Embed Size (px)
Citation preview

RespiratoryRespiratory Pleural and Thoracic Pleural and Thoracic
InjuryInjury
Marnie Quick, RN, MSN, CNRNMarnie Quick, RN, MSN, CNRN

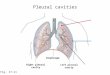
Thoracic cavityThoracic cavity
LungsLungs MediastinumMediastinum
HeartHeart Aorta and great Aorta and great
vesselsvessels EsophagusEsophagus TracheaTrachea

Breathing: inspirationBreathing: inspiration
When the diaphragm When the diaphragm contracts, it moves down, contracts, it moves down, increasing the volume of the increasing the volume of the thoracic cavity When the thoracic cavity When the volume increasesvolume increases, the , the pressurepressure inside inside decreasesdecreases
Air moves Air moves fromfrom an area of an area of higher pressure, higher pressure, the the atmosphereatmosphere,, toto an area of an area of lower pressure, lower pressure, the lungsthe lungs
Pressure within the lungs is Pressure within the lungs is called called intrapulmonary intrapulmonary pressurepressure

Breathing: exhalationBreathing: exhalation Exhalation occurs when the Exhalation occurs when the
phrenic nerve stimulus stopsphrenic nerve stimulus stops The diaphragm relaxes and The diaphragm relaxes and
moves up in the chestmoves up in the chest This This reduces the volumereduces the volume of of
the thoracic cavitythe thoracic cavity When When volume decreases, volume decreases,
intrapulmonary pressure intrapulmonary pressure increasesincreases
Air flows outAir flows out of the lungs to of the lungs to the lower atmospheric the lower atmospheric pressurepressure

BreathingBreathing
This is normally an unconscious processThis is normally an unconscious process Lungs naturally recoil, so exhalation restores Lungs naturally recoil, so exhalation restores
the lungs to their resting positionthe lungs to their resting position However, in respiratory distress, particularly However, in respiratory distress, particularly
with airway obstruction, exhalation can create with airway obstruction, exhalation can create increased work of breathing as the abdominal increased work of breathing as the abdominal muscles try to force air out of the lungsmuscles try to force air out of the lungs
If two areas of different pressure If two areas of different pressure communicate, gas will move communicate, gas will move from the area of from the area of higher pressure to the area of lower pressurehigher pressure to the area of lower pressure

Respiratory airways and Respiratory airways and unitunit

Lungs are surrounded Lungs are surrounded by thin tissue called the by thin tissue called the pleura, a continuous pleura, a continuous membrane that folds membrane that folds over itselfover itself
Parietal pleuraParietal pleura lines the lines the chest wallchest wall
Visceral pleura Visceral pleura (pulmonary)(pulmonary) covers the covers the lung lung
Pleural Pleural anatomyanatomy

Normally, the Normally, the two membranes two membranes are separated are separated only by the only by the lubricating lubricating pleural fluidpleural fluid
Fluid Fluid reduces reduces frictionfriction, allowing , allowing the pleura to the pleura to slide easily slide easily during breathingduring breathing
Pleural Pleural anatomyanatomy
Parietal pleuraParietal pleura Visceral pleura Visceral pleura
Normal Pleural Fluid Quantity: Approx. 25mL per lung
Normal Pleural Fluid Quantity: Approx. 25mL per lung
LungLung
RibsIntercostal muscles

Pleural physiologyPleural physiology
The area between the pleura is called the pleural The area between the pleura is called the pleural space (sometimes referred to as “potential space (sometimes referred to as “potential space”)space”)
Normally, vacuum (negative pressure) in the Normally, vacuum (negative pressure) in the pleural space keeps the two pleura together and pleural space keeps the two pleura together and allows the lung to expand and contractallows the lung to expand and contract
During inspiration, the During inspiration, the intrapleural pressureintrapleural pressure is is approximately approximately -8cmH-8cmH2200 (below atmosphere)(below atmosphere)
During exhalation, During exhalation, intrapleural pressureintrapleural pressure is is approximately approximately -4cmH-4cmH2200

When pressures are When pressures are disrupteddisrupted
If air or fluid enters the If air or fluid enters the pleural space between pleural space between the parietal and the parietal and visceral pleura, the -visceral pleura, the -4cmH4cmH220 pressure 0 pressure gradient that normally gradient that normally keeps the lung against keeps the lung against the chest wall the chest wall disappears and the disappears and the lung collapseslung collapses
Intrapulmonary pressure: -4cmH20
Intrapleural pressure: -8cmH20

Pleural injury:Pleural injury: Pneumothorax Pneumothorax
Etiology/Patho- air Etiology/Patho- air in pleural spacein pleural space ClosedClosed OpenOpen Tension Tension
Clinical Clinical manifestations manifestations Emergency managEmergency manag Lewis 586 Table 28-Lewis 586 Table 28-
2020

Closed PneumothoraxClosed Pneumothorax
Chest wall is intactChest wall is intact Rupture of the lung and Rupture of the lung and
visceral pleura allows visceral pleura allows air into the pleural air into the pleural spacespace
Spontaneous- no Spontaneous- no apparent cause (thin apparent cause (thin individual)individual)
Blunt trauma-CPR/fallBlunt trauma-CPR/fall Penetrating from Penetrating from
fractured ribsfractured ribs

Open PneumothoraxOpen Pneumothorax
Opening in the Opening in the chest wall chest wall
Allows atmospheric Allows atmospheric air to enter/exit the air to enter/exit the pleural space pleural space during respiration during respiration
Penetrating trauma: Penetrating trauma: stab, gunshot, stab, gunshot, impalementimpalement

Tension pneumothoraxTension pneumothorax
Tension Tension pneumothoraxpneumothorax occurs occurs when a when a closed closed pneumothoraxpneumothorax creates creates positive pressure in positive pressure in the pleural space that the pleural space that continues to buildcontinues to build
That pressure is then That pressure is then transmitted to the transmitted to the mediastinum (heart mediastinum (heart and great vessels)and great vessels)

Mediastinal shiftMediastinal shift
Mediastinal shiftMediastinal shift occurs occurs when the pressure gets when the pressure gets so high that it pushes so high that it pushes the heart and great the heart and great vessels into the vessels into the unaffected side of the unaffected side of the chestchest
These structures are These structures are compressed from compressed from external pressure and external pressure and cannot expand to cannot expand to accept blood flowaccept blood flow
Cardiovascular collapseCardiovascular collapse

Which is more life Which is more life threatening?threatening?

Pleural injury: Pleural injury: Hemothorax Hemothorax
Blood in pleural spaceBlood in pleural space Caused by trauma; lungCaused by trauma; lung malignancy; pulmonary malignancy; pulmonary
embolus; complication embolus; complication anticoagulant therapyanticoagulant therapy
Like pneumothorax- Like pneumothorax- lung can collapse lung can collapse
Manifestations similar Manifestations similar to pneumothorax; blood to pneumothorax; blood loss symptoms; dull loss symptoms; dull percussion over blood percussion over blood

Free floating rib fracture may Free floating rib fracture may result in Flail chest with paradoxic result in Flail chest with paradoxic
respirationsrespirations

Pleural effusionPleural effusion
Fluid in the pleural space is Fluid in the pleural space is pleural effusionpleural effusion TransudateTransudate is a clear fluid is a clear fluid
that collects in the pleural that collects in the pleural space when there are fluid space when there are fluid shifts in the body from shifts in the body from conditions such as CHF, conditions such as CHF, malnutrition, renal and malnutrition, renal and liver failureliver failure
ExudateExudate is a cloudy fluid is a cloudy fluid with cells and proteins with cells and proteins that collects when the that collects when the pleura are affected by pleura are affected by malignancy or diseases malignancy or diseases such as tuberculosis and such as tuberculosis and pneumonia. Pus-empyemapneumonia. Pus-empyema

Pleural effusion- common Pleural effusion- common manifestations and collaborative manifestations and collaborative
carecare Common manifestationsCommon manifestations
Dyspnea, pleuritic pain, dec/absent breath sounds, Dyspnea, pleuritic pain, dec/absent breath sounds, limited chest wall movementlimited chest wall movement
Diagnostic tests- Chest X-ray; CT; analysis of Diagnostic tests- Chest X-ray; CT; analysis of aspirated fluid from thoracentesisaspirated fluid from thoracentesis
Treatment- Treatment- Thoracentesis- insert needle into space to drain Thoracentesis- insert needle into space to drain
fluidfluid Treat underlying causeTreat underlying cause administer O2administer O2

Thoracentesis- needle to Thoracentesis- needle to remove fluidremove fluid

Collaborative care for Collaborative care for pleural/thoracic Injuriespleural/thoracic Injuries
Diagnostic tests- chest X-ray; CT; O2 sats; ABG’s/CBC; Diagnostic tests- chest X-ray; CT; O2 sats; ABG’s/CBC; analysis of aspirated fluid; pulmonary function studiesanalysis of aspirated fluid; pulmonary function studies
High Fowlers; O2; rest to dec O2 demandHigh Fowlers; O2; rest to dec O2 demand Treatment depends on severity- chest tube to restore Treatment depends on severity- chest tube to restore
negative pressurenegative pressure Emergency management chest trauma (Lewis p 567 Emergency management chest trauma (Lewis p 567
Table 28-21)Table 28-21) Emergency management thoracic injury (Lewis p 566 Emergency management thoracic injury (Lewis p 566
Table 28-20)Table 28-20)

Chest SurgeriesChest SurgeriesLewis 567 Table 28-22Lewis 567 Table 28-22
Exploratory thoracotomyExploratory thoracotomy Incision into thorax to look for injured or Incision into thorax to look for injured or
bleeding tissuebleeding tissue Thoracotomy not involving lungThoracotomy not involving lung VATSVATS
Video-assisted thoracic surgery to do Video-assisted thoracic surgery to do lung biopsy, lobectomy, ectlung biopsy, lobectomy, ect

Chest Tubes– to remove air & Chest Tubes– to remove air & fluid fluid
Also called “thoracic catheters”
Different sizes From infants to adults Small for air, larger for
fluid Different configurations
Curved or straight Types of plastic
PVC Silicone
Coated/Non-Coated Heparin Decrease friction

Chest tube insertionChest tube insertion
Choose site
Explore with finger
Place tube with clamp
Suture tube to chest
Photos courtesy trauma.org

Different placement of chest Different placement of chest tubes to remove air & to tubes to remove air & to
remove fluidremove fluid

Chest tubes in placeChest tubes in place

Prevent air & fluid from Prevent air & fluid from returning to the pleural spacereturning to the pleural space
Chest tube is attached to a Chest tube is attached to a drainage devicedrainage device Allows air and fluid to leave the chestAllows air and fluid to leave the chest Contains a one-way valve to prevent air & Contains a one-way valve to prevent air &
fluid returning to the chestfluid returning to the chest Designed so that the device is below the Designed so that the device is below the
level of the chest tube for gravity level of the chest tube for gravity drainage or attached to suctiondrainage or attached to suction
What happens if you clamp the chest What happens if you clamp the chest tube?tube?

Water suction on left Dry suction Water suction on left Dry suction rightright
Lewis p. 570 Fig 28-8 Lewis p. 570 Fig 28-8

Prevent air & fluid from returning to the pleural space
Prevent air & fluid from returning to the pleural space
Most basic conceptMost basic concept Straw attached to Straw attached to
chest tube from chest tube from patient is placed under patient is placed under 2cm of fluid (water 2cm of fluid (water seal)seal)
Just like a straw in a Just like a straw in a drink, air can push drink, air can push through the straw, but through the straw, but air can’t be drawn air can’t be drawn back up the strawback up the straw
Most basic conceptMost basic concept Straw attached to Straw attached to
chest tube from chest tube from patient is placed under patient is placed under 2cm of fluid (water 2cm of fluid (water seal)seal)
Just like a straw in a Just like a straw in a drink, air can push drink, air can push through the straw, but through the straw, but air can’t be drawn air can’t be drawn back up the strawback up the straw
Tube open to atmosphere vents air
Tube from patient

Prevent air & fluid from Prevent air & fluid from returning to the pleural spacereturning to the pleural space
For drainage, a second For drainage, a second bottle was addedbottle was added
The first bottle collects The first bottle collects the drainagethe drainage
The second bottle is The second bottle is the water sealthe water seal
With an extra bottle With an extra bottle for drainage, the for drainage, the water seal will then water seal will then remain at 2cm remain at 2cm

Restore negative pressure in Restore negative pressure in the pleural spacethe pleural space
Many years ago, it was believed that Many years ago, it was believed that suction was always required to pull air and suction was always required to pull air and fluid out of the pleural space and pull the fluid out of the pleural space and pull the lung up against the parietal pleuralung up against the parietal pleura
However, recent research has shown that However, recent research has shown that suction may actually prolong air leaks from suction may actually prolong air leaks from the lung by pulling air through the opening the lung by pulling air through the opening that would otherwise close on its ownthat would otherwise close on its own
If If suctionsuction is required, a is required, a third bottlethird bottle is added is added

Restore negative pressure in Restore negative pressure in the pleural spacethe pleural space
The The depth of the depth of the waterwater in the suction in the suction bottle determines bottle determines the amount of the amount of negative pressure negative pressure that can be that can be transmitted to the transmitted to the chest, chest, NOT the NOT the reading on the reading on the vacuum regulatorvacuum regulator

How a chest drainage system How a chest drainage system worksworks
Expiratory positive pressureExpiratory positive pressure from the from the patient helps push air and fluid out of patient helps push air and fluid out of the chest (cough, Valsalva)the chest (cough, Valsalva)
GravityGravity helps fluid drainage as long as helps fluid drainage as long as the chest drainage system is below the chest drainage system is below the level of the chestthe level of the chest
SuctionSuction can improve the speed at can improve the speed at which air and fluid are pulled from the which air and fluid are pulled from the chestchest

From bottles to one boxFrom bottles to one box

At the bedsideAt the bedside
Keep drain below the chest Keep drain below the chest for gravity drainagefor gravity drainage
This will cause a This will cause a pressure pressure gradientgradient with relatively with relatively higher pressure in the higher pressure in the chestchest
Fluid, like air, moves from Fluid, like air, moves from an area of higher pressure an area of higher pressure to an area of lower to an area of lower pressurepressure
Same principle as raising Same principle as raising an IV bottle to increase an IV bottle to increase flow rateflow rate

Setting up the Chest drainage Setting up the Chest drainage systemsystem
Follow the manufacturer’s instructions for Follow the manufacturer’s instructions for adding water to the 2cm level in the water adding water to the 2cm level in the water seal chamber, and to the 20cm level in the seal chamber, and to the 20cm level in the suction control chamber (unless a different suction control chamber (unless a different level is ordered)level is ordered)
Connect 6' patient tube to thoracic catheterConnect 6' patient tube to thoracic catheter Connect the drain to vacuum, and slowly Connect the drain to vacuum, and slowly
increase vacuum until increase vacuum until gentle bubblinggentle bubbling appears in the suction control chamberappears in the suction control chamber

Setting up suctionSetting up suction
Vigorous bubbling is Vigorous bubbling is loudloud and disturbing to and disturbing to most patientsmost patients
Will also cause Will also cause rapid evaporationrapid evaporation in the in the chamber, which will chamber, which will lower suction levellower suction level
Too much bubbling is Too much bubbling is not needed clinicallynot needed clinically in 98% of patients – more is not betterin 98% of patients – more is not better
If too much, turn down vacuum source If too much, turn down vacuum source until bubbles go away, then slowly until bubbles go away, then slowly increase until they reappear, then stopincrease until they reappear, then stop

MonitoringMonitoring
Water seal is a window Water seal is a window into the pleural spaceinto the pleural space
Not only for pressureNot only for pressure If air is leaving the chest, If air is leaving the chest,
bubbling will be seen herebubbling will be seen here Air meter (1-5) provides a Air meter (1-5) provides a
way to “measure” the air way to “measure” the air leaving and monitor overleaving and monitor over
time – getting better or time – getting better or worse?worse?

Disposable chest Disposable chest drainsdrains
Collection chamberCollection chamber Fluids drain directly into chamber, calibrated Fluids drain directly into chamber, calibrated
in mL fluid, write-on surface to note level and in mL fluid, write-on surface to note level and time When full will need to change ENTIRE time When full will need to change ENTIRE systemsystem
Water sealWater seal One way valve, U-tube design, can monitor One way valve, U-tube design, can monitor
air leaks & changes in intrathoracic pressureair leaks & changes in intrathoracic pressure Suction control chamberSuction control chamber
U-tube, narrow arm is the atmospheric vent, U-tube, narrow arm is the atmospheric vent, large arm is the fluid reservoir, system is large arm is the fluid reservoir, system is regulated, easy to control negative pressureregulated, easy to control negative pressure

Portable chest drainage Portable chest drainage systemsystem

What about dependent What about dependent loops?loops?

If chest tube comes out? Three sided If chest tube comes out? Three sided taped gauze! What happens if all 4 taped gauze! What happens if all 4
sides taped?sides taped?

Nursing assessment and pertinent Nursing assessment and pertinent nursing problems/interventionsnursing problems/interventions
Health history-respiratory disease, injury, Health history-respiratory disease, injury, smoking, progression of symptomssmoking, progression of symptoms
Physical exam- degree of apparent resp distress, Physical exam- degree of apparent resp distress, lung sounds, O2 sat, VS, LOC, neck vein lung sounds, O2 sat, VS, LOC, neck vein distention, position of tracheadistention, position of trachea
All require observation for lung symptomsAll require observation for lung symptoms Pertinent nursing problemsPertinent nursing problems
Acute painAcute pain Ineffective airway clearanceIneffective airway clearance Impaired gas exchangeImpaired gas exchange Home careHome care Nursing Care Plans Thoracotomy 28-2 & Chest tube 28-Nursing Care Plans Thoracotomy 28-2 & Chest tube 28-
2121

Atrium chest video -WebsiteAtrium chest video -Website
If desire more information go to the If desire more information go to the websitewebsite
Once on website- go to the bottom of Once on website- go to the bottom of the page and select video player to the page and select video player to view videosview videos
http://www.atriummed.com/Products/Chest_Drains/edu-ocean.asp

Est of thoracic expansion:Est of thoracic expansion:A. ExhalationA. Exhalation
B. Maximal inhalationB. Maximal inhalation

Normal auscultatory soundsNormal auscultatory sounds

Lung percussions areas & Lung percussions areas & sounds sounds