Embed Size (px)
Citation preview
Knee Osteoarthritis: Viscosupplementation to Cartilage Transplantation and Resurfacing Procedures
Resurfacing Procedures and the Degenerative Knee “Joint Resurfacing”
AAOS Annual Meeting – ICL February 18, 2011
Phil Davidson, MDHeiden Davidson Orthopedics
Park City, UT USA
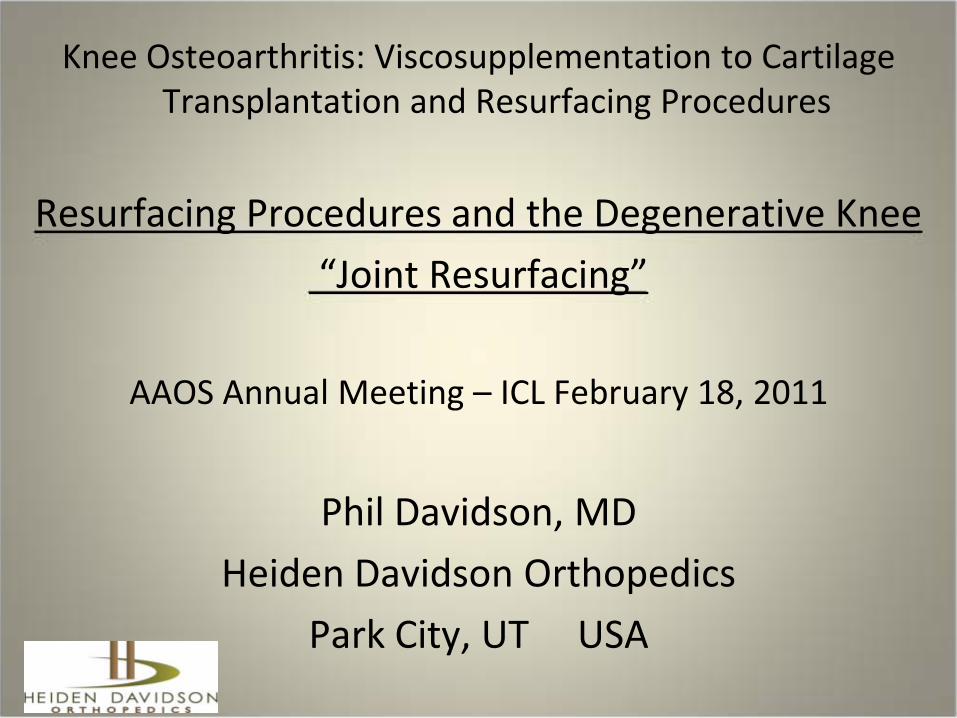
DisclosureArthrosurface – consultant, stock options
29 y.o. mother of 3

Defining the Issue: Why discuss or consider Joint Resurfacing for the Degenerative Knee• 2 main scenarios where
this is relevant1. Younger patients in
whom traditional TKA is not an attractive option
2. “Middle Age” or “Boomer” patients wanting to maintain high levels of function
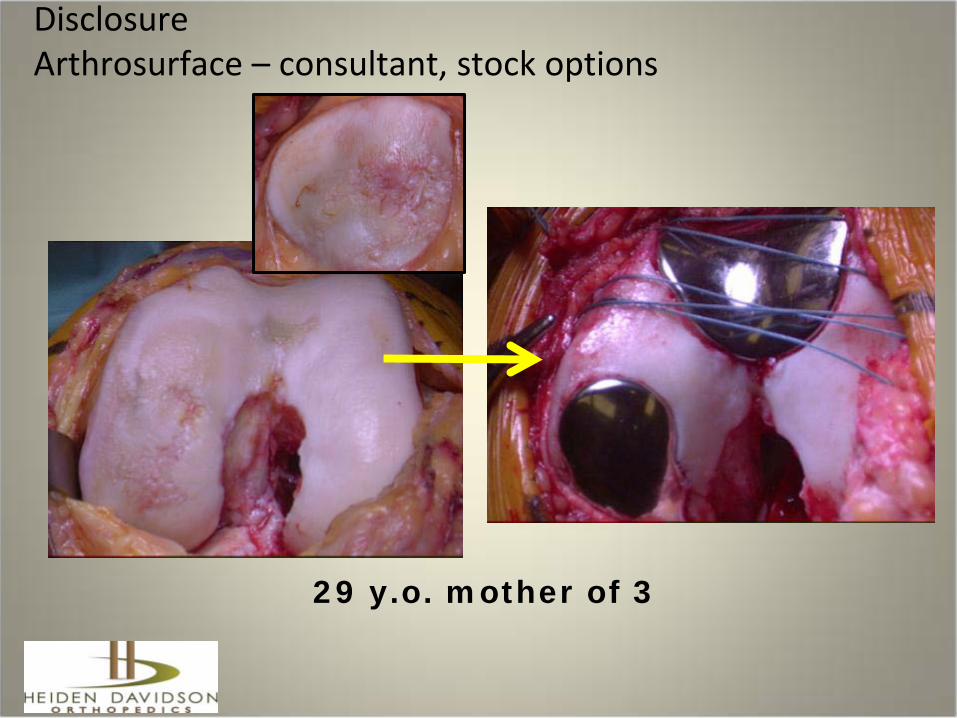
Intro to Joint Resurfacing• Variety of Lesions• Variety of Etiologies • Variety of Options• Focus of this ICL is on
degenerative lesions• Degenerative lesions MUCH more
common than focal defects• Goal is to make sense of
evaluating and treating an array of degenerative pathology while incorporating some new treatment paradigms

Joint ResurfacingA wide realm between…..
Arthroscopic debridement Traditional TKA
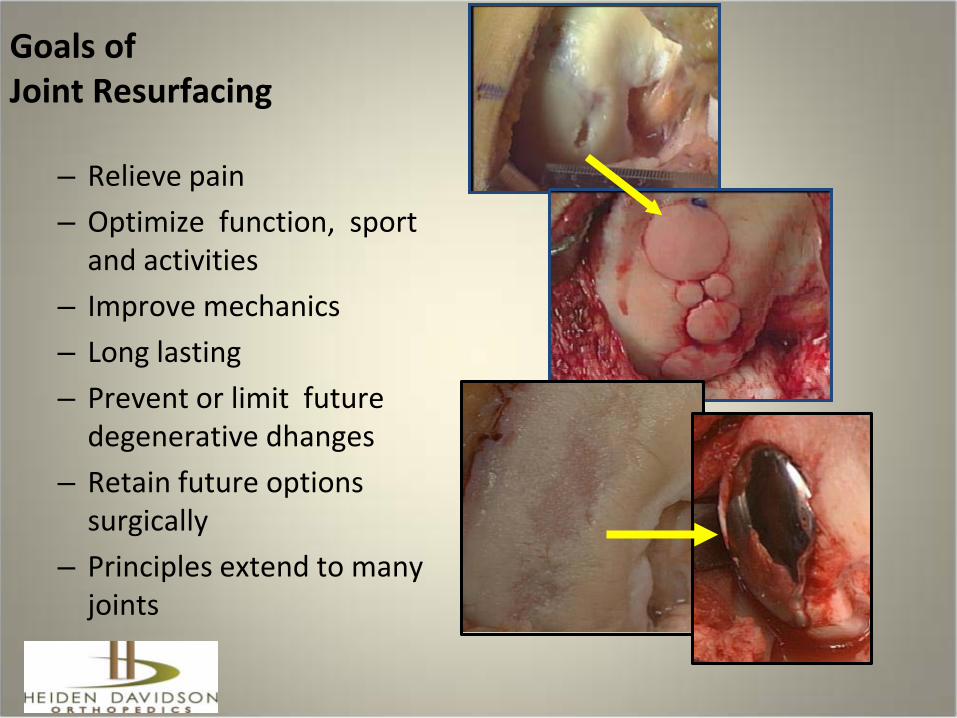
Goals of Joint Resurfacing
– Relieve pain– Optimize function, sport
and activities– Improve mechanics– Long lasting – Prevent or limit future
degenerative dhanges– Retain future options
surgically – Principles extend to many
joints

Joint Resurfacing Treatments:…an evolving continuum of options, biological thru prosthetic• Debridement • Marrow stimulation• Biological restoration
– Biologic grafts – Biosynthetics– Scaffolds– Cellular therapy
• Prosthetic Resurfacing– Bio-Prosthetic mix – Inlay Arthroplasty– Onlay Arthroplasty – Total Joint
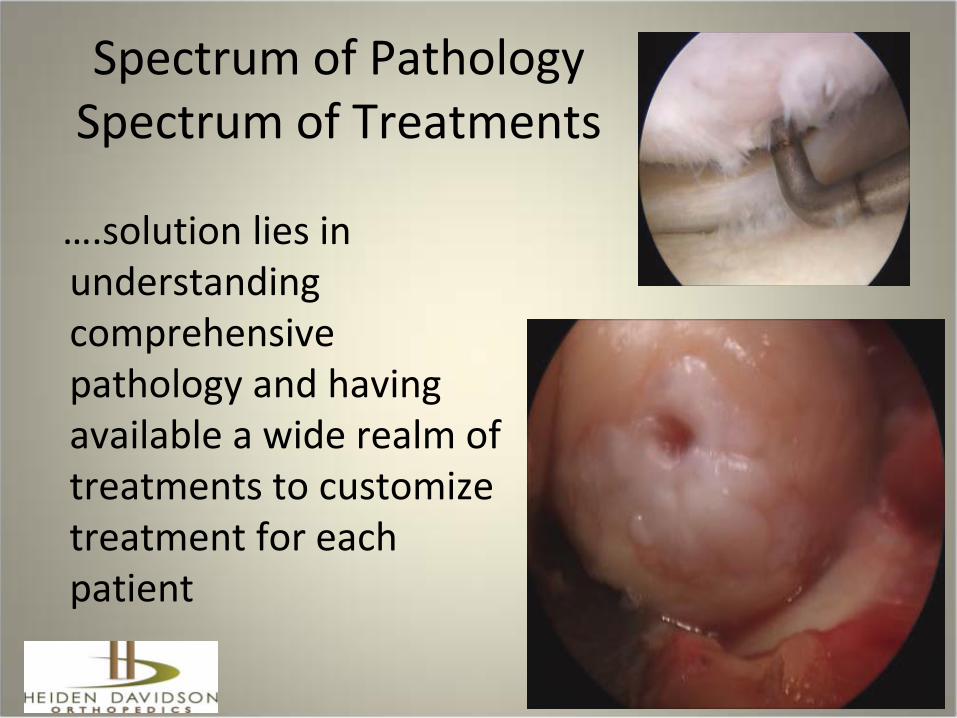
Spectrum of PathologySpectrum of Treatments
….solution lies in understanding comprehensive pathology and having available a wide realm of treatments to customize treatment for each patient
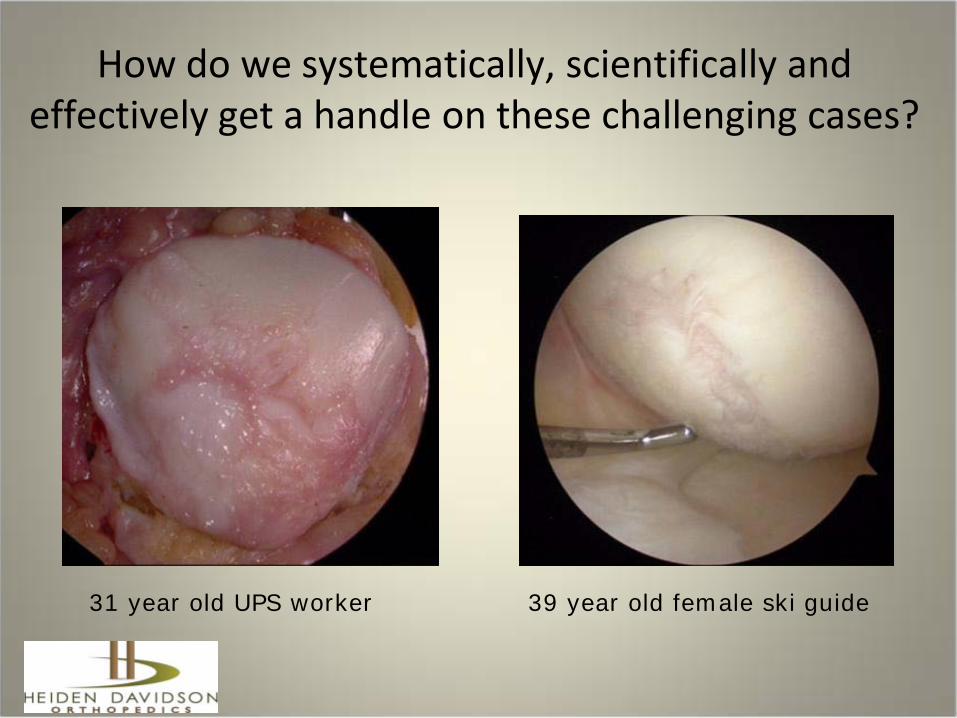
How do we systematically, scientifically and effectively get a handle on these challenging cases?
39 year old female ski guide 31 year old UPS worker
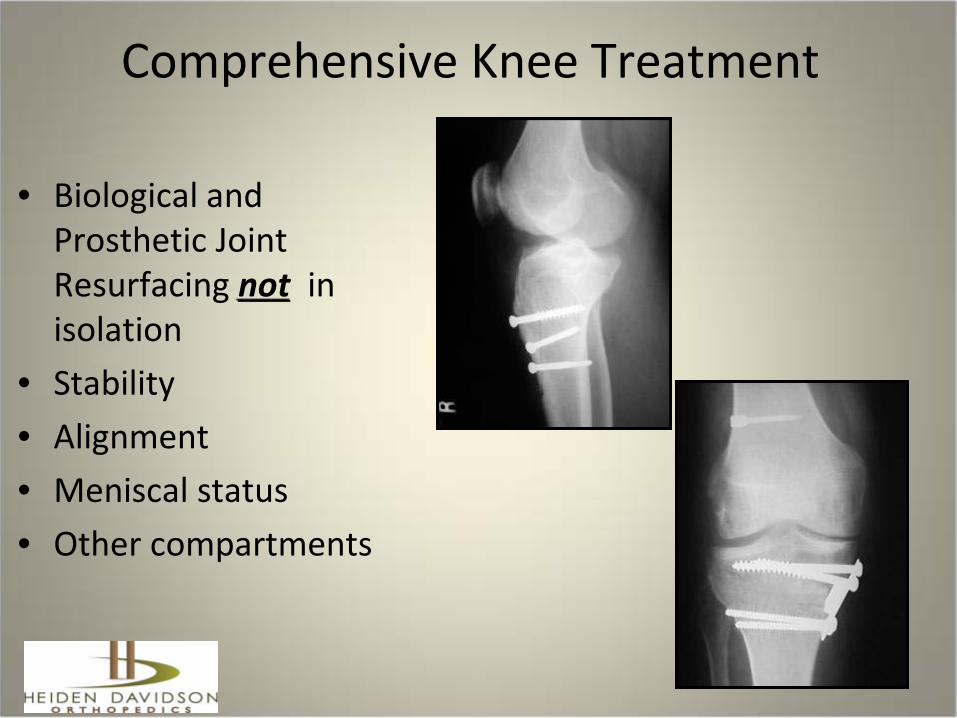
Comprehensive Knee Treatment
• Biological and Prosthetic Joint Resurfacing not in isolation
• Stability• Alignment• Meniscal status• Other compartments
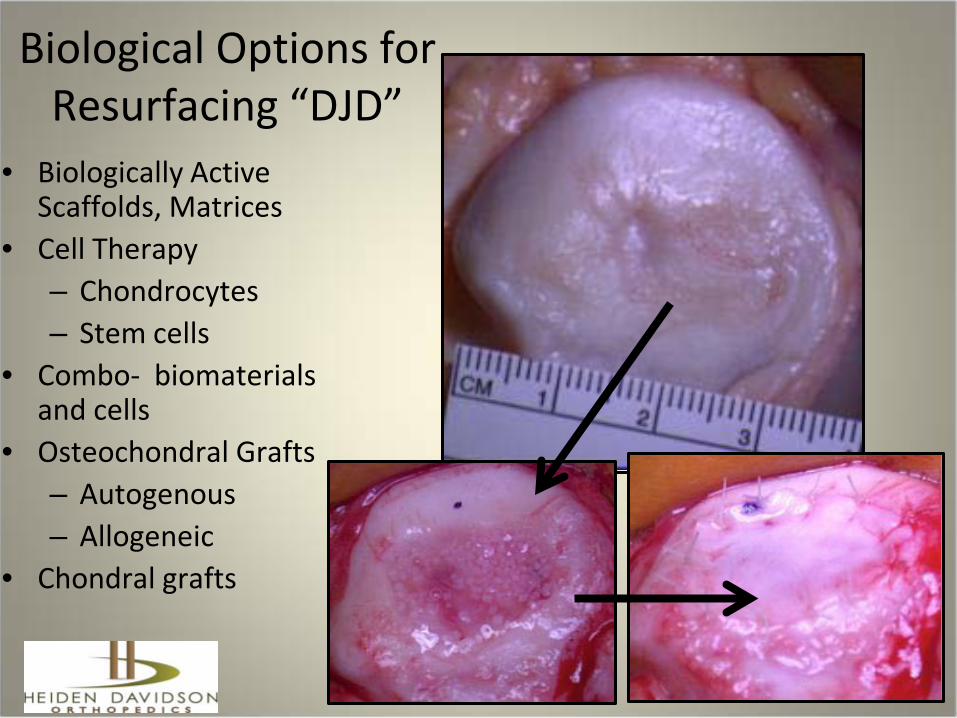
Biological Options for Resurfacing “DJD”
• Biologically Active Scaffolds, Matrices
• Cell Therapy – Chondrocytes– Stem cells
• Combo- biomaterials and cells
• Osteochondral Grafts– Autogenous– Allogeneic
• Chondral grafts
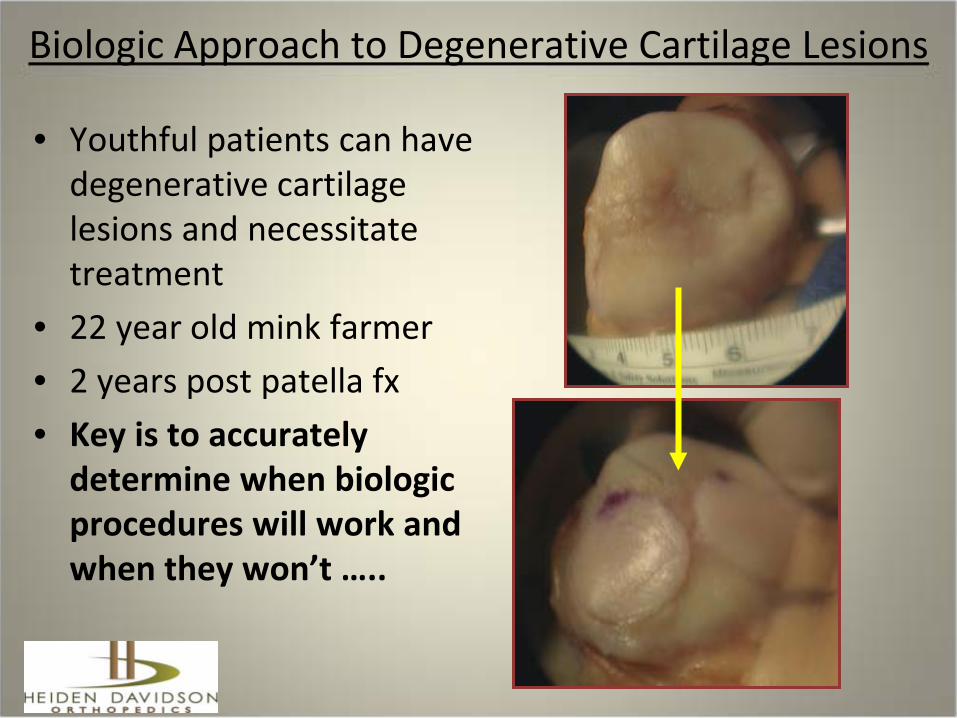
Biologic Approach to Degenerative Cartilage Lesions
• Youthful patients can have degenerative cartilage lesions and necessitate treatment
• 22 year old mink farmer • 2 years post patella fx • Key is to accurately
determine when biologic procedures will work and when they won’t …..
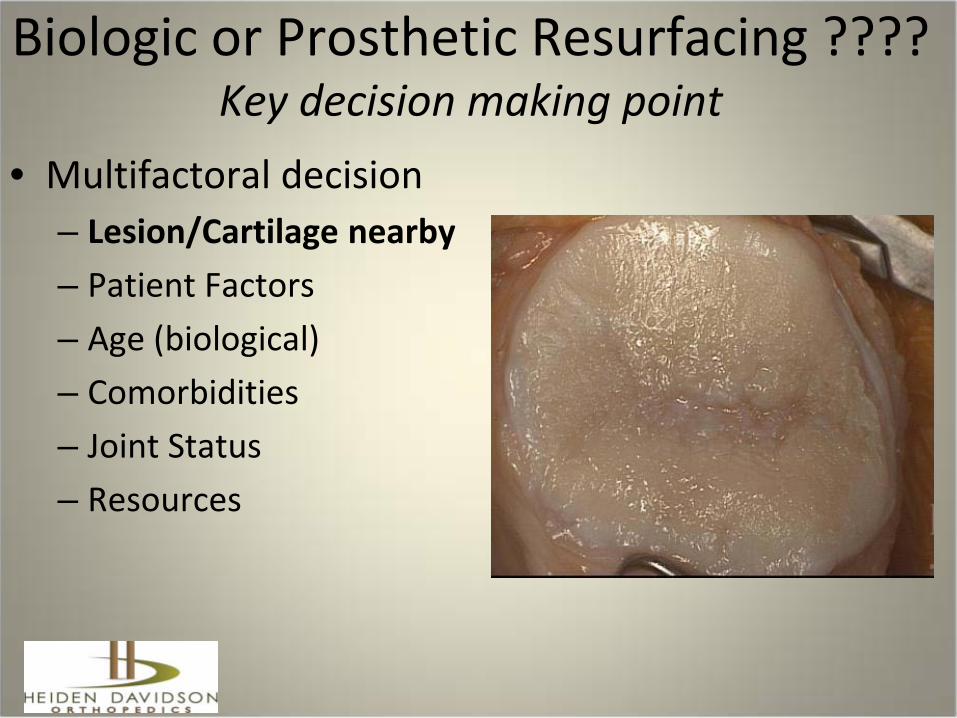
Biologic or Prosthetic Resurfacing ???? Key decision making point
• Multifactoral decision– Lesion/Cartilage nearby– Patient Factors – Age (biological)– Comorbidities– Joint Status – Resources
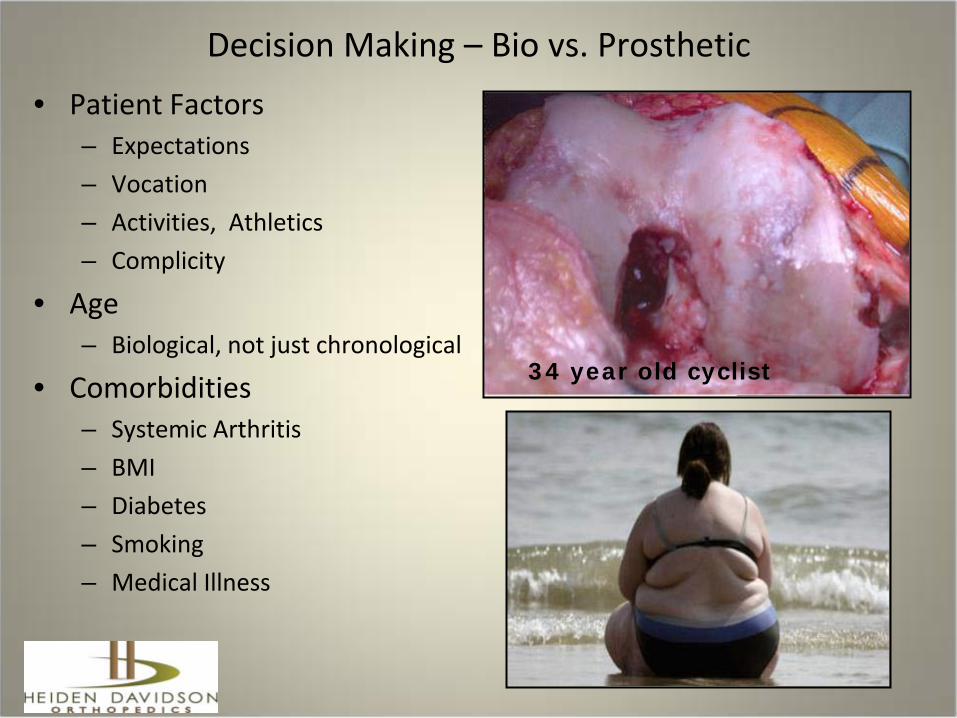
Decision Making – Bio vs. Prosthetic• Patient Factors
– Expectations– Vocation – Activities, Athletics – Complicity
• Age– Biological, not just chronological
• Comorbidities– Systemic Arthritis – BMI– Diabetes– Smoking– Medical Illness
34 year old cyclist
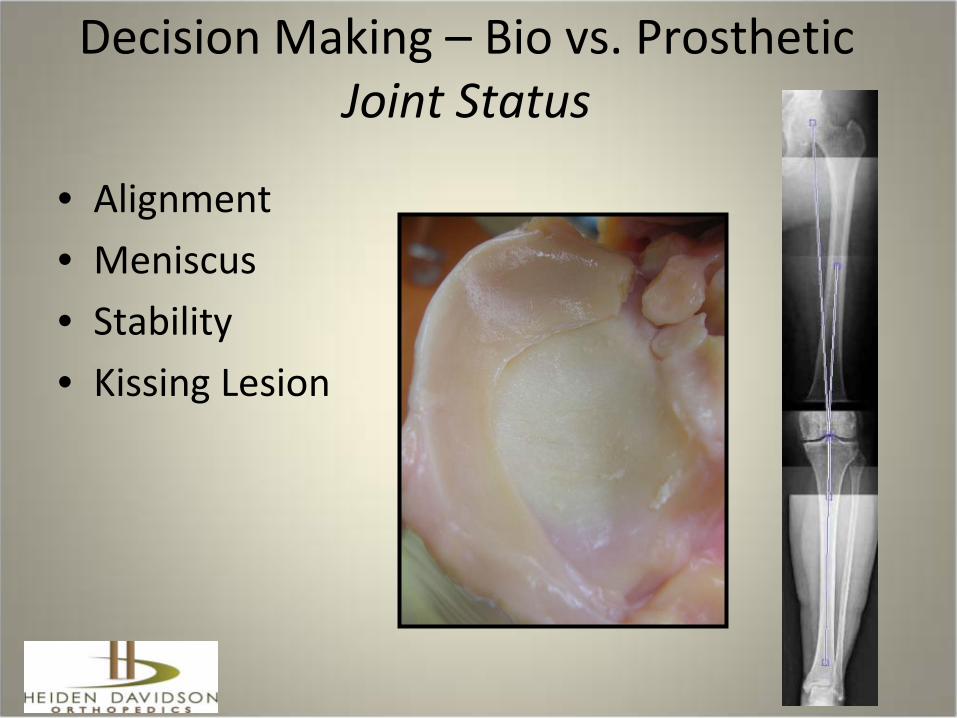
Decision Making – Bio vs. ProstheticJoint Status
• Alignment• Meniscus• Stability• Kissing Lesion

Decision Making – Bio vs. ProstheticJoint Morphology
• Biologic Solutions are less likely to work in joint which has lost contour
• Mechanical stresses on bio surfaces must be taken into account
• Is the joint “out of round” – osteophytes or flattening

Radiographic Guide to Bio vs. ProstheticKellgren-Lawrence Grading Scale Generally Biological ……Grade 0 = Normal Grade 1 = Doubtful narrowing of the joint
space and possible osteophytic lipping
Grade 2 = Definite osteophytes, definite narrowing of the joint space
Generally Prosthetic…..Grade 3 = Moderate multiple osteophytes,
definite narrowing of joints space, some sclerosis and possible deformity of bone contour
Grade 4 = large osteophytes, marked narrowing of joint space, severe sclerosis and definite deformity of bone contour.
KL 2
KL 2
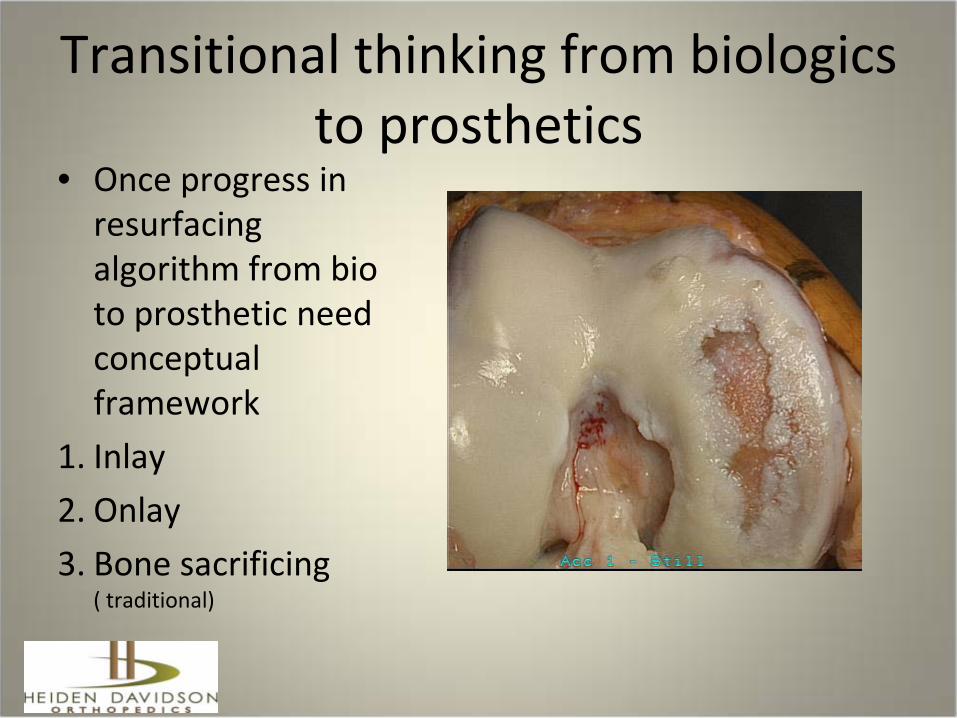
Transitional thinking from biologics to prosthetics
• Once progress in resurfacing algorithm from bio to prosthetic need conceptual framework
1. Inlay2. Onlay3. Bone sacrificing
( traditional)
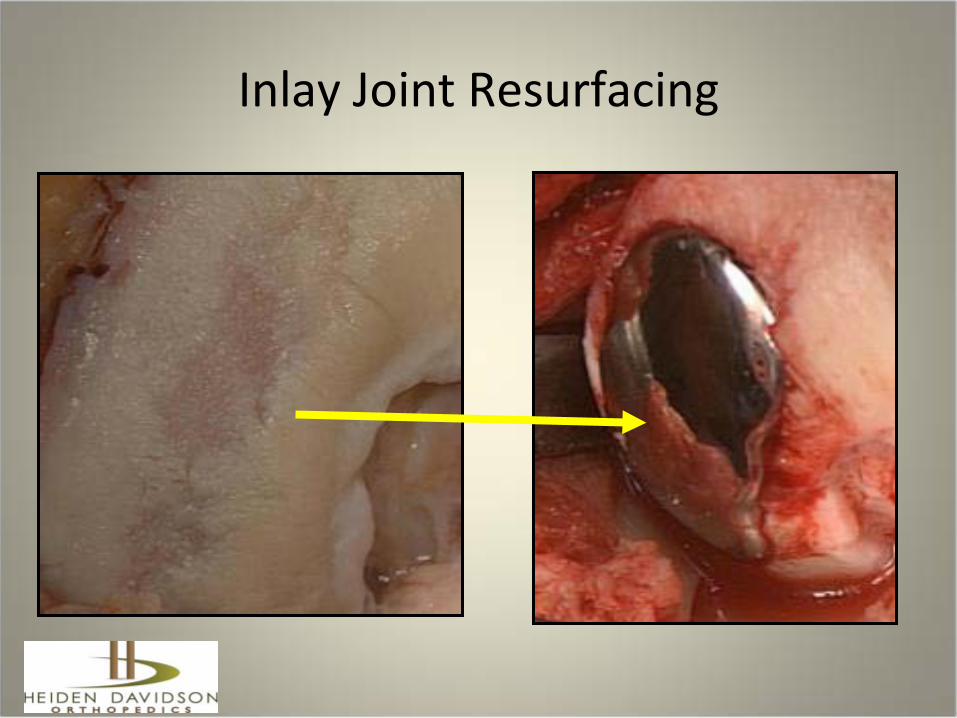
Inlay Joint Resurfacing
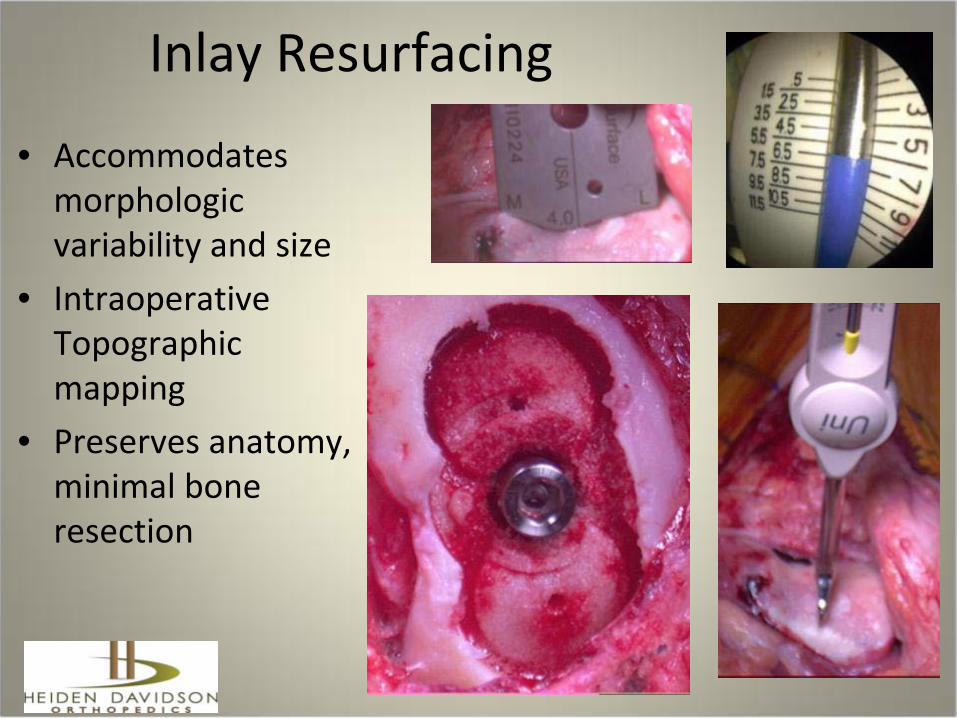
Inlay Resurfacing
• Accommodates morphologic variability and size
• Intraoperative Topographic mapping
• Preserves anatomy, minimal bone resection
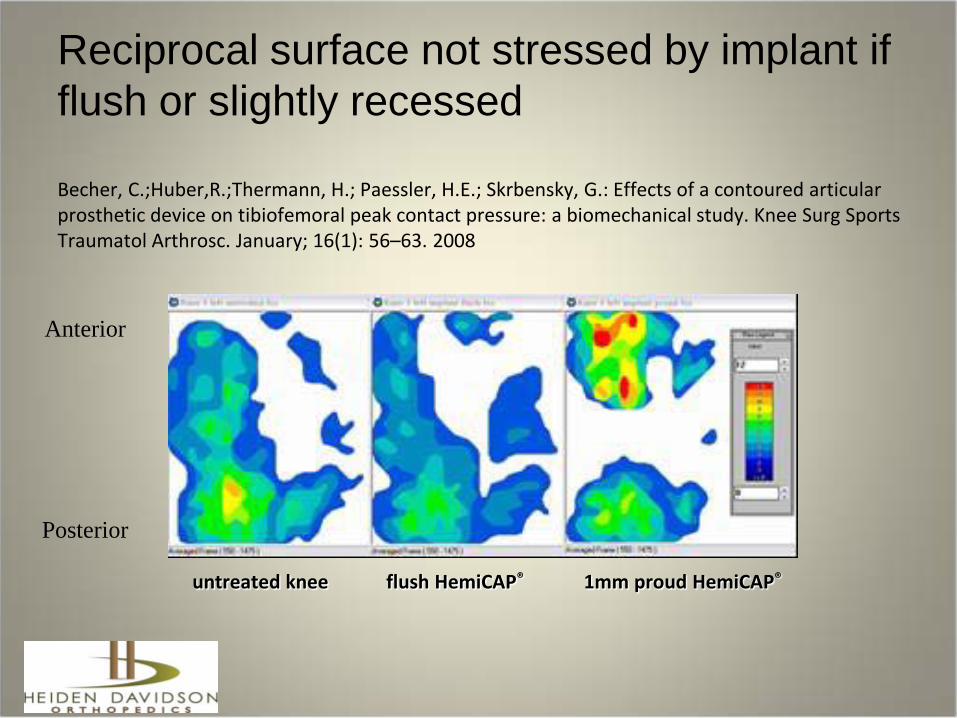
untreated knee flush HemiCAP® 1mm proud HemiCAP®
Reciprocal surface not stressed by implant if flush or slightly recessed
Becher, C.;Huber,R.;Thermann, H.; Paessler, H.E.; Skrbensky, G.: Effects of a contoured articular prosthetic device on tibiofemoral peak contact pressure: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. January; 16(1): 56–63. 2008
Anterior
Posterior
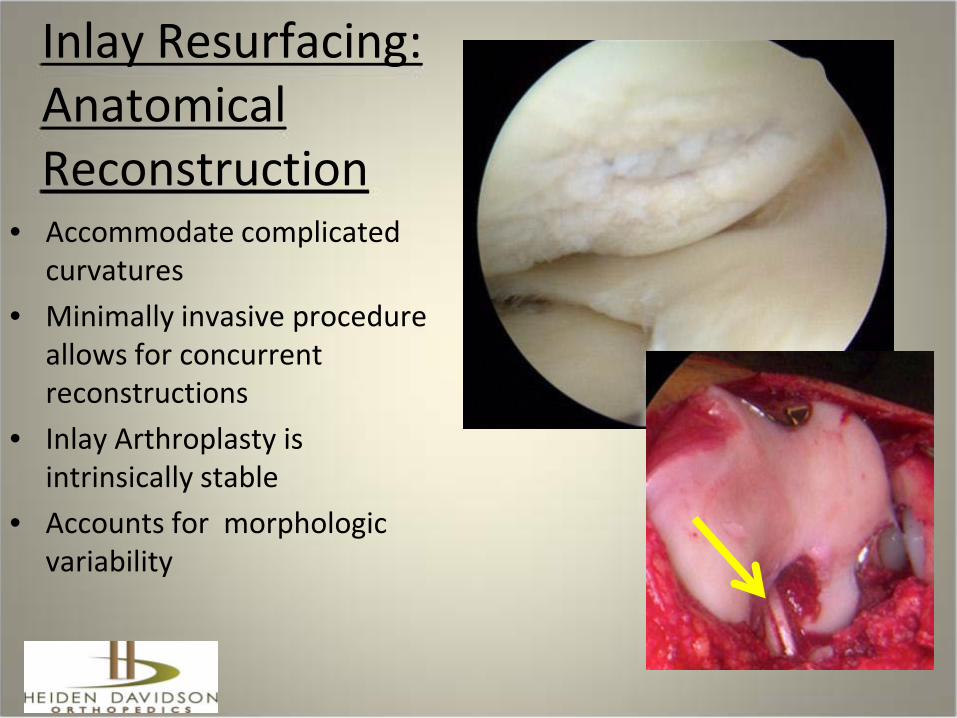
Inlay Resurfacing: Anatomical Reconstruction
• Accommodate complicated curvatures
• Minimally invasive procedure allows for concurrent reconstructions
• Inlay Arthroplasty is intrinsically stable
• Accounts for morphologic variability

Inlay – Contoured Articular Prosthesis
• Geometry based on patient’s native anatomy
• Intraoperative joint mapping
• Account for complex asymmetrical geometry
• Extension of biological resurfacing
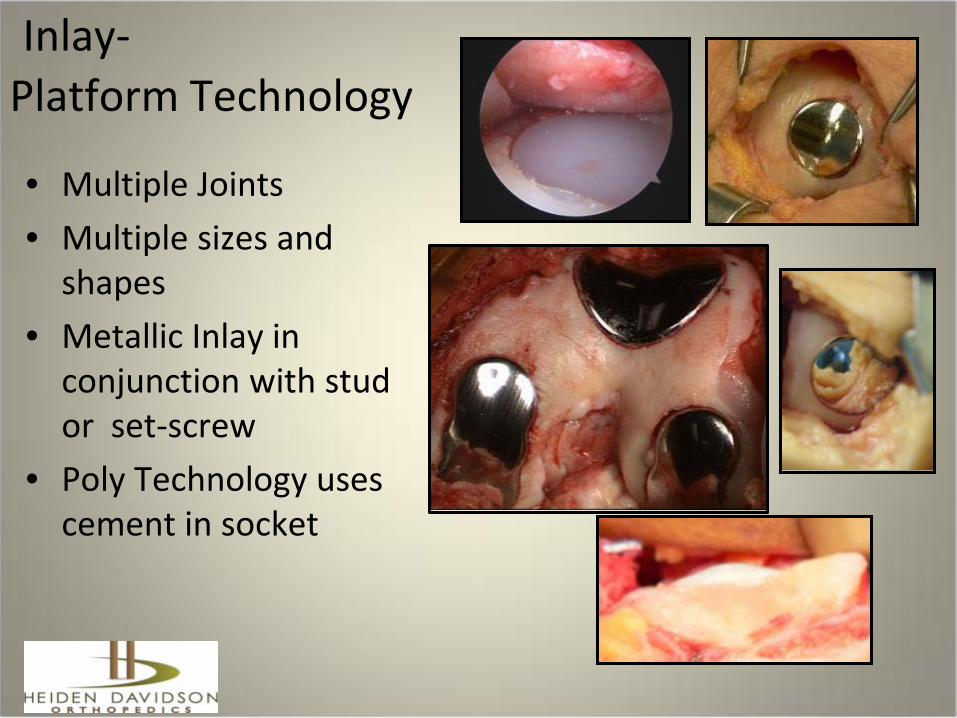
Inlay-Platform Technology
• Multiple Joints• Multiple sizes and
shapes• Metallic Inlay in
conjunction with stud or set-screw
• Poly Technology uses cement in socket
Inlay Advantages• Able to restore mechanical homeostasis “smoothness”• Alleviate pain• Low volume, prevents encroachment on other parts of
joint• Minimally invasive, low morbidity• Revision to subsequent arthroplasty is easy due to
shallow implant bed with minimal bone resection• Ample room for ACL, osteotomy, soft tissue procedures • Relatively focal treatment preserving healthy adjacent
anatomy

Inlay Limitations and Concerns
• Limited/Little angular correction can be obtained with an inlay implant
• Must accommodate or account for loss of ROM• Stiff knee- consider tissue releases, other choices
• Must consider reciprocal surface, resurface if needed• Extensive tibial cartilage loss mandates onlay
resurfacing to cover more of tibia • Be cautious and specific about referred pain and
radiating pain patterns.
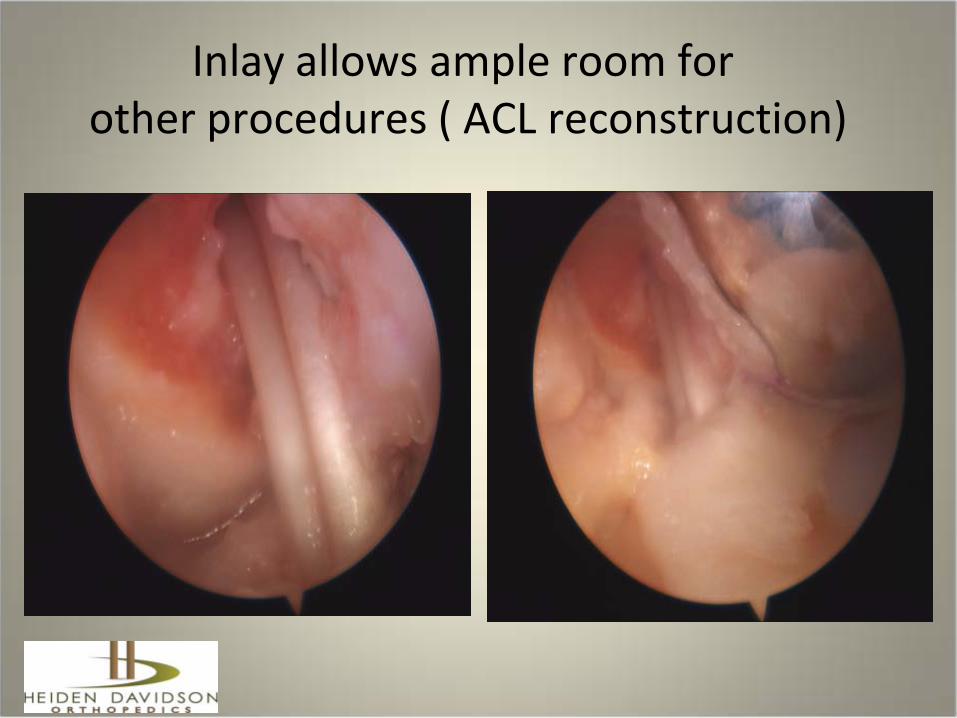
Inlay allows ample room forother procedures ( ACL reconstruction)
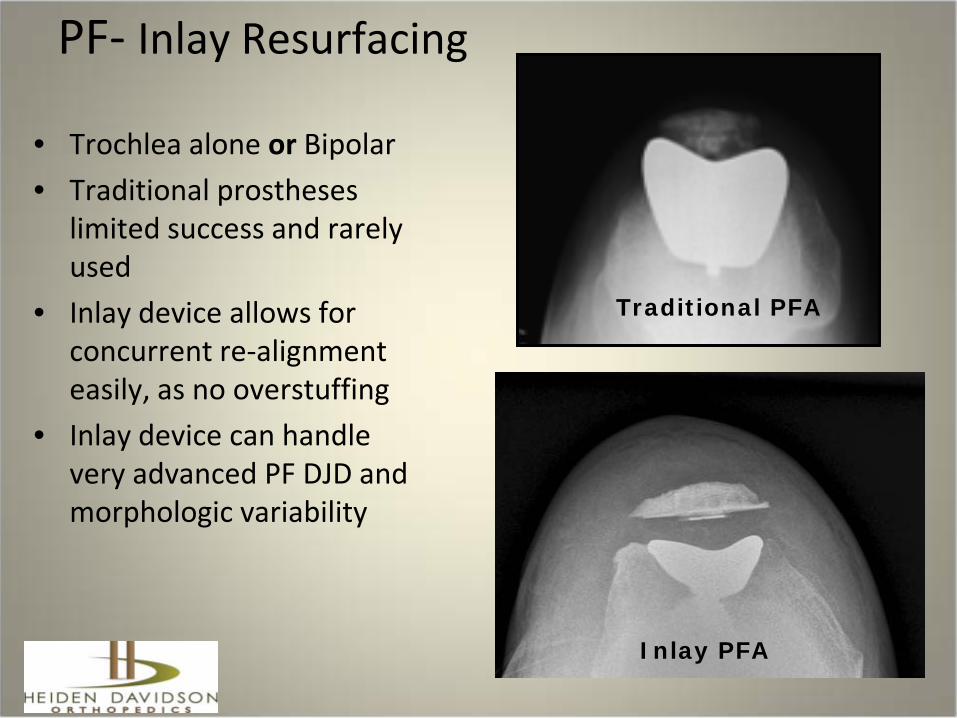
PF- Inlay Resurfacing
• Trochlea alone or Bipolar • Traditional prostheses
limited success and rarely used
• Inlay device allows for concurrent re-alignment easily, as no overstuffing
• Inlay device can handle very advanced PF DJD and morphologic variability
Traditional PFA
Inlay PFA
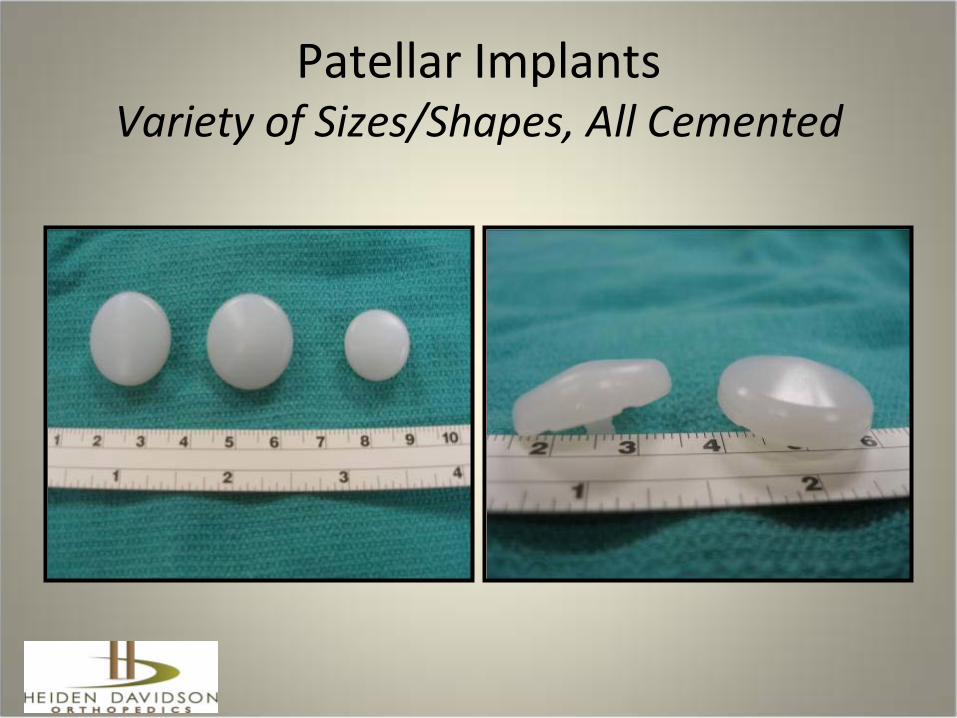
Patellar Implants Variety of Sizes/Shapes, All Cemented
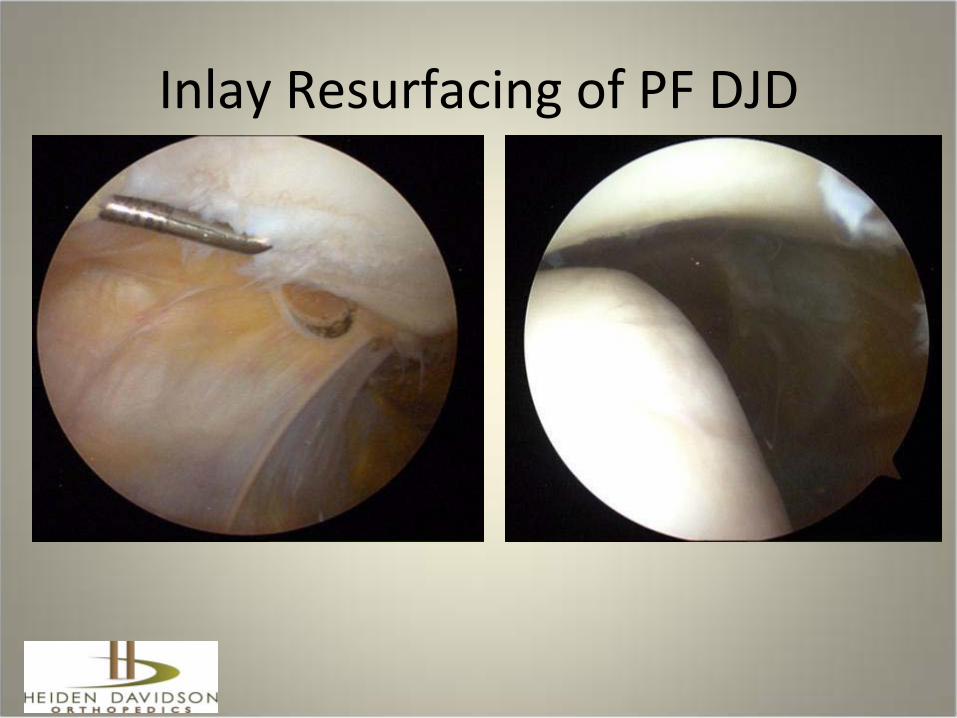
Inlay Resurfacing of PF DJD
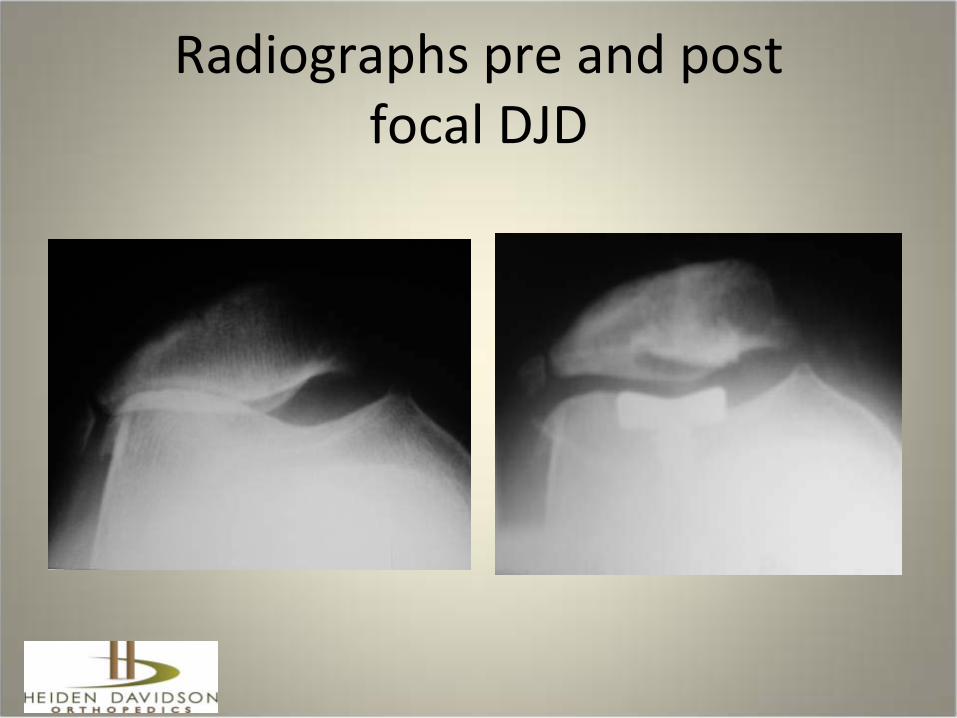
Radiographs pre and postfocal DJD
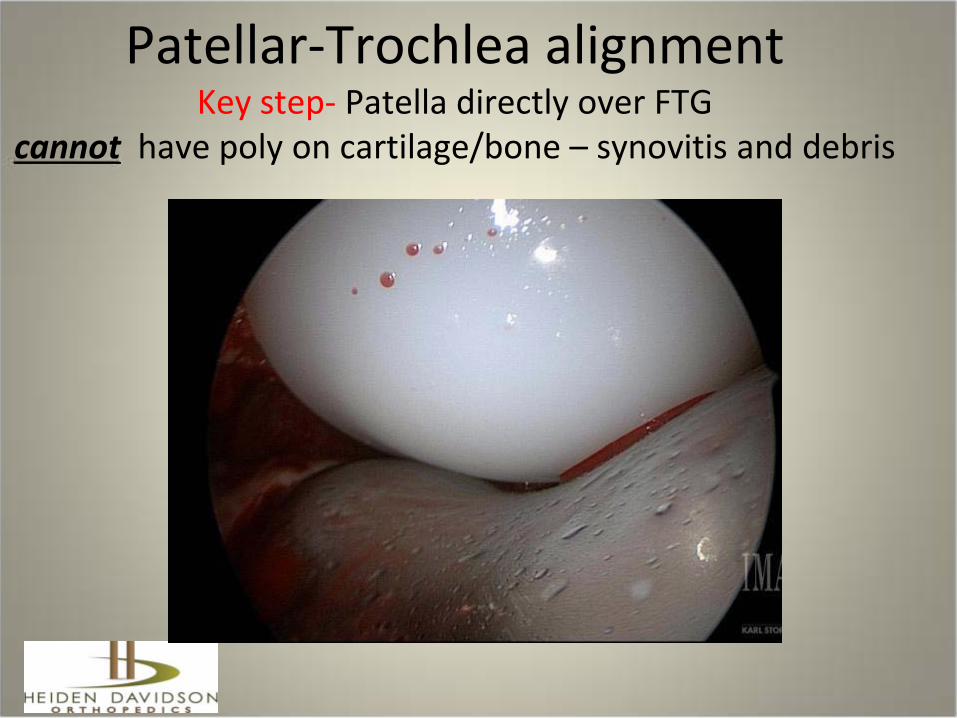
Patellar-Trochlea alignment Key step- Patella directly over FTG
cannot have poly on cartilage/bone – synovitis and debris

Case # 1 – 42 year old female
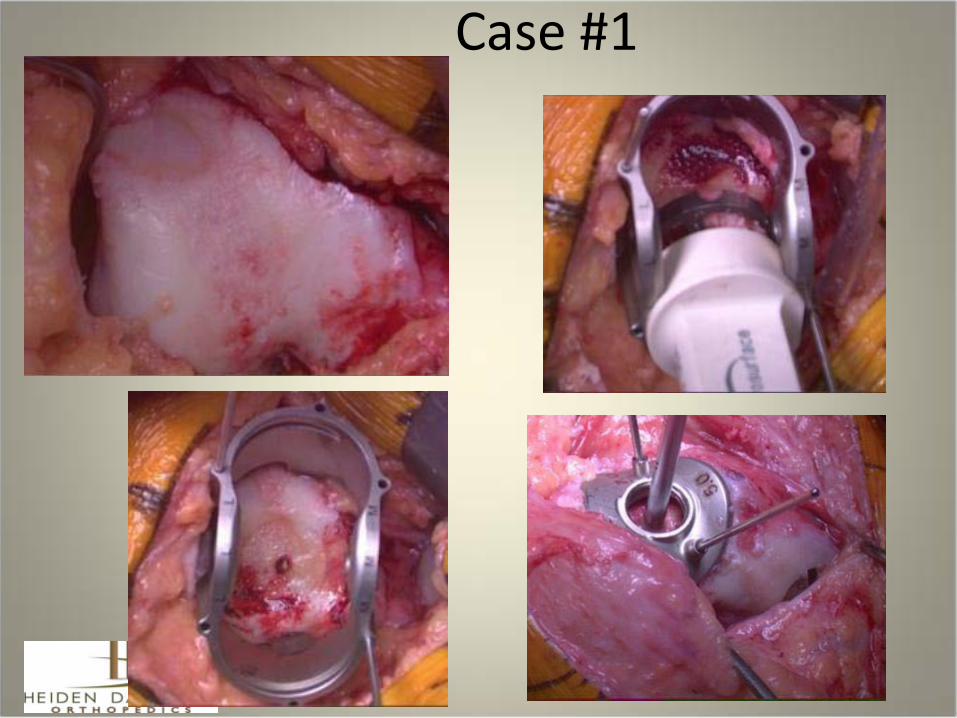
Case #1
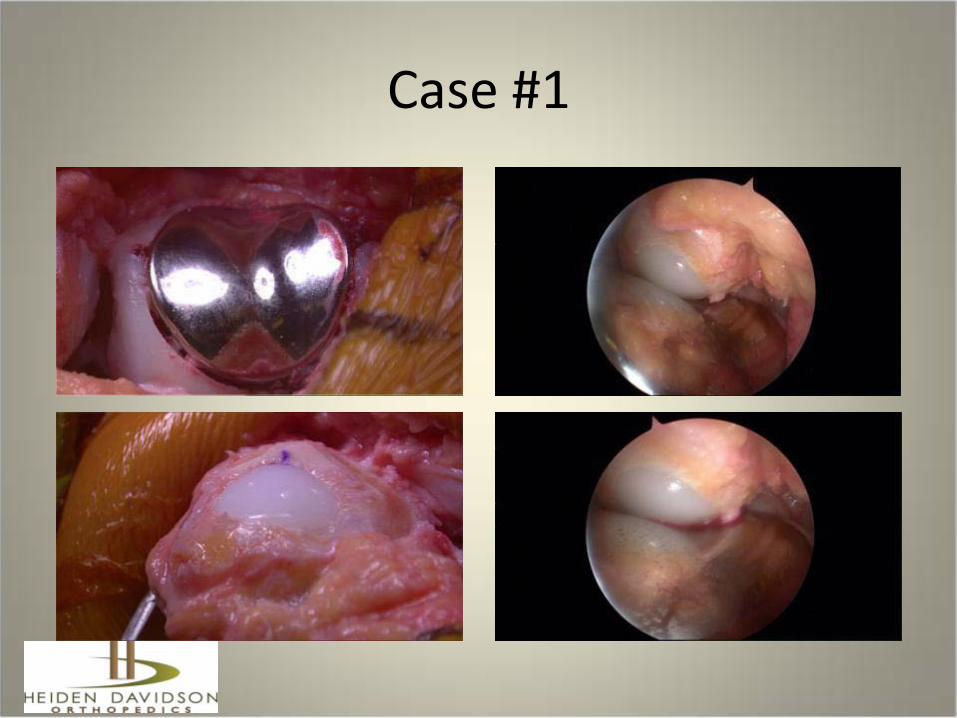
Case #1

Inlay Unicompartmental resurfacing arthroplasty
aka….UniCAP™scope assisted Uni, AKR , etc..
Cementation
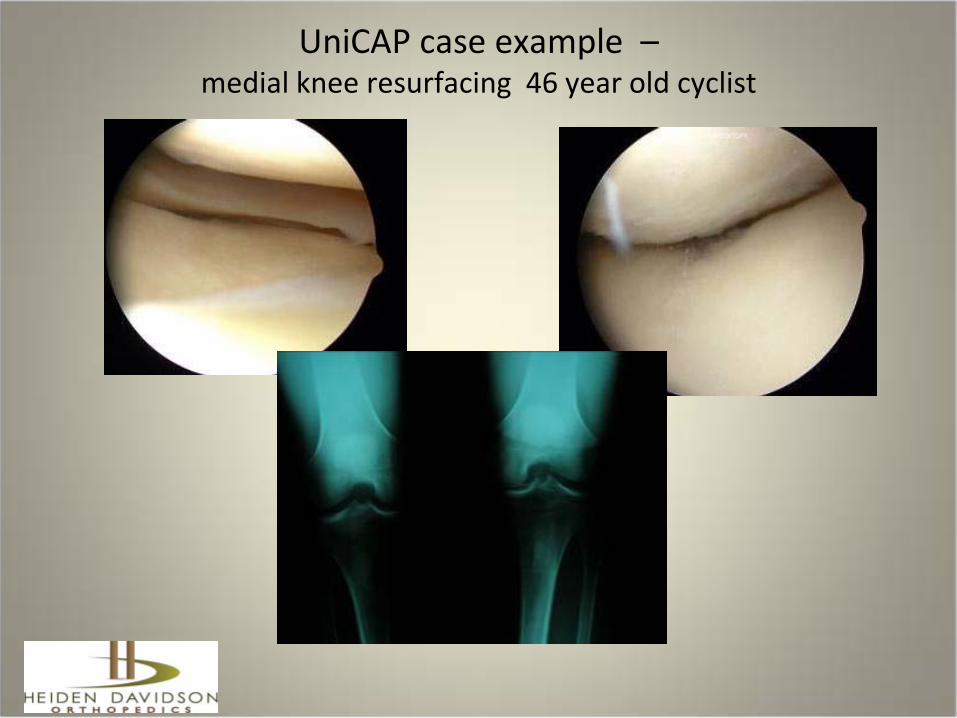
UniCAP case example –medial knee resurfacing 46 year old cyclist
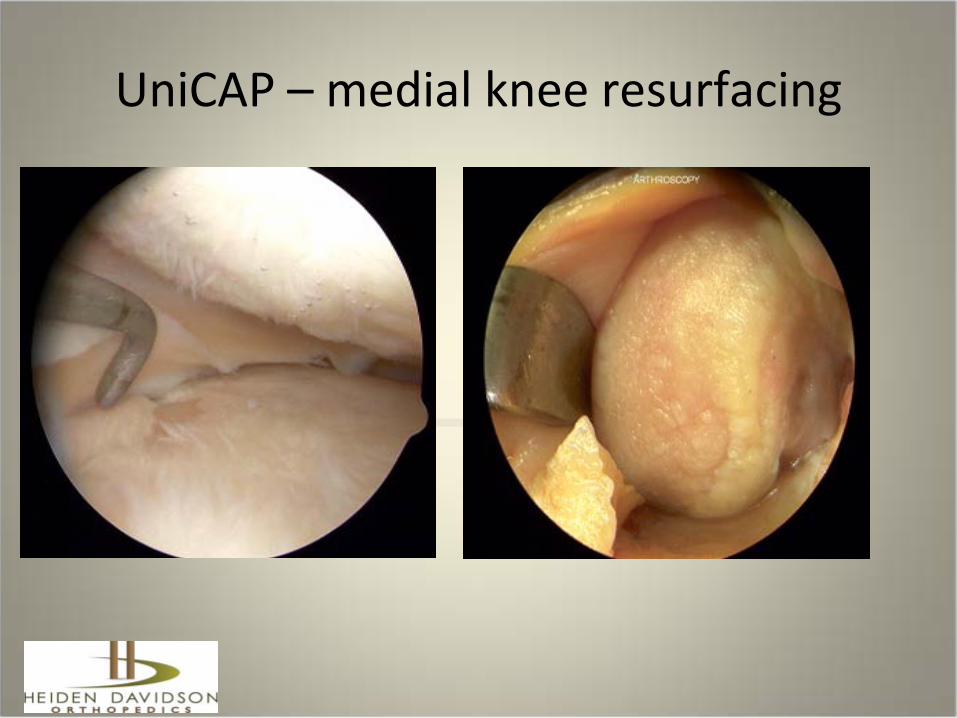
UniCAP – medial knee resurfacing

UniCAP – medial knee resurfacing
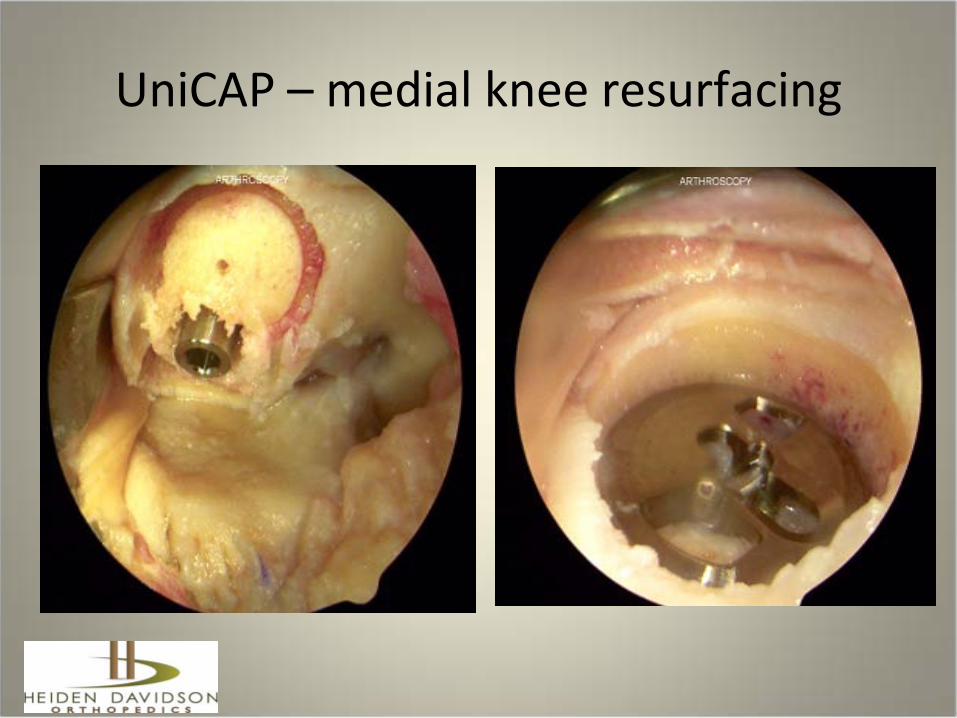
UniCAP – medial knee resurfacing

UniCAP – medial knee resurfacing
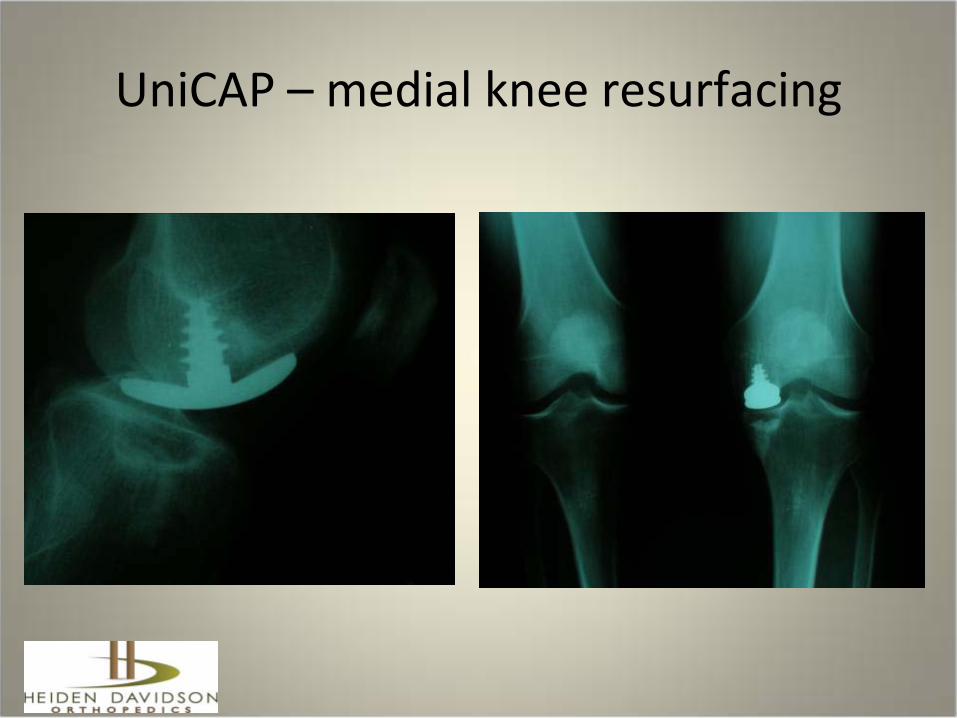
UniCAP – medial knee resurfacing

Combining Inlay and Onlay Technologies
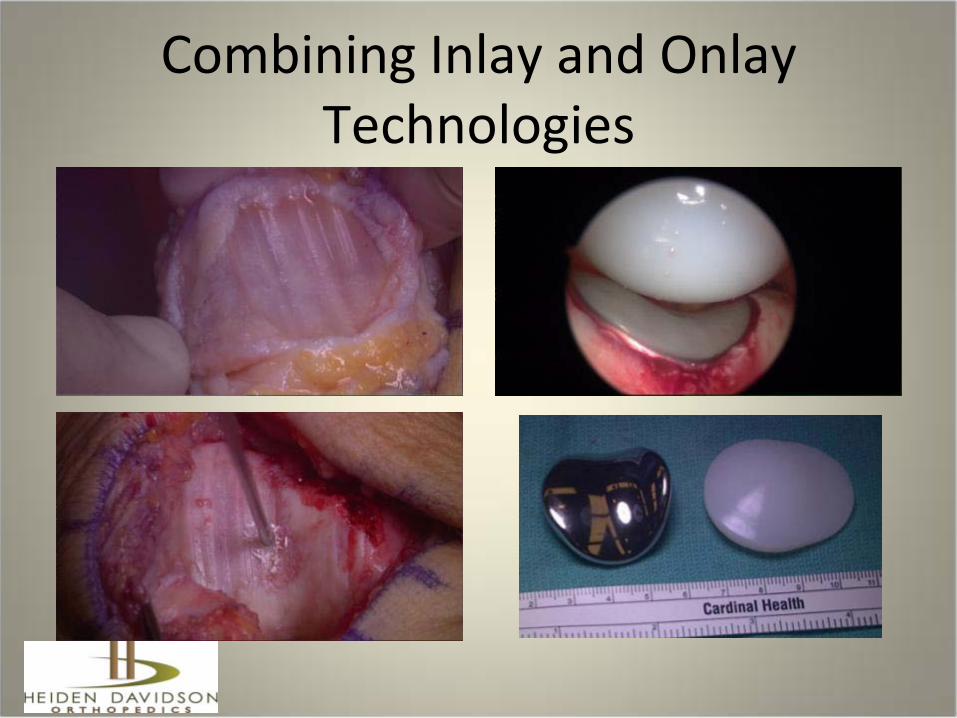
Combining Inlay and Onlay Technologies
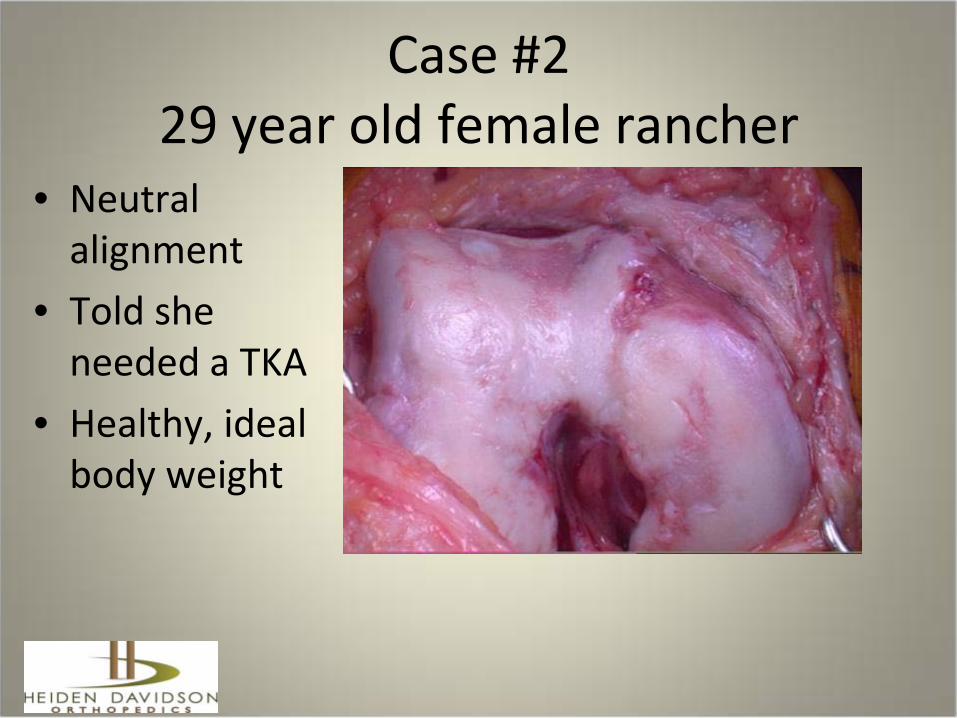
Case #229 year old female rancher
• Neutral alignment
• Told she needed a TKA
• Healthy, ideal body weight
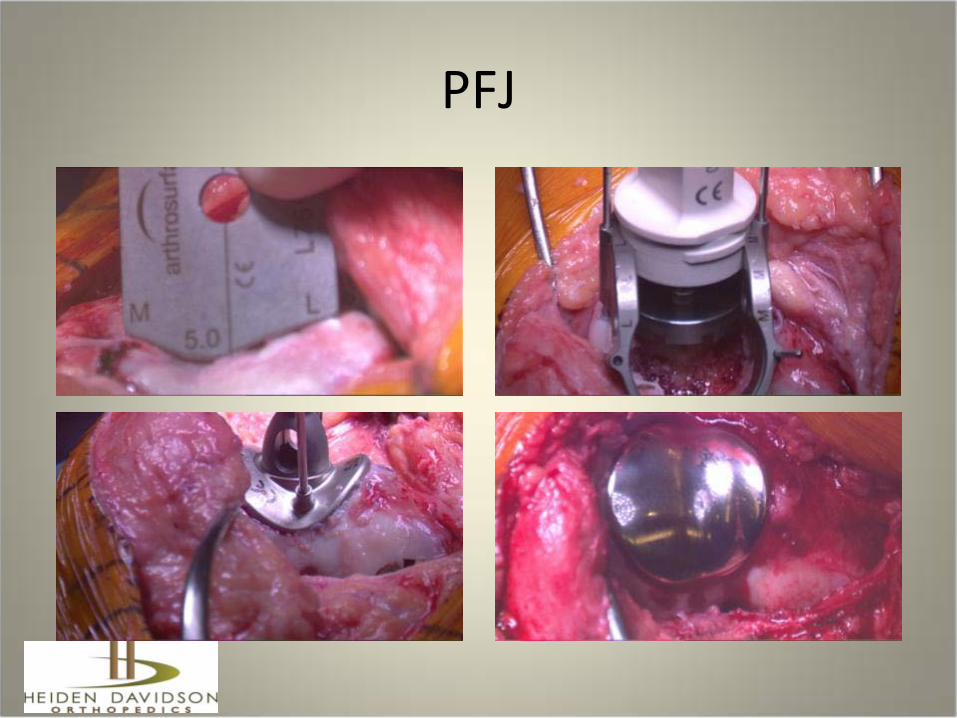
PFJ
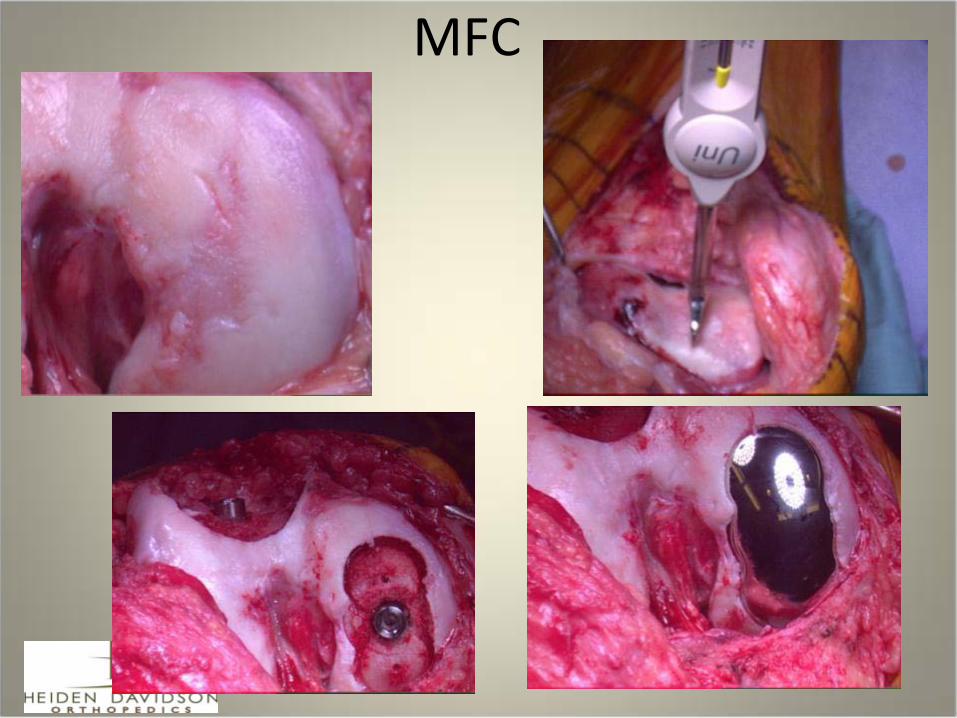
MFC
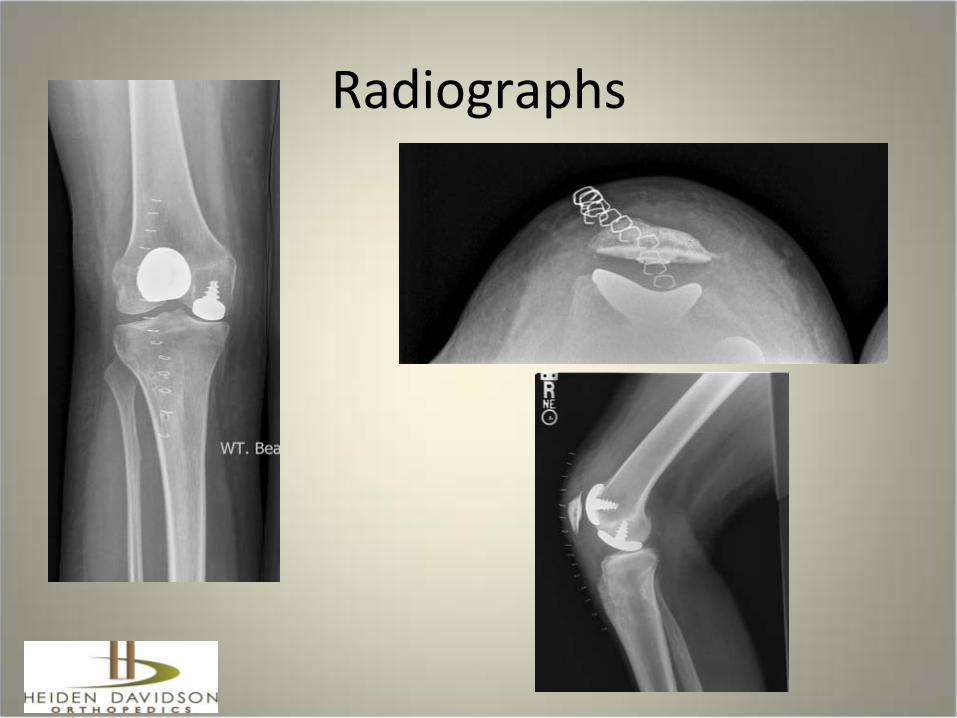
Radiographs
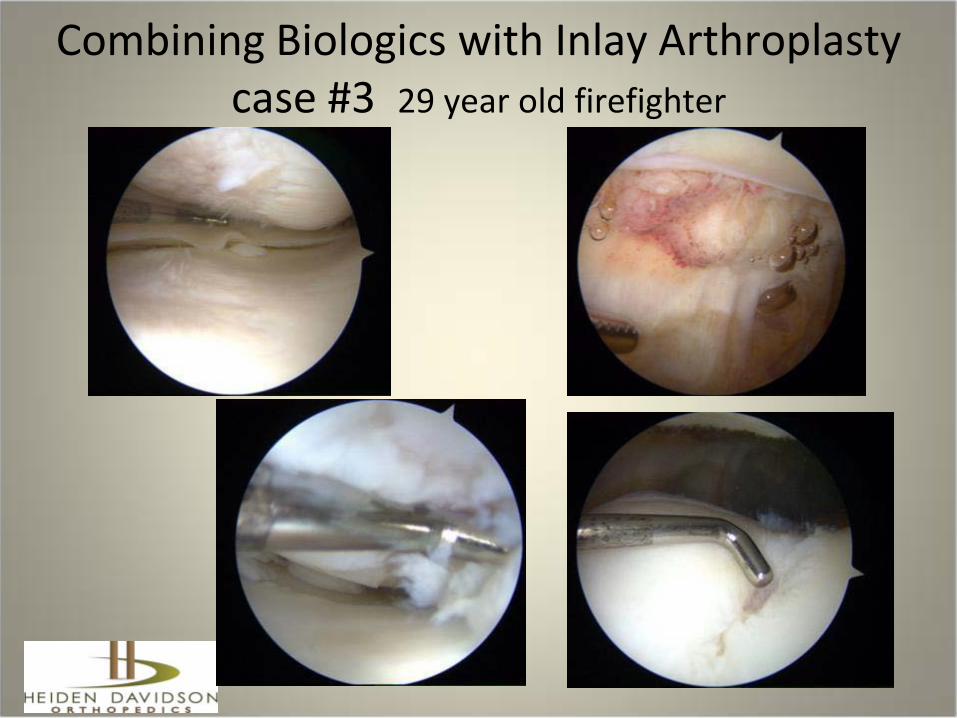
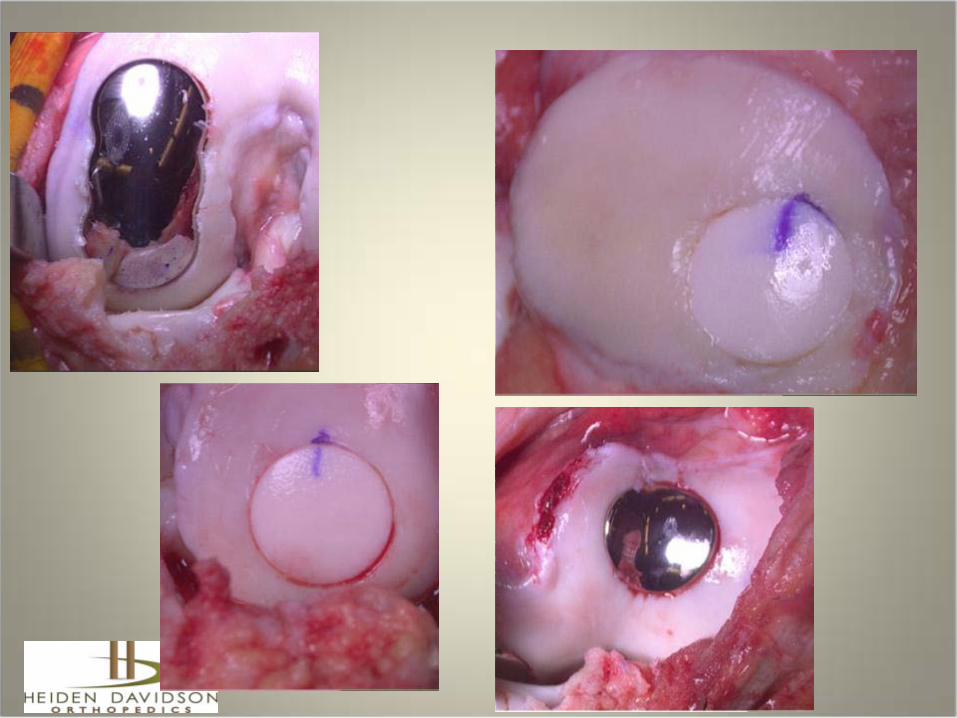
Combining Biologics with Inlay Arthroplastycase #3 29 year old firefighter

MFC Patella
LFC
FTG

•6 wks post op back at work light duty•12 wks post op full RTW as firefighter

Technical Failure38 yr old 9 mos post op - no pain relief from unipolar Inlay
synovitis, cartilage debris, implant proud, tibial wear, FTG defect
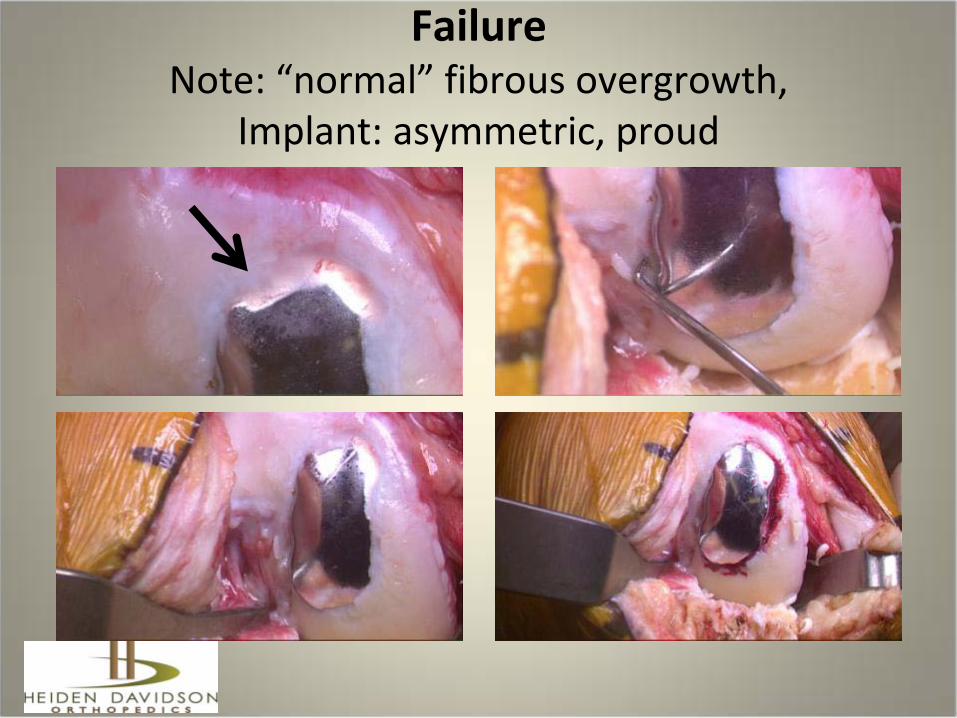
FailureNote: “normal” fibrous overgrowth,
Implant: asymmetric, proud

Inlay removal- revision to Onlay UKAwith Inlay FTG
Indications Inlay Contraindications
• Minimal angular deformity
• Large focal or limited degenerative lesions
• Limited, not diffuse disease
• Grade IIIC,D or IV
• Extensile disease• Angular deformity• Large Tibial defects• Peripheral tibial defects• Cartilage compromise
elsewhere in joint
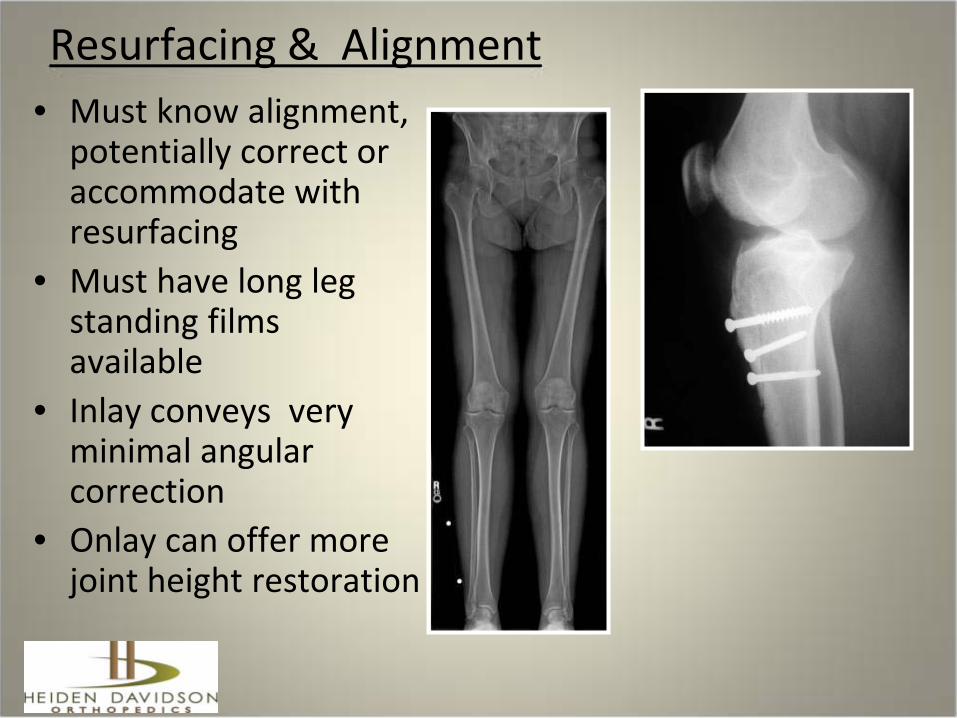
Resurfacing & Alignment• Must know alignment,
potentially correct or accommodate with resurfacing
• Must have long leg standing films available
• Inlay conveys very minimal angular correction
• Onlay can offer more joint height restoration
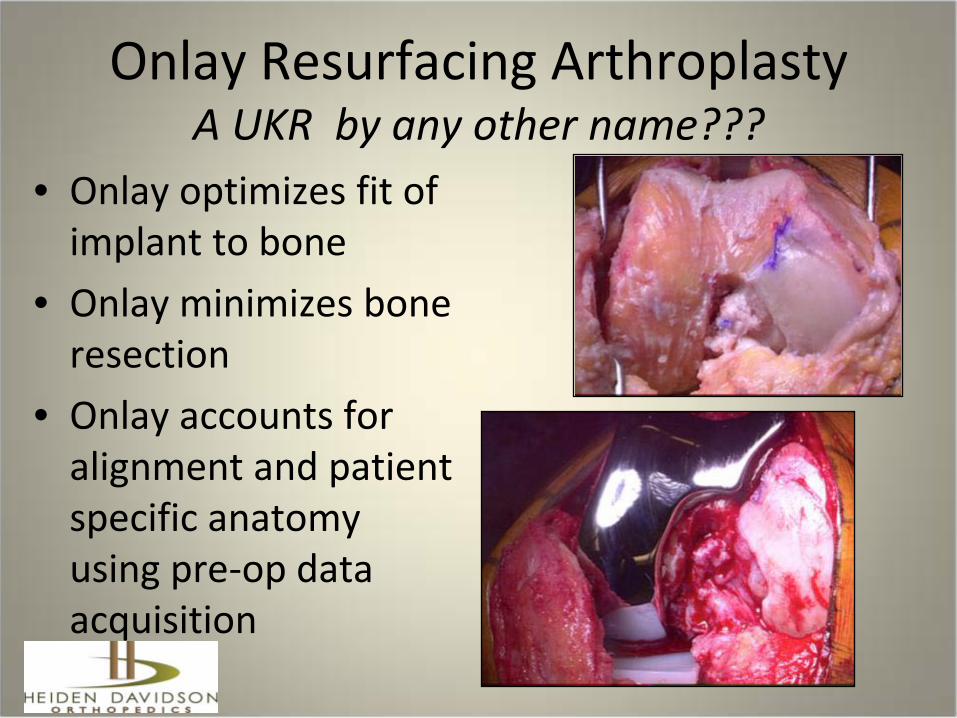
Onlay Resurfacing ArthroplastyA UKR by any other name???
• Onlay optimizes fit of implant to bone
• Onlay minimizes bone resection
• Onlay accounts for alignment and patient specific anatomy using pre-op data acquisition
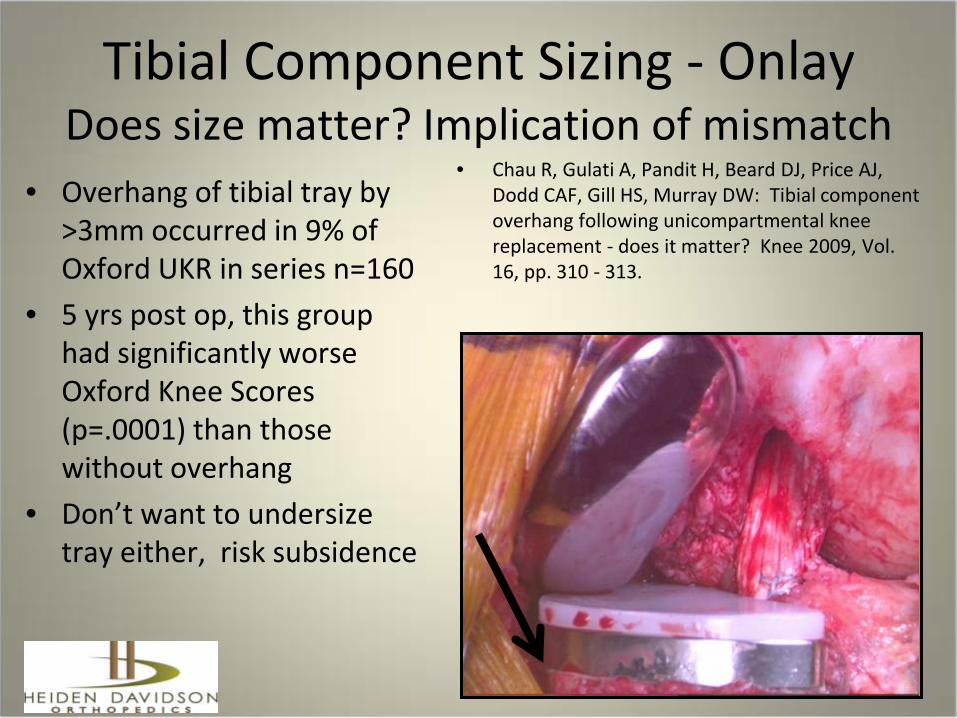
Tibial Component Sizing - OnlayDoes size matter? Implication of mismatch
• Overhang of tibial tray by >3mm occurred in 9% of Oxford UKR in series n=160
• 5 yrs post op, this group had significantly worse Oxford Knee Scores (p=.0001) than those without overhang
• Don’t want to undersize tray either, risk subsidence
• Chau R, Gulati A, Pandit H, Beard DJ, Price AJ, Dodd CAF, Gill HS, Murray DW: Tibial component overhang following unicompartmental knee replacement - does it matter? Knee 2009, Vol. 16, pp. 310 - 313.

Onlay Resurfacing • Very little bone
resection on distal femur
• Implants custom made from CT scan
• More accurate fit may increase longevity
• Accommodate morphologic variability, “odd sizes and shapes”

Case #4Onlay
Biologic Treatment - Injured Worker
Onlay Knee Resurfacing Theoretical advantages
• Line-to-line bone conformity of components• Can preoperatively manipulate/correct malalignment
and angulation• Minimize bone resections• Simplify procedure, potentially more predictable
outcomes • Facilitate optimal load transfer, possible greater
longevity• Lesser bone cuts, theoreticallyh longer lasting, facilitate
easier and/or fewer revisions
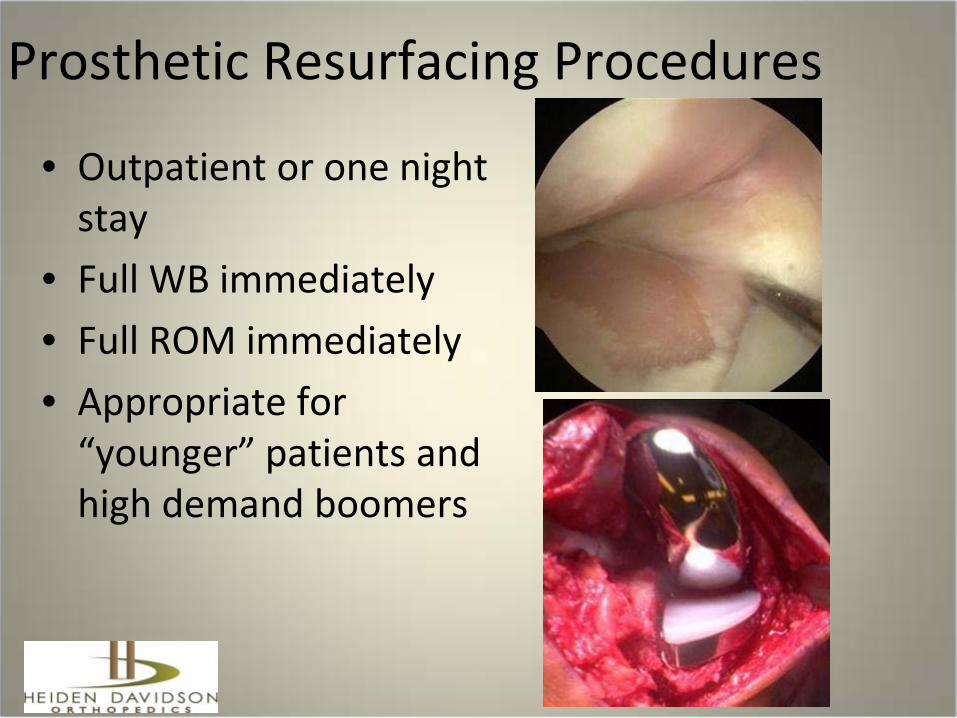
Prosthetic Resurfacing Procedures
• Outpatient or one night stay
• Full WB immediately• Full ROM immediately• Appropriate for
“younger” patients and high demand boomers

Managing Utilization-…..facilitating planning
• Arthroscopic images are extremely helpful
• MRI – 3T Fat Suppressed Fast Spin Echo, cartilage sequences
• Have multiple options available
• Role for in-office diagnostic arthroscopy??

Updating Traditional TKA• Pre op limb imaging can yield data about bone shape , size
and alignment• Alignment, sizing and intended corrections can be
precisely calculated preoperatively • This digital information can be used to plan, create cutting
guides and manufacture implants• Increases precision• Increases efficiency by: decreasing OR time, instruments,
and inventory • May lessen or obviate the need for intraoperative
navigation systems• Saves time and money while potentially making
outcomes more predictable and ultimately better.

Updating Traditional TKA
• Pre-op templated cutting guides/blocks
• Avoid/minimize intraoperative intra and extra medullary alignment guides
• These traditional guides can be used as “double-check”
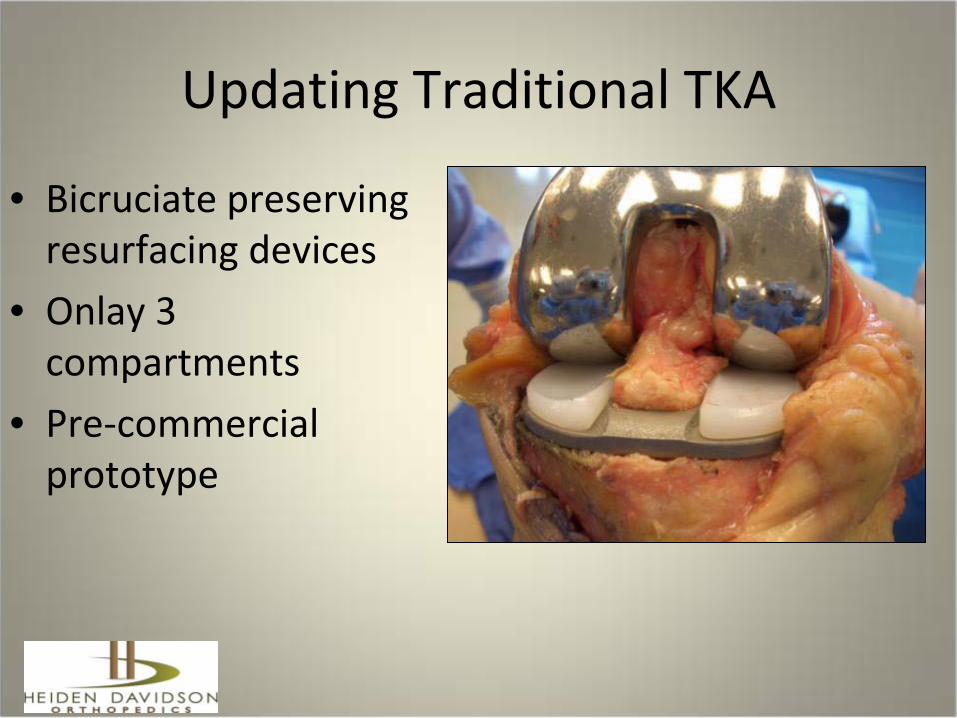
Updating Traditional TKA
• Bicruciate preserving resurfacing devices
• Onlay 3 compartments
• Pre-commercial prototype
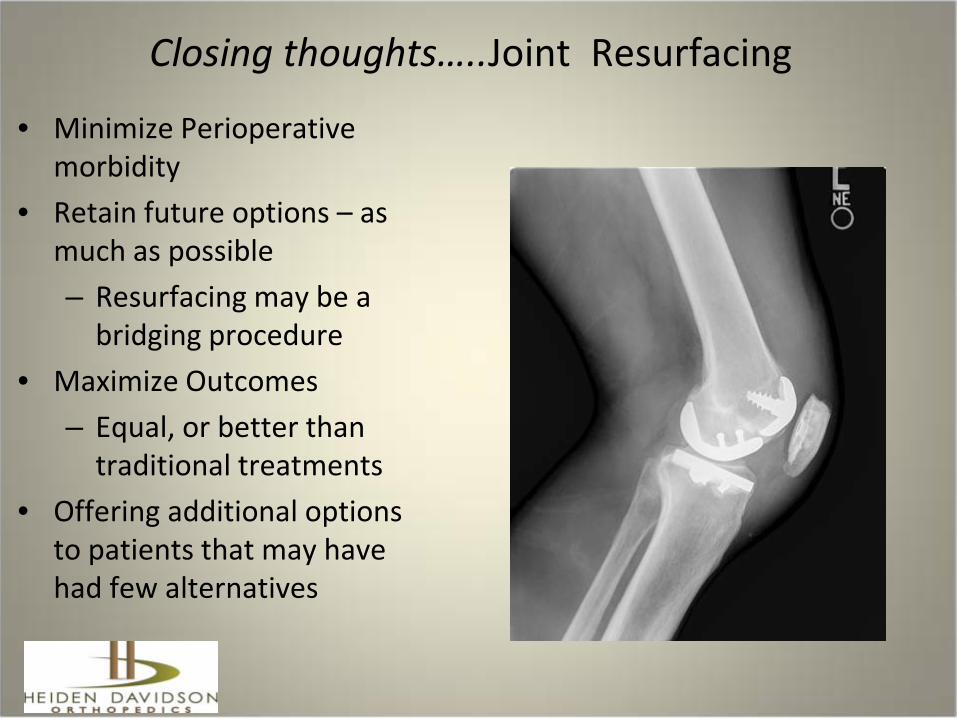
Closing thoughts…..Joint Resurfacing
• Minimize Perioperative morbidity
• Retain future options – as much as possible– Resurfacing may be a
bridging procedure• Maximize Outcomes
– Equal, or better than traditional treatments
• Offering additional options to patients that may have had few alternatives
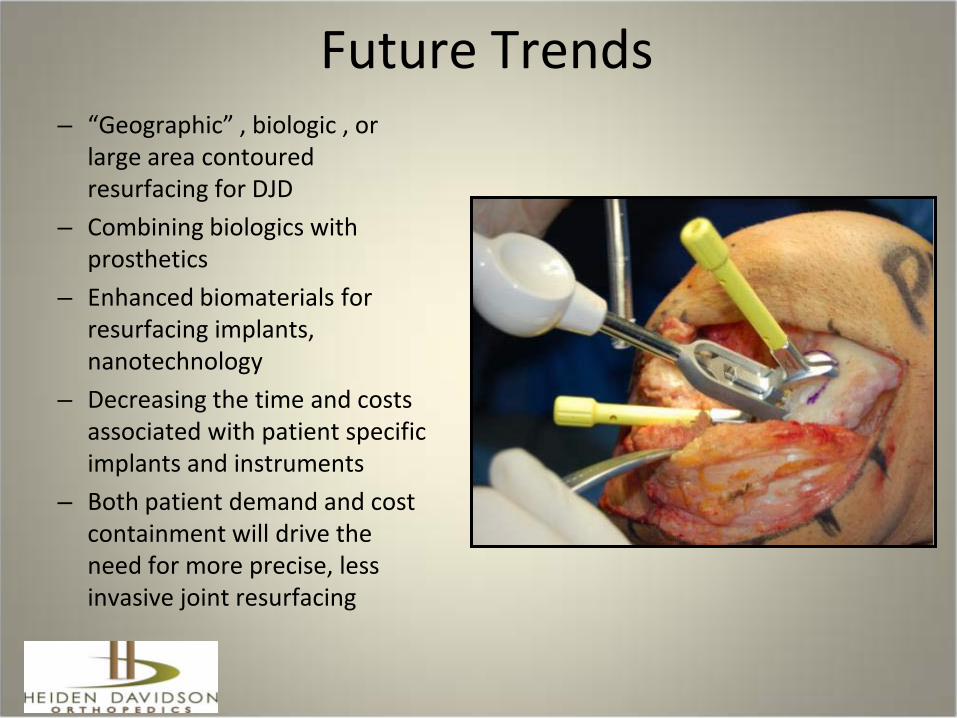
Future Trends– “Geographic” , biologic , or
large area contoured resurfacing for DJD
– Combining biologics with prosthetics
– Enhanced biomaterials for resurfacing implants, nanotechnology
– Decreasing the time and costs associated with patient specific implants and instruments
– Both patient demand and cost containment will drive the need for more precise, less invasive joint resurfacing
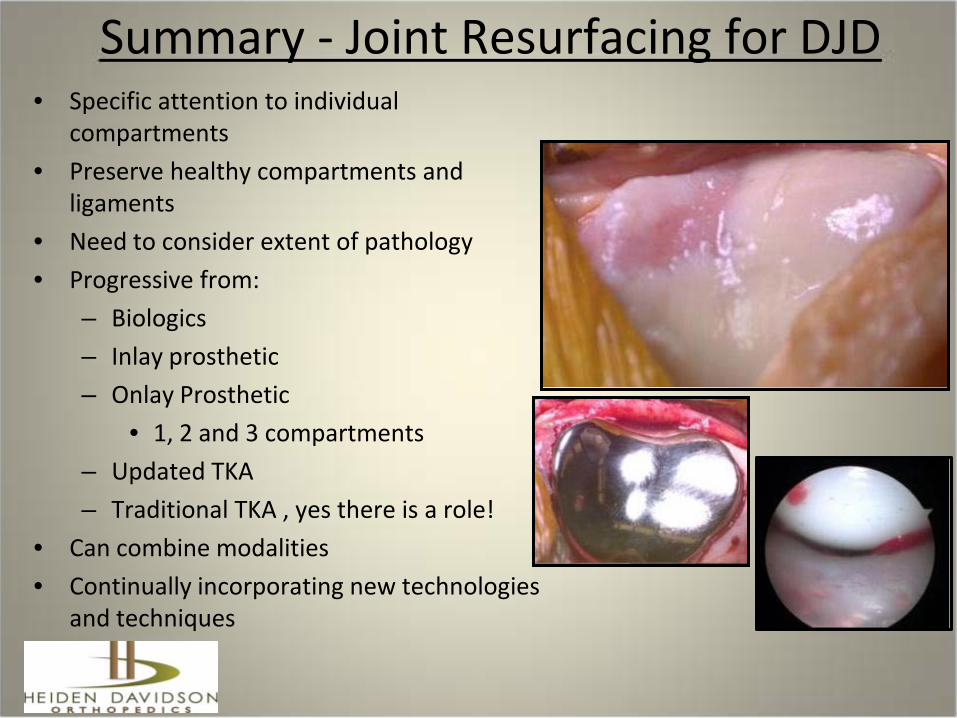
Summary - Joint Resurfacing for DJD• Specific attention to individual
compartments• Preserve healthy compartments and
ligaments• Need to consider extent of pathology • Progressive from:
– Biologics – Inlay prosthetic – Onlay Prosthetic
• 1, 2 and 3 compartments– Updated TKA – Traditional TKA , yes there is a role!
• Can combine modalities • Continually incorporating new technologies
and techniques