil induced gastrointestinal mucositis
5001
effect on 5-fluorouracil-induced intestinal mucositis in rats. Benef Microbes 2015; 6: 113-118.
11) JuSTino Pf, MElo lf, noguEira af, MoraiS cM, MEnDES wo, franco aX, Souza EP, ribEiro ra, Souza Mh, Soa-rES PM. Regulatory role of Lactobacillus acidophilus on inflammation and gastric dysmotility in intestinal mucositis induced by 5-fluorouracil in mice. Cancer Chemother Pharmacol 2015; 75: 559-567.
12) hooVEr ww, gErlach Eh, hoban DJ, ElioPouloS gM, PfallEr Ma, JonES rn. Antimicrobial activity and spectrum of rifaximin, a new topical rifamycin deri-vative. Diagn Microbiol Infect Dis 1993; 16: 111-118.
13) howarTh gS, franciS gl, cool Jc, Xu X, byarD rw, rEaD lc. Milk growth factors enriched from chee-se whey ameliorate intestinal damage by metho-trexate when administered orally to rats. J Nutr 1996; 126: 2519-2530.
14) lE ManDaT SchulTz a, bonnarD a, barrEau f, aigrain y, PiErrE-louiS c, bErrEbi D, PEuchMaur M. Expres-sion of TLR-2, TLR-4, NOD2 and pNF-kappaB in a neonatal rat model of necrotizing enterocolitis. PLoS One 2007; 2: e1102.
15) froloVa l, DraSTich P, roSSMann P, KliMESoVa K, TlaSKaloVa-hogEnoVa h. Expression of Toll-like receptor 2 (TLR2), TLR4, and CD14 in biopsy samples of patients with inflammatory bowel dise-ases: upregulated expression of TLR2 in terminal ileum of patients with ulcerative colitis. J Histo-chem Cytochem 2008; 56: 267-274.
16) bowEn JM, gibSon rJ, TSyKin a, STringEr aM, logan rM, KEEfE DM. Gene expression analysis of multiple gastrointestinal regions reveals activation of com-mon cell regulatory pathways following cytotoxic chemotherapy. Int J Cancer 2007; 121: 1847-1856.
17) PriScianDaro lD, gEiEr MS, buTlEr rn, cuMMinS ag, howarTh gS. Probiotic factors partially improve para-meters of 5-fluorouracil-induced intestinal mucositis in rats. Cancer Biol Ther 2011; 11: 671-677.
18) Maioli Tu, DE MElo SilVa b, DiaS Mn, PaiVa nc, car-DoSo Vn, fErnanDES So, carnEiro cM, DoS SanToS MarTinS f, DE VaSconcEloS gEnEroSo S. Pretreatment with Saccharomyces boulardii does not prevent the experimental mucositis in Swiss mice. J Ne-gat Results Biomed 2014; 13: 6.
19) JuSTino Pf, MElo lf, noguEira af, coSTa JV, SilVa lM, SanToS cM, MEnDES wo, coSTa Mr, franco
aX, liMa aa, ribEiro ra, Souza Mh, SoarES PM. Treatment with Saccharomyces boulardii re-duces the inflammation and dysfunction of the gastrointestinal tract in 5-fluorouracil-induced intestinal mucositis in mice. Br J Nutr 2014; 111: 1611-1621.
20) DuPonT hl. Review article: the antimicrobial ef-fects of rifaximin on the gut microbiota. Aliment Pharmacol Ther 2016; 43: 3-10.
21) gao J, gillillanD Mg 3rD, owyang c. Rifaximin, gut microbes and mucosal inflammation: unraveling a complex relationship. Gut Microbes 2014; 5: 571-575.
22) DE la cabaDa bauchE J, DuPonT hl. New Develop-ments in Traveler’s Diarrhea. Gastroenterol Hepa-tol (N Y) 2011; 7: 88-95.
23) baJaJ JS. Review article: potential mechanisms of action of rifaximin in the management of he-patic encephalopathy and other complications of cirrhosis. Aliment Pharmacol Ther 2016; 43: 11-26.
24) PiMEnTEl M. Review article: potential mechani-sms of action of rifaximin in the management of irritable bowel syndrome with diarrhoea. Aliment Pharmacol Ther 2016; 43: 37-49.
25) gionchETTi P, rizzEllo f, VEnTuri a, ugolini f, roS-Si M, brigiDi P, JohanSSon r, fErriEri a, Poggioli g, caMPiEri M. Review-antibiotic treatment in inflam-matory bowel disease: rifaximin, a new possible approach. Eur Rev Med Pharmacol Sci 1999; 3: 27-30.
26) TurSi a, EliSEi w, giorgETTi gM, inchingolo cD, nEnna r, Picchio M, Maiorano M, PEnna a, lEcca Pg, branDiMarTE g. Effectiveness of different the-rapeutic strategies in preventing diverticulitis re-currence. Eur Rev Med Pharmacol Sci 2013; 17: 342-348.
27) ciobanu l, TaulEScu M, PrunDuS r, Diaconu b, an-DrEica V, caToi c, PaScu o, TanTau M. Effects of rifa-ximin on indomethacin-induced intestinal damage in guinea-pigs. Eur Rev Med Pharmacol Sci 2014; 18: 344-351.
28) DarKoh c, lichTEnbErgEr lM, aJaMi n, Dial EJ, Jiang zD, DuPonT hl. Bile acids improve the antimicro-bial effect of rifaximin. Antimicrob Agents Che-mother 2010; 54: 3618-3624.





























