Embed Size (px)
Citation preview
Review of Primary
Intracerebral Hemorrhage
Réza Behrouz, DOAssistant Professor of Neurology
University of South Florida College of Medicine

85%ISCHEMIC
15%HEMORRHAGIC
STROKE
HEMORRHAGIC STROKE
1/3Subarachnoid
2/3Intracerebral

DEFINITION
Acute extravasation of blood into the brain
parenchyma
EPIDEMIOLOGY
•
More common in men–
Subarachnoid hemorrhage more common in women
•
Risk increases dramatically with age–
Risk doubles every 10 years after age 35
–
Mean age 60
•
2X in Blacks, Asians and Hispanics than Whites
Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Stroke.
1999;30:905-915

EPIDEMIOLOGY
•
US prevalence
37,000 ‐
52,000
•
US annual death rate
20,000
•
US overall annual cost $ 6 Billion
Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Stroke.
1999;30:905-915

Roosevelt
Lenin
Al-Sabah
Sharon

PRESENTATION
•
Sudden onset focal neurological deficit–
85% during active
hours of the day
•
Smooth progression over time–
TIAs unusual
•
Elevated blood pressure (90%)–
Regardless of a pre-existing history of hypertension
Caplan LR. Intracerebral Hemorrhage.
Caplan’s Stroke: A Clinical Approach. Third Edition. 2000.Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Stroke.
1999;30:905-915.

PRESENTATION
•
Nausea & emesis
~ 55 %
•
Early or abrupt change in LOC
~ 50 %
•
Headache ~ 40 %
•
Seizures
~ 10%
Caplan LR. Intracerebral Hemorrhage.
Caplan’s Stroke: A Clinical Approach. Third Edition. 2000.Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage. Stroke.
1999;30:905-915.

PRIMARY SECONDARY
Unrelated to an underlying congenital or acquired brain lesions or
abnormalities
Related to
a pre-existing intracranial abnormality
Manno EM et al. Emerging Medical and Surgical Management Strategies in the Evaluation and Treatment of Intracerebral Hemorrhage. Mayo Clin Proc. March 2005;80(3):420-433.

PRIMARY HypertensionHypertensionCerebral Amyloid AngiopathyAnticoagulantsThrombolyticsDrug UseBleeding Diathesis
SECONDARYVascular MalformationsAneurysmsIntracranial NeoplasmCerebral InfarctionsVenous InfarctionMoyamoya DiseaseCerebral Vasculitis
Manno EM et al. Emerging Medical and Surgical Management Strategies in the Evaluation and Treatment of Intracerebral Hemorrhage. Mayo Clin Proc. March 2005;80(3):420-433.

Hypertension70%
AmyloidAngiopathy
20%
Anticoagulants (8%)
Drug Use
Bleeding Diathesis

HYPERTENSIVE HEMORRHAGE
•
HTN: the most important risk factor
•
Exact quantification of risk difficult to ascertain–
Smoking and excessive alcohol can increase the risk
•
Treatment of HTN decreases risk of ICH by
~ 50%
•
Recurrent risk of HH is 1-2% per year–
If blood pressure is well controlled
Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.Hypertension Detection and Follow-up Program Cooperative Group. Five year findings.
JAMA
1982;247:633-8.
HYPERTENSIVE HEMORRHAGE
•
Rupture of deep-penetrating arteries
–
Originate from major cerebral arteries
–
Unprotected from direct effects of HTN
•
Diameter
–
100 -
600 μm
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

HYPERTENSIVE HEMORRHAGE
StriatumThalamus
Pons
Lobar
Cerebellum

HYPERTENSIVE HEMORRHAGE
•
Charcot -
Bouchard aneurysms–
Not seen in all cases
•
Lipohyalinosis –
More plausible explanation
Qureshi AI et al. Spontaneous Intracerebral Hemorrhage.
N Eng J Med.
Vol 344, No 19. May 10, 2001.Manno EM et al. Emerging Medical and Surgical Management Strategies in the Evaluation and Treatment of Intracerebral Hemorrhage. Mayo Clin Proc. March 2005;80(3):420-433.

AMYLOID ANGIOPATHY
•
Different than systemic amyloidosis
•
~ 20 % of ICH cases > 70
•
Risk with advancing age
•
Lobar or cortical
•
Multiple
•
Recurrent –
Rate 5-15% per year
•
Less severe than HH
•
History of cognitive decline
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

AMYLOID ANGIOPATHY
•
Diagnosis at autopsy
•
Lobar micro-hemorrhages
•
Most are clinically silent
•
Strongly suggests the diagnosis–
Age > 70–
History of lobar hemorrhage
•
Reflects disease severity and recurrence risk
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

AMYLOID ANGIOPATHY
Beta/A4-amyloid in vessel Fluorescent stained wall unstained
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

COAGULOPATHY
•
Warfarin–
Increases risk 5 -
10 times
–
AR 0.3 -
1.7 % per year–
Doubles the mortality of ICH
•
Aspirin–
AR 0.2 % per year
•
Bleeding disorders
•
Mostly lobar
•
Hemorrhage develops gradually
Hart RG et al. Oral anticoagulants and intracerebral hemorrhage. Facts and hypotheses.
Stroke 1995. 26:1471-77.Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.
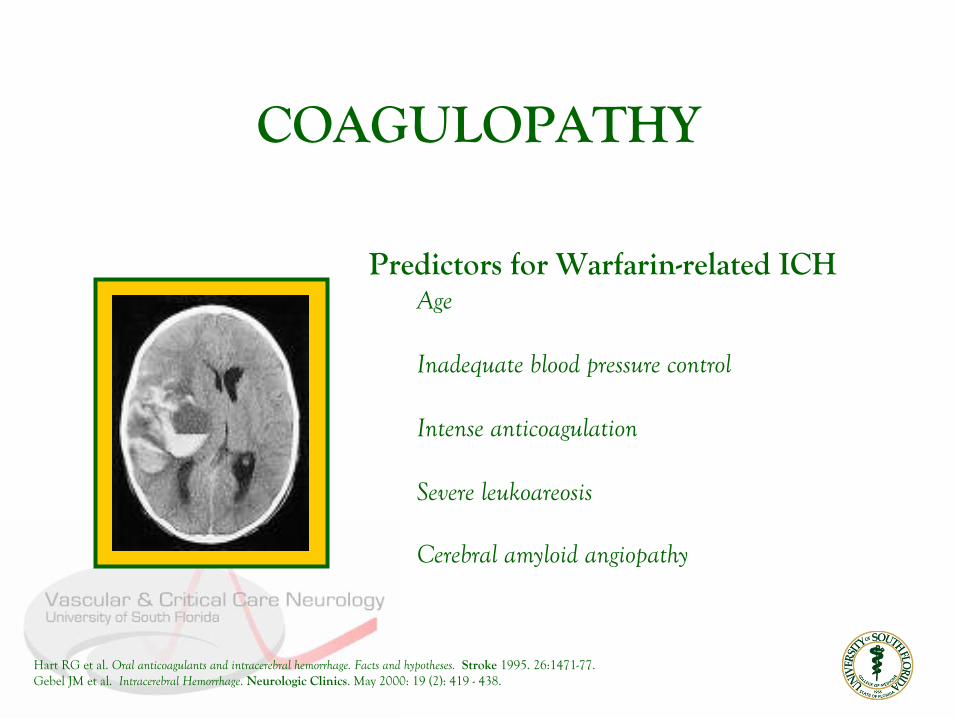
COAGULOPATHY
Predictors for Warfarin-related ICHAge
Inadequate blood pressure control
Intense anticoagulation
Severe leukoareosis
Cerebral amyloid angiopathy
Hart RG et al. Oral anticoagulants and intracerebral hemorrhage. Facts and hypotheses.
Stroke 1995. 26:1471-77.Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.
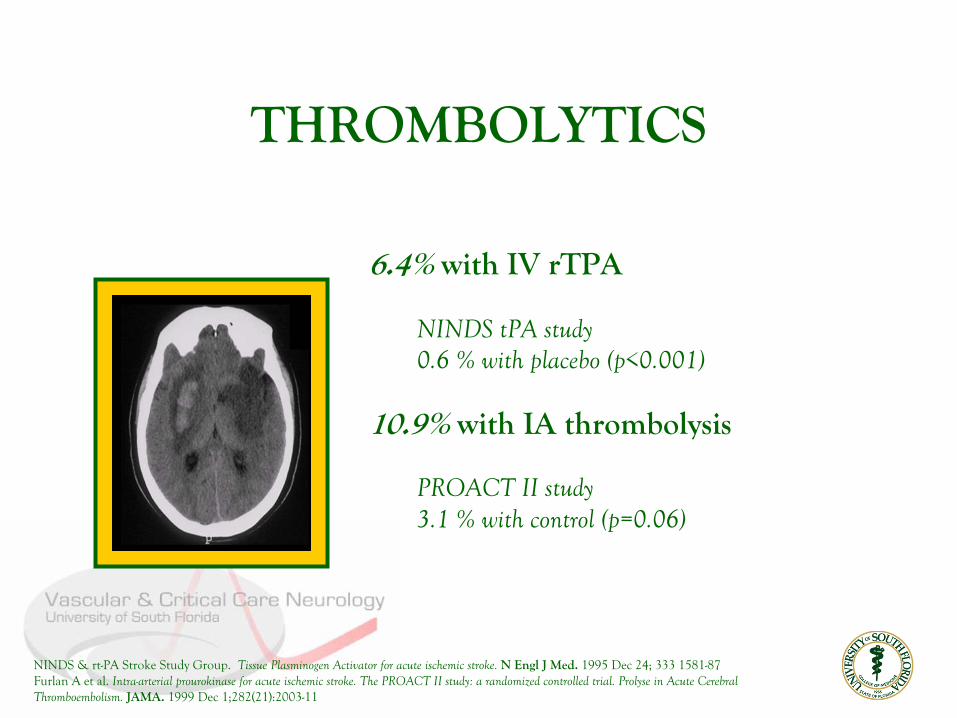
THROMBOLYTICS
6.4% with IV rTPA
NINDS tPA
study0.6 % with placebo (p<0.001)
10.9% with IA thrombolysis
PROACT II study3.1 % with control (p=0.06)
NINDS & rt-PA Stroke Study Group. Tissue Plasminogen
Activator for acute ischemic stroke.
N Engl
J Med.
1995 Dec 24; 333 1581-87Furlan
A et al. Intra-arterial prourokinase
for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse
in Acute Cerebral Thromboembolism. JAMA. 1999 Dec 1;282(21):2003-11

THROMBOLYTICS
Influential factorsNIHSS > 20
Age > 75
Edema and mass effect on baseline CT
Initial CT hypo-attenuation > 33% of MCA distribution
NINDS tPA
Study Group. Intracerebral
Hemorrhage After Intravenous t-PA Therapy for Ischemic Stroke. Stroke.
1997;28:2109-2118.Larrue
V et al. Risk factors for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen
activator: a secondaryanalysis of the European-Australian Acute Stroke Study (ECASS II).
Stroke 2001 Feb;32(2):438-41.

DRUGS
• 1% of all cases
• CulpritsCocaine, Amphetamines, Ephedrines
• Mainly young patients
• Predisposing factorsHypertension, AVM
Gebel JM et al. Intracerebral Hemorrhage. Neurologic Clinics. May 2000: 19 (2): 419 -
438.
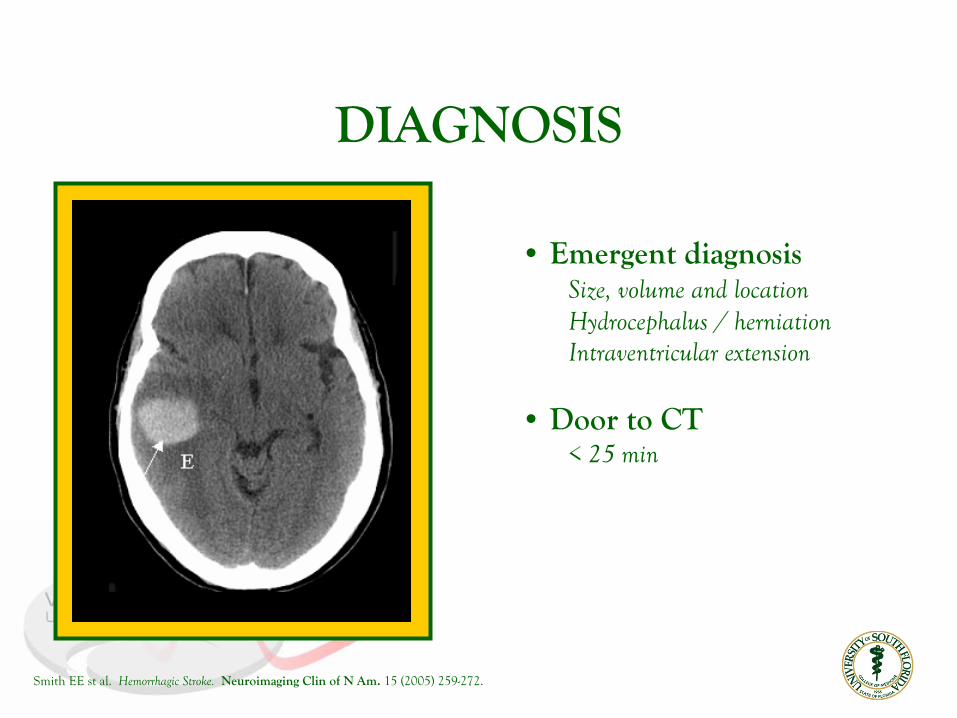
DIAGNOSIS
• Emergent diagnosisSize, volume and locationHydrocephalus / herniationIntraventricular extension
• Door to CT< 25 min
Smith EE st al. Hemorrhagic Stroke.
Neuroimaging Clin of N Am.
15 (2005) 259-272.

DIAGNOSIS -
CT
•Disappears Within 2 to 4 weeks
• Severe anemia Reduces attenuation
Smith EE st al. Hemorrhagic Stroke.
Neuroimaging Clin of N Am.
15 (2005) 259-272.

DIAGNOSIS -
MRI
• LimitationsTimePatient monitoring
• RecommendedAlmost all patients with ICH
• Structural abnormalities
• Time course
Smith EE st al. Hemorrhagic Stroke.
Neuroimaging Clin of N Am.
15 (2005) 259-272.
ACUTE MANAGEMENT
!StopHemorrhage
Stabilize Hemodynamics
Complications

COAGULOPATHY
•
Successful reversal
–
INR < 1.4
•
Time is important
–
Early reversal of coagulopathy is critical
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

COAGULOPATHY
Repeat INR in 4 hours Administer FFP if >1.4 -
otherwise every 6 hours
Vitamin K10 mg IV
FFP15 mL/kg
6 units
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

COAGULOPATHY
Heparin reversalProtamine sulfate 10-50 mg IV over 1-3 minutesOR 1 mg for every 100 units of Heparin
Platelet transfusion4-8 unitsGoal platelet count > 100,000Use in ASA/Clopidogrel-related ICH controversial
Mayer SA et al. Treatment of intracerebral hemorrhage. Lancet Neurology
2005;4:662-72.

BLOOD PRESSURE
MAP
< 130 mmHg
With a history of hypertension
Ideally between 90 to 110 mmHgCPP > 70 mmHg
AgentsNicardipine (5-15 mg/hr), Labetolol (2-8 mg/min), EsmololHydralazine and Nitroprusside NOT recommended in acute ICH
Mayer SA et al. Optimizing blood pressure in neurological emergencies.
Neurocritical Care.
2004. 1: 287-99Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage.
Stroke.
1999;30:905-915
COMPLICATIONS
• Hematoma expansionIntra-parenchymal Intra-ventricular
•Hydrocephalus
•Edema and herniation
• Seizures
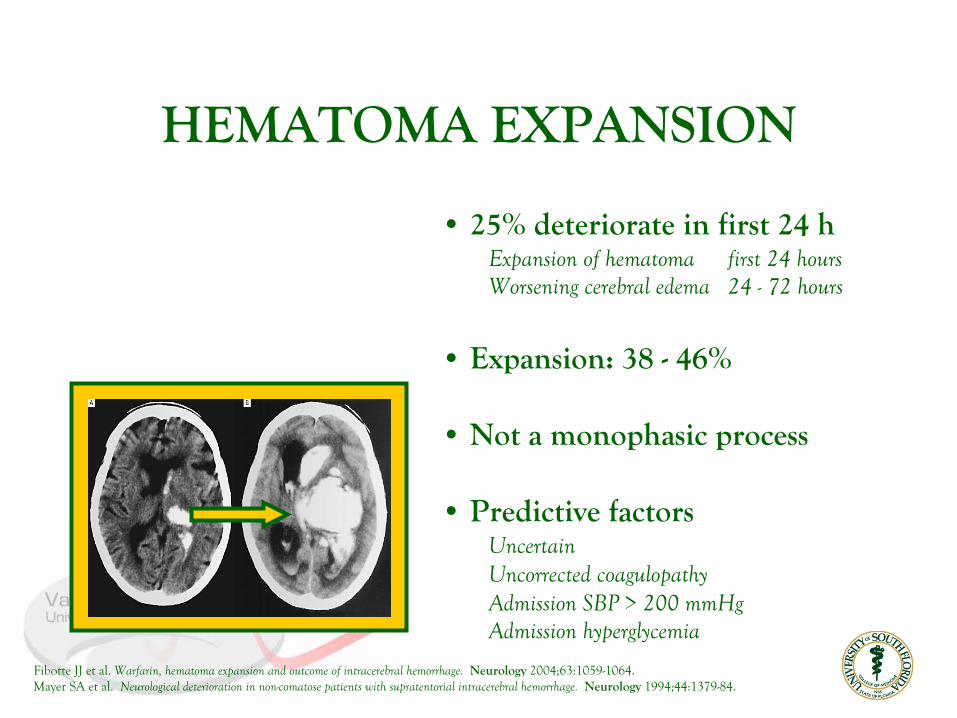
HEMATOMA EXPANSION
• 25% deteriorate in first 24 hExpansion of hematoma first 24 hoursWorsening cerebral edema
24 -
72 hours
• Expansion: 38 -
46%
• Not a monophasic process
• Predictive factors UncertainUncorrected coagulopathyAdmission SBP > 200 mmHgAdmission hyperglycemia
Fibotte JJ et al. Warfarin, hematoma expansion and outcome of intracerebral hemorrhage.
Neurology
2004;63:1059-1064.Mayer SA et al. Neurological deterioration in non-comatose patients with supratentorial intracerebral hemorrhage.
Neurology 1994;44:1379-84.

INTRAVENTRICULAR EXTENSION
• 20 - 40%Deep hemorrhagesLarge Hemorrhages
• SymptomsMeningismusAlteration of consciousness
• Volume of IVEProportionally affects mortality
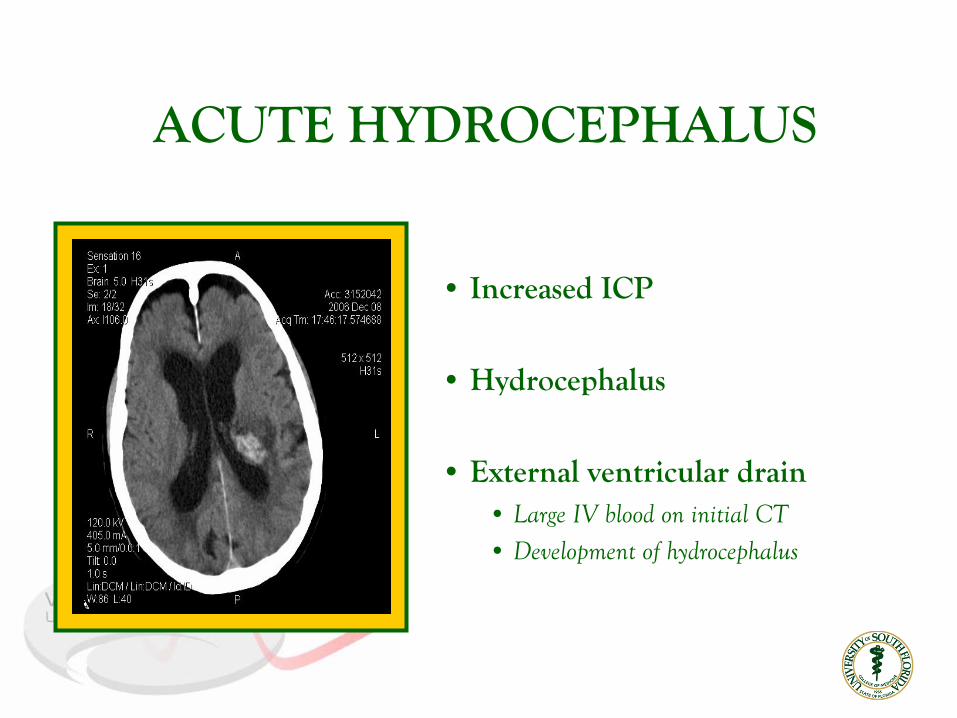
ACUTE HYDROCEPHALUS
• Increased ICP
• Hydrocephalus
• External ventricular drain• Large IV blood on initial CT• Development of hydrocephalus

EDEMA
•
Chief complication in the first few days
• Can increase by 75%
• Increased mass effect
• Increased ICP
• Herniation
Qureshi AI et al. Spontaneous Intracerebral Hemorrhage.
N Eng J Med.
Vol 344, No 19. May 10, 2001Gebel JM et al. Relative edema volume is a predictor of outcome in patients with
hyperacute intracerebral hemorrhage. Stroke 2002; 33:2636 -
41.
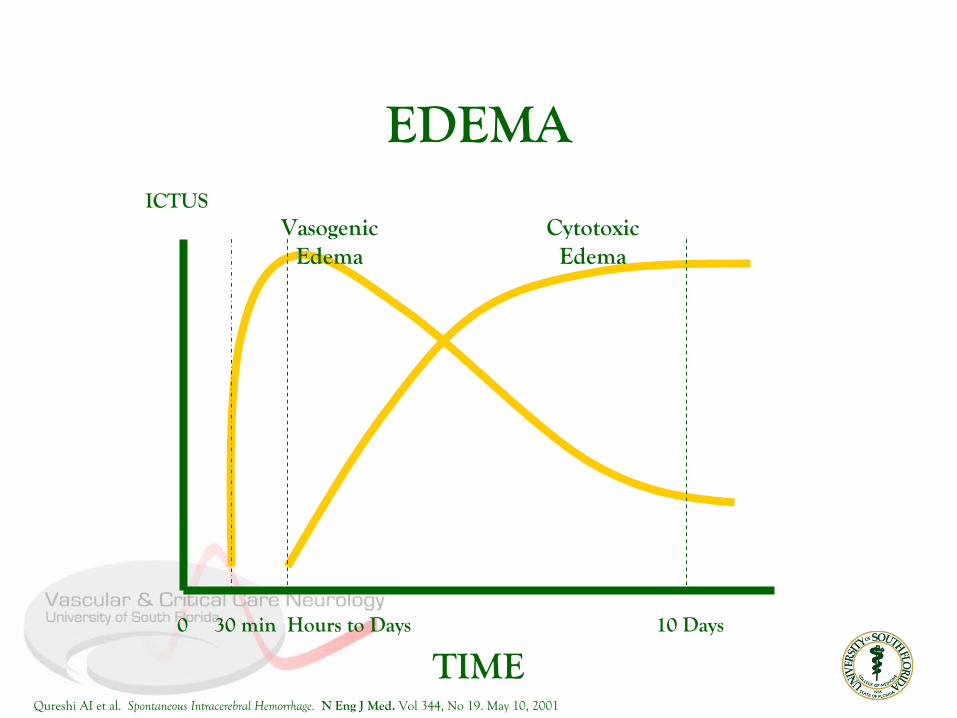
EDEMA
0 30 min Hours to Days
10 Days
TIME
ICTUSVasogenic
EdemaCytotoxic
Edema
Qureshi AI et al. Spontaneous Intracerebral Hemorrhage.
N Eng J Med.
Vol 344, No 19. May 10, 2001
EDEMA / HERNIATION
•HyperventilationInitial mode of therapy to gain immediate controlTransient
effect
• 20% Mannitol IV0.5 to 1.0 g/kg IV bolus every 4 hours
• Hypertonic Saline IV3% (250 mL), 7.5% (100 mL) and 10% (75 mL) = 7.5 g NaCl
Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage.
Stroke.
1999;30:905-915

EDEMA / HERNIATION
• Pharmacological comaPentobarbital
•Do not use corticosteroids
Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage.
Stroke.
1999;30:905-915
SEIZURES
• Presenting symptom in 10%
• Risk of development of epilepsy
5%
• Non-convulsing status epilepticus
1-2 %
EEG indicated in prolonged comatose states
• Lobar hemorrhage An independent risk factor for early seizures
Vespa PM et al. Acute seizures after intracerebral hemorrhage.
Neurology
2003;60:1441-46Passero S et al. Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia. 2002;431175-80.
SEIZURES• Early seizure
Early < 14 daysMore commonTaper AED off after one month if seizure free
• Late seizuresLate > 14 daysMay need lifetime AED therapy
• AED prophylaxis may be beneficialNo randomized trial has addressed the efficacyUse for lobar ICH Taper off after one month if seizure free
Vespa PM et al. Acute seizures after intracerebral hemorrhage.
Neurology
2003;60:1441-46Passero S et al. Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia. 2002;431175-80.

EARLY SURGICAL EVACUATION
• May be performed as a life-saving measure
• Benefit in long-term outcome is questionableTen studies (5 randomized) Conflicting resultsOverall, no proof that early surgery is superior to medical therapy
• Over 7000 annual surgeries are performed
worldwide
Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage.
Stroke.
1999;30:905-915

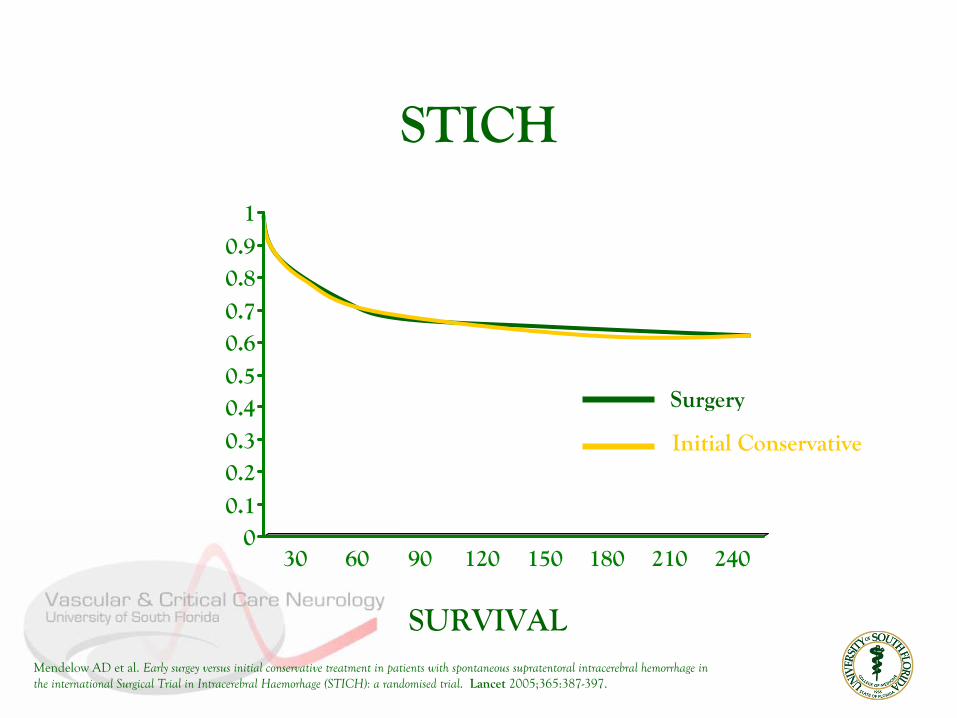
Mendelow AD et al. Early surgey versus initial conservative treatment in patients with spontaneous supratentoral intracerebral hemorrhage in the international Surgical Trial in Intracerebral Haemorhage (STICH): a randomised trial. Lancet
2005;365:387-397.
Randomized, parallel groupPrimary ICH -
GCS > 5 and hematoma diameter > 2 cm
1033 patients with supra-tentorial hemorrhage“Uncertainty principle”1/2 allocated to early surgery + medical therapySurgery within 72 hours1/2 allocated to initial medical therapyBaseline characteristics well-matched
Outcome assessed at 6 months months
STICH
Mendelow AD et al. Early surgey versus initial conservative treatment in patients with spontaneous supratentoral intracerebral hemorrhage in the international Surgical Trial in Intracerebral Haemorhage (STICH): a randomised trial. Lancet
2005;365:387-397.
00.10.20.30.40.50.60.70.80.9
1
30 60 90 120 150 180 210 240
STICH
Mendelow AD et al. Early surgey versus initial conservative treatment in patients with spontaneous supratentoral intracerebral hemorrhage in the international Surgical Trial in Intracerebral Haemorhage (STICH): a randomised trial. Lancet
2005;365:387-397.
SURVIVAL
Surgery
Initial Conservative

Mendelow AD et al. Early surgey versus initial conservative treatment in patients with spontaneous supratentoral intracerebral hemorrhage in the international Surgical Trial in Intracerebral Haemorhage (STICH): a randomised trial. Lancet
2005;365:387-397.
STICH
Favorable outcome = BI >95 and mRS <2
Neither the absolute (2%) nor the relative benefit (10%)of early surgery was significant (p=0.414).
EARLY SURGICAL EVACUATION
•worldwide
Broderick JP et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage.
Stroke.
1999;30:905-915
Patients with cerebellar ICH > 3 cm who are deteriorating, show signs of brainstem compression or hydrocephalus
Patients with lobar ICH that is 1 cm or less from the cortical surface

• Hematoma growth Is a critical determinant of morbidity and mortality
• Ultra-early hemostatic therapy Arrests ongoing bleeding and minimizes hematoma growth
• rFVIIaCurrently approved for hemorrhage in hemophiliacs
resistant
to Factor VIII or IX replacement therapy Causes local initiation of coagulation cascade after vascular damage.
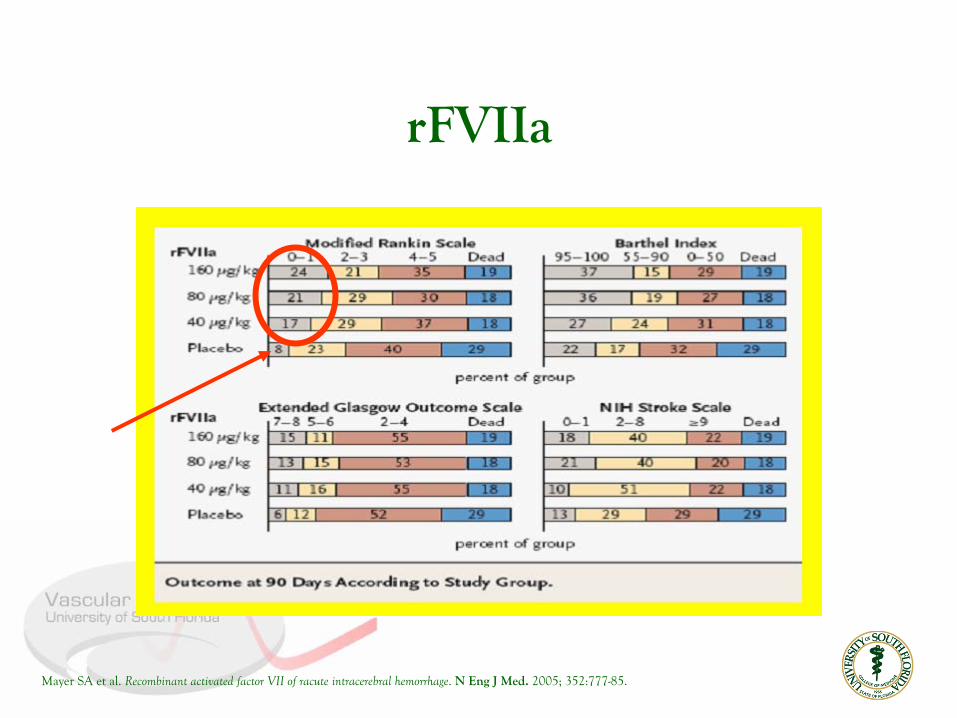
rFVIIa
Mayer SA et al. Recombinant activated factor VII of racute intracerebral hemorrhage. N Eng J Med.
2005; 352:777-85.

rFVIIa
Mayer SA et al. Recombinant activated factor VII of racute intracerebral hemorrhage. N Eng J Med.
2005; 352:777-85.

rFVIIa
Mayer SA et al. Recombinant activated factor VII of racute intracerebral hemorrhage. N Eng J Med.
2005; 352:777-85.
•
Limited hematoma growth
by ~ 50 % (p = 0.01)
•
Relative reduction in
mortality 35%p = 0.025 -
rFVIIa versus
placebo
rFVIIa
Mayer SA et al. Recombinant activated factor VII of racute intracerebral hemorrhage. N Eng J Med.
2005; 352:777-85.

rFVIIa
• Thirty day mortality
30-50%
Depends upon various factorsWith Warfarin on board ~ 70%
• Only ~ 25% will be independent in 6 monthsmonths
PROGNOSIS
Qureshi AI et al. Spontaneous Intracerebral Hemorrhage.
N Eng J Med.
Vol 344, No 19. May 10, 2001.

THE LAW OF 30’S
ICH volume > 30
mLMortality
~ 30
%
In
30
days
PROGNOSIS

ICH SCORE
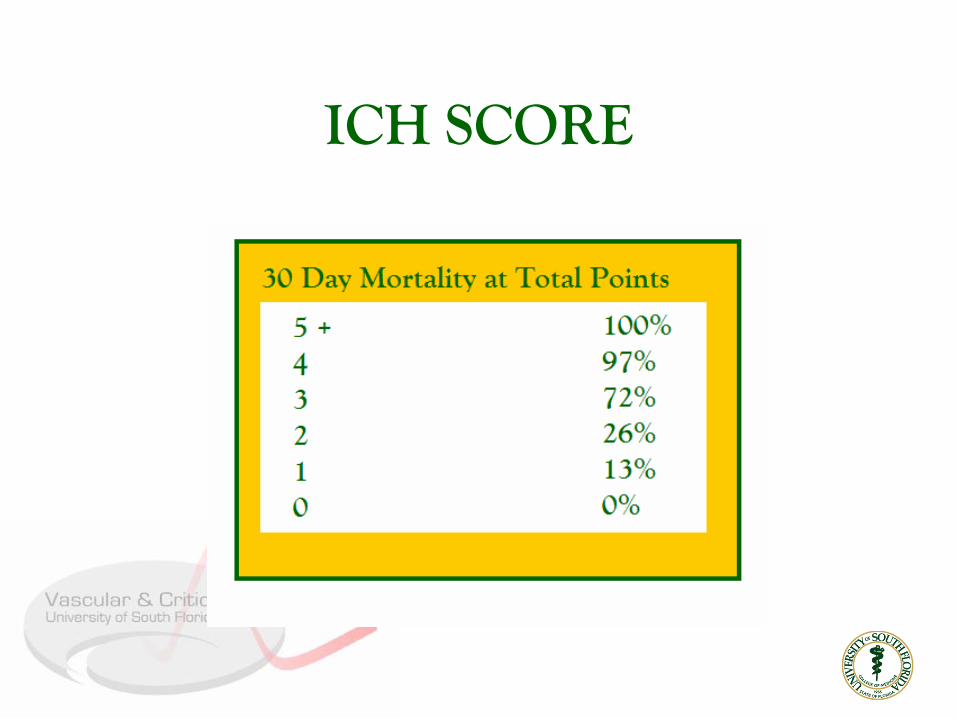
ICH SCORE

Acute therapyATACH -
Antihypertensive therapy in ICHINTERACT -
Effects of aggressive BP loweringDITCH -
Intraventricular thrombolysis
GeneticsGOCHA -
Genetics of Warfarin-related ICH
Surgical interventionSTICH IIMISTIE -
Intra-hematomal tPA and stereotactic evacuation
FUTURE STUDIES

EpidemiologyPathophysiologic mechanismsDiagnostic methodsManagement schemesPrognosisNew directions
SUMMARY

THANK YOU





























