Embed Size (px)
DESCRIPTION
The Urology Nurse - NP/PA November 2010, VOL 2, NO 6 • SUPPLEMENT
Citation preview

S U P P L E M E N T
©2010 Novellus Healthcare Communications, LLC
November 2010 www.TheUrologyNurse.com VOL 2, NO 6 • SUPPLEMENT
Brought to you by Watson, the manufacturer of
In Recognition ofUrology Nurses
and Associates Week
Society of UrologicNurses and Associates(SUNA) 2010
Reports from the

We CelebrateYour Commitment to Caring
Urology Nurses and Associates Week
Watson would like to say thank you to the
urologic healthcare professionals who provide
unique and challenging care every day.
During the week of November 1-7, Watson
will join the Society of Urologic Nurses and
Associates (SUNA) to celebrate urologic
healthcare professionals everywhere.
At Watson, we share your commitment to
urologic health. Our therapeutic portfolio
includes products for 3 of the top 5 urologic
conditions—BPH,* prostate cancer, and OAB.†
By specializing in treatment options that
continue to change the landscape of urology,
Watson is helping people live better.
© 2010, Watson Pharma, Inc., Morristown, NJ 07960. All rights reserved. 06877 9/10
*Benign prostatic hyperplasia†Overactive bladder

Novellus Healthcare Communications � 3
TABLE OF CONTENTS
EDITORIAL CORRESPONDENCE should be addressedto EDITORIAL DIRECTOR, Novellus Healthcare Com-munications, LLC, 241 ForsgateDrive, Suite 205D,MonroeTownship, NJ 08831. E-mail: [email protected]: CORRESPONDENCE REGARDINGSUBSCRIPTIONS OR CHANGE OF ADDRESS shouldbe directed to CIRCULATION DIRECTOR, NovellusHealthcare Communications, LLC, 241 Forsgate Drive,Suite 205D, Monroe Township, NJ 08831. YEARLY SUB-SCRIPTION RATES: One year: $99.00 USD; Two years:$149.00 USD; Three years: $199.00 USD. Correspondenceregarding permission to reprint all or part of any articlepublished in this journal should be addressed toREPRINT PERMISSIONS DEPARTMENT, NovellusHealthcare Communications, LLC, 241 Forsgate Drive,Suite 205D, Monroe Township, NJ 08831. The ideas andopinions expressed in The Urology Nurse®-NP/PA do notnecessarily reflect those of the Editorial Board, theEditorial Director, or the Publisher. Publication of anadvertisement or other product mention in The UrologyNurse®-NP/PA should not be construed as an endorse-ment of the product or the manufacturer’s claims.Readers are encouraged to contact themanufacturerwithquestions about the features or limitations of the productsmentioned. Neither the Editorial Board nor the Publisherassumes any responsibility for any injury and/or dam-age to persons or property arising out of or related to anyuse of the material contained in this periodical. Pleaseconvey any errors to the Editorial Director. The UrologyNurse®-NP/PA: ISSN# applied for.
The Urology Nurse®-NP/PA is published by NovellusHealthcare Communications, LLC, 241 Forsgate Drive,Suite 205D,Monroe Township, NJ 08831. Telephone: 732-992-1891. Fax: 732-656-7938. Copyright ©2010 byNovellus Healthcare Communications, LLC. All rightsreserved. The Urology Nurse®-NP/PA is a registered trade-mark of Novellus Healthcare Communications, LLC. Nopart of this publicationmaybe reproduced or transmittedin any form or by any means now or hereafter known,electronic ormechanical, including photocopy, recording,or any informational storage and retrieval system, with-out written permission from the Publisher. Printed in theUnited States of America.
Directors, Client ServicesMark Timko
Russell [email protected]
Jack [email protected]
Editorial DirectorKristin Lee Siyahian
Copy EditorBjarne Hansen
Senior Production ManagerAlaina Pede
Business ManagerBlanche Marchitto
Executive AdministratorAndrea Boylston
Editorial ContactTelephone: 732-992-1891Fax: 732-656-7938
Novellus Healthcare Communications, LLC241 Forsgate Drive, Suite 205DMonroe Township, NJ 08831
4 Conference Highlights: Society of UrologicNurses and Associates
4 A Prescription for Everyday Ethics
5 Physical Therapy for Pelvic Floor Dysfunction
6 Benign Prostatic Hyperplasia: Evaluation;Treatment Options
11 A SUNA Debate: Should We Really be Using PSA?
13 Simple Intervention Boosts SpermCryopreservation in Men With Cancer
14 Anejaculation Common After Radiotherapy forProstate Cancer

A Prescription forEveryday EthicsThe fine art of knowing, and doing, what mustbe done
Laughter is a common response to keynoteaddresses, but tears, far less so. This mightbe especially true given a topic such as“Ethics in Today’s Healthcare Environ-ment: Why Being Ethical Matters.” How-ever, Jack A. Gilbert, EdD, FACHE,quickly set the tone by asserting that ethicsare at the core of the human condition andthat “it’s not just about work, it’s about ourlives.” It’s about the courage it takes tospeak up, even in those small momentswhen something just does not seem quiteright. It’s about what happens in thosemoments when you choose to either saysomething or just quietly walk away.To put the issue in perspective, Gilbert
related the history of the healthcare giantJohnson & Johnson (J&J), a highly suc-cessful business that began life with, at itscore, a hierarchical code of ethics: Thewelfare of customer comes first; profits ofshareholders last. With this credo as theorganizing principle, J&J has thrived forover 100 years. That is, until recently. J&Jhas experienced a series of setbacks, thelast one occurring this past September,when the recall of the analgesic Motrinprompted a congressional investigation.“Just because you have something in place[the credo] it doesn’t mean that is still haslife. It has to be regenerated.” What J&J
fell victim to, said Gilbert, is what hetermed “ethical erosion,” which is inessence the acceptance of that which isjust a little bit wrong. Once a little wrongis accepted, a great big wrong may well bein your future.Consider the workaround: There is a
protocol in place, but there’s simply notime – you’re being commanded, driven bythe so-called “tyranny of the urgent,” butthe work must be done, so just this onceyou make an exception, and procedure isignored. “Well-meaning people in well-meaning organizations are susceptible toethical erosion,” said Gilbert. The problemis that it sets a precedent.
Illustrating this point is a recent study ofmedical errors: Imagine the shape of apyramid constructed from the bottom upby mishaps of escalating seriousness; sen-tinel events, being the lowest in number,are represented as the peak of the pyramid,with harmful events just below, and non-harmful events – being the most common,in which things went just a little bit wrong– serving as the pyramid’s base. Havingdrilled down to discover the root cause of
sentinel events, what the study found wasthat error started out small – at the base.Gilbert extended this conclusion by sug-gesting that the very ground on which thepyramid sits represents the event of theworkaround, the moment where nothingactually went wrong, yet still managed tospark the genesis of a serious, life-threaten-ing lapse in procedure. Is the solution med-ical perfection? No. But on a day-to-daybasis it’s about where to draw the line.And it shouldn’t be comparative; it’s
about what is non-negotiable behavior forthe individual. “Common practice is notethical practice,” said Gilbert. “Just be-cause someone else does it doesn’t make itright.” Gilbert has actually heard compla-cency defended as being relative to theindustry as a whole. “I have an actual fearthat I will see a billboard someday and itwill say ‘We hurt fewer people than ourcompetition.’ ”
Ethical Wisdom“If ethical erosion is subtle, I suggest
something equally subtle to oppose it –ethical wisdom.” By this Gilbert means theinnate awareness of right and wrong.Though indeed subtle, and perhaps vague,these gut feelings have generated real data.Recall the 100,000 Lives Campaign spon-sored by the Institute for HealthcareImprovement, a national effort to reducepreventable deaths. Reporting to rapid re-sponse teams, nurses, and even family mem-bers of patients, were encouraged to speakup when they felt something was wrong
4 � November 2010
CONFERENCE HIGHLIGHTS: SUNA 2010
Conference Highlights: Society ofUrologic Nurses and Associates (SUNA)October 8-11, 2010, Boston, MA
IntroductionMeeting for the 41st annual conference, over 400 SUNA members gathered to hear the latest data regard-ing medication, and to review, and in some cases train in, advanced techniques for the diagnosis and man-agement of urologic dysfunctions. Reviewed in this Urology Nurse – NP/NA newsletter are four presenta-tions representing a range of interests, from the ethics of every day nursing decisions to physical therapyto improve symptoms of incontinence to the effective management of benign prostate hyperplasia. Alsoincluded are highlights from a SUNA debate regarding the medical utility of widespread PSA screening.
It’s about the courage ittakes to speak up, evenin those small momentswhen something justdoesn’t seem quite right.

with the patient, or patient care, even ifthe concern could not be readily identi-fied. Eighteen months after the program’sinitiation, an estimated 122,000 lives weresaved in the 3100 participating hospitals.Gilbert credits this accomplishment to thenurse’s innate sense of what is the rightthing to do.The sense exists for wrong action, as
well as inaction. Yet, in everyday life, com-municating this sense is problematic.“Even the simplest conversation can bedifficult to have,” said Gilbert. If you’re ina meeting and you’re uncomfortable withwhat’s being said… Do you stick your neckout? Do you risk censure, or possibly afriendship? You might even doubt thatinner sense, thinking, Well, what do I real-ly know? “It’s not easy,” Gilbert acknowl-edged, “it’s about trusting yourself.”It’s also about having faith in a collec-
tive wisdom. “I’m not saying everyone hasit in equal measure, but there’s enough togo around.” Talk to your peers. What yousense, what you feel, someone else is feel-ing. Where this leads critically dependson what Gilbert describes as the existingethical culture experienced in the work-place, and here is where the topic be-comes concrete.
The Action Items of Ethical CultureThese five qualities create and sustain thebody of ethical culture:
MindfulnessAcknowledge your gut feelings. Remainaware.
VoiceIf you see something, say something. Doesthis carry risks? Certainly. Yet, it calls intoquestion the very reasons why someoneenters the healthcare profession: to be ofservice; to help those who can’t help them-selves; to put the needs of the patient first.
RespectStriving to understand others rather thanfighting to be understood. Truly, deeply, lis-tening to the ideas of others will oftenreveal two things: 1) There is more thanone way to skin a cat, and 2) You haveallies you never dreamed of.
TenacityStick to your guns. This is not as dreary asit sounds. When you spend your day doingwhat you value, the personal rewards areclear – it’s energizing.
LegacyMeaning, work toward an ethical bequest,a lasting institutional integrity, in whatev-er small way you can.
To this final point Dr Gilbert used theexample of one of the grandest cathedralsin the world, Notre Dame, Paris. Con-struction of this extraordinary building,using architectural methods without prece-dent, began in 1160 and was completed in1345. No one who conceived of the struc-ture, and only a very few who participatedin its creation ever saw the completedcathedral, yet, day by day, in individualsmall measures, artisans came to work anddid their part.
“In working toward this ethical culture,we may not finish, we may not see thegrand ending, but we will pass it on,” saidGilbert. “The small moments in which wechose to say something or not, those arethe moments in which cathedrals arebuilt.”�
Physical Therapy forPelvic Floor DysfunctionYour patients want a return of function; PTswant to see your patients
“Physical therapy (PT) is not just aboutdoing Kegels.” So began Laurie Knox, PT,York Hospital, York, ME. In fact, PT foryour patients with pelvic floor (PF) dys-function may involve a range of muscletraining techniques from Kegels, certainly,to electrical stimulation, biofeedback, theuse of weights or, in some cases, a simplechange in behavior. To choose among themone must first recognize the highly specificneeds of the individual before designing atreatment plan.Briefly, the PF consists of the urogenital
triangle (first, second, and third layer); theanal triangle; bony boundaries; and thepelvic diaphragm. The overall function ofthe PF is the support of organs: the sphinc-
Novellus Healthcare Communications � 5
CONFERENCE HIGHLIGHTS: SUNA 2010
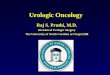
Figure 1. Ethical Erosion and Ethical Wisdom Will Impact the Health ofEthical Pathways
© New Page Consulting, Inc. All rights reserved.
Intentions:Vision, Mission, Values, Strategy, Goals
EthicalErosion
EthicalWisdom
Performance:Safety, Quality of Care, Financial Health,
Satisfaction, Retention, Reputation
Ethical Pathways
“In working toward thisethical culture, we maynot finish, we may not seethe grand ending, but wewill pass it on.”

teric closing off of all openings (the focusof this discussion), and sexual function(dysfunction of which may cause painfulintercourse, not discussed here).And then, there are muscles; “Muscles
are muscles no matter where they are inthe body, and there are a lot of them in thepelvic floor.” The pelvic diaphragm con-sists of two paired muscles, the levator ani,and the coccygeus, which close the inferi-or outlet of the pelvis, while both support-ing the PF and elevating it to help releasefeces. Other muscles include the piriformismuscle and the obturator internus. “Thesetwo are very important from the PT per-spective,” said Knox, “because these mus-cles are very tight in a lot of people but arecritical to normal function.”PF dysfunctions include: urinary incon-
tinence (stress, urge, mixed); fecal inconti-nence; overactive bladder; pelvic organprolapse; pelvic pain; and sexual dysfunc-tion. “Nearly all patients walk through thedoor with the chief complaint of loss offunction,” said Knox. “Very few say, ‘MsKnox, I have a dysfunction of my pelvicfloor’. It’s the functional component that’simportant to the patient.”
Getting to Know YouThey don’t call them “physical terrorists”for nothing, so it’s important that you tellyour patients that at the initial PT evalua-tion, internal examination of the PF is com-mon practice. “People are shocked whenthey come to PT and we tell them they aregoing to undergo an internal digital exam.”The full evaluation will involve taking a
history (which may reveal a problem unre-lated to the PF), a musculoskeletal exam(including body posture and gait, whichdemonstrate how the body is being used),connective tissue exam (surgical scars mayrestrict movement of the PF), and (take adeep breath) a PF exam. Also performed is
a rectal exam to assess contractile strengthand coccygeal mobility.After evaluation comes the treatment
plan. To illustrate the potential of PT inthis setting, the example of stress inconti-nence was chosen. “There are four possibleapproaches here,” explained Knox.1) Body awareness. The patients are
encouraged to consciously contract the PFduring activities that induce localized pres-sure, eg, contracting the PF before they lifta box, and holding that tension for theduration of the lift.2) Strength training. Kegels. The patients
are taught to perform regular strength train-ing over time. Diligence is required; resultswill take weeks.3) Indirect Training. The PF can be
trained indirectly by contraction of theinternal abdominal muscles, especially thetransverses. In a sense, this is training thePF through the back door.4) Functional training. Patients are
asked to contract their PF during differentactivities; walking, yard work, house work,and the like.
Critical to three of these approaches isthe ability to isolate and activate the PFmuscles. A study from 1991 estimated that30% of patients were unable to contracttheir PF on the first visit. This strongly sug-gests the need for, if not requires, repeatedfollow-up. Should the patient have thisinitial difficulty, several options are avail-able, including direct electrical stimulationand biofeedback.“E-stim is not very pleasant,” warned
Knox, “but if you hit the motor point unit,the pelvic floor will contract. It’s very effec-tive in helping patients find their way.”And e-stim devices can be used in thehome. On the other hand, biofeedback,generally office-based, is popular withpatients, aids in locating the PF, and can beextremely useful in situations where thepatient needs to learn to relax.
Where the Boys AreData indicate that urinary incontinence iscommon after prostatectomy. Though theclinical evidence for PT in this setting isnot robust, the rationale for its use is thatPF contraction increases the strength of the
external urethral sphincter resulting in hy-pertrophy of the striatum muscle, therebyincreasing mechanical pressure on the ure-thra. “The issue is not if it works, butwhether PTs ever get to see these guys,” saidKnox. Another issue is when these menshould be seen. “By the time they’ve hadtheir surgery, and then they’re incontinent,and then you send themdown, these guys aredevastated. The last thing they want is tocome and see me so that I can teach themhow to do a pelvic floor muscle contraction.”
Knox strongly advocates sending pros-tatectomy candidates to PT before theprocedure. “It’s much easier to teach themwhile they’re functional.” If they contin-ue to exercise preoperatively, they will bein much better shape postoperatively. Atthis point a question was raised aboutwhether preoperative conditioning wouldbe covered by insurance. Knox did notspecifically know but suspected that itwould be, given that cancer benefits aremore generous compared with other dis-ease states. “What I can tell you is that it’sworthwhile. Males who are incontinentpostoperatively are extremely compliantwith PF training.”�
Benign ProstaticHyperplasia: Evaluation;Treatment OptionsA review of current trends in the managementof BPH
The population is aging. There are current-ly 37millionmen older than 50 years in theUnited States, and an estimated 50% ofthese individuals have histologic, benignprostate hyperplasia (BPH). A detailedunderstanding of the condition – diagnosis,progression, and treatment options – will be
6 � November 2010
CONFERENCE HIGHLIGHTS: SUNA 2010
“People are shocked whenthey come to PT and wetell them they are goingto undergo an internaldigital exam.”
“The last thing they wantis to come and see meso that I can teach themhow to do a pelvic floormuscle contraction.”

critical to effectively manage a rapidly ex-panding patient population.Key to this understanding is that BPH
is progressive. “By the age of 70 years,80%-90% of all men will have developedBPH,” said Dr Bhalchandra Parulkar,assistant professor of urology, University ofMassachusetts Medical School, Worcester.That doesn’t mean this same segment of thepopulation all have an enlarged prostate, or,for that matter, a noticeable urinary ob-struction. “If you take a needle biopsy andlook at the pathology slide you will see BPH– the term is used as a synonym for havingan enlarged prostate, but that’s not reallytrue. BPH is a histological diagnosis.”Those who have histological BPH do
not always have an enlarged prostate; thisis an important distinction when consider-ing a diagnosis or potential treatmentoptions. When a physician or nurse per-forms a digital rectal examination (DRE),that person is feeling the outside of theprostate; however, the symptoms of BPHare produced from within. “For some indi-viduals the capsule enclosing the prostateis tight. When the prostate starts growingthe capsule prevents it from expanding,therefore, it grows inwards.” This producesthe same symptoms as those seen with anenlarged prostate, but without the physicalsize. In general, this discussion is framed bythe consideration of an enlarged prostate,defined as a prostate of ≥30 mL in volume.At 30 mL and above, prostate size slow-
ly starts making greater demands of thebladder, eventually resulting in hypertro-phy of the muscles. The muscles then con-tract more frequently, thereby creating thecombined problems of a weak urine stream,because of a blocked urethra, and irritativesymptoms such as frequency, urgency, andurge incontinence. “Hesitancy is a classicand common symptom of enlarged pros-tate, however, storage symptoms are themost bothersome,” said Parulkar. Most mendon’t mind taking some extra time to estab-lish a urine stream, but frequency, urgency,or nocturia can have a significant impacton quality of life.
Putting Your Finger on the Problem“If the diagnosis of BPH was simple, everyprimary care MD would treat it. But there
are many other conditions that mimic pros-tate symptoms.” These include prostate can-cer, bladder cancer, prostatitis, urinarytract infections, renal dysfunction, dia-betes, urethral narrowing, and interstitialcystitis. All these possibilities must beruled out, but first, when the patient pre-sents, there must be a consideration of risk.“On a patient’s first visit I consider thesefactors for BPH progression: age over 50,prostate exceeding 30 mL in volume, PSA≥1.4 ng/mL, an AUA-SI score over 7, andweak urinary flow.”
Diagnostic workup will include a DRE,labs for creatinine, urinary analysis for in-fection, and PSA. Further tests may in-clude a urine flow study, postvoid residuevia ultrasound, and, if needed, urodynam-ics and cystoscopy. A voiding diary mayalso be requested to establish functionalbladder capacity, as well to inform in caseswhere the chief complaint is nocturia.Finally, the patient is asked to completethe international prostate symptom scoreto establish the severity of the given com-plaint; scores range from mild to severe.Consider a patient who is young (55
years) who has presented with amild urolog-
ic complaint but has a 30-gram prostate.“You can bet that with time that prostate isgoing to grow and cause more problems,”said Parulkar. This is particularly true if thereis an older close relative with BPH. He sug-gested that a good urologic physician ornurse would anticipate worsening symptomsand recommend preventive treatment.What if you chose a less aggressive ap-
proach? Remember, BPH is progressive.Data indicate that men older than 60 yearswith enlarged prostates and obstructivesymptoms have a 39% lifetime risk ofrequiring surgery. Further, if left untreated,1 in 6 patients with an enlarged prostate,urologic symptoms, and a PSA ≥1.4 experi-ence acute urinary retention or BPH-relat-ed surgery within 4 years of diagnosis. “Youmust get a baseline PSA,” advised Parulkar.“It’s a good predictor of BPH progression.”The higher the PSA, the faster the growth.And keep a sharp eye out – once a prostateprogresses beyond 60 grams, most of thesimple treatments options are off the table.But it is worth noting that the prostatedoesn’t grow quickly on a yearly basis.
Treatment OptionsAlpha-blockersAlpha receptors are present on the prostateand related blood vessels; receptor antago-nism results in loss of local muscle tone. “Iftone is lost, the urethra expands, the blad-der neck expands, and this creates a widerpassage for the urine to flow. Alpha-block-ers do not reduce the prostate size but effec-tively achieve symptom relief – “and that’swhat the patient came to you for,” said
Novellus Healthcare Communications � 7
CONFERENCE HIGHLIGHTS: SUNA 2010
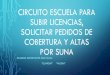
Figure 2. Natural History of BPH
And keep a sharp eye out –once a prostate progressesbeyond 60 grams, mostof the simple treatmentsoptions are off the table.
Increased DetrusorPressure
Increased UrethralResistance
Hyperplasia
Decreased BladderStorage
LUTSUrg./Freq./Nocturia

Rapid BPH symptom relief starts in 3 to 4 days1,2
• A majority of patients achieved at least a 3-point improvement in IPSS† total score3
• Significant improvements in total IPSS at all time points studied (P<0.0001)1,2
*RAPAFLO® is indicated for the treatment of the signs and symptoms of benign prostatic hyperplasia (BPH). RAPAFLO® is not indicated for the treatment of hypertension.
† International Prostate Symptom Score
References: 1. RAPAFLO® (silodosin) Capsules full Prescribing Information. 2. Marks LS, Gittelman MC, Hill LA, et al. Rapid effi cacy of the highly selective α1A-adrenoceptor antagonist silodosin in men with signs and symptoms of benign prostatic hyperplasia: pooled results of 2 phase 3 studies. J Urol. 2009;181:2634-2640. 3. Data on file, Watson Laboratories, Inc. 4. Marks LS, Gittelman MC, Hill LA, et al. Silodosin in the treatment of the signs and symptoms of benign prostatic hyperplasia: a 9-month open-label extension study. Urology. 2009;74:1318-1322. 5. Marks LS. Reply to editorial comment. Urology. 2009;74:1323-1324.Models are for illustrative purposes only.
© 2010, Watson Pharma, Inc., Morristown, NJ 07960. All rights reserved. 06317 1/10
THAT KEEPS HIM GOING
IN THE TREATMENT OF SYMPTOMATIC BPH*
RAPID RELIEF

Important Safety Information
RAPAFLO® is contraindicated in patients with severe renal impairment (CCr <30 mL/min), severe hepatic impairment (Child-Pugh score ≥10), and with use of strong CYP3A4 inhibitors.
Postural hypotension with or without symptoms (eg, dizziness) may develop when beginning treatment with RAPAFLO®.As with all alpha-blockers, there is a potential for syncope. Patients should be warned of the possible occurrences of such events and should avoid situations where injury could result. RAPAFLO® should be used with caution in patients with moder-ate renal impairment. Patients should be assessed to rule out the presence of prostate cancer prior to starting treatment with RAPAFLO®. Patients planning cataract surgery should inform their ophthalmologist that they are taking RAPAFLO®.
The most common side effects are retrograde ejaculation, dizziness, diarrhea, orthostatic hypotension, headache, nasopharyngitis, and nasal congestion.
Please see brief summary of full Prescribing Information on adjacent page.
For more information, please visit www.rapafl o.com
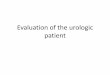
Sustained relief for up to 1 year • Significant improvement in total IPSS and irritative
and obstructive IPSS subscores3,4
– Patients continuing RAPAFLO® therapy experienced additional improvements in IPSS scores over the 9-month uncontrolled, open-label period3,4
– Patients continuing RAPAFLO® therapy experienced an ~9-point overall reduction in IPSS total score over 52 weeks5
Convenient dosing regimen• One 8-mg capsule taken
once daily with a meal1RAPAFLO® 8 mg
#30 SIG: 1 CAPPO DAILY
WITH A MEAL
Changes in IPSS Over 52 Weeks5‡
-10.0
-8.0
-6.0
-4.0
-2.0
Mea
nC
han
gein
IPS
Sfr
om
Bas
elin
eto
Wee
k52
21
12
Baseline
Continuing RAPAFLO®
‡Patients received RAPAFLO® for 12 weeks in the double-blind controlled trials and for 40 weeks in the uncontrolled, open-label phase.
n=206
Changes in IPSS Over 52 Weeks5‡
-10.0
-8.0
-6.0
-4.0
-2.0
Mea
n C
han
ge in
IPS
S f
rom
B
asel
ine
to W
eek
52
21
12
Baseline
Continuing RAPAFLO®
‡Patients received RAPAFLO® for 12 weeks in the double-blind controlled trials and for 40 weeks in the uncontrolled, open-label phase.
n=206

BRIEF SUMMARYFor full Prescribing Information, see package insert.INDICATIONS AND USAGERAPAFLO, a selective alpha-1 adrenergic receptor antagonist, is indicated for the treatment of the signs and symptoms of benign prostatic hyperplasia (BPH). RAPAFLO is not indicated for the treatment of hypertension.CONTRAINDICATIONS
Severe renal impairment (CCr < 30 mL/min)Severe hepatic impairment (Child-Pugh score ≥ 10)Concomitant administration with strong Cytochrome P450 3A4 (CYP3A4) inhibitors (e.g., ketoconazole, clarithro-mycin, itraconazole, ritonavir) [see Drug Interactions]
WARNINGS AND PRECAUTIONSOrthostatic EffectsPostural hypotension, with or without symptoms (e.g., dizziness) may develop when beginning RAPAFLO treatment. As with other alpha-blockers, there is potential for syncope. Patients should be cautioned about driving, operating machin-ery, or performing hazardous tasks when initiating therapy [see Adverse Reactions and Use in Specific Populations].Renal ImpairmentIn a clinical pharmacology study, plasma concentrations (AUC and Cmax) of silodosin were approximately three times higher in subjects with moderate renal impairment compared with subjects with normal renal function, while half-lives of silodosin doubled in duration. The dose of RAPAFLO should be reduced to 4 mg in patients with moderate renal impairment. Exercise caution and monitor such patients for adverse events [see Use in Specific Populations].RAPAFLO is contraindicated in patients with severe renal impairment [see Contraindications].Hepatic ImpairmentRAPAFLO has not been tested in patients with severe hepatic impairment, and therefore, should not be prescribed to such patients [see Contraindications and Use in Specific Populations].Pharmacokinetic Drug-Drug InteractionsIn a drug interaction study, co-administration of a single 8 mg dose of RAPAFLO with 400 mg ketoconazole, a strong CYP3A4 inhibitor, caused a 3.8-fold increase in maximum plasma silodosin concentrations and 3.2-fold increase in silodosin exposure (i.e., AUC). Concomitant use of ketoconazole or other strong CYP3A4 inhibitors (e.g., itraconazole, clarithromycin, ritonavir) is therefore contraindicated [see Drug Interactions].Pharmacodynamic Drug-Drug InteractionsThe pharmacodynamic interactions between silodosin and other alpha-blockers have not been determined. However, interactions may be expected, and RAPAFLO should not be used in combination with other alpha-blockers [see DrugInteractions].A specific pharmacodynamic interaction study between silodosin and antihypertensive agents has not been performed. However, patients in the Phase 3 clinical studies taking concomitant antihypertensive medications with RAPAFLO did not experience a significant increase in the incidence of syncope, dizziness, or orthostasis. Nevertheless, exercise caution during concomitant use with antihypertensives and monitor patients for possible adverse events [see AdverseReactions and Drug Interactions].Caution is also advised when alpha-adrenergic blocking agents including RAPAFLO are co-administered with PDE5 inhibitors. Alpha-adrenergic blockers and PDE5 inhibitors are both vasodilators that can lower blood pressure. Con-comitant use of these two drug classes can potentially cause symptomatic hypotension [see Drug Interactions].Carcinoma of the ProstateCarcinoma of the prostate and BPH cause many of the same symptoms. These two diseases frequently co-exist. There-fore, patients thought to have BPH should be examined prior to starting therapy with RAPAFLO to rule out the presence of carcinoma of the prostate.Intraoperative Floppy Iris SyndromeIntraoperative Floppy Iris Syndrome has been observed during cataract surgery in some patients on alpha-1 blockers or previously treated with alpha-1 blockers. This variant of small pupil syndrome is characterized by the combination of a flaccid iris that billows in response to intraoperative irrigation currents; progressive intraoperative miosis despite preoperative dilation with standard mydriatic drugs; and potential prolapse of the iris toward the phacoemulsifica-tion incisions. Patients planning cataract surgery should be told to inform their ophthalmologist that they are taking RAPAFLO [see Adverse Reactions].Laboratory Test InteractionsNo laboratory test interactions were observed during clinical evaluations. Treatment with RAPAFLO for up to 52 weeks had no significant effect on prostate-specific antigen (PSA). ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.In U.S. clinical trials, 897 patients with BPH were exposed to 8 mg RAPAFLO daily. This includes 486 patients exposed for 6 months and 168 patients exposed for 1 year. The population was 44 to 87 years of age, and predominantly Cauca-sian. Of these patients, 42.8% were 65 years of age or older and 10.7% were 75 years of age or older. In double-blind, placebo controlled, 12-week clinical trials, 466 patients were administered RAPAFLO and 457 patients were administered placebo. At least one treatment-emergent adverse reaction was reported by 55.2% of RAPAFLO treated patients (36.8% for placebo treated). The majority (72.1%) of adverse reactions for the RAPAFLO treated patients (59.8% for placebo treated) were qualified by the investigator as mild. A total of 6.4% of RAPAFLO treated patients (2.2% for placebo treated) discontinued therapy due to an adverse reaction (treatment-emergent), the most commonreaction being retrograde ejaculation (2.8%) for RAPAFLO treated patients. Retrograde ejaculation is reversible upon discontinuation of treatment.Adverse Reactions observed in at least 2% of patients:The incidence of treatment-emergent adverse reactions listed in the following table were derived from two 12-week, mul-ticenter, double-blind, placebo-controlled clinical studies of RAPAFLO 8 mg daily in BPH patients. Adverse reactions that occurred in at least 2% of patients treated with RAPAFLO and more frequently than with placebo are shown in Table 1. Table 1 Adverse Reactions Occurring in ≥ 2% of Patients in 12-week, Placebo-Controlled Clinical Trials
In the two 12-week, placebo-controlled clinical trials, the following adverse events were reported by between 1% and2% of patients receiving RAPAFLO and occurred more frequently than with placebo: insomnia, PSA increased, sinusitis, abdominal pain, asthenia, and rhinorrhea. One case of syncope in a patient taking prazosin concomitantly and one caseof priapism were reported in the RAPAFLO treatment group.In a 9-month open-label safety study of RAPAFLO, one case of Intraoperative Floppy Iris Syndrome (IFIS) was reported.Postmarketing ExperienceThe following adverse reactions have been identified during post approval use of silodosin. Because these reactions arereported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency orestablish a causal relationship to drug exposure:Skin and subcutaneous tissue disorders: toxic skin eruption, purpuraHepatobiliary disorders: jaundice, impaired hepatic function associated with increased transaminase values
DRUG INTERACTIONSModerate and Strong CYP3A4 InhibitorsIn a clinical metabolic inhibition study, a 3.8-fold increase in silodosin maximum plasma concentrations and 3.2-fold increase in silodosin exposure were observed with concurrent administration of a strong CYP3A4 inhibitor, 400 mg ketoconazole. Use of strong CYP3A4 inhibitors such as itraconazole or ritonavir may cause plasma concentrations of silodosin to increase. Concomitant administration of strong CYP3A4 inhibitors and RAPAFLO is contraindicated [seeContraindications and Warnings and Precautions].The effect of moderate CYP3A4 inhibitors on the pharmacokinetics of silodosin has not been evaluated. Concomitant administration with moderate CYP3A4 inhibitors (e.g., diltiazem, erythromycin, verapamil) may increase concentration of RAPAFLO. Exercise caution and monitor patients for adverse events when co-administering RAPAFLO with moderate CYP3A4 inhibitors.Strong P-glycoprotein (P-gp) InhibitorsIn vitro studies indicated that silodosin is a P-gp substrate. Ketoconazole, a CYP3A4 inhibitor that also inhibits P-gp, caused significant increase in exposure to silodosin. Inhibition of P-gp may lead to increased silodosin concentration. RAPAFLO is therefore not recommended in patients taking strong P-gp inhibitors such as cyclosporine.Alpha-BlockersThe pharmacodynamic interactions between silodosin and other alpha-blockers have not been determined. However, interactions may be expected, and RAPAFLO should not be used in combination with other alpha-blockers [see Warnings and Precautions].DigoxinThe effect of co-administration of RAPAFLO and digoxin 0.25 mg/day for 7 days was evaluated in a clinical trial in 16 healthy males, aged 18 to 45 years. Concomitant administration of RAPAFLO and digoxin did not significantly alter the steady state pharmacokinetics of digoxin. No dose adjustment is required.PDE5 InhibitorsCo-administration of RAPAFLO with a single dose of 100 mg sildenafil or 20 mg tadalafil was evaluated in a placebo-controlled clinical study that included 24 healthy male subjects, 45 to 78 years of age. Orthostatic vital signs were monitored in the 12-hour period following concomitant dosing. During this period, the total number of positive ortho- static test results was greater in the group receiving RAPAFLO plus a PDE5 inhibitor compared with RAPAFLO alone. No events of symptomatic orthostasis or dizziness were reported in subjects receiving RAPAFLO with a PDE5 inhibitor.Other Concomitant Drug TherapyAntihypertensivesThe pharmacodynamic interactions between silodosin and antihypertensives have not been rigorously investigated in a clinical study. However, approximately one-third of the patients in clinical studies used concomitant antihypertensive medications with RAPAFLO. The incidence of dizziness and orthostatic hypotension in these patients was higher than in the general silodosin population (4.6% versus 3.8% and 3.4% versus 3.2%, respectively). Exercise caution during con- comitant use with antihypertensives and monitor patients for possible adverse events [see Warnings and Precautions].Metabolic InteractionsIn vitro data indicate that silodosin does not have the potential to inhibit or induce cytochrome P450 enzyme systems. Food InteractionsThe effect of a moderate fat, moderate calorie meal on silodosin pharmacokinetics was variable and decreased silodosin maximum plasma concentration (Cmax) by approximately 18 - 43% and exposure (AUC) by 4 - 49% across three different studies. Safety and efficacy clinical trials for RAPAFLO were always conducted in the presence of food intake. Patients should be instructed to take silodosin with a meal to reduce risk of adverse events. USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category B. RAPAFLO is not indicated for use in women. An embryo/fetal study in rabbits showed decreased maternal body weight at 200 mg/kg/day (approximately 13-25 times the maximum recommended human exposure or MRHE of silodosin via AUC). No statistically significant teratogenicity was observed at this dose. Silodosin was not teratogenic when administered to pregnant rats during organogenesis at 1000 mg/kg/day (estimated to be approximately 20 times the MRHE). No maternal or fetal effects were observed at this dose. Rats and rabbits do not produce glucuronidated silodosin, which is present in human serum at approximately 4 times the level of circulating silodosin and which has similar pharmacological activity to silodosin. No effects on physical or behavioral development of offspring were observed when rats were treated during pregnancy and lactation at up to 300 mg/kg/day.Pediatric UseRAPAFLO is not indicated for use in pediatric patients. Safety and effectiveness in pediatric patients have not been established.Geriatric UseIn double-blind, placebo-controlled, 12-week clinical studies of RAPAFLO, 259 (55.6%) were under 65 years of age, 207 (44.4%) patients were 65 years of age and over, while 60 (12.9%) patients were 75 years of age and over. Orthostatic hypotension was reported in 2.3% of RAPAFLO patients < 65 years of age (1.2% for placebo), 2.9% of RAPAFLO patients ≥ 65 years of age (1.9% for placebo), and 5.0% of patients ≥ 75 years of age (0% for placebo). There were otherwise no significant differences in safety or effectiveness between older and younger patients.Renal ImpairmentThe effect of renal impairment on silodosin pharmacokinetics was evaluated in a single dose study of six male patients with moderate renal impairment and seven male subjects with normal renal function. Plasma concentrations of silo-dosin were approximately three times higher in subjects with moderate renal impairment compared with subjects with normal renal function. RAPAFLO should be reduced to 4 mg per day in patients with moderate renal impairment. Exercise caution and monitor patients for adverse events. RAPAFLO has not been studied in patients with severe renal impairment. RAPAFLO is contraindicated in patients with severe renal impairment [see Contraindications and Warnings and Precautions].Hepatic ImpairmentIn a study comparing nine male patients with moderate hepatic impairment (Child-Pugh scores 7 to 9), to nine healthy male subjects, the single dose pharmacokinetics of silodosin were not significantly altered in patients with hepatic impairment. No dosing adjustment is required in patients with mild or moderate hepatic impairment. RAPAFLO has not been studied in patients with severe hepatic impairment. RAPAFLO is contraindicated in patients with severe hepatic impairment [see Contraindications and Warnings and Precautions].OVERDOSAGERAPAFLO was evaluated at doses of up to 48 mg/day in healthy male subjects. The dose-limiting adverse event was postural hypotension.Should overdose of RAPAFLO lead to hypotension, support of the cardiovascular system is of first importance. Res-toration of blood pressure and normalization of heart rate may be accomplished by maintaining the patient in the supine position. If this measure is inadequate, administration of intravenous fluid should be considered. If necessary, vasopressors could be used, and renal function should be monitored and supported as needed. Dialysis is unlikely to be of significant benefit since silodosin is highly (97%) protein bound.
Adverse ReactionsRAPAFLON = 466n (%)
PlaceboN = 457n (%)
Retrograde Ejaculation 131 (28.1) 4 (0.9)Dizziness 15 (3.2) 5 (1.1)Diarrhea 12 (2.6) 6 (1.3)Orthostatic Hypotension 12 (2.6) 7 (1.5)Headache 11 (2.4) 4 (0.9)Nasopharyngitis 11 (2.4) 10 (2.2)Nasal Congestion 10 (2.1) 1 (0.2)
Manufactured by: Watson Laboratories, Inc., Corona, CA 92880 USA Distributed by: Watson Pharma, Inc., Morristown, NJ 07962 USAUnder license from: Kissei Pharmaceutical Co., Ltd., Nagano, JapanAddress medical inquiries to: WATSON Medical Communications, P.O. Box 1953, Morristown, NJ 07962-1953 800-272-5525For additional information see: www.rapaflo.comor call 1-866-RAPAFLO (727-2356)Rx Only Revised: November 2009 173761-2 S1109

Novellus Healthcare Communications � 11
CONFERENCE HIGHLIGHTS: SUNA 2010
Parulkar, adding that patients are encour-aged by the rapid onset of action for thisclass of drugs and their relative inexpensivecost. However, as the prostate continues togrow, symptoms may eventually worsen. Thecombination of an alpha-blocker with a 5-alpha reductase inhibitor may be recom-mended for patients with very large prostates(well larger than 30 mL).
Saw PalmettoSometimes combined with zinc and seleni-um. This is an option if a patient has mildsymptoms but prefers not to use prescrip-tion medication. Some patients do experi-ence symptom relief, however, randomizedstudies indicate no benefit beyond theplacebo effect.
5-Alpha Reductase InhibitorsThe rationale for the use of these agents isto prevent the conversion of testosteroneto dihydrotestosterone (DHT), which isrequired for prostate growth. “These drugsdecrease DHT but do not eliminate testos-terone, so men don’t experience too manysignificant adverse reactions,” said Parulkar,“and the earlier you use them, the betterthey will work.” These agents will shrinkthe prostate, but as mentioned in the con-text of symptoms without enlargement, thistreatment will be ineffective. A furtherdownside: “These drugs take up to 6months to work. That can be a hard sell tothe uncomfortable patient.” There is alsothis caveat: If your patient is taking thesedrugs, future PSA values must be doubled.
Surgical OptionsStents.Typically used in nursing homes. Notfor use in younger patients.Needle Ablation Radiofrequency.A very pre-cise technique using an endoscope throughthe urethra that applies heat to the pros-tate and destroys and collapses target tis-
sue. Patients go home the same day with acatheter.Microwave Therapy. Similar to radiofre-quency in that it heats the tissue. Thismethod is rapid, and catheters are general-ly not required.Laser Vaporization. Also rapid, but notwidely available.TURP. The most invasive approach withthe greatest chance of complications, shortof open prostatectomy. TURP requireshospitalization and use of a general orspinal anesthetic. Recovery time, duringwhich strenuous activity must be avoided,lasts up to 6 weeks.Concluding his review, Dr Parulkar cau-
tioned listeners. “Keep in mind that withall these methods, the potential forprostate cancer still exists. The tissueyou’re targeting is internal, oncogenesisoccurs at the periphery.” Patients willrequire continued follow-up.�
A SUNA Debate: ShouldWe Really Be Using PSA?Recent data suggest that widespread screeningprograms are ineffective (maybe)
Everyone likes a good debate. However,if the loser in such an argument is thepatient, which side does one root for, thegood data, or the good intention? The datacome from two large, randomized trialsrecently published. The case for goodintentions – generated by the desire to dosomething to reduce the high rates of inci-dence for prostate cancer (PCa) – was pre-sented by Silvia Maxwell, ACNP-BC,CUNP, Detroit Medical Center, whoadvanced her argument by presenting thescope of the problem.“The National Cancer Institute esti-
mates that 217,730 new cases will be diag-nosed for 2010, eventually resulting in over32,000 deaths.” As most healthcare pro-viders know, the sooner a cancer is detect-ed the better the treatment outcome, “andright now, the PSA test is our primary toolin the early detection of these prostate can-cers.” And therein lies the debate: the twoaforementioned trials, the Prostate, Lung,Colorectal, and Ovarian Cancer Screening
Trial1 and the European Randomized Studyof Screening for Prostate Cancer2 investiga-tions, enrolling over 130,000 men com-bined, did not definitively show that PSAreally saves lives on the basis of widespreadscreening. “The problem,” said Maxwell,“is that, while PSA is specific for prostate,it is not specific for cancer.”
First identified as a prostate marker in1966, PSA was established as a tumormarker in 1979 and approved as a diagnos-tic test in 1994. After the introduction ofthe test there was a marked increase inPCa detection and a 30% decline in PCa-related deaths. However, one cannot saythat the test was directly responsible forthe percentage of the decline, as therewere concurrent advances in treatmentoptions. What was apparent was that forthat initiation period, PCa was overdiag-nosed. “This can be attributed to the factthat there is no universally accepted cutoffPSA threshold (generally held to bearound 4 ng/mL).”Further, an elevated PSA may not be
related to PCa. Increased PSA levels maybe indicative of infection or inflammation,urethral trauma, recent ejaculation, orDRE. Levels may be artificially depressedby the use of antibiotics, the use of finas-teride or dutasteride to treat BPH, or thepatient’s body mass index (BMI). For BMI≥35, PSA values are artificially low. Again,to be of relevance, the test needs to aid inthe identification of tumors in their earlystages. If the cancer remains localized, 5-year survival rates are near 100%; formetastatic disease, 5-year survival drops to32% for whites and 29% for African-Americans. “African-Americans have thehighest rates in the world,” said Maxwell.Other risk factors include age ≥65 years;family history; and, of epidemiologicalinterest, <12 years of formal education.
The rationale for the useof these agents is toprevent the conversionof testosterone todihydrotestosterone (DHT).
After the introduction ofthe test there was a markedincrease in PCa detectionand a 30% decline inPCa-related deaths.

12 � November 2010
CONFERENCE HIGHLIGHTS: SUNA 2010
So, yes, PCa is a serious healthcare issue,but is the information PSA is giving usworth all the biopsies? “I do believe thatover the years many men have beenovertreated,” Maxwell admitted, and thatmore discussion needs to be had with menabout what the score means. “A value of 2or 2.5 indicates a very slow-growing tumorof very little eventual risk.” This is partic-ularly true for the elderly.
Con: The Data Clearly Show Thatthe Import of PSA Is Not ClearSusanQuallich,ANP-BC,NP-C,CUNO,
Division of Sexual and ReproductiveMedi-cine, Department of Urology, University ofMichigan, was not quite as circumspect inher arguments. “There is no agreed con-sensus about how to assess a defined group,or way to treat people who have elevatedPSA.” Issues include: who should bescreened, how screening should be offered,how often, and how to advise patientsabout results. Its value as an all-comer, pop-ulation-based screen is unclear even to theexperts. Consider the guidelines: Ameri-can Urological Association – yes to screen-ing, but only for the well counseled; WorldHealth Organization – no to screeninguntil large randomized trials show benefit;European Association of Urology – no towidespread screening based on insufficientevidence of benefit.“It has been said that widespread screen-
ing for PSA has created a pseudo epidem-
ic,” asserted Quallich, adding that, “Wedon’t have really good evidence for bene-fit, but we have a lot of evidence for harm.”It has even lead one Harvard epidemio-logist to go on record saying that PSAscreening “…is a disaster of contempo-rary medicine.”3
The term “disaster” is relative, but thatPSA can have a negative impact is finite.Since its introduction, PSA has all but dou-bled the chance that an individual man willbe diagnosed with PCa – in 1980 it was 1 in11, today it is 1 in 6. This is largely an in-crease in local detection, not metastasis, notthe life-threatening cancers. “We see menwith elevated PSA but don’t really knowwhat to do with that information. Evenbefore biopsy, this information alone in-creases anxiety.” Studies have shown thatjust the idea that someone might have can-cer has a negative impact on health. Pa-tients may experience depression, anxiety,voiding problems, and bowel problems; andwith PCa treatment, which may or may nothave been necessary; erectile dysfunction;
bowel dysfunction, and incontinence. It’snoteworthy that 50% of men with an ele-vated PSA never have clinical symptoms.“Ultimately you can make the argumentwith PSA screening that we’re violating theidea that we do no harm.” And we haven’teven begun to discuss the cost.Finally, the minute a PSA threshold for
concern seems to be established, new dataprovide nothing but confusion. “One ofthe most interesting findings to come outin the last 8-12 months is that obesitycauses a PSA to be lower than it wouldactually be,” said Quallich. This is reallysignificant. We have all heard about theobesity epidemic – with widespread screen-ing, what are we to do with these numbers?A comment from the audience side-
stepped the debate regarding the wisdomof widespread screening to say that PSAvelocity, not merely a single measure, washighly informative for the individual. Thisidea framed the debate: value to the indi-vidual patient versus service to the popula-tion at large.�
References1. Andriole GL, Crawford ED, Grubb RL 3rd, et al.Mortality results from a randomized prostate-cancer screening trial. N Engl J Med. 2009;360:1310-1319.
2. Schröder FH, Hugosson J, Roobol MJ, et al.Screening and prostate-cancer mortality in arandomized European study. N Engl J Med.2009;360:1320-1328.
3. Adami HO. The prostate cancer pseudo-epi-demic. Acta Oncol. 2010;49:298-304.
Issues include: who shouldbe screened, how screeningshould be offered, howoften, and how to advisepatients about results.

Novellus Healthcare Communications � 13
NEWS FROM THE UROLOGY NURSE
An hour-long lecture by a fertility special-ist during oncology grand rounds dramat-ically improves the rate of pretreatmentsperm cryopreservation in young men withcancer, according to data presented at theAmerican Urological Association 2010Annual Scientific Meeting.The researchers found that educating
oncologists by a urologist specializing inmale infertility increased sperm cryopreser-vation in male cancer 4-fold. “Eventhough our study was observational, ourresults highlight the importance of educat-ing our colleagues in the oncology worldabout this resource,” Daniel H. WilliamsIV, MD, Assistant Professor of Urology andDirector of Male Reproductive MedicineandMicrosurgery, University of Wisconsin,Madison, said in an interview with TheOB/GYN and Infertility Nurse.DrWilliams’ team compared sperm cryo-
preservation rates before and after the lec-ture, which focused on the risks of cancertreatment–induced male infertility, ad-vances in assisted reproductive technology,and the local availability of sperm cryo-preservation.The dramatic increase in sperm cryo-
preservation seen 1 month after a singlelecture was maintained at follow-up sever-al months later.Because of therapeutic advances, pedi-
atric and adult cancer survivors are living“well into” their reproductive years, Dr
Williams pointed out. However, most can-cer treatment regimens have adverse ef-fects on testicular function and male repro-ductive potential, and posttreatmentfecundity is difficult to predict.
“Sperm cryopreservation provides anopportunity to preserve a man’s fertilitybefore cancer treatment,” DrWilliams said.The American Society of Clinical On-cology has recommended that oncologistsroutinely discuss the potential for infertilityalong with fertility preservation optionswith patients before cancer therapy andrefer interested patients to reproductivespecialists. In addition, the guidelines rec-ommend that semen cryopreservation beadopted as standard practice.In contrast, epidemiologic studies indi-
cate that most young male cancer patientsare not advised to bank sperm before their
cancer treatment. Surveys have consis-tently identified a lack of information asthe main reason for the low sperm cryo-preservation rate.About 40 healthcare practitioners at-
tended the lecture. Attendees were mostlypediatric and adult oncologists but alsoincluded oncology nurses and other staff.In the 24-month period before the lec-
ture, only 1 patient with cancer per monthbanked his sperm. After the lecture, therate increased significantly, to 3.7 patientswith cancer per month over the subsequent7 months (P<.001).Most of the change was comprised of a
nearly 6-fold increase in the number ofpatients with nontesticular cancer, from0.42 to 2.42 per month (P<.001).“With improvements in cancer thera-
pies, young men of reproductive age whodevelop cancers – lymphomas, leukemias,and testicular malignancies, among others– are surviving longer,” Dr Williams said.“As a result, cancer treatments now focusnot only on survival but on quality of life,and fertility and fertility potential is a largecomponent of quality of life after cancertreatment.”Continued efforts should be made to
educate healthcare professionals aboutsperm cryopreservation, with an emphasison improving the comprehensive cancercare and posttreatment quality of life inthese patients, he added.�
Simple Intervention Boosts SpermCryopreservation in Men With CancerBY JILL STEIN
“Cancer treatments nowfocus not only on survivalbut on quality of life,and fertility and fertilitypotential is a largecomponent of quality of lifeafter cancer treatment.”—Daniel H. Williams IV, MD

14 � November 2010
NEWS FROM THE UROLOGY NURSE
Most men who undergo radiation therapy(RT) for prostate cancer will develop an-ejaculation over time, according to DoronStember, MD, a urology fellow at Me-morial Sloan-Kettering Cancer Center inNew York City, who presented at theAmerican Urological Association 2010annual meeting the results of a study thatexamined the ejaculation profiles of 364men who underwent localized RT forprostate cancer.“It is widely known that anejaculation
occurs after a radical prostatectomy andmay be a significant cause of bother andsexual dissatisfaction,” Dr Stember said.“In contrast, patients and physicians donot commonly associate radiation therapy
with anejaculation. We undertook thisstudy because our clinical experience hassuggested that many men do, in fact, loseantegrade ejaculatory function after RT.”The overwhelming majority of prior
analyses of patients with pelvic RT-associ-ated sexual dysfunction have focused onerectile dysfunction, often without men-tion of changes in ejaculatory dysfunction.Anejaculation is thought to result from aprogressive scarring mechanism in theprostate tissue (including the ejaculatoryducts) that leads to obstruction of theejaculate.Overall, 16% of the men in this study
complained of anejaculation at 1 year, 69%at 3 years, and 89% at 5 years. “There was
a clear trend toward an increasing propor-tion of patients experiencing anejacula-tion…after RT,” he said. The risk factorsfor failure to ejaculate at 3 years included:• High RT doses• Older age• A history of androgen deprivationtherapy• Smaller prostates at the time of RT.
Orgasm domain scores on the widelyvalidated International Index of ErectileFunction questionnaire decreased marked-ly throughout follow-up. “We recommendthat the high likelihood of inability toejaculate should be discussed with menprior to RT,” Dr Stember advised.�
Anejaculation Common After Radiotherapyfor Prostate CancerBY JESSICA A. SMITH
NOV0310

BRIEF SUMMARYFor full Prescribing Information, see package insert.INDICATIONS AND USAGERAPAFLO, a selective alpha-1 adrenergic receptor antagonist, is indicated for the treatment of the signs and symptoms of benign prostatic hyperplasia (BPH). RAPAFLO is not indicated for the treatment of hypertension.CONTRAINDICATIONS
Severe renal impairment (CCr < 30 mL/min)Severe hepatic impairment (Child-Pugh score ≥ 10)Concomitant administration with strong Cytochrome P450 3A4 (CYP3A4) inhibitors (e.g., ketoconazole, clarithro-mycin, itraconazole, ritonavir) [see Drug Interactions]
WARNINGS AND PRECAUTIONSOrthostatic EffectsPostural hypotension, with or without symptoms (e.g., dizziness) may develop when beginning RAPAFLO treatment. As with other alpha-blockers, there is potential for syncope. Patients should be cautioned about driving, operating machin-ery, or performing hazardous tasks when initiating therapy [see Adverse Reactions and Use in Specific Populations].Renal ImpairmentIn a clinical pharmacology study, plasma concentrations (AUC and Cmax) of silodosin were approximately three times higher in subjects with moderate renal impairment compared with subjects with normal renal function, while half-lives of silodosin doubled in duration. The dose of RAPAFLO should be reduced to 4 mg in patients with moderate renal impairment. Exercise caution and monitor such patients for adverse events [see Use in Specific Populations].RAPAFLO is contraindicated in patients with severe renal impairment [see Contraindications].Hepatic ImpairmentRAPAFLO has not been tested in patients with severe hepatic impairment, and therefore, should not be prescribed to such patients [see Contraindications and Use in Specific Populations].Pharmacokinetic Drug-Drug InteractionsIn a drug interaction study, co-administration of a single 8 mg dose of RAPAFLO with 400 mg ketoconazole, a strong CYP3A4 inhibitor, caused a 3.8-fold increase in maximum plasma silodosin concentrations and 3.2-fold increase in silodosin exposure (i.e., AUC). Concomitant use of ketoconazole or other strong CYP3A4 inhibitors (e.g., itraconazole, clarithromycin, ritonavir) is therefore contraindicated [see Drug Interactions].Pharmacodynamic Drug-Drug InteractionsThe pharmacodynamic interactions between silodosin and other alpha-blockers have not been determined. However, interactions may be expected, and RAPAFLO should not be used in combination with other alpha-blockers [see DrugInteractions].A specific pharmacodynamic interaction study between silodosin and antihypertensive agents has not been performed. However, patients in the Phase 3 clinical studies taking concomitant antihypertensive medications with RAPAFLO did not experience a significant increase in the incidence of syncope, dizziness, or orthostasis. Nevertheless, exercise caution during concomitant use with antihypertensives and monitor patients for possible adverse events [see Adverse Reactions and Drug Interactions].Caution is also advised when alpha-adrenergic blocking agents including RAPAFLO are co-administered with PDE5 inhibitors. Alpha-adrenergic blockers and PDE5 inhibitors are both vasodilators that can lower blood pressure. Con-comitant use of these two drug classes can potentially cause symptomatic hypotension [see Drug Interactions].Carcinoma of the ProstateCarcinoma of the prostate and BPH cause many of the same symptoms. These two diseases frequently co-exist. There-fore, patients thought to have BPH should be examined prior to starting therapy with RAPAFLO to rule out the presence of carcinoma of the prostate.Intraoperative Floppy Iris SyndromeIntraoperative Floppy Iris Syndrome has been observed during cataract surgery in some patients on alpha-1 blockers or previously treated with alpha-1 blockers. This variant of small pupil syndrome is characterized by the combination of a flaccid iris that billows in response to intraoperative irrigation currents; progressive intraoperative miosis despite preoperative dilation with standard mydriatic drugs; and potential prolapse of the iris toward the phacoemulsifica-tion incisions. Patients planning cataract surgery should be told to inform their ophthalmologist that they are taking RAPAFLO [see Adverse Reactions].Laboratory Test InteractionsNo laboratory test interactions were observed during clinical evaluations. Treatment with RAPAFLO for up to 52 weeks had no significant effect on prostate-specific antigen (PSA).ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.In U.S. clinical trials, 897 patients with BPH were exposed to 8 mg RAPAFLO daily. This includes 486 patients exposed for 6 months and 168 patients exposed for 1 year. The population was 44 to 87 years of age, and predominantly Cauca-sian. Of these patients, 42.8% were 65 years of age or older and 10.7% were 75 years of age or older. In double-blind, placebo controlled, 12-week clinical trials, 466 patients were administered RAPAFLO and 457 patients were administered placebo. At least one treatment-emergent adverse reaction was reported by 55.2% of RAPAFLO treated patients (36.8% for placebo treated). The majority (72.1%) of adverse reactions for the RAPAFLO treated patients (59.8% for placebo treated) were qualified by the investigator as mild. A total of 6.4% of RAPAFLO treated patients (2.2% for placebo treated) discontinued therapy due to an adverse reaction (treatment-emergent), the most commonreaction being retrograde ejaculation (2.8%) for RAPAFLO treated patients. Retrograde ejaculation is reversible upon discontinuation of treatment.Adverse Reactions observed in at least 2% of patients:The incidence of treatment-emergent adverse reactions listed in the following table were derived from two 12-week, mul-ticenter, double-blind, placebo-controlled clinical studies of RAPAFLO 8 mg daily in BPH patients. Adverse reactions that occurred in at least 2% of patients treated with RAPAFLO and more frequently than with placebo are shown in Table 1. Table 1 Adverse Reactions Occurring in ≥ 2% of Patients in 12-week, Placebo-Controlled Clinical Trials
In the two 12-week, placebo-controlled clinical trials, the following adverse events were reported by between 1% and2% of patients receiving RAPAFLO and occurred more frequently than with placebo: insomnia, PSA increased, sinusitis, abdominal pain, asthenia, and rhinorrhea. One case of syncope in a patient taking prazosin concomitantly and one caseof priapism were reported in the RAPAFLO treatment group.In a 9-month open-label safety study of RAPAFLO, one case of Intraoperative Floppy Iris Syndrome (IFIS) was reported.Postmarketing ExperienceThe following adverse reactions have been identified during post approval use of silodosin. Because these reactions arereported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency orestablish a causal relationship to drug exposure:Skin and subcutaneous tissue disorders: toxic skin eruption, purpuraHepatobiliary disorders: jaundice, impaired hepatic function associated with increased transaminase values
DRUG INTERACTIONSModerate and Strong CYP3A4 InhibitorsIn a clinical metabolic inhibition study, a 3.8-fold increase in silodosin maximum plasma concentrations and 3.2-fold increase in silodosin exposure were observed with concurrent administration of a strong CYP3A4 inhibitor, 400 mg ketoconazole. Use of strong CYP3A4 inhibitors such as itraconazole or ritonavir may cause plasma concentrations of silodosin to increase. Concomitant administration of strong CYP3A4 inhibitors and RAPAFLO is contraindicated [see Contraindications and Warnings and Precautions].The effect of moderate CYP3A4 inhibitors on the pharmacokinetics of silodosin has not been evaluated. Concomitant administration with moderate CYP3A4 inhibitors (e.g., diltiazem, erythromycin, verapamil) may increase concentration of RAPAFLO. Exercise caution and monitor patients for adverse events when co-administering RAPAFLO with moderate CYP3A4 inhibitors.Strong P-glycoprotein (P-gp) InhibitorsIn vitro studies indicated that silodosin is a P-gp substrate. Ketoconazole, a CYP3A4 inhibitor that also inhibits P-gp, caused significant increase in exposure to silodosin. Inhibition of P-gp may lead to increased silodosin concentration. RAPAFLO is therefore not recommended in patients taking strong P-gp inhibitors such as cyclosporine.Alpha-BlockersThe pharmacodynamic interactions between silodosin and other alpha-blockers have not been determined. However, interactions may be expected, and RAPAFLO should not be used in combination with other alpha-blockers [see Warnings and Precautions].DigoxinThe effect of co-administration of RAPAFLO and digoxin 0.25 mg/day for 7 days was evaluated in a clinical trial in 16 healthy males, aged 18 to 45 years. Concomitant administration of RAPAFLO and digoxin did not significantly alter the steady state pharmacokinetics of digoxin. No dose adjustment is required.PDE5 InhibitorsCo-administration of RAPAFLO with a single dose of 100 mg sildenafil or 20 mg tadalafil was evaluated in a placebo-controlled clinical study that included 24 healthy male subjects, 45 to 78 years of age. Orthostatic vital signs were monitored in the 12-hour period following concomitant dosing. During this period, the total number of positive ortho- static test results was greater in the group receiving RAPAFLO plus a PDE5 inhibitor compared with RAPAFLO alone. No events of symptomatic orthostasis or dizziness were reported in subjects receiving RAPAFLO with a PDE5 inhibitor.Other Concomitant Drug TherapyAntihypertensivesThe pharmacodynamic interactions between silodosin and antihypertensives have not been rigorously investigated in a clinical study. However, approximately one-third of the patients in clinical studies used concomitant antihypertensive medications with RAPAFLO. The incidence of dizziness and orthostatic hypotension in these patients was higher than in the general silodosin population (4.6% versus 3.8% and 3.4% versus 3.2%, respectively). Exercise caution during con- comitant use with antihypertensives and monitor patients for possible adverse events [see Warnings and Precautions].Metabolic InteractionsIn vitro data indicate that silodosin does not have the potential to inhibit or induce cytochrome P450 enzyme systems. Food InteractionsThe effect of a moderate fat, moderate calorie meal on silodosin pharmacokinetics was variable and decreased silodosin maximum plasma concentration (Cmax) by approximately 18 - 43% and exposure (AUC) by 4 - 49% across three different studies. Safety and efficacy clinical trials for RAPAFLO were always conducted in the presence of food intake. Patients should be instructed to take silodosin with a meal to reduce risk of adverse events. USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category B. RAPAFLO is not indicated for use in women. An embryo/fetal study in rabbits showed decreased maternal body weight at 200 mg/kg/day (approximately 13-25 times the maximum recommended human exposure or MRHE of silodosin via AUC). No statistically significant teratogenicity was observed at this dose. Silodosin was not teratogenic when administered to pregnant rats during organogenesis at 1000 mg/kg/day (estimated to be approximately 20 times the MRHE). No maternal or fetal effects were observed at this dose. Rats and rabbits do not produce glucuronidated silodosin, which is present in human serum at approximately 4 times the level of circulating silodosin and which has similar pharmacological activity to silodosin. No effects on physical or behavioral development of offspring were observed when rats were treated during pregnancy and lactation at up to 300 mg/kg/day.Pediatric UseRAPAFLO is not indicated for use in pediatric patients. Safety and effectiveness in pediatric patients have not been established.Geriatric UseIn double-blind, placebo-controlled, 12-week clinical studies of RAPAFLO, 259 (55.6%) were under 65 years of age, 207 (44.4%) patients were 65 years of age and over, while 60 (12.9%) patients were 75 years of age and over. Orthostatic hypotension was reported in 2.3% of RAPAFLO patients < 65 years of age (1.2% for placebo), 2.9% of RAPAFLO patients ≥ 65 years of age (1.9% for placebo), and 5.0% of patients ≥ 75 years of age (0% for placebo). There were otherwise no significant differences in safety or effectiveness between older and younger patients.Renal ImpairmentThe effect of renal impairment on silodosin pharmacokinetics was evaluated in a single dose study of six male patients with moderate renal impairment and seven male subjects with normal renal function. Plasma concentrations of silo-dosin were approximately three times higher in subjects with moderate renal impairment compared with subjects with normal renal function. RAPAFLO should be reduced to 4 mg per day in patients with moderate renal impairment. Exercise caution and monitor patients for adverse events. RAPAFLO has not been studied in patients with severe renal impairment. RAPAFLO is contraindicated in patients with severe renal impairment [see Contraindications and Warnings and Precautions].Hepatic ImpairmentIn a study comparing nine male patients with moderate hepatic impairment (Child-Pugh scores 7 to 9), to nine healthy male subjects, the single dose pharmacokinetics of silodosin were not significantly altered in patients with hepatic impairment. No dosing adjustment is required in patients with mild or moderate hepatic impairment. RAPAFLO has not been studied in patients with severe hepatic impairment. RAPAFLO is contraindicated in patients with severe hepatic impairment [see Contraindications and Warnings and Precautions].OVERDOSAGERAPAFLO was evaluated at doses of up to 48 mg/day in healthy male subjects. The dose-limiting adverse event was postural hypotension.Should overdose of RAPAFLO lead to hypotension, support of the cardiovascular system is of first importance. Res-toration of blood pressure and normalization of heart rate may be accomplished by maintaining the patient in the supine position. If this measure is inadequate, administration of intravenous fluid should be considered. If necessary, vasopressors could be used, and renal function should be monitored and supported as needed. Dialysis is unlikely to be of significant benefit since silodosin is highly (97%) protein bound.
Adverse ReactionsRAPAFLON = 466n (%)
PlaceboN = 457n (%)
Retrograde Ejaculation 131 (28.1) 4 (0.9)Dizziness 15 (3.2) 5 (1.1)Diarrhea 12 (2.6) 6 (1.3)Orthostatic Hypotension 12 (2.6) 7 (1.5)Headache 11 (2.4) 4 (0.9)Nasopharyngitis 11 (2.4) 10 (2.2)Nasal Congestion 10 (2.1) 1 (0.2)
Manufactured by: Watson Laboratories, Inc., Corona, CA 92880 USA Distributed by: Watson Pharma, Inc., Morristown, NJ 07962 USAUnder license from: Kissei Pharmaceutical Co., Ltd., Nagano, JapanAddress medical inquiries to: WATSON Medical Communications, P.O. Box 1953, Morristown, NJ 07962-1953 800-272-5525For additional information see: www.rapaflo.comor call 1-866-RAPAFLO (727-2356)Rx Only Revised: November 2009 173761-2 S1109

IN THE TREATMENT OF SYMPTOMATIC BPH*
THAT KEEPS HIM GOING
*Benign prostatic hyperplasia
RAPAFLO® is indicated for the treatment of the signs and symptoms of benign prostatic hyperplasia (BPH). RAPAFLO® is not indicated for thetreatment of hypertension.
Important Safety Information
RAPAFLO® is contraindicated in patients with severe renal impairment (CCr <30 mL/min), severe hepatic impairment (Child-Pugh score ≥10), and with use of strong CYP3A4 inhibitors.
Postural hypotension with or without symptoms (eg, dizziness) may develop when beginning treatment with RAPAFLO®. As with all alpha-block-ers, there is a potential for syncope. Patients should be warned of the possible occurrences of such events and should avoid situations where injury could result. RAPAFLO® should be used with caution in patients with moderate renal impairment. Patients should be assessed to rule out the presence of prostate cancer prior to starting treatment with RAPAFLO®. Patients planning cataract surgery should inform their ophthalmologist that they are taking RAPAFLO®.
The most common side effects are retrograde ejaculation, dizziness, diarrhea, orthostatic hypotension, headache, nasopharyngitis, and nasal congestion.
Please see brief summary of Full Prescribing Information on adjacent page.
Models are for illustrative purposes only.
www.rapafl o.com
© 2010, Watson Pharma, Inc., Morristown, NJ 07960. All rights reserved. 06318 1/10
RAPID RELIEF