Embed Size (px)
Citation preview

Renal pathology associated with stem cell transplantation Megan L. Troxell MD/PhD, OHSU
Hematopoietic stem cell transplantation (HCT, formerly known as bone marrow
transplantation) is an integral part of treatment with curative intent for many hematological malignancies, aplasias, and some solid tumors, while it is also occasionally applied in treatment of autoimmune conditions. In basic principle, the recipient is treated with a conditioning regimen (combinations of radiation and/or chemotherapy) to deplete bone marrow cells, immunity, and destroy residual tumor, followed by infusion of progenitor cells capable of reconstituting hematopoiesis.[Gajewski; Copelan] Historically, this process involved complete myeloablation with transplantation of cells derived from an HLA-identical sibling. However, in the current era, advances have expanded available conditioning regimens, source of cells, and donor pool to increase the availability of HCT and improve outcomes (Table 1).[Gajewski; Copelan; Li; Pasquini] For instance, collection of G-CSF mobilized progenitor cells from the peripheral blood (PBSCT) has largely replaced bone marrow harvest.[Gajewski; Copelan; Li; Pasquini] Further, autologous transplantation, in which the patient’s own marrow is cryopreserved and then replenished, allowing marrow rescue after high-dose tumor chemotherapy with severe marrow toxicity, is seeing vastly increasing use.[Gajewski; Copelan; Li; Pasquini] Each of these variations also modifies the risk of systemic and renal co-morbidities like toxicity, infection, organ failure, acute and chronic graft versus host disease (GVHD), and graft versus tumor effect.[Gajewski; Copelan; Pasquini] As in kidney transplantation, attention to HLA-matching of donor and recipient is crucial in HCT. Even in HLA-identical sibling transplants, minor histocompatibility antigens are mismatched, potentially leading to GVHD or rarely, rejection of the grafted cells.[Gajewski; Copelan; Pasquini] Current research is elucidating interplay of histocompatibility related genes such as KIR (natural Killer Immunoglobulin-like Receptors, of which HLA-C is a ligand), natural killer cell receptors, and polymorphisms of cytokine and chemokine genes (TNF-a, IL-6, IL-10, interferon-gamma, etc).[Gajewski; Toubai]
The HCT transplant recipient is exposed to a number of renal insults before, during, and after stem transplantation (Table 2), which interact with the patients genotype and phenotype to influence transplant complications and outcome. Increasingly, patients have underlying medical conditions such as obesity, metabolic syndrome, hypertension and renal insufficiency. Patients receiving transplants for malignancy have inevitably been treated with multiple chemotherapies and often blood transfusion prior to transplant induction, and perhaps suffer sequelae of the cancer itself including paraneoplastic syndromes, anemia, or tumor lysis syndrome.[Gajewski; Copelan; Singh; Parikh] Conditioning regimens for HCT such as radiation and chemotherapy incite damage to proliferating cells and tissues other than the marrow, with the endothelium particularly susceptible to radiation damage. [Gajewski; Copelan; Singh; Parikh] In the immediate post-transplant period, patients are exposed to fluid imbalance, and some suffer capillary-leak syndrome, or veno-occlusive disease. [Gajewski; Copelan; Singh; Parikh] Before the transplanted stem cells engraft, there is a period of profound pan-hypocellularity with ensuing risk of bleeding, and sepsis as well as fungal and viral infections. Anti-microbial agents given to prevent or treat infections have their own toxicities. Acute and chronic

GVHD are important co-morbidities in allogeneic transplantation, discussed below; the immunosuppressive medications for GVHD prophylaxis/therapy are not risk-free. Transplant associated-thrombotic microangiopathy (TA-TMA) affects a small subset of unfortunate HCT recipients.[Laskin] Given the complexity of factors involved, and the variability of HCT regimens within and even between centers, it has proven challenging to establish firm associations between potential risk factors, kidney disease, and other clinicopathologic outcomes. In the sections below, the pathophysiology of GVHD and transplant associated thrombotic microangiopathy will be covered, followed by renal histopathology in HCT.
Graft versus Host Disease (GVHD)
Patients receiving allogeneic HCT are at risk for graft versus host disease, and are treated with immunousuppressive prophylaxsis early after transplant, usually calcineurin-inhibitor or methotrexate based. Previously, acute and chronic graft versus host disease (GVHD) were distinguished strictly temporally, with a post-transplant day 100 threshold. However, it is now recognized that acute and chronic GVHD are pathophysiologically distinct, and may even have overlapping time courses; thus, diagnostic criteria have been revised accordingly.[Filipovic]
Acute GVHD
Acute GVHD involves a cascade of tissue damage amplified by immune and cytokine activation. The HCT conditioning regimen results in damage of host cells and tissues, with activation of antigen presenting cells (APC), and cytokine release (esp. TNF-alpha, IL-1beta, IL-6).[Socie 2009; Garnett; Ferrarra] Notably, injury to the gastrointestinal mucosa inevitably exposes pathogens and their inflammatory stimuli; viral infection has a similar effect. This process leads to activation and co-stimulation of donor T-cells that react against host antigens, which then expand and differentiate.[Socie 2009; Garnett; Ferrarra] These activated T-cells migrate to target tissues, and while destroying host tissue, also recruit other leukocytes.[Socie 2009; Garnett; Ferrarra] Further tissue destruction results in yet more inflammatory cytokine release, amplifying the inflammatory cascade (the so-called ‘cytokine storm’).[Socie 2009; Garnett; Ferrarra] The regulatory subset of T-cells (Treg: CD4+CD25+FoxP3+) are thought to exert an inhibitory influence in animal models and human studies; Tregs have been shown to be diminished in acute GVHD. The complexity of acute GVHD and our lack of complete mechanistic understanding is illustrated by the observation that some cell types and cytokines may either amplify, or inhibit GVHD depending on the inflammatory milieu and timing of administration (interferon-gamma, IL-10, TGF-beta).[Socie 2009; Garnett; Ferrarra] A capillary leak or ‘engraftment’ syndrome sharing some of the clinical sequelae, and perhaps even some of the cellular and cytokine activation pathways, has been reported in autologous transplant recipients around the time of neutrophil recovery, and is difficult to distinguish from acute GVHD in some allogeneic recipients.[Spitzer]
Patients with acute GVHD present clinically with symptoms such as a maculopapillary rash (epidermal involvement), nausea, vomiting, anorexia, ileus (GI involvement), and/or cholestatic hepatitis (liver). In patients with suspected acute GVHD, infection should be carefully excluded. A clinical grading system of acute GVHD severity has been established, by assessing extent of involvement in the 3 main target

organ systems (skin, GI, liver), denoted Grade I-mild, Grade 2-moderate, Grade III-severe.[Gajewski; Ferrara] Patients receiving reduced intensity conditioning (RIC) regimens are at lower risk of acute GVHD, thought to be associated with less profound tissue damage during conditioning. In the RIC setting, acute GVHD may occur somewhat later post-HCT, even after 100 days.[Filipovich] Likewise, donor lymphocyte infusions may sometimes be administered after HCT when enhanced graft versus tumor effect is needed; this may result in a mild acute GVHD picture, as lymphocytes are administered without toxic conditioning.[Socie 2009; Garnett; Ferrarra] The prevalence of acute GVHD is generally related to the degree of HLA match: 35-45% with matched sibling donor, 60-80% in 1 antigen mismatched unrelated donor),[Ferrara] with a greater incidence in PBSCT as compared to BMT recipients.[Johnston] Acute GVHD may prove fatal in up to 15% of affected recipients.[Socie 2009; Garnett; Ferrarra] Steroids are the mainstay of treatment for acute GVHD, with other forms of immunosuppression also applied in refractory cases (including extracorporeal photopheresis); there has been recent interest in infusion of mesenchymal stromal cells.[Baird; Ferrara; Blazar]
Chronic GVHD In contrast to acute GVHD, chronic GVHD has differences in time course, signs and symptoms, histopathologic features, and pathophysiology, which remains poorly understood. Current theories relate chronic GVHD to autoimmune disorders, perhaps associated with immune dysregulation.[Bruijn; Gajewski; Cutler; Garnett; Filipovich; Tyndall; Ferrara; Blazar] In chronic GVHD, T-cell interplay with macrophages, and B-cells, with chronic inflammation thought to contribute to stimulation of tissue fibroblasts (TGF-beta1, PDGF mediated).[Blazar] The role of antibodies has been a topic of recent interest. Elevated levels of serum auto- or allo- antibodies can be found in up to 70% of HCT patients, including anti-nuclear antibodies, anti-smooth muscle antibodies, anti-mitochondrial antibodies, then allo-antibodies to minor histocompatibility antigens include H-Y antigens in male recipients of stem cells from female donors. [Kapur; Miklos; Zhang] Miklos has reported an odds ratio for chronic GVHD of 15.5 in patients with H-Y antibodies.[Miklos] Interestingly, similar to patients with systemic sclerosis (scleroderma), antibodies to platelet derived growth factor receptor (PDGFR) have been identified in a group of patients with extensive chronic GVHD.[Kapur] These antibodies were shown to activate Ha-ras, ERK(1/2) and lead to increased type collagen I gene expression in fibroblasts in vitro.[Kapur] Chronic GVHD generally manifests clinically as a sclerosing process with examples including lichen-planus like changes of skin and mucous membranes, skin depigmentation, esophageal webs, bronchiolitis obliterans, fasciitis/myositis, dry eyes or sicca syndrome, etc.[Gajewski; Filipovich; Carpenter; Ferrara; Blazar] Again, clinical diagnostic and grading criteria for chronic GVHD have recently been refined.[Filipovic] In this formulation of “Signs and symptoms of chronic GVHD,” nephrotic syndrome is currently listed amongst the “other features” with a footnote: “Can be acknowledged as part of the chronic GVHD symptomatology if the diagnosis is confirmed.”[Filipovic] Chronic GVHD is estimated to affect between 30-65% of HCT recipients, differing by regimen, center and other risk factors.[Gajewski; Filipovich; Carpenter; Ferrara; Blazar] The deleterious chronic GVHD often parallels a beneficial graft vs. tumor effect, with chronic GVHD patients having lower relapse.[Gajewski; Filipovich;

Carpenter; Ferrara; Blazar; Baird] While most patients with chronic GVHD have a history of acute GVHD, one-third are reported to develop chronic GVHD denovo. [Gajewski; Filipovich; Carpenter; Ferrara; Blazar] Like with acute GVHD, steroids are the mainstay of therapy for chronic GVHD, often in combinations with calcineurin inhibitors, with active research into other novel regimens ongoing for treatment of refractory cases.[ Baird; Culter 2006; Ferrara; Blazar] Transplantation-associated thrombotic microangiopathy (TA-TMA) For many years a hemolytic-uremia (HUS) like or thrombotic thrombocytopenic purpura (TTP) like syndrome has been recognized in HCT recipients, often with onset within the first 100 days post-HCT and associated with up to 75% mortality,[Elliott; Laskin] though also occurring many months if not years post transplant,[Antignac; Oyama; Elliott; Ho; Laskin; Jodele; Upadhyay] Although HCT associated thrombotic microangiopathy (TMA) shares the hallmarks of endothelial injury, microangiopathic red cell injury, and platelet consumption, it is now recognized to be distinct from HUS and TTP arising in other settings. Specifically, ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13, hallmark of TTP) has proven to be unperturbed in post-HCT TMA-like syndromes.[Elliott; Laskin] The term transplantation associated thrombotic microangiopathy (TA-TMA) is currently favored (other names over time have included ‘conditioning associated HUS,’ ‘bone marrow transplant nephropathy,’ ‘radiation nephritis’).
Even so, there is little agreement on clinical diagnostic criteria; thus the incidence and risk factors have been difficult to establish; [Ho; Elliott; Hingnorani Singh] a reasonable estimate would be TA-TMA affecting 5-10% of HCT recipients. Inevitably, systemic TA-TMA manifests with combinations of schistocytes and red blood cell fragmentation on blood smear; thrombocytopenia; elevated LDH; renal and/or neurologic dysfunction without other explanation, in the setting of negative direct and indirect coombs test.[Elliott; Ho; Singh] The kidney is particularly susceptible to this process, and histologic features are covered in detail in the renal pathology section below. Both radiation and calcineurin inhibitors, along with virally mediated endothelial injury, inflammatory cytokines and VEGF dysregulation, have been associated with endothelial injury or TMA in other settings, and are common exposures in HCT.[Hingnorani; Changsirikulchai; Laskin 2011; Singh] Various single center clinical studies have cited risk factors for TA-TMA to include infection, matched unrelated donor, HLA-mismatch, RIC, acute GVHD.[Elliott; Laskin 2011; Singh] Prior pediatric reports suggested an association with cis-retinoic acid administration;[Haysom] reports of newer GVHD prophylactic regimens using concomitant sirolimus and tacrolimus administration have also noted an increase in TA-TMA. [Cutler 2005; Rosenthal; Shayani] A large autopsy study from Fred Hutchinson cancer center found the multivariate odds ratio of renal TMA to be 2.7 for female vs. male donor; 1.8-2.2 with total body irradiation vs. none; 3.9 with grade II-IV acute GVHD vs. grade 0-I; 2.3 for adenoviral infection versus none; surprisingly, cyclosporine use had an odds ratio of 1.4 in the third dosage quartile and was only 0.9-1.0 in other dose ranges. [Changsirikulchai] In this study, 2 sets of clinical criteria for TA-TMA were poorly predictive of kidney autopsy findings, [Changsirikulchai] and in an autopsy study from another institution, only 6 of 8 were identified clinically pre-mortem.[Siami]

Historically, plasmapheresis was the mainstay of TA-TMA treatment, generally with poorer response as compared to TMA of other causes.[Laskin 2011] Reduction of calcineurin-based immunosuppression may be possible in a subset of patients.[Laskin 2011] Newly developed agents undergoing study in TA-TMA include rituximab, TNF-alpha and complement inhibitors.[Laskin 2011] Following on recent data indicating alternative complement pathway abnormalities in atypical HUS in non-transplant patients, in a cohort of 6 pediatric patients with TA-TMA Jodele et al. found five recipients and one donor to have heterozygous deletion of CFHR3-CHFR1 gene region. Further, the three patients receiving allogeneic transplants had CFH antibodies, presumably denovo post transplantation. [Jodele 2013]. In small case series from this group and another case report, patients with severe TA-TMA were treated with the anti-complement C5 antibody eculizumab, with resolution in 5 of 7, and death in the other 2 critically ill patients. [Peffault; Jodele 2014] Interestingly, in successfully treated TA-TMA patients, eculizumab has been discontinued, unlike the experience thus far with atypical-HUS patients. [Peffault; Jodele 2014] Acute Kidney Injury post-HCT As discussed above, the process of HCT subjects recipients to a wide variety of insults, many of which are nephrotoxic and synergistic (Table 2). Depending on the AKI definitional criteria, the patient population and transplant protocol, an estimated 20-75% of HCT recipients experience acute kidney injury (AKI) during their course;[Parikh; Singh] most never undergo renal biopsy. Risks of AKI generally parallel the type of transplant and conditioning regimen. Myeloablative allogeneic transplant recipients have the greatest incidence of AKI (up to 75% with Grade II AKI or greater), [Schrier; Parikh; Singh] in that patients are subjected to the most toxic conditioning, often experience acute and chronic GVHD, and are exposed to potentially nephrotoxic GVHD prophylaxis (calcineurin inhibitors). About 40% of patients receiving reduced intensity (RIC) allogeneic transplants experience AKI, which may occur a bit later after transplant as compared to myeloablative; these patients experience less toxic induction, with perhaps less resultant risk of sepsis or infection.[Schrier; Parikh; Singh] Yet, RIC recipients require GVHD prophylaxis, and are selected based on their older age and greater co-morbidities at baseline (which may include chronic kidney disease). Autologous HCT recipients have the lowest incidence of AKI, on order of 20-25%,[Schrier; Parikh; Singh] although they undergo an intense conditioning regimen, there is no risk of GVHD or need for prophylaxis.
Sinusoidal obstruction syndrome (hepatic veno-occlusive disease) carries a particularly high risk for AKI or even renal failure.[Parikh; Singh] Renal failure requiring dialysis occurs in a smaller number of HCT recipients, especially immediately during or after transplant, with risk paralleling that of AKI (5% in autologous or RIC, up to 30% in myeloablative allogeneic), and mortality is high in this group.[Schrier; Parikh; Singh] Indeed, Cohen has calculated a 16-fold risk of end stage renal disease among HCT recipients, as compared to 2.7-fold risk amongst patients treated for solid tumors.[Cohen] Treatment for AKI or renal failure in this setting is primarily supportive, while reducing exposure to potentially nephrotoxic agents. [Noel; Schrier; Parikh; Singh; Clajus] A glimpse of histopathologic changes during HCT engraftment is provided by allograft kidney biopsies of small numbers of patients undergoing combined HCT and

kidney transplant in Immune Tolerance Network trials.[Farris] Farris et al. reported findings in 12 biopsies from 10 patients from 10-24 days post kidney-HCT transplant during the period of marrow regeneration and mixed chimerism, many of whom presented with AKI and/or systemic features of capillary leak/engraftment syndrome (fever, fluid retention).[Farris] Principal findings included marked tubular injury, along with interstitial edema and hemorrhage.[Farris] Further, there was peritubular and capillary congestion, with red blood cells, monocytes, myeloperoxidase-positive cells, and T-cells. Remarkably, electron microscopic analysis showed reactive endothelial changes and segmental endothelial loss in both glomeruli and peritubular capillaries.[Farris] Additionally, two biopsies were found to have acute antibody mediated rejection, and two acute cellular rejection.[Farris] While this study provides a tantalizing view of renal pathology during post-HCT AKI and capillary leak syndrome, these were biopsies of the simultaneous kidney allograft, and might not reflect findings in native kidneys during HCT. Chronic Kidney Disease post-HCT Hematopoietic stem cell recipients have an estimated 15-20% incidence of chronic kidney disease (CKD), which manifests as slowly increasing creatinine/decreasing glomerular filtration rate (GFR), often accompanied by anemia and hypertension.[Singh, Hingorani 2006; Ellis; Parikh; Abboud] As with AKI, CKD is inevitably multifactorial. Again based on varying definitions, transplant populations, and regimens, the incidence of and risk factors for CKD varies considerably in the literature (Table 3). Prior AKI is recognized as an important risk factor for CKD, with others including calcineurin exposure, GVHD, TA-TMA, and possibility radiation-based conditioning.[Ellis; Weiss; Ando; Al-Hazzouri; Choi; Hingnorani 2007; Saddadi] Like AKI, CKD is also lower in autologous or RIC HCT recipients.[Singh, Hingorani 2006; Ellis; Parikh; Abboud] In the absence of proximate treatable cause, therapy is generally empiric as in other cohorts with CKD (ACE/ARB, blood pressure reduction), along with calcineurin inhibitor minimization. [Hingorani 2006; Ando; Abboud; Singh] Renal histopathology post-HCT: glomerular disease As discussed above, renal injury in HCT recipients is often multi-factorial, and may not lead to tissue biopsy if acute/self-limited or slowly chronic. The literature on pathologic changes in HCT is comprised of a mixture of case reports, small single center biopsy series, and autopsy studies, which often focus on a single clinicopathologic cohort such as nephrotic syndrome, membranous nephropathy (MN), TA-TMA, viral infection, etc. The role of chronic GVHD in HCT-related renal pathology remains enigmatic, and is discussed further in the membranous nephropathy section. Although there is publication bias, several themes emerge.
The incidence of post-HCT nephrotic syndrome is difficult to establish, but it can be estimated as 0.5-4%,[Srinivasan, Perrotta, Colombo, Reddy, Kemper, Chan, Troxell, Luo, Fraile] and manifests later post-transplant, often after the first year (Table 4).[Brukamp; Hu] Many of these patients undergo biopsy, revealing membranous nephropathy or minimal change disease. These and other glomerular findings are discussed below (Table 4). Although some patients with severe thrombotic microangiopathy (TA-TMA) cannot undergo renal biopsy due to bleeding risk, this

nevertheless represents another common theme in post-HCT renal biopsy pathology. Infections, most notably polyomavirus or adenovirus, are important to recognize on biopsy and may be clinically unsuspected. Tubulointerstitial pathology such as acute interstitial nephritis or acute tubular injury/necrosis represent the primary pathologic lesion in another subset of cases. In series reporting renal histopathologic findings in detail, a striking observation is that many biopsies demonstrate multiple abnormalities impacting glomeruli, vessels, tubules, and/or interstitium (Table 5, Figures 1-2). [Lin; El-seisi; Chang; Terrier; Troxell; terrier; Schwarz; Mii; Brinkerhoff]
Membranous Nephropathy (MN) Membranous nephropathy (MN) is the most common glomerular disease in kidney biopsies in HCT recipients; more than 79 cases have been reported in the literature, representing about 57% of post-HCT glomerular disease, or 36% of published post-HCT renal biopsies (Table 4).[Brukamp; Srinivasan; Colombo; Reddy; Chang; Kemper; Terrier; Troxell; Hu; Huang; Fraile-Pilar; Niscola, among others] Male recipients make up 72% of reported MN cases; of the minority reporting donor/recipient sex, 6/15 represent female donor to male recipient, while the remainder were sex matched (1 female to female, the remainder male, Table 4). HCT patients with MN generally present with the nephrotic syndrome, or nephrotic range proteinuria, and have nearly normal creatinine, as in MN in other clinical settings (Table 4).[Brukamp; Srinivasan; Colombo; Reddy; Chang; Kemper; Terrier; Troxell; Hu; Huang; Fraile-Pilar; Niscola, among others] Most patients are treated with immunosuppressive regimens, leading to complete resolution in about 60-70%.[Hu; Niscola; Upadhyay] Typical light microscopic features of MN include thick-appearing glomerular basement membranes, with ‘spikes’ or ‘corrugated’ texture as seen on silver stains. Immunofluorescence microscopy demonstrates deposition of immunoglobulin G, both light chains, and often C3 along capillary loops in a typical granular pattern. Corresponding subepithelial electron dense deposits are seen on ultrastructural analysis (Figure 1). MN has been seen in biopsies together with FSGS, microaneurysms, mesangiolysis, global glomerulosclerois, interstitial inflammation, interstitial fibrosis, acute tubular injury, tubular atrophy, arteriolar hyalinosis, arteriosclerosis. [Lin; Chang, Terrier; Troxell]
Phospholipase A2 receptor (PLA2R) has been identified as a target of autoantibodies (especially IgG4 subclass) in so-called primary or idiopathic MN.[Beck] Only a few post-HCT patients have been studied either serologically or by tissue immunofluorescence for PLA2R or IgG4 antibodies to date. Terrier reported 5 French patients with post-allogeneic HCT MN (all but one RIC), and noted dominant or co-dominant IgG4 deposition in 3 of 4 tested biopsies.[Terrier] Huang et al studied 5 allogeneic HCT recipients and likewise found that all had dominant or co-dominant IgG4 deposition in kidney tissue by immunofluorescence; however only 1 had positive serum PLA2R antibodies.[Huang] Abboud mentioned negative serum PLA2R in each of 3 tested post-HCT patients with MN.[Abboud] Given the prevalence of MN in post-HCT patients with chronic GVHD, possible temporal correlation with tapering of immunosuppression, and favorable response to treatment with immunosuppression, many authors have put forth post-HCT MN as a potential renal manifestation of chronic GVHD. Two meta-analyses have explored this

question in particular detail.[Brukamp; Hu] Brukamp concluded that the literature supported the concept of renal GVHD, specifically glomerular lesions with nephrotic syndrome clinically (membranous glomerulopathy or minimal change disease histopathologically).[Brukamp] In contrast, based partially on the low incidence of MN in HCT-patients with chronic GVHD (comparable to incidence of MN in the population overall), along with the similar high rate of chronic GVHD amongst HCT patients with MN and rate of chronic GVHD in HCT patients overall, Hu reached a different conclusion, recognizing complex and likely multi-factorial contributions to HCT associated glomerular disease.[Hu] In a review of renal disease in HCT and solid organ transplantation, Clajus additionally emphasized the occurrence in autologous HCT recipients, potential influence of chemotherapy related podocyte pathology, relapse associated paraneoplastic phenomena, and the contribution of endothelial and tubulointerstitial injury to proteinuria, and concluded that it is “matter of debate whether proteinuria after HSCT represents a late complication rather than a genuine manifestation of GVHD.”[Clajus] Perhaps immune dysregulation in the setting of HCT facilitates development of MN in patients who are otherwise susceptible due to risk alleles (PLA2R HLA), paraneoplastic or infectious exposures.[Stanescu] Clearly, the question of MN or nephrotic syndrome as a renal manifestation of GVHD deserves further study. Minimal change disease Minimal change disease (MCD) is the second most common glomerular disease reported in post-HCT kidney biopsies; representing about 19% of post-HCT glomerular disease, or 12% of published post-HCT renal biopsies (Table 4).[Gomez-Garcia; Brukamp; Chang; Hu; Schwarz, among others] Like in MN, patients generally present with the nephrotic syndrome, or nephrotic range proteinuria; many, but not all, have normal creatinine (Table 4). Renal biopsy with immunofluorescence and/or electron microscopy is need to distinguish MCD from MN or other causes of nephrotic syndrome. MCD generally resolves (70-90%), and many patients are treated with immunosuppressive regimens. [Brukamp; Hu] Characteristic pathologic features of MCD include morphologically normal glomeruli by light microscopy, negative immunofluorescence studies, and diffuse podocyte foot process effacement by electron microscopic analysis (Figure 1). Interestingly, a few cases of post-HCT MCD have been reported or illustrated in association with a brisk interstitial nephritis.[Romagnani; Huskey; Humphreys] Indeed, in non-transplant settings, MCD has been speculated to be associated with T-cell dysregulation or hypersensitivity reaction (eg. Hodgkin lymphoma, drug reaction); thus it makes sense that HCT patients with immune dysregulation should be at risk for MCD. Seconi illustrated a an HCT patient with MCD and serial cytokine measurements demonstrating TNF-alpha and IL-gamma peaking at disease onset and decreasing with reinstatement of immunosuppression and resolution of nephrotic syndrome.[Seconi] However, the number of post-HCT patients presenting with MCD is quite low, and co-incidental association cannot be excluded. Other renal histopathologic findings reported in biopsies with MCD include acute tubular injury/necrosis, arteriopathy.[Chang; Humphreys; Silva; Troxell] Other glomerulonephritides

Various case reports include instances of focal segmental glomerulosclerosis (FSGS) in the setting of HCT, sometimes following or coincident with another glomerular process (Table 4, Figure 1). [Oliveria; Chan; Imai; Brukamp, Chang; Troxell; Fofi; Schwarz; Fraile Pilar; Brinkerhoff] Interestingly, FSGS accounts for 9% of published glomerular disease biopsies in HCT patients, a far lower percentage than reported in the general renal biopsy experience (20-40% and higher).[Dragovic; Swaminathan] This could represent a real phenomenon, reflecting underlying features of the HCT population, or sampling/publication bias in which HCT patients with slowly progressive renal dysfunction and proteinuria are not offered biopsy. It will be interesting to see whether FSGS increases over time in the HCT population as patients survive longer post transplant with fewer early systemic and renal complications.
Individual case reports or small series have rarely reported other glomerular abnormalities in HCT recipients, including IgA nephropathy, membranoproliferative glomerulonephritis (MPGN), mesangial proliferative glomerulonephritis (sometimes with mesangiolysis), some without description and/or illustration (Table 4). Additionally, five cases of crescentic glomerulonephritis have been reported, including two ANCA associated and one anti-glomerular basement membrane disease (Table 4).[Takeuchi; Suehiro; Kingdon, Nouri; Brinkerhoff] Again, HCT patients with these glomerular lesions often have concomitant tubulointerstitial or vascular pathology.
Renal histopathology post-HCT: Transplantation-associated thrombotic microangiopathy (TA-TMA) Critical illness and propensity for bleeding often preclude renal tissue sampling in acute life threatening TA-TMA, and the patient is treated based on clinical and laboratory parameters. Nevertheless, TA-TMA may be renal limited or clinically unsuspected, making renal biopsy crucial in diagnosis and appropriate treatment in this subset of patients. Based on the reported TA-TMA renal biopsies, patients have been biopsied even well over 1 year post-HCT (average 16.8 months, range 1 week-7.75 years), generally with elevated creatinine (average 2, range 1-6), and non-nephrotic proteinuria (Table 4).[Antignac; Butcher; Chang; Chan; Glezerman; Mii; Laskin; Brinkerhoff] Interestingly, about 40% of patients biopsied for TA-TMA underwent autologous HCT, a far lower percentage than reported for MN or MCD (about 5%, Table 4). Risk factors for TA-TMA have been discussed above; however, it is worth emphasizing that autopsy studies have seen associations with prior infection, or death due to infection. [Changsirikulchai; Siami] Light microscopic changes in vascular and glomerular endothelium in TMA are often dramatic, but alternatively, they may be only focal and quite subtle. [Siami; Laskin] Characteristically, arterioles and small arteries show intimal swelling, often with a concentric myxoid or mucoid character, along with fibrinoid necrosis, insudated fibrin, or thrombosis. Thus, glomeruli are often ischemic, with wrinkling and retraction of the tuft. Further, glomeruli are classically described as ‘bloodless’ due to glomerular endothelial cell swelling; intralumenal fibrin may also been seen. Mesangial zones can be expanded by edematous fibrillary material (so-called mesangiolysis). Fragments of red blood cells can be seen entrapped in the swollen vascular or glomerular endothelium, or in the mesangium. In chronic thrombotic microangiopathy, capillary walls may appear thick on

H&E stains, or ‘double contoured’ on PAS or silver stains due to chronic injury resulting in new basement membrane formation.
The glomerular ultrastructural correlates of these changes are classic and include swollen endothelial cells separated from the glomerular basement membrane by a lucent zone including flocculent debris and cellular fragments (Figures 1-2). Similar changes in the mesangial zone correspond to mesangiolysis. Fibrin tactoids may been seen in the subendothelial zone, in the capillary lumen, elsewhere in glomeruli, or in involved arterioles/arteries. Podocyte foot process effacement is common. In chronic lesions, there is organization with formation of new inner glomerular basement membrane, often delicate and lamillated. Chronic TMA shares ultrastructural features with allograft glomerulopathy in transplanted kidneys. Subtle endothelial injury or subendothelial widening can be seen in post-HCT biopsies with other diagnoses. By immunofluorescence analysis, glomeruli in TA-TMA are typically negative for immune complexes; non-specific insudative staining may be seen, along with fibrin. Likewise, fibrin and accompanying protein may be seen in small vessels. Two small studies have recently described C4d deposition along glomerular capillary loops or in arterioles in HCT renal biopsies with TA-TMA (in numbers comparable to our unpublished experience in non-transplant TMA patients);[Mii; Laskin 2013] other labs do not observe C4d staining in TMA, suggesting differences by method or antibody. Thus, further study is needed as to specificity or implications of C4d as a marker of complement activation in the setting of endothelial injury or perhaps even humoral GVHD.[Mii; Laskin 2011, Laskin 2013] Renal histopathology post-HCT: Infection HCT recipients should be thought of as immunosuppressed hosts, even after marrow engraftment and tapering of GVHD prophylaxis. Thus, they are susceptible to the usual spectrum of infectious agents, both systemically, and in the kidney. Interstitial nephritis, granulomas, or necrosis, should prompt consideration of bacterial, mycobacterial and fungal organisms. Tubular nuclear enlargement may be merely reactive, but it should lead to evaluation for viral cytopathic change. Cytomegalovirus and adenovirus may be seen in the kidney as well as the gastrointestinal system and liver; polyomavirus has unique trophism for the renourinary tract. Infections like CMV not only wreck havoc on their own, but resultant immune activation tends to increase GVHD (or rejection in solid organ transplantation), and may be associated with secondary bacterial or fungal infections. Polyomavirus
The polyomavirus family includes simian virus 40 (SV40), BK, JC and the recently described Merkel Cell polyomavirus, among others. Ninety percent of the adult population is seropositive for BK polyomavirus, and the virus generally remains latent in the urothelium, but is sporadically reactivated, especially during episodes of immunosuppression.[Stracke; O’donnell; Limaye] BK and rarely JC polyomaviruses are a well-established cause of nephropathy in renal transplant patients, and of hemorrhagic cystitis in HCT patients, but also may cause polyomavirus nephropathy in HCT. Several groups have advocated for BK surveillance in HCT populations, as has become common place in renal transplant recipients.[Verghese; O’donnell] Polyomavirus bladder infection

is an important cause of hemorrhagic cystitis, with potential contribution from chemotherapeutic agents (particularly cyclophosphamide, busulfan, etoposide), radiation, CMV and adenovirus.[Kloos; Bruno] Incidence of hemorrhagic cystitis is reported as 5-20% in modern pediatric HCT series.[Kloos; Koskenvuo] In addition to pain and anemia, blood clots in hemorrhagic cystitis may lead to kidney obstruction. In a single center study of allogeneic HCT recipients, O’donnell et al. reported a 65% incidence of BK viruria, 17% incidence of BK viremia, and both of 2 biopsied patients (2%) with polyomavirus nephropathy.[O’donnell] HCT patients with polyomavirus nephropathy have been biopsied about 2 years post transplant, all with elevated creatinine at the time of biopsy (Table 4). [Shapiro; Stracke; Chang; Lekakis: Limaye; Verghese]
Histologic features of polyomavirus nephropathy in HCT recipients includes tubular epithelial intranuclear inclusions with a glassy to granular texture, and basophilic to pale staining, sometimes surrounded by a clear halo, but without cytoplasmic inclusions. Pale glassy casts may contain viral debris in severe cases. Viral inclusions are accompanied by interstitial inflammation, tubulitis and tubular epithelial injury. Polyomavirus can be nicely demonstrated in tissue sections by immunohistochemistry or alternatively in-situ hybridization. Ultrastructurally, infected nuclei contain 40-50 nm polyomaviral particles, often arranged as a tightly packed lattice.[Colvin]
Adenovirus
Adenovirus infection is increasingly recognized as a complication in HCT, including enteritis, hemorrhagic cystitis, hepatitis, pneumonia, encephalitis, and multiorgan failure. Bruno reported a predominantly autopsy series of 21 cases of adenovirus nephritis over a 21 year period (during which time 6329 patients were treated with HCT, 0.3%).[Bruno] Most patients presented with acute kidney injury, which was often attributed clinically to other causes such as drug toxicity. Adenoviral inclusions may be seen in renal tubular epithelial nuclei; however, the distinctive features of adenovirus as compared to CMV and BK include necrosis of tubules and interstitium, often with surrounding granulomatous and neutrophilic inflammation.[Bruno: Storsley; Lim; Colvin] Like BK, adenovirus has a proclivity for the medulla and distal nephron. [Bruno; Storsley; Lim; Colvin] Again, immunohistochemical (or in-situ hybridization) studies are practical in confirming adenovirus in biopsy samples. Ultrastructurally, adenovirus particles are each 70- to 80-nm, often packed in arrays of variable electron density, within tubular epithelial nuclei or cytoplasm.[Lim; Gibson; [Bruno: Storsley; Lim; Colvin]
Cytomegalovirus
Active cytomegalovirus (CMV) end-organ disease in HCT recipients has been reduced by prophylactic antiviral therapy or a program of surveillance followed by prompt treatment of detectable virus.[Ariza-Heredia] CMV seropositive recipients are at greatest risk of CMV reactivation and disease.[Gajeweski; Ariza-Heredia] Other risk factors for CMV in HCT include age, UBSCT, conditioning (especially total body irradiation, fludarabine, or T-cell depletion), GVHD, low CD4 count, allogeneic as compared to autologous graft; RIC regimens increase risk of late CMV.[Ariza-Heredia] While CMV pneumonitis incidence ranges from 1-30%, and the culmulative incidence of CMV GI disease in HCT patients is reported at about 2% at 2 years, incidence of renal

CMV infections in HCT is lower.[Ariza-Heredia] Drugs used for CMV prophylaxis or therapy such as foscarnet, or to a lesser degree gancyclovir and analogs, also have renal toxicity.[Ariza-Heredia]
Histopathologically, CMV can be seen as typical ‘owl-eye’ nuclear inclusions, sometimes accompanied by cytoplasmic inclusions, focally in tubular epithelial cells, or less commonly in endothelial cells (peritubular capillary, arterial, even glomerular), podocytes, or mononuclear leukocytes.[Colvin; Rane] Viral infection is often accompanied by an inflammatory infiltrate, often including plasma cells, which may even be granulomatous.[Colvin; Rane] In renal transplant patients, CMV glomerulopathy has also been described, characterized by endothelial cell swelling, fibrillar deposits in capillaries, mononuclear cell infiltrate and mild segmental hypercellularity, and CMV is associated with increased TA-TMA. [Weiss 2007; Rane; Onuigbo] Immunohistochemical or in-situ hybridization studies on biopsy tissue are useful for specific confirmation. As in other organ systems, ultrastructural evaluation reveals viral particles of 150 nm with a dense core surrounded by a membrane envelope, often in both nucleus and cytoplasm. [Colvin] Herpes simplex virus is a relative, also with propensity for infection of the immunocompromised population, but rarely directly affects the kidney.
Renal histopathology post-HCT: Tubulointerstitial pathology
HCT patients with kidney tubulointerstitial lesions are under-biopsied and/or under-reported as compared to patients with glomerular disease or nephrotic presentation. Nevertheless, case reports and small series have documented acute tubular injury/necrosis (ATN), acute interstitial nephritis, and chronic interstitial nephritis (CIN) in HCT patients (Tables 4-5). As discussed above, AKI in immediate post-transplant period is quite common and generally does not prompt biopsy. As in other settings, HCT patients with ATN or acute interstitial nephritis (AIN) most often present with elevated creatinine and decreased renal function, with low-moderate levels of proteinuria and hematuria, and reported biopsies have been performed about 6 months post-HCT (range 1-10 months, Table 4).[Butcher; Imai; Chang; Terrier; Troxell; Homma; Chan 2008; Schwarz; Brinkerhoff] Again, HCT recipients have exposure to a number of agents potentially injurious to renal tubules including hemodynamic, multiple drugs, infection, etc. Likewise, AIN could be a manifestation of drug hypersensitivity, post-viral syndrome, or inflammatory/regenerative response to tubular injury; however, in this population, it could also derive from an immune reconstitution or dysregulation syndrome, or a form of GVHD. In a female HCT-patient with MCD and AIN, Romagnani et al. used molecular techniques to demonstrate high levels of the SRY gene in inflammation rich areas, confirming (male) donor derivation of the infiltrating T-cells (and ruling out T-ALL relapse).[Romagnani] Similarly, using fluorescence in-situ hybridization, Kimura demonstrated female donor derivation of the inflammatory cell infiltrate accompanying a crescentic IgA nephropathy.[Kimura] Several autopsy studies and one biopsy case have noted tubulitis and/or peritubular capillaritis in HCT patients.[Homma, Kusumi, El-Seisi] One group found association with a history of severe acute or extensive chronic GVHD,[Kusumi] while the other did not.[El-Seisi] Interpretation of these autopsy studies are complicated by inflammation that may be associated with the peri-mortem period (infection, sepsis, bleeding, multi-organ failure, etc). Nevertheless, etiology of ATN or AIN may remain inapparent in individual cases.

Typical histologic features of acute tubular injury (ATN) include ectatic tubules lined by flattened epithelial cells with loss of brush border and reactive nuclei. With increasing severity, sloughed epithelial cells are seen in tubular lumens, and scattered mitotic figures in intact regenerating cells. AIN is characterized by an interstitial inflammatory cell infiltrate, which can be patchy and sometimes quite sparse, often with scattered tubulitis. The infiltrate is usually mixed, but predominantly mononuclear with a minority of eosinophils or neutrophils. Necrosis, granulomas, or tubular nuclear inclusions, should prompt consideration of infection; neutrophilic casts are most commonly seen in pyelonephritis or reflux nephropathy. Prolonged interstitial nephritis and/or tubular injury leads to interstitial fibrosis and tubular atrophy.
Renal histopathology post-HCT: Chronic vascular and renal disease
Although TA-TMA is a deleterious vascular complication of HCT, and radiation therapy is known to cause intimal fibrosis or myointimal proliferation, sometimes with accompanying foam cells and medial fibrosis,[Fajardo] particular renovascular effects of HCT have not been characterized. Nevertheless, these would be difficult to separate from the arterio- and arteriolosclerosis that are becoming ubiquitous in the general middle-age population. Arteriolar medial hyalinosis is a potential histologic correlate of chronic calcineurin inhibitor toxicity; however, arteriolar hyaline may be seen in hypertension, diabetes, and may be non-specific.(Figure 2)
Like acute tubulointerstitial pathology mentioned above, chronic tubulointerstitial and even chronic glomerular damage is under recognized in the renal HCT literature, and again would be difficult, if not impossible, to dissect from pre-existing or unrelated chronic renal injury. Among studies providing a comprehensive view of renal biopsy or autopsy pathology, over half of specimens demonstrate substantial interstitial fibrosis and tubular atrophy, over half show global glomerulosclerosis (average 10%- 20% globally sclerotic glomeruli per biopsy), and over half have arteriolar hyaline (Table 5, Figure 2).[El-Seisi; Chang; terrier; Troxell; Mii; Schwarz; Brinkerhoff] Importantly, these studies also emphasize that morphologic renal lesions are often multiple, with glomerular, tubulointerstitial and vascular lesions co-existing.
Renal histopathology post-HCT: Recurrent malignancy Multiple myeloma, plasma cell dyscrasia, and B-cell lymphoproliferative disease are common indications for HCT. Thus, recurrence after HCT once again exposes the kidney to potentially injurious excess of light chain, which may manifest as amyloidosis, monoclonal immunoglobulin deposition disease, or light chain cast nephropathy-tubulopathy.[Chang] Various glomerular diseases, most notably membranous nephropathy or minimal change disease, may occur as paraneoplastic sequalae of recurrent solid or hematolymphoid malignancies. The kidney may rarely be directly infiltrated by recurrent tumor. Certainly, renal effects of recurrent disease are also underreported in the literature. Kidney Transplant after HCT In HCT recipients with end-stage renal disease (ESRD), survival on dialysis is reported to be particularly poor, with an estimated 45-50% 2-year survival.[Hamawi] Small pediatric and adult case series have reported favorable outcomes with post-HCT

kidney transplantation.[Upadhyay; Butcher; Thomas; Hamawi] In the situation where the hematopoietic stem cells and subsequent kidney are derived from the same donor, little or no long-term immunosuppression is needed.[Upadhyay; Butcher; Thomas; Hamawi] Upadhyay and Fine have recently reviewed post-HCT kidney and other solid organ transplantation.[Upadhyay] These patients, like all transplant recipients, remain suspectible to infection and second malignancies. Post-transplant lymphoproliferative disorder (PTLD) and second malignancies Recipients of HCT or other solid organ transplants are susceptible to post-transplant lymphoproliferative disorder (PTLD), often related to Epstein-Barr virus (EBV) infection/reactivation, with risk related to donor and recipient EBV status, type of allograft, and intensity of immunosuppression, among other factors. PTLD incidence in HCT is about 1%, [Opelz] and may manifest in lymph nodes, tonsils or in any solid organ. Based on the World Health Organization classification, the spectrum of PTLD includes early (mononucleosis like, plasmacytic hyperplasia), polymorphic, monomorphic (clonal and classified as per lymphoma), and classical-Hodgkin like.[Swerdlow] Heavily treated patients with hematologic malignancies are particularly susceptible to subsequent myelodysplasia or leukemia.
The incidence of epithelial or solid tumors is estimated at 2 to 6-fold that of the general population, and tend to occur late, median 5-6 years post-HCT. [Socie 2012; Davidson-Moncada] HCT and other transplant patients have particular susceptibility to skin cancers, and we have seen a broad variety of malignancies in our local HCT population (renal cell carcinoma, lung carcinoma, pancreatic carcinoma, head & neck squamous cell carcinoma, breast carcinoma, sarcoma, etc); hepatocellular (especially with Hepatatis C) and thyroid cancers are also relatively common.[Socie 2012 and unpublished] However, contributions of factors such as underlying genetics, chemotherapy, radiation, immune dysregulation (chronic GVHD) to second malignancies in HCT patients remain undetermined. Conclusion The kidney is subject to a large variety of injurious factors before, during and after HCT, leading to a high incidence of AKI and CKD, though renal biopsies may be deferred in many clinical situations. Nevertheless, renal biopsy with light, immunofluorescence and ultrastructural analysis yields important diagnostic insight to guide treatment. Membranous nephropathy is the most common glomerular lesion in the setting of HCT, followed by minimal change disease. However, renal biopsy often reveals a number of concurrent abnormalities in glomeruli, tubules, interstitium, and vessels.

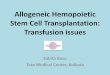
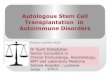
Figure 1: Common ultrastructural findings in post-HCT glomerular pathology A: Minimal change disease with diffuse podocyte foot process effacement B: Membranous nephropathy with subepithelial electron dense deposits and podocyte foot process effacement C: Thrombotic microangiopathy showing a prominent subendothelial lucent layer. This example also has diffuse podocyte injury. D: From a case of FSGS with diabetic nephropathy, mesangial sclerosis is prominent at the margin of a nodule (lower right), and glomerular basement membranes are thick. Podocyte foot process effacement is also seen. Figure 2: Renal biopsy reveals multiple pathologies in a HCT patient The patient received a bone marrow transplant for ALL almost 3 years prior. Her post-transplant course was complicated by recurrent hip infections with significant antibiotic exposure. She received calcineurin inhibitors during the first 8 post-HCT months, but not since. At the time of biopsy, she had nephrotic range proteinuria (urine protein:creatinine ratio=11), and serum creatinine had decreased to 1.3. A: H & E light microscopy demonstrates abundant arteriolar hyaline (arrows), and atrophy of surrounding tubules with interstitial fibrosis. The glomerular mesangial zones appear expanded with thick-appearing capillary loops and retraction of the tuft. B: Jones silver stain shows glomerular basement membrane double contours, with hyaline again prominent in the hilar arteriole. Subtle spikes were apparent in rare segments (not shown). C: IgG1 immunofluorescence with segmental immune deposits along capillary loops. There was great variation in staining within glomeruli (as shown) and between glomeruli (not shown). IgG, kappa, and lambda had the same pattern. IgG3 and IgG4 were negative, while IgG2 stained very weakly. D: Electron microscopy shows an expanded, somewhat lucent, subendothelial zone, consistent with thrombotic microangiopathic change, and injured podocytes. E: Electron microscopy with rare subepithelial electron dense deposit (arrow); no others were seen in the small sample for electron microscopy. Within the expanded subendothelial zone there is hyaline/debris.

A
DC
BFigure 1

A
E
C
D
BFigure 2

Table 1: ABC’s of hematopoietic cell transplantation Transplant parameter Definition and comments Conditioning regimen Myeloablative Maximal intensity chemotherapy and/or radiation resulting in hematopoietic (and
tumor) destruction Reduced Intensity Conditioning (RIC) Less intense conditioning regimen geared toward immunosuppression to facilitate
engraftment & graft versus tumor effect rather Initially yielding mixed marrow chimerism (donor + recipient stem cells), generally converting to pure donor Allows HCT in older, more debilitated patients Less acute GVHD due to less cellular and especially mucosal injury Also called ‘mini’ transplant, or ‘non-myeloablative’
Cell Source Bone Marrow (BMT) Hematopoietic progenitors are harvested directly from marrow (eg. Iliac crest) Peripheral Blood (PBSCT) G-CSF and chemotherapy mobilized hematopoietic progenitors, harvested from
peripheral blood Usually encompasses stem cell enrichment (CD34-selection) or T-cell depletion Greater GVHD and graft versus tumor effect
Umbilical Cord (UBSCT) From cord blood banks More tolerant of HLA-mismatches; often 2 donors are required to obtain sufficient numbers of stem cells for engraftment
Donor Autologous Donor’s own hematopoietic progenitors are infused after chemotherapy
No risk of GVHD; no graft versus tumor effect Implies need for tumor free HCT harvest
Syngeneic Hematopoietic progenitors from an identical twin donor Allogeneic Hematopoietic progenitors from another individual Matched related donor (MRD) Sibling with identical HLA profile (eg. 8/8 loci) Haploidentical Identical at half of HLA loci (1 chromosome, eg. parent-child or siblings)

Matched unrelated donor (MUD) HLA matched non-relative (mismatched unrelated may be used if no other options) more minor histocompatibility mismatches than relative

Table 2: Cumulative renal risks factors and co-morbidities of hematopoietic cell transplantation Prior to transplant Patient’s genotype and phenotype
Medical history (age, hypertension, obesity, metabolic syndrome) Prior chemotherapy Effects of malignancy Blood Transfusion Pre-existing renal insufficiency
During/early post- HCT
Conditioning Chemotherapy Radiation Tumor lysis syndrome Marrow transfusion toxicity (DMSO/cell debris/protein precipitates) Capillary leak Fluid imbalance/pre-renal/hypoperfusion (esp. nausea/vomiting/diarrhea/mucositis) Sinusoidal obstruction syndrome (Veno-occlusive disease) Profound pancytopenia/immunosuppression Sepsis Viral infection Fungal infection Drugs Anti-microbial (treatment/prophylaxis) Anti-GVHD (treatment/prophylaxis, esp. calcineurin inhibitors, also methotrexate, predisone) Thrombotic microangiopathy GVHD (acute) Imaging (contrast agents) Obstruction: extra-renal (hemorrhagic cystitis, fungal ball), intratubular (crystals, drug etc) Renal vein thrombosis
Later post HCT
GVHD (chronic); immune dysregulation Thrombotic microangiopathy Drugs Anti-microbial (treatment/prophylaxis) Anti-GVHD (immunosuppression for treatment/prophylaxis, esp. calcineurin-inhibitors, also methotrexate, predisone) Treatment of side effects (eg. Biphosphonates for treatment of bone loss; hypoglycemics for diabetes) Infections, esp. viral, fungal Obstruction from retroperitoneal fibrosis, lymphadenopathy Recurrence Post-transplant lymphoproliferative disorder; second malignancies (hematopoietic, RCC)
Compiled from Parikh, Singh, Sawinski and others

Table 3: Incidence and risk factors for chronic kidney disease after hematopoietic cell transplant: selected studies, odds ratios Risk factor Ellis (meta
analysis) Weiss
(N=122) Ando
(N=158) Al-Hazzouri
(N=221) Choi
(N=1190) Hingorani (N=1635)
Saddadi (N=1693)
% Chronic Kidney Disease
66% 17% 27% 4.4% 23% 4%
Acute Kidney Injury
2.57 32.8 9.9 4.0 1.7
Calcineurin inhibitor (Long term)
2.3 3.7 2.1 3.5 1.2-2.8
Graft versus Host Disease
1.75 (chronic) 4.2 1.2-1.7 2.01 (acute) 1.6 1.8-2.0 2.9
Total Body Irradiation
2.56 (>11 Gy) All had 2 Gy 2.3 All had TBI 0.9 1.1 (any) None had TBI
Allogeneic (vs autologous)
All Allo Allo Allo 2.70 MUD 2.5 3.4
Ablative (vs Reduced Intensity Conditioning)
All RIC All Ablative 1.5 1.3
Definitions of CKD and other parameters vary by study; see primary references for details

Table 4: Meta-analysis of published renal biopsy findings in hematopoietic cell transplantation Primary biopsy diagnosis (of 225 published)
Number published Recipient male sex
Radiation Type of cells Chronic GVHD at proteinuria onset
Onset (post-HCT months) Creatinine (mg/dL) Proteinuria (g/day) As Average (range)
Membranous Nephropathy
80 (36% of all) (57% of GN)
51/71 (72%) 19/48 (40%) Allo-BMT 37/54 (69%) Allo-PBSCT 15/54 (27%) Autologous 2/54 ( 4%)
48/62 (77%) Onset: 23.2 (3-134) Cr: 1.2 (0.6-4.1) Pr: 10.9 (1.1-35)
Minimal Change Disease
27 (12% of all) (19% of GN)
9/21 (43%) 7/15 (47%) Allo-BMT 8/19 (42%) Allo-PBSCT 8/19 (42%) Allo-UBSCT 2/19 (11%) Autologous 1/19 ( 5%)
13/20 (65%) Onset:20 (3-105) Cr: 2.1 (0.9-3.5) Pr: 12.6 (2.5-19.9)
Other Glomerular
12-FSGS 1-collapsing 5-IgA 3-MPGN 6-Mesangial Prolif 5-Crescent 1-Immune complex
8/10 FSGS 4/6 FSGS Allo-BMT 6/9 FSGS Allo-PBSCT 3/9 FSGS
FSGS Onset: 52.5 (2-228) Cr: 2.0 (0.8-2.7) Pr: 9.6 (2.4-25)
Thrombotic Microangio-pathy
47 (21% of all) 15/28 (58%) 30/34 (88%) Allo-BMT 10/37 (27%) Allo-PBSCT 9/37 (24%) Allo-UBSCT 2/37 ( 5%) Autologous 16/37 (43%)
Onset:16.8 (0.25-93) Cr: 2.2 (1-6) Pr: 1.6 (0-11.3)
Viral 11-Polyoma 3-Adenovirus
3/9 (33%) Polyoma Onset: 25.2 (3-56) Cr: 2.9 (1.7-4.4)
ATN/AIN 21 (9% of all) 1- anti-TBM
9/11 (82%) 5/6 (83%) Allo-PBSCT 2/5 Allo-UBSCT 1/5 Autologous 2/5
Onset: 5.5 (1-10) Cr: 4.6 (2.2-9.2)
CIN/HTN 3 (1% of all)

The above reflects primary pathology and does not include multiple biopsy diagnoses/lesions, or autopsy cases. Table 5 expanded from Hu too include: Akar; Ansari; Antignac; Brinkerhoff; Brukamp; Bruno; Butcher; Forslund; Fraile-Pilar; Glezerman; Goodwin; Haysom; Homma; Huang; Huskey; Ikegame; Imai; Jodele 2013; Kim; Laskin 2013; Limaye; Luo; Maeda; Mii; O’donnell; Olivera; Oyama; Petropoulou; Schwarz; Stracke; Verghese; Wang Anti-TBM: anti-tubular basement membrane BMT: Bone marrow transplant (marrow source of cells) Crescent: includes 2 ANCA-associated cases; 1 anti-glomerular basement membrane FSGS: focal segmental glomerulosclerosis MPGN: Membranoproliferative glomerulonephritis PBSCT: peripheral blood stem cell transplant UBSCT: umbilical cord stem cell transplant

Table 5. Chronic, tubular and vascular kidney lesions reported in HCT recipients Parameter El-Seisi ‘03
(Nova Scotia, N=26, autopsy)
Chang ’07 (U Washington,
n=20)
Terrier ’07 (France, n=5
all MN)
Schwarz ‘10 (Hannover n=14)
Mii ’11 (Japan, n=7,
all TMA)
Brinkerhoff ’14 + Troxell ’08
(Stanford, OHSU n=29)
Global glomerulosclerosis
73% (Any) 60% (any) Avg/bx 13%
14% (Any) 100% (Any) Avg/bx 11%
75% (Any) Avg/bx 20%
Interstitial fibrosis/ tubular atrophy
54% (Any) 65% (Any) 40% (Diffuse)
100% (Any) 40% (diffuse)
50% (>=20%) 57% (>25%) 63% (>=20%) Avg/bx 30%
Acute tubular necrosis
31% “ tubular cell degenerate”
30% 79% 45%
Arteriolar hyaline 46% 10% 100% 48% Calcification 69% 14%

References
Abboud I, Peraldi MN, Hingorani S. Chronic kidney diseases in long-term survivors after allogeneic hematopoietic stem cell transplantation: monitoring and management guidelines. Semin Hematol. 2012;49:73-82.
Akar H, Keven K, Celebi H, et al. Nephrotic syndrome after allogeneic peripheral blood stem cell transplantation. J Nephrol. 2002 Jan-Feb;15(1):79-82.
Ando M, Ohashi K, Akiyama H, et al. Chronic kidney disease in long-term survivors of myeloablative allogeneic haematopoietic cell transplantation: prevalence and risk factors. Nephrol Dial Transplant. 2010;25:278-82.
Al-Hazzouri A, Cao Q, Burns LJ, et al. Similar risks for chronic kidney disease in long-term survivors of myeloablative and reduced-intensity allogeneic hematopoietic cell transplantation. Biol Blood Marrow Transplant. 2008;14:658-63.
Ansari M, Vukicevic M, Rougemont AL, et al. Do NK cells contribute to the pathophysiology of transplant-associated thrombotic microangiopathy? Am J Transplant. 2011;11:1748-52.
Antignac C, Gubler MC, Leverger G, et al. Delayed renal failure with extensive mesangiolysis followingbone marrow transplantation. Kidney Int. 1989;35:1336–44.
Ariza-Heredia EJ, Nesher L, Chemaly RF. Cytomegalovirus diseases after hematopoietic stem cell transplantation: a mini-review. Cancer Lett. 2014;342:1-8.
Baird K, Pavletic SZ. Chronic graft versus host disease. Curr Opin Hematol. 2006;13:426-35. Beck LH Jr, Bonegio RG, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen
in idiopathic membranous nephropathy. N Engl J Med. 2009 Jul 2;361(1):11-21. Blazar BR, Murphy WJ, Abedi M. Advances in graft-versus-host disease biology and therapy. Nat
Rev Immunol. 2012;12:443-58. Brinkerhoff B, Houghton, DC, Troxell ML. Spectrum of Renal Pathology Findings in
Hematopoietic Cell Transplant Patients. USCAP 2014 Abstract #1668. Bruijn JA, van Elven EH, Hogendoorn PC, et al. Murine chronic graft-versus-host disease as a
model for lupus nephritis. Am J Pathol. 1988;130:639-41. Brukamp K, Doyle AM, Bloom RD, et al. Nephrotic syndrome after hematopoietic cell
transplantation: do glomerular lesions represent renal graft-versus-host disease? Clin J Am Soc Nephrol. 2006;1:685-94.
Bruno B, Zager RA, Boeckh MJ, et al. Adenovirus nephritis in hematopoietic stem-cell transplantation. Transplantation. 2004;77:1049.
Butcher JA, Hariharan S, Adams MB, et al.Renal transplantation for end-stage renal disease following bone marrow transplantation: a report of six cases, with and without immunosuppression. Clin Transplant. 1999;13:330-5.
Carpenter PA. Late effects of chronic graft-versus-host disease. Best Pract Res Clin Haematol. 2008;21:309-31.
Chan GS, Lam MF, Au WY, et al. Clinicopathologic analysis of renal biopsies after haematopoietic stem cell transplantation. Nephrology (Carlton). 2008;13:322-30.
Chang A, Hingorani S, Kowalewska J, et al. Spectrum of renal pathology in hematopoietic cell transplantation: a series of 20 patients and review of the literature. Clin J Am Soc Nephrol. 2007;2:1014-23.
Changsirikulchai S, Myerson D, Guthrie KA, et al. Renal thrombotic microangiopathy after hematopoietic cell transplant: role of GVHD in pathogenesis. Clin J Am Soc Nephrol. 2009;4:345-53.
Clajus C, Hanke N, Gottlieb J, et al. Renal comorbidity after solid organ and stem cell transplantation. Am J Transplant. 2012;12:1691-9.
Choi M, Sun C-L, Kurian S, et al. Incidence and predictors of delayed chronic kidney disease in long-term survivors of hematopoietic cell transplantation. Cancer. 2008;113:1580–7.
Cohen EP, Drobyski WR, Moulder JE. Significant increase in end-stage renal disease after hematopoietic stem cell transplantation. Bone Marrow Transplant. 2007 May;39(9):571-2.
Colvin RB, Nickeleit V. Renal Transplant Pathology. In: Jennette JC, Olson JL, Schwartz MM, Silva FG. Heptinstall’s Pathology of the Kidney. Philadelphia:Lippincott Williams & Wilkins, 2007: 1441-9.
Copelan EA. Hematopoietic stem-cell transplantation. N Engl J Med. 2006;354:1813-26.

Cutler C, Henry NL, Magee C, et al. Sirolimus and thrombotic microangiopathy after allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11:551-7.
Cutler C, Antin JH. Chronic graft-versus-host disease. Curr Opin Oncol. 2006;18:126-31. Davidson-Moncada JK, Pittaluga S, Roth M et al. Second cancers early post allogeneic transplant:
the case of 'unrestrained' malignancy? Bone Marrow Transplant. 2013;48:872-4. Dragovic D, Rosenstock JL, Wahl SJ, et al. Increasing incidence of focal segmental
glomerulosclerosis and an examination of demographic patterns. Clin Nephrol. 2005;63:1-7. Ellis MJ, Parikh CR, Inrig JK, et al. Chronic kidney disease after hematopoietic cell
transplantation: a systematic review. Am J Transplant. 2008;8:2378-90. El-Seisi S, Gupta R, Clase CM, et al. Renal pathology at autopsy in patients who died after
hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2003;9:683-8. Fajardo LF. The pathology of ionizing radiation as defined by morphologic patterns. Acta Oncol.
2005;44:13-22. Farris AB, Taheri D, Kawai T, et al. Acute renal endothelial injury during marrow recovery in a
cohort of combined kidney and bone marrow allografts. Am J Transplant. 2011;11:1464-77. Ferrara JL, Levine JE, Reddy P, et al. Graft-versus-host disease. Lancet. 2009;373:1550-61. Forslund T, Anttinen J, Hallman H, et al. Mesangial proliferative glomerulonephritis after
autologous stem cell transplantation. Am J Kidney Dis. 2006;48:314-20. Fraile P, Vazquez L, Caballero D, et al. Chronic graft-versus-host disease of the kidney in patients
with allogenic hematopoietic stem cell transplant. Eur J Haematol. 2013;91:129-34. Garnett C, Apperley JF, Pavlů J. Treatment and management of graft-versus-host disease:
improving response and survival. Ther Adv Hematol. 2013;4:366-378. Gajewski JL, Ippoliti C, Ma Y, et al. Blood and Marrow Transplantation. In: Snyder E (ed).
Rossi’s Principles of Transfusion Medicine, Philadelphia: Lippencott Williams & Wilkins, 2002: Chapter 38.
Glezerman IG, Jhaveri KD, Watson TH, et al.Chronic kidney disease, thrombotic microangiopathy, and hypertension following T cell-depleted hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2010;16:976-84.
Goodwin JE, Palmer M, Pashankar F, et al. A 7-year-old boy with renal insufficiency and proteinuria after stem cell transplant for T-cell acute lymphoblastic leukemia. Clin Nephrol. 2013 Feb 8. [Epub ahead of print] PMID: 23391318
Hamawi K, De Magalhaes-Silverman M, Bertolatus JA. Outcomes of renal transplantation following bone marrow transplantation. Am J Transplant. 2003 Mar;3(3):301-5.
Haysom L, Ziegler DS, Cohn RJ, et al. Retinoic acid may increase the risk of bone marrow transplant nephropathy. Pediatr Nephrol. 2005;20:534-8. Epub 2005 Feb 18.
Hingorani S. Chronic kidney disease in long-term survivors of hematopoietic cell transplantation: epidemiology, pathogenesis, and treatment. J Am Soc Nephrol. 2006;17:1995-2005.
Hingorani S. Chronic kidney disease after pediatric hematopoietic cell transplant. Biol Blood Marrow Transplant. 2008;14(1 Suppl 1):84-7. Erratum in: Biol Blood Marrow Transplant. 2008 Nov;14(11):1317-8.
Ho VT, Cutler C, Carter S, et al. Blood and marrow transplant clinical trials network toxicity committee consensus summary: thrombotic microangiopathy after hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2005;11:571-5.
Homma CI, Kami M, Masuo S, et al. Graft-versus-host disease of the kidney after rapid tapering of cyclosporin following reduced intensity hematopoietic stem cell transplantation. Bone Marrow Transplant. 2005;35:929-30.
Hu SL, Colvin GA, Rifai A, et al. Glomerulonephritis after hematopoietic cell transplantation: IgA nephropathy with increased excretion of galactose-deficient IgA1. Nephrol Dial Transplant. 2010;25:1708-13.
Hu SL. The role of graft-versus-host disease in haematopoietic cell transplantation-associated glomerular disease Nephrol Dial Transplant. 2011; 26:2025-31.
Huang X, Qin W, Zhang M, et al. Detection of Anti-PLA2R Autoantibodies and IgG Subclasses in Post-Allogeneic Hematopoietic Stem Cell Transplantation Membranous Nephropathy. Am J Med Sci. 2013;346:32–37.
Humphreys BD, Vanguri VK, Henderson J, et al. Minimal-change nephrotic syndrome in a hematopoietic stem-cell transplantat recipient. Nat Clin Pract Nephrol. 2006;2:535-9; quiz 540.

Huskey J, Rivard C, Myint H, et al. Minimal change disease in graft versus host disease: a podocyte response to the graft? Clin Nephrol. 2013 Dec;80(6):469-73.
Ikegame K, Takimoto T, Takahashi R, et al. Lethal adenovirus infection in a patient who had undergone nonmyeloablative stem cell transplantation. Int J Hematol. 2001;74:95-100.
Imai H, Oyama Y, Miura AB, et al. Hematopoietic cell transplantation-related nephropathy in Japan. Am J Kidney Dis. 2000;36:474-80.
Jodele S, Licht C, Goebel J, et al. Abnormalities in the alternative pathway of complement in children with hematopoietic stem cell transplant-associated thrombotic microangiopathy. Blood. 2013;122:2003-7.
Jodele S, Fukuda T, Vinks A, et al. Eculizumab therapy in children with severe hematopoietic stem cell transplantation-associated thrombotic microangiopathy. Biol Blood Marrow Transplant. 2013 Dec 23. pii: S1083-8791(13)01162-2. doi: 10.1016/j.bbmt.2013.12.565. [Epub ahead of print]
Johnston L. Acute graft-versus-host disease: differing risk with differing graft sources and conditioning intensity. Best Pract Res Clin Haematol. 2008;21:177-92.
Kapur R, Ebeling S, Hagenbeek A. B-cell involvement in chronic graft-versus-host disease. Haematologica. 2008;93:1702–11.
Kemper MJ, Güngör T, Halter J, et al.Favorable long-term outcome of nephrotic syndrome after allogeneic hematopoietic stem cell transplantation. Clin Nephrol. 2007;67:5-11.
Kim JY, Lee MY, Kim B, et al. Membranoproliferative glomerulonephritis following allogeneic hematopoietic stem cell transplantation. Clin Exp Nephrol. 2010;14:630-2.
Kloos RQ, Boelens JJ, de Jong TP, et al. Hemorrhagic cystitis in a cohort of pediatric transplantations: incidence, treatment, outcome, and risk factors. Biol Blood Marrow Transplant. 2013;19:1263-6.
Kimura S, Horie A, Hiki Y, et al. Nephrotic syndrome with crescent formation and massive IgA deposition following allogeneic bone marrow transplantation for natural killer cell leukemia/lymphoma. Blood. 2003;101:4219-21.
Koenecke C, Hertenstein B, Schetelig J, et al. Solid organ transplantation after allogeneic hematopoietic stem cell transplantation: a retrospective, multicenter study of the EBMT. Am J Transplant. 2010;10:1897-906.
Koskenvuo M, Dumoulin A, Lautenschlager I, et al. BK polyomavirus-associated hemorrhagic cystitis among pediatric allogeneic bone marrow transplant recipients: treatment response and evidence for nosocomial transmission. J Clin Virol. 2013;56:77-81.
Kusumi E, Kami M, Hara S, et al. Postmortem examination of the kidney in allogeneic hematopoietic stem cell transplantation recipients: possible involvement of graft-versus-host disease. Int J Hematol. 2008;87:225-30.
Laskin BL, Maisel J, Goebel J, et al. Renal Arteriolar C4d Deposition: A Novel Characteristic of Hematopoietic Stem Cell Transplantation-Associated Thrombotic Microangiopathy. Transplantation. 2013;96:217-223.
Laskin BL, Goebel J, Davies SM, et al. Small vessels, big trouble in the kidneys and beyond: hematopoietic stem cell transplantation-associated thrombotic microangiopathy. Blood. 2011;118:1452-62.
Lekakis LJ, Macrinici V, Baraboutis IG, et al. BK virus nephropathy after allogeneic stem cell transplantation: a case report and literature review. Am J Hematol. 2009;84:243-6.
Li HW, Sykes M. Emerging concepts in haematopoietic cell transplantation. Nat Rev Immunol. 2012 May 25;12(6):403-16.
Limaye AP, Smith KD, Cook L, et al. Polyomavirus nephropathy in native kidneys of non-renal transplant recipients. Am J Transplant. 2005;5:614–620.
Lin J, Markowitz GS, Nicolaides M, et al. Membranous glomerulopathy associated with graft-versus-host disease following allogeneic stem cell transplantation. Report of 2 cases and review of the literature. Am J Nephrol. 2001 Sep-Oct;21(5):351-6
Luo XD, Liu QF, Zhang Y, et al. Nephrotic syndrome after allogeneic hematopoietic stem cell transplantation: etiology and pathogenesis. Blood Cells Mol Dis. 2011;46:182-7.
Maeda K, Suzuki K, Mizutani M, et al. A case of chronic kidney disease with thrombotic microangiopathy in a hematopoietic stem cell transplant recipient. Clin Exp Nephrol. 2010;14:474-8
Mii A, Shimizu A, Masuda Y, et al. Renal thrombotic microangiopathy associated with chronic humoral graft versus host disease after hematopoietic stem cell transplantation. Pathol Int. 2011;61:34-41.

Mii A, Shimizu A, Kaneko T, et al. Renal thrombotic microangiopathy associated with chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Pathol Int. 2011;61:518-27.
Miklos DB, Kim HT, Miller KH, et al. Antibody responses to H-Y minor histocompatibility antigens correlate with chronic graft-versus-host disease and disease remission. Blood. 2005;105:2973-8
Niscola P, Tendas A, Luo XD, et al. The management of membranous glomerulopathy in allogeneic stem cells transplantation: updated literature. Cardiovasc Hematol Agents Med Chem. 2013;11:67-76.
Noël C, Hazzan M, Noël-Walter MP, et al. Renal failure and bone marrow transplantation. Nephrol Dial Transplant. 1998;13:2464-6.
Nouri-Majelan N, Sanadgol H, Ghafari A, et al. Antineutrophil cytoplasmic antibody-associated glomerulonephritis in chronic graft-versus-host disease after allogenic hematopoietic stem cell transplantation. Transplant Proc. 2005;37:3213-5.
Onuigbo M, Haririan A, Ramos E, et al.Cytomegalovirus-induced glomerular vasculopathy in renal allografts: a report of two cases. Am J Transplant. 2002;2:684-8.
O'Donnell PH, Swanson K, Josephson MA, et al.BK virus infection is associated with hematuria and renal impairment in recipients of allogeneic hematopoetic stem cell transplants. Biol Blood Marrow Transplant. 2009;15:1038-1048.
Opelz G, Döhler B. Lymphomas after solid organ transplantation: a collaborative transplant study report. Am J Transplant. 2004;4:222-30.
Oyama Y, Komatsda A, Imai H, et al. Late onset bone marrow transplant nephropathy. Intern Med. 1996;35:489–93.
Parikh CR, Schrier RW, Storer B, et al. Comparison of ARF after myeloablative and nonmyeloablative hematopoietic cell transplantation. Am J Kidney Dis. 2005;45:502-9.
Parikh CR, Coca SG. Acute renal failure in hematopoietic cell transplantation. Kidney Int. 2006;69:430-5.
Pasquini MC, Wang Z. Current use and outcome of hematopoietic stem cell transplantation: CIBMTR Summary Slides, 2012. Available at: http://www.cibmtr.org
Peffault de Latour R, Xhaard A, Fremeaux-Bacchi V, et al. Successful use of eculizumab in a patient with post-transplant thrombotic microangiopathy. Br J Haematol. 2013;161:279-280.
Perrotta S, Conte ML, La Manna A, et al. Membranous glomerulopathy in children given allogeneic hematopoietic stem cell transplantation. Haematologica. 2005;90 Suppl:ECR31.
Petropoulou AD, Robin M, Rocha V, et al. Nephrotic syndrome associated with graft rejection after unrelated double cord blood transplantation. Transplantation. 2010 Oct 15;90(7):801-2.
Rane S, Nada R, Minz M, et al. Spectrum of cytomegalovirus-induced renal pathology in renal allograft recipients. Transplant Proc. 2012;44:713-6.
Reddy P, Johnson K, Uberti JP, et al. Nephrotic syndrome associated with chronic graft-versus-host disease after allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplant. 2006;38:351-7.
Rosenthal J, Pawlowska A, Bolotin E, et al. Transplant-associated thrombotic microangiopathy in pediatric patients treated with sirolimus and tacrolimus. Pediatr Blood Cancer. 2011;57:142-6.
Saddadi F, Hakemi M, Najafi I, et al. Chronic kidney disease after hematopoietic cell transplantation: frequency, risk factors, and outcomes. Transplant Proc. 2009;41:2895-7.
Sakarcan A, Neuberg RW, McRedmond KP, et al. Membranoproliferative glomerulonephritis develops in a child with autologous stem cell transplant. Am J Kidney Dis. 2002;40:E19.
Sawinski D. The kidney effects of hematopoietic stem cell transplantation. Adv Chronic Kidney Dis. 2014;21:96-105.
Schrier RW, Parikh CR. Comparison of renal injury in myeloablative autologous, myeloablative allogeneic and non-myeloablative allogeneic haematopoietic cell transplantation. Nephrol Dial Transplant. 2005;20:678-83.
Schwarz A, Haller H, Schmitt R Biopsy-diagnosed renal disease in patients after transplantation of other organs and tissues. Am J Transplant. 2010;10:2017-25.
Seconi J, V Watt V, Ritchie DS. Nephrotic syndrome following allogeneic stem cell transplantation associated with increased production of TNF-alpha and interferon-gamma
by donor T cells. Bone Marrow Transplant. 2003;32:447–450.

Shapiro S, Robin M, Espe´rou H, et al. Polyomavirus nephropathy in the native kidneys of an unrelated cord blood transplant recipient followed by a disseminated polyomavirus infection. Transplantation. 2006;82: 292–293.
Shayani S, Palmer J, Stiller T, et al. Thrombotic microangiopathy associated with sirolimus level after allogeneic hematopoietic cell transplantation with tacrolimus/sirolimus-based graft-versus-host disease prophylaxis. Biol Blood Marrow Transplant. 2013;19:298-304.
Siami K, Kojouri K, Swisher KK, et al. Thrombotic microangiopathy after allogeneic hematopoietic stem cell transplantation: an autopsy study. Transplantation. 2008;85:22-8.
Singh N, McNeely J, Parikh S, et al. Kidney complications of hematopoietic stem cell transplantation. Am J Kidney Dis. 2013;61:809-21.
Socié G. Graft-versus-host disease--from the bench to the bedside? N Engl J Med. 2005;353:1396-7
Socié G, Blazar BR. Acute graft-versus-host disease: from the bench to the bedside. Blood. 2009;114:4327-36. Socié G. Chronic GVHD: B cells come of age. Blood. 2011;117:2086-7.
Socié G, Rizzo JD. Second solid tumors: screening and management guidelines in long-term survivors after allogeneic stem cell transplantation. Semin Hematol. 2012 Jan;49(1):4-9.
Spitzer TR. Engraftment syndrome following hematopoetic stem cell transplantation. Bone Marrow Transplant. 2001;27:893-8.
Srinivasan R, Balow JE, Sabnis S, et al. Nephrotic syndrome: an under-recognised immune-mediated complication of non-myeloablative allogeneic haematopoietic cell transplantation. Br J Haematol. 2005;131:74-9.
Stanescu HC, Arcos-Burgos M, Medlar A, et al. Risk HLA-DQA1 and PLA(2)R1 alleles in idiopathic membranous nephropathy. N Engl J Med. 2011;364:616-26.
Stevenson WS, Nankivell BJ, Hertzberg MS. Nephrotic syndrome after stem cell transplantation. Clin Transplant. 2005;19:141-4.
Storsley L, Gibson IW. Adenovirus interstitial nephritis and rejection in an allograft. J Am Soc Nephrol. 2011;22:1423-7.
Stracke S, Helmchen U, vonMuller L, et al. Polyoma virus-associated interstitial nephritis in a patient with acute myeloic leukaemia and peripheral blood stem cell transplantation. Nephrol Dial Transplant. 2003;18: 2431–2433.
Swaminathan S, Leung N, Lager DJ, et al. Changing incidence of glomerular disease in Olmsted County, Minnesota: a 30-year renal biopsy study. Clin J Am Soc Nephrol. 2006;1:483-7.
Swerdlow SH, Webber SA, Chadburn A et al. Post-transplant lymphoproliferative disorders. In: Swerdlow SH, Campo E, Harris NL et al. editors. WHO classification of tumours of haematopoietic and lymphoid tissues. Lyon (France): IARC Press; 2008: 345-50.
Terrier B, Delmas Y, Hummel A, et al. Post-allogeneic haematopoietic stem cell transplantation membranous nephropathy: clinical presentation, outcome and pathogenic aspects. Nephrol Dial Transplant. 2007;22:1369-76.
Thomas SE, Hutchinson RJ, DebRoy M et al. Successful renal transplantation following prior bone marrow transplantation in pediatric patients. Pediatr Transplant. 2004;8:507-12.
Toubai T, Sun Y, Reddy P. GVHD pathophysiology: is acute different from chronic? Best Pract Res Clin Haematol. 2008;21:101-17.
Troxell ML, Pilapil M, Miklos DB, et al.Renal pathology in hematopoietic cell transplantation recipients. Mod Pathol. 2008;21:396-406.
Tyndall A, Dazzi F. Chronic GVHD as an autoimmune disease. Best Pract Res Clin Haematol. 2008;21:281-9.
Upadhyay K, Fine RN. Solid organ transplantation following end-organ failure in recipients of hematopoietic stem cell transplantation in children. Pediatr Nephrol. 2013 Aug 16. [Epub ahead of print]
Verghese PS, Finn LS, Englund JA, et al. BK nephropathy in pediatric hematopoietic stem cell transplant recipients. Pediatr Transplant. 2009;13:913-8.
Wang HH, Yang AH, Yang LY et al. Chronic graft-versus-host disease complicated by nephrotic syndrome. J Chin Med Assoc. 2011;74:419-22.
Weiss M, Liapis H, Tomaszewsi JE et al. Pyelonephritis and other infections, reflux nephropathy, hydronephrosis, and nephrolithasis. In: Jennette JC, Olson JL, Schwartz MM, Silva FG. Heptinstall’s Pathology of the Kidney. Philadelphia:Lippincott Williams & Wilkins, 2007: 1010-26.

Weiss AS, Sandmaier BM, Storer B, et al. Chronic kidney disease following non-myeloablative hematopoietic cell transplantation. Am J Transplant. 2006;6:89-94.
Zhang C, Todorov I, Zhang Z, et al. Donor CD4+ T and B cells in transplants induce chronic graft-versus-host disease with autoimmune manifestations. Blood. 2006;107:2993-3001