Embed Size (px)
Citation preview

Acta Med Scand 200: 93-97, 1976
Reduction of Isoniazid Bioavailability in Normal Men by Concomitant Intake of Food
A. Melander, K. Danielson, A. Hanson, L. Jansson, C. Rerup, B. Schersten, T. Thulin and E. WAhlin
From the Departments of Pharmacology (Division of Clinical Pharmacology) and Clinical ChemiNry (Division of Toxicology), University of Lund,
Malmo General Hospital, Malmo, and the Unit for Community Care Sciences, Dalby, Sweden
ABSTRACT. The influence of food intake on the bio- availability of isoniazid (INH) has been examined in nine healthy male volunteers. INH was administered as a single oral dose, both in fasting state and to- gether with a standardized breakfast. Numerous ve- nous blood samples were obtained 5 min-6 hours after the INH ingestion, and the concentrations of un- metabolized INH in serum were assessed by spectro- photometry. The observations indicate that both the peak concentration and the total amount of INH ab- sorbed are greatly reduced when the drug is ingested together with food. Hence it is recommended that, in the treatment of tuberculosis with INH, the drug should be given on an empty stomach. The data may also have some bearing on the use of INH for assess- ing acetylation rates and estimating dosages of hydralazine and related drugs.
Among patients and physicians alike, a common question regarding oral administration of drugs is whether the tablet(s) should be taken on an empty stomach or together with food. This question often remains unanswered, as information about the in- fluence of food intake on the gastrointestinal ab- sorption of drugs is available only exceptionally. In an effort to obtain such information, we have stud- ied the bioavailability of different drugs after single- dose administration both on a fasting stomach and together with a standardized meal.
Isoniazid (INH) was included in the studies for several reasons. In addition to the fact that diges- tion-induced changes in gastric emptying and gas- trointestinal motility and blood flow might alter the absorbed quantity of many drugs, INH is a highly
reactive compound which may be easily affected both by various food components and by food- induced changes in the gastrointestinal acid-base balance. Indeed, antacid drugs have been shown to reduce the absorption of INH (3). Nevertheless, it is recommended, at least in this country, that in the treatment of tuberculosis the single daily dose of INH should be taken together with a meal. Apart from its use as a tuberculostatic drug, INH is in- creasingly employed as a test substance in the phenotyping of acetylation capacity, but there is no general agreement as to whether in this test the drug should be taken before or together with the breakfast.
The present study indicates that both the peak concentration and the total amount of INH ab- sorbed are greatly reduced when the drug is in- gested together with food. Thus, in the treatment of tuberculosis with INH, the drug should be given on an empty stomach. The data may also have some bearing on the use of INH for assessing acetyla- tion rates and estimating dosages of hydralazine and related drugs.
MATERIAL AND METHODS Nine clinically healthy male volunteers, aged 28-35, weight range 67-77 kg, served as test subjects. Liver func- tion, as judged by assessments of transaminase and bili- rubin levels in blood, was normal in all. After total absten- tion from food and liquid for ten hours (9 p.m. -7 am. ) , a polyethene cannula was inserted into an antebrachial vein, and 10 ml of blood was collected (0 value-blank). Thereafter, INH-100 mg/lO kg b.wt. (100 mg tablets, all of the same brand and batch, Tibinidea, Ferrosan,
Acta Med Scand 200

94 A . Melander et al.
Table I . Estimates of kinetic parameters of INH in nine healthy male volunteers given a single oral dose on an empty stomach and together with a standardized breakfast t,,,=estimated time of peak concentration, k,=influx (absorption) constant, k,=elimination constant, th=elimina- tion half-life. AUC=serum concentration curve area
Observed Observed Mean absorption Absorption peak con- Empirical con-
Subj. delay half-life centration AUC centra- no. (min) tmax(min) k l (min) ( d m l ) k , tt(min) 1360 tion
Fasting I 15 2 10 3 5 4 50 5 20 6 10 7 30 8 40 9 5
90 30 30 80 90 45 50 90 15
0.01191 0.14991 0.12276 0.091 12 0.02603 0.07773 0.21740 0.05899 0.00352
Non-fasting 1 10 90 0.01673 2 35 110 0.02044 3 25 90 0.02668 4 25 I10 0.02109 5 40 120 0.01819 6 6 0 150 0.01940 7 10 100 0.02675 8 40 105 0.04693 9 15 115 0.02358 Satistical significance of difference (paired observations) between fasting and non-fasting conditions N.S.
58 5 6 8
27 9 3
12 2
41 34 26 33 38 36 41 15 29
7.1 0.01464 12.6 0.008942 14.0 0.007720 8.8 0.007392 8.5 0.006752 8.6 0.006404
12.7 0.002985 12.3 0.00372 1 45.8 0.003523
4.4 0.009054 3.8 0.0081 10 3.4 0.007841 3.9 0.005704 3.1 0.008139 2.5 0.005605 3.4 0.003257 5.9 0.002636 8.9 0.003016
p<O.001 N.S.
47 78 89 94
103 108 232 186 197
76 85 88
122 85
124 215 263 230
N.S.
I206 1251 1376 I 242 1 307 1 560 2 735 2 314 4 070
823 710 698 823 575 538
1 873 1 365 2 295
p<o.001
3.50 3.57 3.89 4.01 3.84 4.46 8.29 7.23
11.50
2.33 2. I9 2.08 2.46 1.80 1.79 5.35 4.27 6.65
p<o.001
Malmo, Swedenbwas ingested either together with 100 ml of drinking water or immediately after a standard- ized breakfast. The breakfast, prepared by a dietician, was composed of 150 ml low-fat milk, 100 ml orange juice, 1 egg, 2 pieces of crisp bread, 5 g margarine, 20 g orange marmalade, and 20 g cheese. This equaled 20 g (20%) protein, 17 g (35%) fat, and 50 g (45%) carbo- hydrates and a total energy of 1840 kJ (440 kcal). About 100 ml non-sweetened, black coffee was included. The dietician or the nurse collecting the blood samples sur- veilled eating and intake of tablets. When the tablets were taken on an empty stomach, the subjects abstained from food and liquid for another two hours after drug adminis- tration.
Blood samples (about 10 ml) were obtained before (0 hour) and at about 5 , 10, 15, 30, 45, 60, 75, 90, 105, 120, 150, 180, 240, 300, and 360 min after drug ingestion. The exact time (adjusted to the nearest minute) of blood sampling (when the sampling tube was half-filled) was re- corded and used in calculations and graphs. Before each blood sampling, 1-2 ml blood was obtained and discarded, and after each sampling 2 4 ml0. I5 M saline was injected via the cannula. The blood samples were left at room temperature for more than one but less than two hours. They were then centrifuged, and serum was collected and frozen at -20°C till the next morning when the measure-
ment of INH concentrations was carried out. The INH assays were always performed on the day after the ex- periment, since it had been discovered that the amount of INH in a frozen standard sample changed with time. A spectrophotometric technique ( 5 ) was used to assess the levels of unmetabolized INH in serum.
The absorption and elimination of the drug were as- sumed to follow first order kinetics. Ideally, the formula for the blood concentration of INH (Y) in relation to time ( t ) would then be
where k , is the influx (absorption) constant, k2 the elimina- tion constant, and a a factor proportional to the dose (2). The constant k2 was estimated from the linear part of the semilog plot (logy vs. time). Together with t,,,, the time of peak concentration in blood, k, was used to assess k, by iterative approximation on a computer to assure a four- digit estimate. The delay in onset of full influx (absorp- tion) was judged by eye from the graphs. The trapezoidal integral of the experimental curve, Jexp, from the initial point of full influx until 360 min was determined on a computer. The integral of the blood concentration curve, Jcalc, between the initial point of full influx and 360 min,
Acta Mt-d Scand 200
Food intake: influence of INH bioavailability 95
15
5
15
5
15
5
4
I 2
1 4
I 6
2
5
6
3
I I I
6
I I 1 - a 4 6 n r
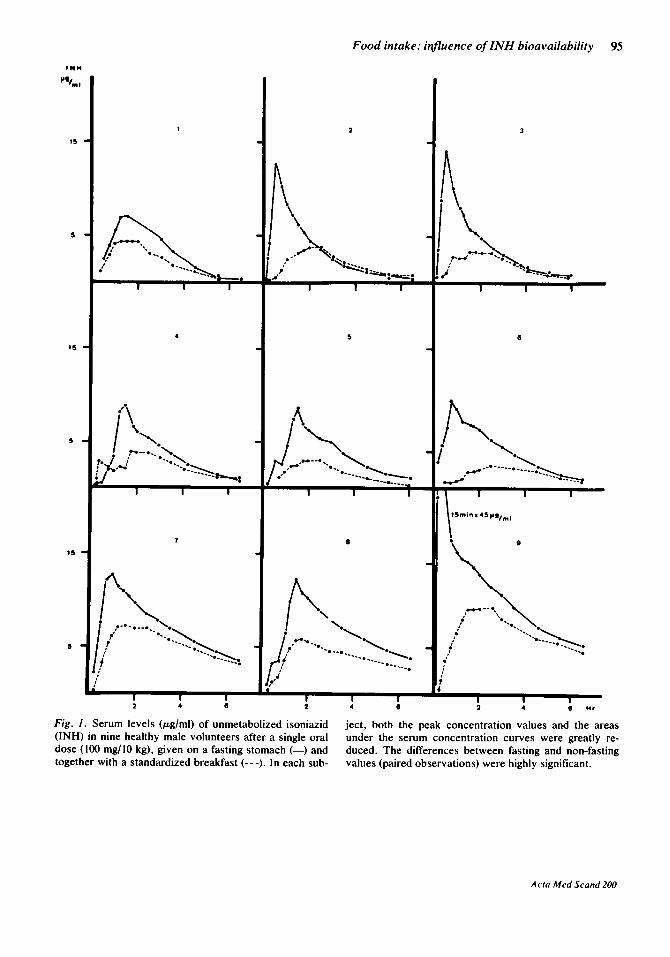
Fig. I. Serum levels (pg/ml) of unmetabolized isoniazid (INH) in nine healthy male volunteers after a single oral dose (100 mg/lO kg), given on a fasting stomach (-) and together with a standardized breakfast (---). In each sub-
ject, both the peak concentration values and the areas under the serum concentration curves were greatly re- duced. The differences between fasting and non-fasting values (paired observations) were highly significant.
Acta Med Scand 200
96 A . Melander et al.
was calculated for a = 1. Using a =Jexp/Jcalc, the curve was calculated and superimposed on the experimental graph. Dividing Jexp by (360 - initial point of full influx) yielded the mean serum level during the experiment.
Statistical differences were assessed by the 1- or the F- test on paired observations.
RESULTS It is generally agreed that the rate of INH acetyla- tion is genetically determined and that subjects can be classified as rapid or slow acetylators by estima- tion of the half-life of INH elimination from serum. According to this criterion there were three slow (t, ,*>3 hours) and six rapid (t112<2 hours) acetyla- tors (Table I, Fig. 1). Some of the latter may in fact be intermediates. From semilog-plotted curves it appeared that under fasting conditions there were both slow and rapid acetylators whose INH levels seemed to reflect a rapid distribution phase preced- ing a slower elimination phase. In most subjects, however, the elimination phase seemed to com- pletely overlap the distribution phase. Fig. 1 and Table I show also that there were great interindi- vidual differences in both the peak concentrations and the values of the areas under the sedm Cbn- centration curves (AUC), during fasting as well as non-fasting conditions.
Whether he was a rapid or a slow acetylator, each subject had lower mean serum levels of INH when the drug had been ingested after the breakfast than when it had been taken on an empty stomach. In- deed, both the peak concentrations and the AUC values were reduced in each individual (Fig. I , Table I), and both the difference between fasting and non-fasting mean peak values, mean AUC values, and mean concentration values were highly significant (Table I). In eight of the nine subjects the absorption rate was decreased when the drug was taken in the postprandial state, but this difference did not reach statistical significance (Table I).
In the postprandial curves, fewer recordings could be assumed with certainty to belong to the elimination phase, thus rendering the estimation of the elimination rate less accurate. During non-fast- ing conditions, the calculated elimination half-life was slightly prolonged in some, but slightly re- duced in some subjects. The mean values (fasting vs. non-fasting) were not significantly different (Fig. 1, Table I).
DISCUSSION A major reason for the clinical assessment of blood concentrations of drugs is the assumption that the blood level is related to the effective drug concen- tration at the site of drug action and hence to the therapeutic effect. For INH it has been observed that, when the drug is given in single daily doses, its therapeutic effect is best associated with the peak serum concentration, whereas its chronic toxicity appears to be related to the total amount absorbed (6).
The present study indicates that concomitant food intake strongly reduces the bioavailability of INH, as both the peak concentration, the mean con- centration, and the total amount absorbed were diminished. INH is assumed to be absorbed pri- marily from the intestine and not from the stomach (1, 4), and administration of antacids together with INH has been found to reduce its absorption, prob- ably as a consequence of delayed gastric emptying (3). Delay in gastric emptying consequent to food intake could hence be a likely explanation of the present findings, but interactions of INH and vari- ous food components may also be important. Ir- respective of the mechanism involved, the observa- tions motivate a strictly defined dosage regimen for INH in the treatment of tuberculosis, with the drug always given on an empty stomach. Moreover, the decision about dose size should be based on assess- ments of single-dose kinetics of INH. When only in- formation on the rate of acetylation is needed, fast- ing conditions are not mandatory but preferable.
Indeed, the great interindividual differences in INH levels recorded even within the rapid and slow acetylator subgroups suggest that the acetylation rate as such may be an insufficient parameter for the proper adjustment of the dosage regimen for INH, hydralazine and other drugs subject to the same mode of biotransformation.
ACKNOWLEDGEMENT This investigation was supported by a grant from AB Ferrosans Jubileumsfond.
REFERENCES 1 . Barley, J. F. , Evered, D. F. & Tromon, S. M.: Trans-
port of isoniazid across rat small intestine in vitro. Biochem. Pharmacol. 21: 2660, 1972.
2. Dost, F. H.: Grundlagen der Pharmakokinetik. Thieme-Verlag, Stuttgart 1W.
Arta Med Scand 200

3. Hurwitz, A. & Schlozman, D. L.: Effects of antacids on gastrointestinal absorption of isoniazid in rat and man. Amer. Rev. resp. Dis. 109:41, 1974.
4. Kakemi, K., Arita, T., Sezaki, H. & Takasugi, N.: Absorption and excretion of drugs. XXII. Absorption of isoniazid and its derivatives. Chem. pharm. Bull. 13:551, 1%5.
5 . Maher, J. R., Whitney, J. M., Chambers, J. S. & Sta-
Food intake: influence of INH bioavailability 97
nonis, D. J.: The quantitative determination of isoni- azid and paraaminosalicylic acid in body fluids. Amer. Rev. Tuberc. 76: 852, 1957.
6. Mitchison, D. A.: Plasma concentrations of isoniazid in the treatment of tuberculosis. In: Biological effects of drugs in relation to their plasma concentrations (ed. D. S. Davies and B. N. C. Pritchard), pp. 169- 182. Macmillan, London 1973.
7 -16298 I Acta Med Scand 200




![CONCOMITANT SYMPTOMS & REMEDIEShomoeopathybooks.com/Repertory of Concomitant Symptoms-1/Repe… · CONCOMITANT SYMPTOMS & REMEDIES :- GRAPH., KALI FACE :[ABDOMEN] : ... aconite if](https://img.dokumen.tips/doc/110x75/5aac6f627f8b9a8f498d0756/concomitant-symptoms-reme-of-concomitant-symptoms-1repeconcomitant-symptoms.jpg)
























