Embed Size (px)
Citation preview

Results of Surgery for Ocular Toxocara canis WILLIAM S. HAGLER, MD, ZANE F. POLLARD, MD, WILLIAM H. JARRETT, MD, EDWIN H. DONNELLY, MD
Abstract: It has been shown that the diagnosis of ocular Toxocara canis is highly accurate when the typical clinical findings are associated with a positive ELISA titer in the serum of 1:8 or greater. The inflammatory reaction in this disorder can be devastating and not infrequently leads to a tractional detachment of the posterior pole or a rhegmatogenous detachment and/or a progressive cyclitic membrane leading to phthisiS bulbi. We have recently performed vitreoretinal surgery on 17 patients with complications secondary to ocular T canis. Fifteen patients had stability or improvement in visual acuity, and one patient had a decrease in visual acuity. There were no surgical complications present. The clinical features, operative techniques used, and postoperative course are summarized, and the indications for the use of various surgical procedures are presented. [Key words: ELISA, scleral buckle, Toxocara canis, traction retinal detachment, vitrectomy.] Ophthalmology 88:1081-1086, 1981
Toxocara canis, the common roundworm of dogs, is a much more common human parasite than previously recognized. Demographic surveys indicate that between one third and one half of all households in the United States have one or more dogs, most of which are infected with T canis as puppies.! Surveys in the New York City area have shown that the prevalence of infection in puppies two to six months of age is greater than 80%. Each adult female worm may shed at least 200,000 ova a day and these eggs may survive in humid soil for many months. Thus the risk of human contamination with T canis is great, both in urban and rural environments.
Human infection occurs when the eggs of the dog roundworm are accidentally ingested, and this can result in severe systemic consequences, which occasionally are fatal. 2 Human infection can take one of two forms. A generalized systemic involvement is termed visceral larva migrans (VLM) and is the more common syndrome. A second syndrome consisting of ocular involvement alone has also been identified. This
Reprint requests to William S. Hagler, MD, 2004 Peachtree Road, NW, Atlanta, GA 30367.
has been referred to by a number of terms including ocular T canis, ocular toxocarasis, nematode endophthalmitis, and toxocara endophthalmitis. We prefer the term ocular T canis because it is more specific, and because not all cases result in an endophthalmitis-type picture. The ocular T canis syndrome is usually seen in the absence of the visceral larva migran syndrome and may result in loss of the eye.
As of 1970, there were only 245 published case reports of ocular T canis. 3 The exact incidence of ocular T canis has never been determined, but it has been estimated that approximately 10% of all cases of uveitis in Britain are caused by this infection.4 Leopold reported a series of 1,000 enucleations in children under the age of 15 and nematode endophthalmitis was diagnosed in 2% of these globes. 5
The clinical manifestations of ocular T canis can vary widely. Although 14 clinical manifestations have been described, only three are common. They consist of either a peripheral or posterior pole granuloma in a quiet eye or an endophthalmitis-type picture mimicking a retinoblastoma. In any of the above cases a tractional, rhegmatogenous, or exudative retinal detachment may occur.
Following the development of the enzyme linked
0161-6420/8111000/10811$00.80 © American Academy of Ophthalmology 1081
OPHTHALMOLOGY. OCTOBER 1981 • VOLUME 88. NUMBER 10
immunosorbend assay (ELISA) test for visceral larva migrans, 6 Pollard et al showed that this test was highly sensitive and specific in patients with the ocular T canis syndrome. 7 Since the publication of these articles, this test has become readily available and the diagnosis of ocular toxocara canis is now being made more easily.
While the use of the ELISA test and a greater clinical awareness of this syndrome has reduced the incidence of enucleations for suspected retinoblastoma, the actual treatment of these inflamed eyes remains difficult. Although steroids and or antihelmintics may produce some quieting of an inflamed eye, they rarely have any effect once vitreous membrane formation has occurred. These vitreous membranes may result in either a tractional or rhegmatogenous retinal detachment, and for these reasons, we have cautiously performed various types of retinal detachment and vitrectomy procedures in an attempt to restore or improve vision in these eyes. In some cases, although the vision has not been improved, the use of surgery has resulted in a quiet eye with prevention of progressive changes and enucleation.
MATERIALS AND METHODS
Since 1976, we have performed vitrectomy and/or scleral buckling procedures on 17 patients with the ocular T canis syndrome who had serologic confirmation of infection with the ELISA test (Table 1). None of these patients had a past or present history compatible with visceral lava migrans.
The visual acuity of our patients was markedly diminished at the time of their initial presentation. All of our patients had an initial visual acuity of 20/200 or worse. Multiple factors were present to account for the diminished vision. The macula in 16 cases was involved either by a retinal detachment or by dragging from a peripheral or posterior pole granuloma. Although only three patients were felt to have an active infection at the time of surgery, 16 patients had some degree of vitreous inflammation accounting for decreased vision. One patient was felt to have cystoid macular edema. Six patients had cataracts at the time of surgery. We reviewed the records of these patients to analyze the type of surgery, results, complications, and visual outcome. All patients have been followed from 6 to 48 months.
1082
Table 1. Ocular Toxocara canis
Type Surgery
Scleral buckle alone Vitrectomy (Iensectomy) Vitrectomy and scleral buckle
Total
No. Patients
3 9 5
17
RESULTS
Ten of the 17 patients operated on were males and 7 were females. Caucasians comprised 12 of the 17, and there were 5 noncaucasians. The age at the time of surgery ranged from 2 years to 22 years, with an average of 8.8 years.
All 17 patients had a retinal detachment. Of the 17 patients, nine were found to have peripheral involvement, and eight had a posterior pole granuloma. Of the nine with peripheral lesions, five had a diffuse pars planitis-type syndrome, one had a cyclitic membrane, and the other three had an isolated granuloma.
The macula was detached in 16 patients, and vitreous bands were present in nine patients. Eight patients had retinal tears, with six of these tears being a peripheral retinal dialysis.
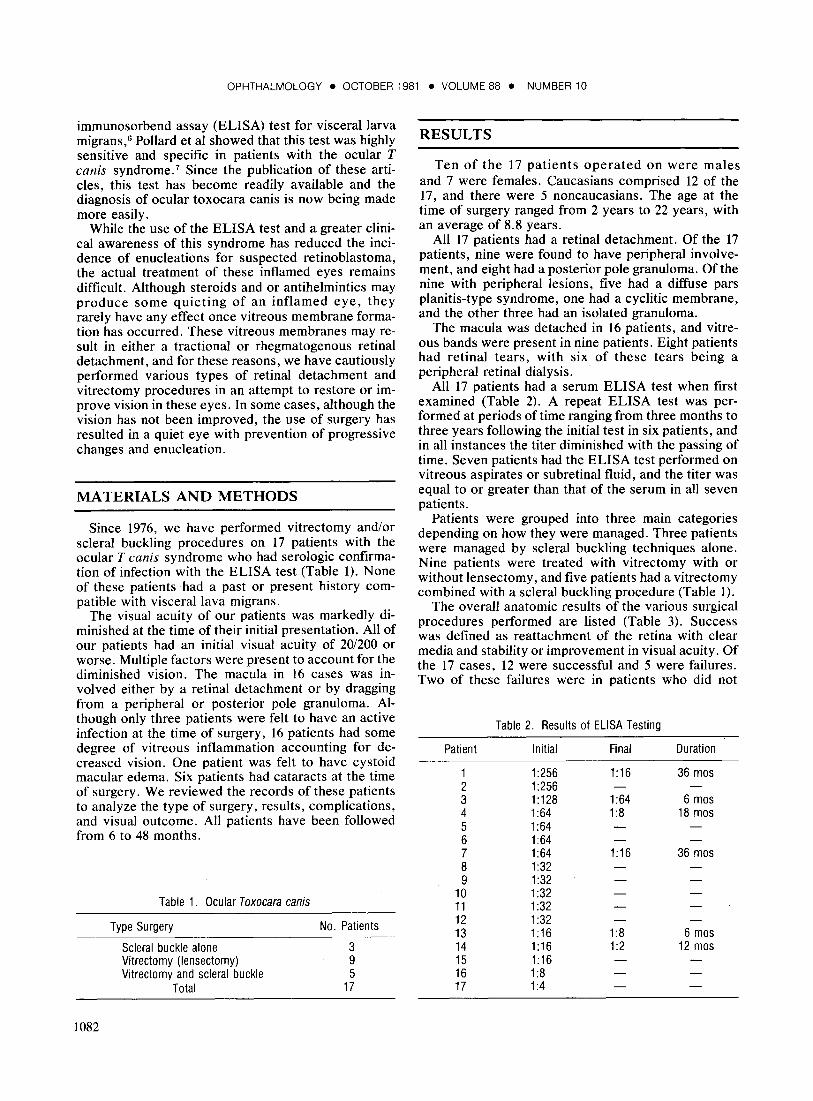
All 17 patients had a serum ELISA test when first examined (Table 2). A repeat ELISA test was performed at periods of time ranging from three months to three years following the initial test in six patients, and in all instances the titer diminished with the passing of time. Seven patients had the ELISA test performed on vitreous aspirates or subretinal fluid, and the titer was equal to or greater than that of the serum in all seven patients.
Patients were grouped into three main categories depending on how they were managed. Three patients were managed by scleral buckling techniques alone. Nine patients were treated with vitrectomy with or without lensectomy, and five patients had a vitrectomy combined with a scleral buckling procedure (Table I).
The overall anatomic results of the various surgical procedures performed are listed (Table 3). Success was defined as reattachment of the retina with clear media and stability or improvement in visual acuity. Of the 17 cases, 12 were successful and 5 were failures. Two of these failures were in patients who did not
Patient
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17
Table 2. Results of ELISA Testing
Initial
1:256 1:256 1 :128 1 :64 1 :64 1:64 1:64 1:32 1:32 1:32 1:32 1:32 1 :16 1 :16 1 :16 1 :8 1 :4
Final
1 :16
1:64 1 :8
1 :16
1:8 1 :2
Duration
36 mos
6 mos 18 mos
36 mos
6 mos 12 mos

HAGLER, et al • RESULTS OF SURGERY FOR OCULAR TOXOCARA CANIS
Table 3. Ocular Toxocara canis Results of Surgery
VA
Stable or Success Failure Improved Worse
Retinal detachment procedure only Vitrectomy with or w/out lensectomy only
Vitrectomy-inoperable rd Vitrectomy-enucleation
Vitrectomy & rd procedure
undergo definitive surgery and only had vitrectomies as an exploratory form of surgery that revealed an inoperable retinal detachment in one and in another a clinical appearance so suggestive of a retinoblastoma that in spite of a positive ELISA test the eye was enucleated. There were four patients that required multiple procedures, and two of these were successful and two failures. In spite of the failure to effect anatomic reattachment of the retina, all 15 patients that were operated on in an attempt to fix the detachment, had at least stability if not improvement in their visual acuity. Of the remaining two patients in this series who did not have definitive surgery, one patient with an inoperable retinal detachment had a decrease in the vision from hand motions to no light perception. Overall, seven patients had a final acuity of 20/200 or better, two of these seven had a visual acuity of 20/50, and three had final acuities of 20/60 to 20/80.
CASE REPORTS
Case 1. JL, a lO-year-old white male, was first seen for blurred vision. His visual acuity in the right eye was 20/400, and he had a diffuse pars planitis-type syndrome with heavy , old, white inflammatory exudates along his inferior ora serrata. An inferior rhegmatogenous retinal detachment involving the macula was present, stemming from a peripheral retinal dialysis. The serum ELISA test was positive I :64. A scleral buckling procedure was performed in September 1976. Postoperatively his media were clear, his retina flat, and his visual acuity was 201100. This case serves to illustrate that the unilateral pars planitis syndrome can be caused by T callis, and in some instances, a rhegmatogenous retinal detachment produced by T callis endophthalmitis can be cured by standard scleral buckling procedures without a vitrectomy.
Case 2. JW, a 9-year-old white male, was seen with a complaint of blurred vision. His visual acuity in the right eye was 3/200, and a diffuse vitreous haze was present with an active vascularized peripheral granuloma and tractional retinal detachment involving the posterior pole. Vitreous bands were present. His serum ELISA test was positive at 1:64, and he was initially treated with steroids and thiabendazole . Following the resolution of his vitreous reaction, a pars plana vitrectomy was performed with the Ocutome®. A vitreous ELISA test was positive at 1: 128. Following release of his tractional retinal detachment, his visual acuity improved to 20/70, his retina was flat, and his media were clear. This
3 6
3
0 3 0 1 7 1 0 1 1 0 1 2 5 0
case illustrates the fact that dense vitreous membranes may occur in ocular T canis and that recent tractional detachment of the macula can be repaired successfully with good return of vision by a vitrectomy procedure without scleral buckling.
DISCUSSION
Ocular involvement with nematodes was first described in 1950, when Wilder8 at the Armed Forces Institute of Pathology (AFIP) examined 46 eyes enucleated with a presumptive diagnosis of retinoblastoma. These eyes exhibited pathological evidence of granulomatous inflammation. Of these 46 eyes, 24 had larva or larval remnants, and 22 showed eosinophilic abscesses suggestive of parasitic involvement. In 1956 Nichols 9 re-examined these specimens and identified T canis larva in five. Thus it became well recognized that a diffuse endophthalmitis mimicking retinoblastoma could result from infection with Toxocara larva. In 1959 Irvine and Irvine 10 gave the first report of a peripheral fundus involvement by a nematode, and in 1960 Ashton ll
described a posterior pole granuloma of the fundus felt to be due to T canis. Thus the three main syndromes, endophthalmitis, peripheral, and posterior granuloma, were described. The clinical syndrome of ocular T canis differs markedly from VLM. A history of pica is less common, and the average age of ocular patients is considerably older, 7.5 years compared with 2 years in VLM. Ocular cases usually have a normal white blood cell count with a normal eosinophil count and no hepatomegaly. Visceral larva migrans rarely co-exists with ocular Toxocara. Of the 245 patients reviewed by Brown with ocular toxocara, only five of these had a history of VLM.3 Pollard et al reported 41 cases of ocular Toxocara, and only two of these had a history compatible with previous VLM.7 Meyers reported 17 cases of ocular Toxocara. and only two of these had a history compatible with the VLM syndrome. 12 In our present series of 17 patients operated on, none has had a past or present history compatible with VLM.
There is no evidence that there is any sexual or racial preference for human ocular T canis infection. We do not believe there is a significnce to the fact that males slightly outnumbered females in our series (10:7) and that caucasians outnumbered noncausians (12:5).
1083

OPHTHALMOLOGY • OCTOBER 1981 • VOLUME 88 • NUMBER 10
CLINICAL PRESENTATION
The ocular findings in T canis infestation are numerous. Fourteen types have been described,13 but only chronic endophthalmitis, posterior pole granulomas, and peripheral granulomas in a quiet eye are common.
Granulomas appear the same whether they exist in the posterior pole or peripherally. They are frequently white uninflamed hemispheric masses roughly two disc diameters or larger in size. The density of the granuloma is dependent on the degree of granulomatous tissue, inflammatory cells, and edema present. Retinal tension lines may radiate from the peripheral and posterior pole granulomas, and fibrous bands may extend into the vitreous and pars plana. 14 Granulomas are usually solitary and unilateral.
All 17 of our patients were selected because they had retinal detachments. Of these 17, nine patients had a peripheral rhegmatogenous type detachment, seven had a tractional detachment of the posterior pole, and one had a combination of the two. Of the nine patients with a rhegmatogenous type of detachment, five had peripheral retinal dialyses. It should be emphasized that in several instances the dialysis was not actually visualized until surgery when the media had cleared and careful indirect ophthalmoscopy with scleral depression was performed. Granulomas are usually solitary and unilateral. In all 17 of our surgical cases, only one eye was involved.
Cyclitic membranes may form and, by circumferential traction, pull the ciliary body away from the sclera causing hypotony and, eventually, a phthisical eye. One of our 17 patients had a cyclitic membrane. Although an exudative retinal detachment has been reported,t5 this is rare and retinal detachments are usually tractional or rhegmatogenous in nature as our series demonstrates.
An endophthalmitis may occur from a granuloma in either a peripheral or posterior pole location. This may manifest itself with decreased vision, leukokoria, and squint. A chronic uveitis of this type may result in vitreous membranes and give rise to tractional or rhegmatogenous retinal detachments. Although we have not had the opportunity to follow all of our patients from the initiation of their disease, it has been our impression that many times vitreous membranes and tractional detachments can occur without an endophthalmitis and may be found when there is no history of an inflamed eye. A unilateral pars planitis type syndrome may occur, and five of our surgical cases had this syndrome. In all five of these patients, there was a heavy exudate in the vitreous base overlying the peripheral retina and pars plana.
We have recently summarized our experience with ocular T canis. A random sample of 100 cases of ocular T canis seen by the above authors was tabulated. From this random sample, we found that posterior pole granulomas occurred in 46% of patients. These were associated with a peripheral mass in another 2m.
1084
Peripheral masses and retinal detachments occurred in 11%, and the pars planitis-type syndrome occurred in 8%. Endophthalmitis occurred in 5.1% (Table 4).
TESTING (TABLE 5)
Of our 17 patients, all had a positive ELISA test. Two of these were positive at 1:4, and the rest were positive at 1:8 or greater. In seven patients, subretinal fluid or vitreous fluid was subjected to the ELISA test and in all ofthese, the titer was equal to or greater than that obtained from the serum. The taking of these samples may help in the diagnosis of borderline cases. In one of our patients with a serum titer of 1:4, the subretinal fluid was positive at 1: 128.
It is important to determine the serial course of serum ELISA titers. No one yet has determined whether these titers remain stable or gradually decline with the passage of time in ocular T canis. We have recently initiated a study to determine this, and follow-up titers have been obtained in 6 of the 17 patients in this series. It is most interesting that the titer has fallen in every instance at least one dilution and in several instances several dilutions (Table 2).
Recently Pollard 16 has reported on ocular Toxocara occurring in siblings of two families. For this reason we feel strongly that other family members of patients with the ocular T canis syndrome should be tested with the ELISA test.
DIFFERENTIAL DIAGNOSIS
From a review of the literature, a number of different entities have been confused with ocular T canis. 14
Retrolental fibroplasia is typically bilateral and without inflammation. Congenital folds of the retina classically begin at the disc and radiate to a large fibrous extension in the periphery. However, they are nearly always associated with some persistence ofthe hyaloid system and there is usually no sign of active inflammation. As mentioned earlier, a unilateral pars planitis
Table 4. Findings in 100 Cases of Ocular Toxocara canis
Presentation
Post pole mass Post pole mass
& peripheral mass Peripheral mass
W/RD Peripheral mass
(unilateral pars planitis)
Endophthalmitis Subcutaneous, orbital,
intralenticular, or iris granuloma
Frequency
46%
29%
11%
8% 5%
Rare

HAGLER, et al • RESULTS OF SURGERY FOR OCULAR TOXOCARA CANIS
Table 5. Sensitivity and Specificity of the ELISA for Diagnosis of Ocular Toxocara canis
Cutoff Titer of Positive
Test
1:2 1 :4 1 :8 1 :16 1:32 1 :64 1 :128 1 :256 1 :512
Sensitivity (%)
95 93 90 85 73 51 24 15 5
Specificity (%)
72 86 91 94 95 97 99
100 100
syndrome occurs in about 8% of patients clinically diagnosed as having ocular T canis. However, the typical par planitis syndrome is bilateral in 80% of patients and is frequently associated with perivasculitis, papillitis, and macular edema.
Toxoplasmosis may cause enough vitreous inflammation to make it's recognition difficult. However, there are usually daughter or satellite lesions present and old scars present also. One confusing note has been that T canis can co-exist with ocular toxoplasmosis. One of our 17 patients had a positive ELISA at 1: 16 and a positive toxoplasmosis titer at 1: 16. At one time it was suspected that the toxoplasmosis parasite invaded the T canis larva 17 but it has been shown that this does not occur. Both organisms may be present in the same sample of dirt, however, and can be ingested at the same time, causing concomitant eye involvement.
Ocular trauma can result in localized proliferative changes and inflammatory signs, but usually the history and associated injuries aid in the differentiation.
Retinoblastoma is probably the most frequently confused entity and failure to properly diagnose it can lead to dire consequences. Retinoblastoma usually occurs in a younger age group and may at times be bilateral. Evidence of growth and vitreous seeding may appear on follow-up examinations and vitreous bands are usually not present. One of our 17 patients had an obviously inoperable retinal detachment and a clinical picture so closely resembling retinoblastoma that even though the ELISA test was positive at 1:32 the eye was enucleated. This eye continued to cause controversy even among the AFIP specialists until electron microscopy was performed.
TREATMENT
Thiabendazole and diethylcarbamazine are broad spectrum antihelmintics that are of minimal value in treating ocular T canis endophthalmitis. When used, they frequently result in increased inflammation felt to be due to death of the Toxocara organism, and there-
fore, steroids are often used along with these antihelmintics. In our 17 patients, we found it difficult to determine whether the inflammatory disease was active or not. In all but one of our patients there was some degree of vitreous haze present. All patients suspected of having active infection were treated with steroids and thiabendazole prior to surgery. Three of our patients had definite inflammatory activity occur following surgery. Thiabendazole and steroids can be used in these situations.
In Wilkinson and Welch's excellent review article examining 41 eyes,14 they found that 18 had peripheral inflammatory masses that were always associated with dense connective tissue strands in the vitreous cavity. They found that many of these were attached to the posterior retina creating tractional detachments and folds in the retina. For these types of patients it is obvious that medical therapy is of limited benefit. To our knowledge there has been only one previous report of the use of vitrectomy in the ocular T canis syndrome. 18 This case involved a 5-year-old girl who had initially been treated with systemic prednisone and then subsequently formed dense vitreous membranes and a retinal detachment. A vitrectomy and scleral buckling procedure was performed. Postoperatively she had an MPP-type retinal detachment with light perception vision.
Although we do not have accurate statistics on what percentage of our total ocular T canis population has required surgery, we do feel that the 17 patients operated on would have had permanent visual loss or would have required enucleation had it not been for surgical intervention. As it was, 15 of our patients had an improvement or stability in visual acuity and all but one retained their globe.
Determining whether or not surgery is indicated or what type of surgery to perform is not always an easy and clear cut decision. This requires a certain amount of judgment and estimation of the present activity of the infection and whether or not it appears that vitreous membranes are developing. If there is only minimal or moderate centripetal traction present, we feel that a standard scleral buckling procedure with some type of encircling element should at least be tried as an initial procedure. In four of our patients, a rhegmatogenous detachment was present and these were treated by scleral buckling alone. One of these patients had a reactivation of infection following scleral buckling and required a vitrectomy for a recurrent detachment. of the three patients treated by scleral buckling alone, all three were judged a success.
If only an endophthalmitis or a tractional detachment of the posterior pole is present, a vitrectomy may be all that is needed. We always hesitate to perform encircling procedures on young children due to induction of myopia and the possibility of late intrusion in patients with long life expectancies. For these reasons, even if a peripheral detachment is present with vitreous traction, a vitrectomy and the use of gas tamponade along with cryopexy would be used in favor of
1085

OPHTHALMOLOGY • OCTOBER 1981 • VOLUME 88 • NUMBER 10
a scleral buckling. One of our patients, who was treated by vitrectomy and fluid gas exchange, required a subsequent scleral buckling six months later for recurrent detachment. Of the nine patients treated by vitrectomy with or without lensectomy, six were deemed a success and three a failure. Two of these three were actually inoperable retinal detachments and vitrectomy was only performed as an exploratory procedure.
Three patients were treated initially with a vitrectomy and scleral buckling and of these three, two failed. Two subsequent patients were also treated by this combination of surgery . One of these patients had had a vitrectomy with fluid gas exchange and subsequently detached and required a scleral buckling procedure, and the other had a scleral buckling procedure with subsequent re-detachment and underwent a vitrectomy and revision of scleral buckle. Both of these cases were deemed a success . Overall then, three out of the five patients treated with a combination of vitrectomy and scleral buckling procedures were deemed a success.
All these patients have been followed from 6 to 48 months. We realize that the follow-up is short in some of these patients and that the ultimate fate of these eyes cannot be determined for several more years. We strongly advocate periodic follow-up on all these patients since visual acuity is frequently poor and these young children may not report any symptoms related to recurrent activity or recurrent retinal detachment.
SUMMARY
Our overall results for surgery indicate that 12 out of 17 cases were successful anatomically, and 15 out of 17 had a stability or improvement in vision even though their retina could not be completely attached. There were no major complications .
1086
REFERENCES
1. Schantz PM, Glickman LT. Toxocaral visceral larva migrans. N Engl J Med 1978: 298:436-9.
2. Brill R, Churg J, Beaver PC. Allergic granulomatosis associated with visceral larva migrans: case report with autopsy findings of Toxocara infection in a child. Am J Clin Pathol 1953: 23: 1208-15.
3. Brown DH. Ocular Toxocara canis. II. Clinical review. J Pediatr Ophthalmol 1970: 7:182-91
4. Perkins ES. Pattern of uveiti s in children. Br J Ophthalmol 1966: 50:169- 85.
5. Leopold IH. Is the dog really man's best fr iend? Am J Ophthalmol 1965; 59:717-9.
6. Cypess RH, Karol MH, Zidian JL, et al. Larva-specific antibodies in patients with visceral larva migrans. J Infect Dis 1977; 135:633-40.
7. Pollard ZF, Jarrett WH, Hagler, WS, et al. ELISA for diagnosis of ocular toxocariasis. Ophthalmology 1979: 86:743-9
8. Wilder HC. Nematode endophthalmitis. Trans Am Acad Ophthalmol Otolaryngol 1951: 55:99-109.
9. Nichols RL. The etiology of visceral larva migrans: I. diagnostic morphology of infective second-stage Toxocara larvae. J Parasitol 1956: 42:349-62.
10. Irvine WC, Irvine AR, Jr. Nematode endophthalmiti s, Toxocara canis. Am J Ophthalmol 1959: 47:185-91.
11. Ashton, N. Larval granulomatosis of the retina due to Toxocara Br J Ophthalmol 1960: 44:129-48.
12. Meyer D. Personal communication , Memphis, 1978. 13. Schlaegel TF Jr, Knox DL. Toxocariasis. In: Duane TO (ed) :
Clini cal Ophthalmology. Hagerstown, Maryland : Harper & Row, 1976: Vol 4, chapt 52: 8-14.
14. Wilkinson CP, Welch RB. Intraocular Toxocara. Am J Ophthalmol 1971: 71 :921-30.
15. Hogan, MJ, Kimura SJ , Spencer WH o Visceral larva migrans and peripheral retinitis. JAMA 1965; 194:1345-7.
16. Pollard , ZF. Ocular Toxocara in siblings of two families. Arch Ophthalmol 1979; 97:2319-20.
17. Hutchison WM. Recent observations on the biology of toxoplasma gondii . Trans Ophthalmol Soc UK 1966; 86:185-9.
18. Biglan AW, Glickman LT, Lobes LA Jr. Serum and vitreous toxocara antibody in nematode endophthalmiti s. Am J Ophthalmol 1979; 88:898-901 .