Embed Size (px)
Citation preview

Recreational mountain biking injuries
S A Aitken, L C Biant, Charles M Court-Brown
ABSTRACTMountain biking is increasing in popularity worldwide.The injury patterns associated with elite level andcompetitive mountain biking are known. This studyanalysed the incidence, spectrum and risk factors forinjuries sustained during recreational mountain biking.The injury rate was 1.54 injuries per 1000 bikerexposures. Men were more commonly injured thanwomen, with those aged 30e39 years at highest risk.The commonest types of injury were wounding, skeletalfracture and musculoskeletal soft tissue injury. Jointdislocations occurred more commonly in older mountainbikers. The limbs were more commonly injured than theaxial skeleton. The highest hospital admission rates wereobserved with head, neck and torso injuries. Protectivebody armour, clip-in pedals and the use of a full-suspension bicycle may confer a protective effect.
The popularity of the sport of mountain biking(MTBing) has increased steadily since its inceptionin the late 1970s, and various disciplines now exist.Cross-country MTBing achieved Olympic status atAtlanta in 1996. The development of DownhillMTBing allows participants to travel much fasteras they aim to reach the bottom of the course in theshortest possible time. Despite the use of protectiveclothing and equipmentdfor example, helmet,gloves, body armour, the risk of injury is everpresent, and there have been concerns regarding thesafety of the sport.The Forestry Commission (FC) in the United
Kingdom adopted MTBing as a key recreationalactivity in 1996 and is now responsible for managingand maintaining many of the countries MTBingcentres.1 One of the largest and most visited is Glen-tressMTBingCentre, situated in theScottishBorders.Early MTBing injury research carried out in the
United States analysed injury patterns in compet-itive mountain bikers at race meetings.2 3 A multi-centre Canadian study analysed injuries requiringTrauma Centre admission but excluded injuriesmanaged on an outpatient basis.4
Epidemiological injury data from recreationalMTBing has proven difficult to obtain. Oneprospective, single-centre study of competitive andrecreational MTBing was conducted in the UnitedKingdom almost 10 years ago.5
The aim of this study was to describe the epide-miology of acute mountain biking injuries in recrea-tional participants, usingGlentressMTBingCentre asa population base. The secondary aimwas to examinepatterns of protective clothing and equipment use.
METHODSThe study was conducted following approval fromthe local research and ethics committee, and withthe assistance of FC Scotland.
The Glentress MTBing centre in Scotland has130 900 visitors a year.1 Five medical facilities servethe local area surrounding Glentress (figure 1); threeAccident and Emergency departments (one traumacentre), one Minor Injuries Unit and the on-siteFirst Aid Station.Mountain bikers seeking medical care at one of
these five facilities, between 1st July 2007 and30th June 2008, were prospectively identified fromtriage data. Those bikers sustaining acute injury,while MTBing at Glentress, were included in thestudy. Verbal consent was gained at triage, andcontact details for each biker were recorded on thedata collection sheet. Bikers whose injuries weresustained in areas outside of Glentress were excludedfrom analysis. Bikers sustaining injuries while not inthe process of actively biking were similarlyexcluded. The first author (SA) then made contactwith each injured biker, within 2 weeks of injury.Consent was obtained for study participation. Datarelating to the accident and resultant injury(s) wererecorded. The injury type and site were classifiedaccording to the criteria outlined in table 1.FC Scotland have been monitoring visitor
numbers at Glentress MTBing centre since 1994,1
and the most up-to-date figures were made availableto the authors by the Information and StatisticsDivision at the completion of the study period. Thelatest visitor survey suggested 93% of visitorsarrived by car (with a mean of 2.4 visitors in eachvehicle). The remaining 7% travelled to Glentress bybus or bicycle.6 Demographical information anddetails of biking patterns and preferences, relating tothe study population, were gathered in two ways:1. Analysis of the latest visitor field survey of
143 bikers at Glentress in Sept 2007. This surveywas conducted by a private marketing firm, onbehalf of FC Scotland. The full results wereobtained from the FC Scotland website.6
2. Analysis of data from four additional fieldsurveys. Data were obtained from 100 mountainbikers (28% of the mean daily total) on fourseparate occasions (400 bikers in total). Theinformation was gathered by the first author(SA) over a 14-week period in 2008 and includeddetails relating to biker demographics, use ofhelmet/gloves/body armour, bicycle design,suspension type, pedal type, grade of trail usedand level of MTBing experience. Questionnaireswere completed on different days of the week,from different sites within Glentress and invarying weather conditions, in order to obtaina random population sample. A copy of thequestionnaire can be found online in appendix 1.
Statistical analysisStatistical calculations and resultant graphicalillustrations were created using Microsoft Excel
< Additional appendix 1 ispublished online only. To viewthis files please visit the journalonline (http://emj.bmj.com).
Department of Trauma andOrthopaedics, Royal InfirmaryEdinburgh, Edinburgh, UK
Correspondence toStuart A Aitken, Department ofTrauma and Orthopaedics, RoyalInfirmary Edinburgh, LittleFrance, Edinburgh EH16 4SU,UK; [email protected]
Accepted 7 March 2010Published Online First20 July 2010
274 Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from
worksheet (Microsoft Inc. 2003). Groups were compared usingchi-squared tests for non-continuous variables and two-samplet tests for continuous variables. A p value threshold of 0.05 wasused to determine significance.
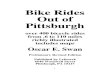
RESULTSThere were 187 000 visitors to Glentress during the study period,of which 130 900 were mountain bikers. The mean number ofbiker visits per day was 359. The results of each of the fivemountain biker surveys were similar, suggesting that a randomsample had been obtained on each occasion. The demographicaldetails of the uninjured biker sample are shown in figure 2. Menaccounted for 83% (108 647) of the MTBing population, withwomen accounting for 17% (22 253). The mean age was 32 yearsfor all bikers; 32 (10e66) years for men, 33 (11e63) years forwomen. Men aged 30e39 years represented the largest agegroup.
Two hundred and two injured mountain bikers presented toone of the five recruiting medical facilities during the 12-monthstudy period. Eighty-eight per cent (178) of injured bikers weremen, while 12% (24) were women (p¼0.12). A “biker exposure”was defined as one person MTBing at Glentress for all or anypart of a day or night. The overall injury rate was 1.54 injuriesper 1000 biker exposures. The rate was higher in men (1.64 per
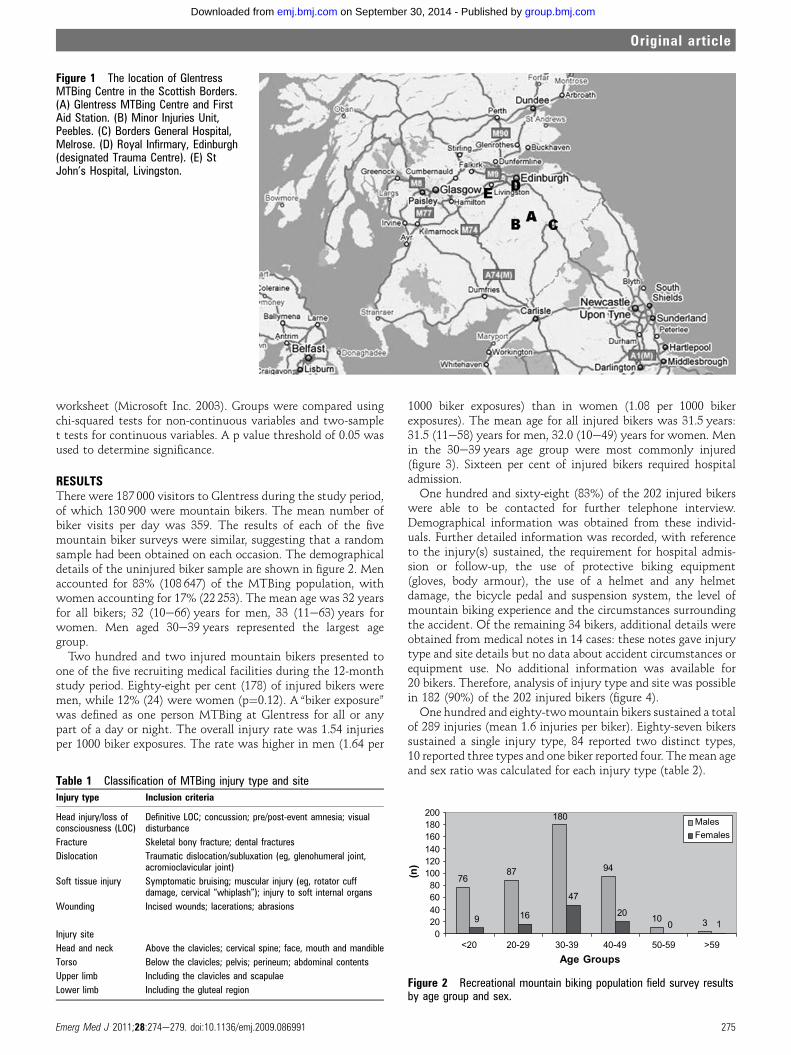
1000 biker exposures) than in women (1.08 per 1000 bikerexposures). The mean age for all injured bikers was 31.5 years:31.5 (11e58) years for men, 32.0 (10e49) years for women. Menin the 30e39 years age group were most commonly injured(figure 3). Sixteen per cent of injured bikers required hospitaladmission.One hundred and sixty-eight (83%) of the 202 injured bikers
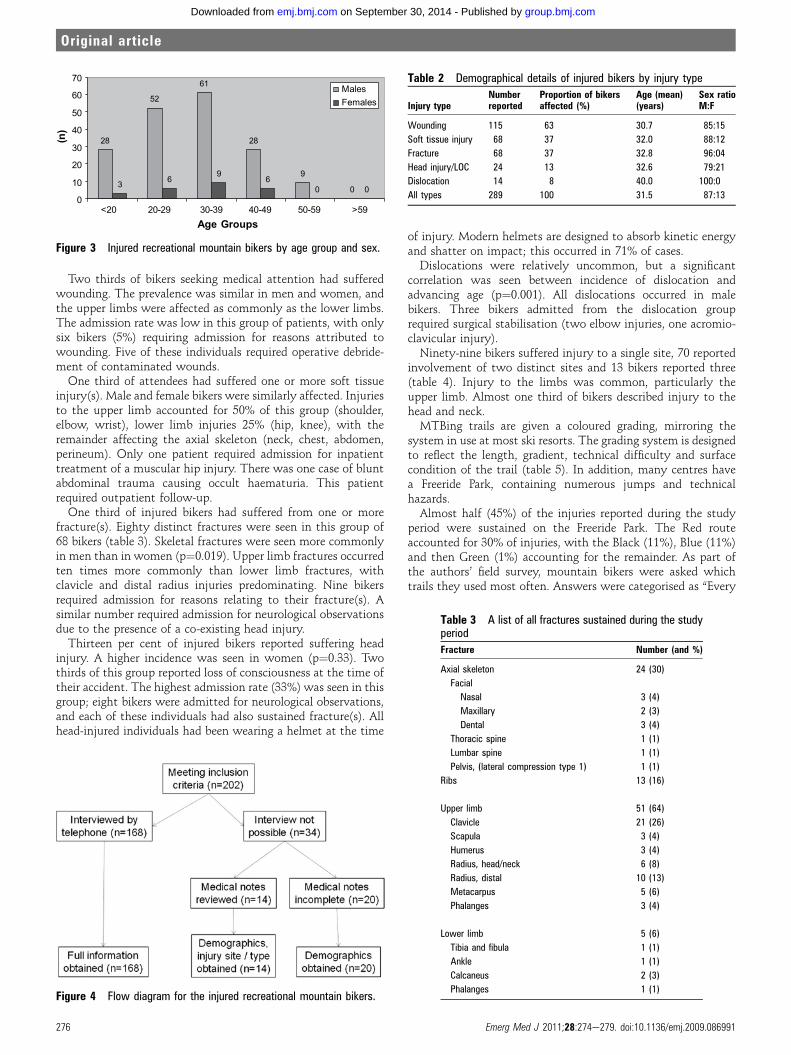
were able to be contacted for further telephone interview.Demographical information was obtained from these individ-uals. Further detailed information was recorded, with referenceto the injury(s) sustained, the requirement for hospital admis-sion or follow-up, the use of protective biking equipment(gloves, body armour), the use of a helmet and any helmetdamage, the bicycle pedal and suspension system, the level ofmountain biking experience and the circumstances surroundingthe accident. Of the remaining 34 bikers, additional details wereobtained from medical notes in 14 cases: these notes gave injurytype and site details but no data about accident circumstances orequipment use. No additional information was available for20 bikers. Therefore, analysis of injury type and site was possiblein 182 (90%) of the 202 injured bikers (figure 4).One hundred and eighty-twomountain bikers sustained a total
of 289 injuries (mean 1.6 injuries per biker). Eighty-seven bikerssustained a single injury type, 84 reported two distinct types,10 reported three types and one biker reported four. Themean ageand sex ratio was calculated for each injury type (table 2).
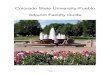
Figure 1 The location of GlentressMTBing Centre in the Scottish Borders.(A) Glentress MTBing Centre and FirstAid Station. (B) Minor Injuries Unit,Peebles. (C) Borders General Hospital,Melrose. (D) Royal Infirmary, Edinburgh(designated Trauma Centre). (E) StJohn’s Hospital, Livingston.
Table 1 Classification of MTBing injury type and site
Injury type Inclusion criteria
Head injury/loss ofconsciousness (LOC)
Definitive LOC; concussion; pre/post-event amnesia; visualdisturbance
Fracture Skeletal bony fracture; dental fractures
Dislocation Traumatic dislocation/subluxation (eg, glenohumeral joint,acromioclavicular joint)
Soft tissue injury Symptomatic bruising; muscular injury (eg, rotator cuffdamage, cervical “whiplash”); injury to soft internal organs
Wounding Incised wounds; lacerations; abrasions
Injury site
Head and neck Above the clavicles; cervical spine; face, mouth and mandible
Torso Below the clavicles; pelvis; perineum; abdominal contents
Upper limb Including the clavicles and scapulae
Lower limb Including the gluteal region
7687
180
94
10 39 16
47
200 1
020406080100120140160180200
<20 20-29 30-39 40-49 50-59 >59Age Groups
(n
)
MalesFemales
Figure 2 Recreational mountain biking population field survey resultsby age group and sex.
Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991 275
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from
Two thirds of bikers seeking medical attention had sufferedwounding. The prevalence was similar in men and women, andthe upper limbs were affected as commonly as the lower limbs.The admission rate was low in this group of patients, with onlysix bikers (5%) requiring admission for reasons attributed towounding. Five of these individuals required operative debride-ment of contaminated wounds.
One third of attendees had suffered one or more soft tissueinjury(s). Male and female bikers were similarly affected. Injuriesto the upper limb accounted for 50% of this group (shoulder,elbow, wrist), lower limb injuries 25% (hip, knee), with theremainder affecting the axial skeleton (neck, chest, abdomen,perineum). Only one patient required admission for inpatienttreatment of a muscular hip injury. There was one case of bluntabdominal trauma causing occult haematuria. This patientrequired outpatient follow-up.
One third of injured bikers had suffered from one or morefracture(s). Eighty distinct fractures were seen in this group of68 bikers (table 3). Skeletal fractures were seen more commonlyin men than in women (p¼0.019). Upper limb fractures occurredten times more commonly than lower limb fractures, withclavicle and distal radius injuries predominating. Nine bikersrequired admission for reasons relating to their fracture(s). Asimilar number required admission for neurological observationsdue to the presence of a co-existing head injury.
Thirteen per cent of injured bikers reported suffering headinjury. A higher incidence was seen in women (p¼0.33). Twothirds of this group reported loss of consciousness at the time oftheir accident. The highest admission rate (33%) was seen in thisgroup; eight bikers were admitted for neurological observations,and each of these individuals had also sustained fracture(s). Allhead-injured individuals had been wearing a helmet at the time
of injury. Modern helmets are designed to absorb kinetic energyand shatter on impact; this occurred in 71% of cases.Dislocations were relatively uncommon, but a significant
correlation was seen between incidence of dislocation andadvancing age (p¼0.001). All dislocations occurred in malebikers. Three bikers admitted from the dislocation grouprequired surgical stabilisation (two elbow injuries, one acromio-clavicular injury).Ninety-nine bikers suffered injury to a single site, 70 reported
involvement of two distinct sites and 13 bikers reported three(table 4). Injury to the limbs was common, particularly theupper limb. Almost one third of bikers described injury to thehead and neck.MTBing trails are given a coloured grading, mirroring the
system in use at most ski resorts. The grading system is designedto reflect the length, gradient, technical difficulty and surfacecondition of the trail (table 5). In addition, many centres havea Freeride Park, containing numerous jumps and technicalhazards.Almost half (45%) of the injuries reported during the study
period were sustained on the Freeride Park. The Red routeaccounted for 30% of injuries, with the Black (11%), Blue (11%)and then Green (1%) accounting for the remainder. As part ofthe authors’ field survey, mountain bikers were asked whichtrails they used most often. Answers were categorised as “Every
28
52
61
28
9
03 69
60 0
0
10
20
30
40
50
60
70
<20 20-29 30-39 40-49 50-59 >59Age Groups
(n
)
MalesFemales
Figure 3 Injured recreational mountain bikers by age group and sex.
Figure 4 Flow diagram for the injured recreational mountain bikers.
Table 2 Demographical details of injured bikers by injury type
Injury typeNumberreported
Proportion of bikersaffected (%)
Age (mean) Sex ratio(years) M:F
Wounding 115 63 30.7 85:15
Soft tissue injury 68 37 32.0 88:12
Fracture 68 37 32.8 96:04
Head injury/LOC 24 13 32.6 79:21
Dislocation 14 8 40.0 100:0
All types 289 100 31.5 87:13
Table 3 A list of all fractures sustained during the studyperiod
Fracture Number (and %)
Axial skeleton 24 (30)
Facial
Nasal 3 (4)
Maxillary 2 (3)
Dental 3 (4)
Thoracic spine 1 (1)
Lumbar spine 1 (1)
Pelvis, (lateral compression type 1) 1 (1)
Ribs 13 (16)
Upper limb 51 (64)
Clavicle 21 (26)
Scapula 3 (4)
Humerus 3 (4)
Radius, head/neck 6 (8)
Radius, distal 10 (13)
Metacarpus 5 (6)
Phalanges 3 (4)
Lower limb 5 (6)
Tibia and fibula 1 (1)
Ankle 1 (1)
Calcaneus 2 (3)
Phalanges 1 (1)
276 Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from
time”, “Usually”, “Seldom” or “Never”, and this allowed for thecalculation of injury incidence for each grade of trail (table 6).
The effect of protective equipmentHelmet usage data were available for 173 injured bikers. All butone of these individuals had been wearing a helmet at the timeof injury. Several designs of mountain bike helmet were used.The simple “Cross-Country (XC)” style helmet aims to protectthe top of the head and was used by 84%. The robust “Full Face”downhill MTBing helmet affords additional protection to theface and mandible (11%), as does the “XC with Face” variant(3%). The “Skater” style helmet falls in-between these twobroad categories; it has no face protection but covers the backand sides of the head. Despite 6% of field survey respondentsreporting use of a Skater helmet, only 1% of injured bikers werewearing this type (p¼0.03). The prevalence of different helmetdesigns was compared between those bikers who had sustaineda head injury and those who had not. No difference was seen. Ofthose individuals whose helmet had shattered, 68% reported nohead injury.
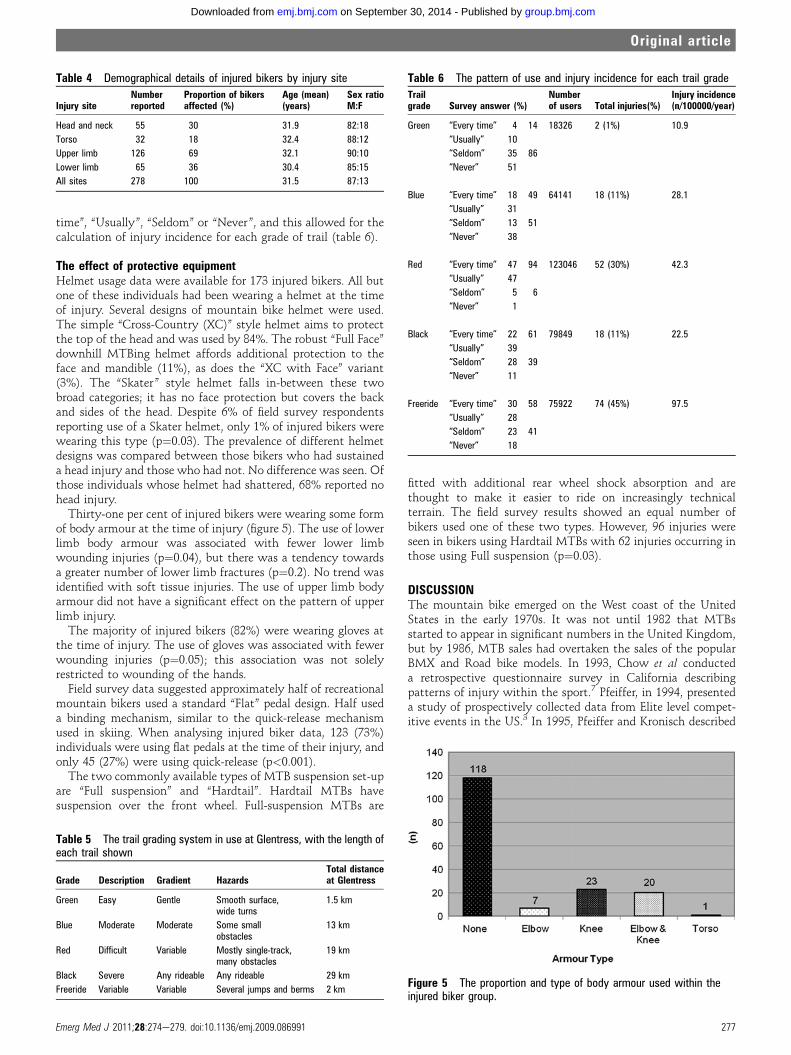
Thirty-one per cent of injured bikers were wearing some formof body armour at the time of injury (figure 5). The use of lowerlimb body armour was associated with fewer lower limbwounding injuries (p¼0.04), but there was a tendency towardsa greater number of lower limb fractures (p¼0.2). No trend wasidentified with soft tissue injuries. The use of upper limb bodyarmour did not have a significant effect on the pattern of upperlimb injury.
The majority of injured bikers (82%) were wearing gloves atthe time of injury. The use of gloves was associated with fewerwounding injuries (p¼0.05); this association was not solelyrestricted to wounding of the hands.
Field survey data suggested approximately half of recreationalmountain bikers used a standard “Flat” pedal design. Half useda binding mechanism, similar to the quick-release mechanismused in skiing. When analysing injured biker data, 123 (73%)individuals were using flat pedals at the time of their injury, andonly 45 (27%) were using quick-release (p<0.001).
The two commonly available types of MTB suspension set-upare “Full suspension” and “Hardtail”. Hardtail MTBs havesuspension over the front wheel. Full-suspension MTBs are
fitted with additional rear wheel shock absorption and arethought to make it easier to ride on increasingly technicalterrain. The field survey results showed an equal number ofbikers used one of these two types. However, 96 injuries wereseen in bikers using Hardtail MTBs with 62 injuries occurring inthose using Full suspension (p¼0.03).
DISCUSSIONThe mountain bike emerged on the West coast of the UnitedStates in the early 1970s. It was not until 1982 that MTBsstarted to appear in significant numbers in the United Kingdom,but by 1986, MTB sales had overtaken the sales of the popularBMX and Road bike models. In 1993, Chow et al conducteda retrospective questionnaire survey in California describingpatterns of injury within the sport.7 Pfeiffer, in 1994, presenteda study of prospectively collected data from Elite level compet-itive events in the US.3 In 1995, Pfeiffer and Kronisch described
Table 4 Demographical details of injured bikers by injury site
Injury siteNumberreported
Proportion of bikersaffected (%)
Age (mean)(years)
Sex ratioM:F
Head and neck 55 30 31.9 82:18
Torso 32 18 32.4 88:12
Upper limb 126 69 32.1 90:10
Lower limb 65 36 30.4 85:15
All sites 278 100 31.5 87:13
Table 5 The trail grading system in use at Glentress, with the length ofeach trail shown
Grade Description Gradient HazardsTotal distanceat Glentress
Green Easy Gentle Smooth surface,wide turns
1.5 km
Blue Moderate Moderate Some smallobstacles
13 km
Red Difficult Variable Mostly single-track,many obstacles
19 km
Black Severe Any rideable Any rideable 29 km
Freeride Variable Variable Several jumps and berms 2 km
Table 6 The pattern of use and injury incidence for each trail grade
Trailgrade Survey answer (%)
Numberof users Total injuries(%)
Injury incidence(n/100000/year)
Green “Every time” 4 14 18326 2 (1%) 10.9
“Usually” 10
“Seldom” 35 86
“Never” 51
Blue “Every time” 18 49 64141 18 (11%) 28.1
“Usually” 31
“Seldom” 13 51
“Never” 38
Red “Every time” 47 94 123046 52 (30%) 42.3
“Usually” 47
“Seldom” 5 6
“Never” 1
Black “Every time” 22 61 79849 18 (11%) 22.5
“Usually” 39
“Seldom” 28 39
“Never” 11
Freeride “Every time” 30 58 75922 74 (45%) 97.5
“Usually” 28
“Seldom” 23 41
“Never” 18
Figure 5 The proportion and type of body armour used within theinjured biker group.
Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991 277
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from

the incidence of different injury types, using predominantlyretrospective data.8 They concluded that future research shouldattempt to determine the relationships between bicycle design,terrain and safety equipment.
The first substantial prospective study of competitive bikerswas conducted by Kronisch, Pfeiffer and Chow in 1996.2 Theylooked at injury rates, types, mechanisms and severity across thetwo popular disciplines of Cross-country and DownhillMTBing. They concluded that the risk of injury is similar in eachdiscipline but uncovered a possible difference in injury patternsbetween men and women. Jeys et al conducted a study ofrecreational and competitive bikers who required Orthopaedicreferral.5 Our study has highlighted that 62% of recreationalmountain biking injuries recorded during our study period didnot require orthopaedic review. Kronisch and Chow examinedmechanisms of injury in competitive MTBing in 20029 andshowed that falling forward over the handlebars was associatedwith a greater severity of injury. The same group furtherexamined sex differences in MTB racing injuries and concludedthat the risk of injury was greater in women10; a finding that hasnot been replicated in our study of recreational bikers.
Kronisch and Pfeiffer in 2002 stated that little had beenlearned about the demographics and injury epidemiology of non-competitive mountain bikers.11 A multi-centre study fromCanada examined 10 years of mountain biking injuries.4 Like thesurvey by Jeys et al, this large study included only patientsrequiring trauma centre admission and, therefore, described themore serious injuries encountered within the sport. Quigley andBoyce reported on a prospectively collected case series of recre-ational and competitive MTBing injuries in 2005, but there wasno control group.12
Men aged 30e39 years accounted for 30% of mountain bikersin the study. As a consequence, injury was most commonly seenin this group. Men aged 20e29 years were somewhat over-represented. It may be that this group ride more aggressively andare willing to take greater risks. The overall injury rate of 1.54injuries per 1000 biker exposures suggests that recreationalmountain biking compares favourably with many other popularsports. Studies looking at indoor and outdoor soccer have foundinjury rates of between 4.0 and 18.0 injuries per 1000 playerexposures,13e15 while rates in competitive rugby union oftenexceed 100.0 per 1000 player games.16 Even the injury rate incompetitive Downhill MTBing (43.4/1000 biker hours)compares favourably with the injury rate found in competitiveBMX cycling (1190/1000 biker hours) at the peak of its popu-larity.2 17
Catastrophic head injury was not seen during the studyperiod, but 30% of bikers reported injury to the head and neckregion. This is twice the proportion reported in the earlyMTBing literature7 and is three times the amount seen in soccerinjuries.18 A reported LOC/Concussion rate of 13% (or 0.2 per1000 biker exposures) is similar to that reported by competitiveMTBing studies.2 3 When comparing this head injury rate withother popular sports, it is similar to that seen in rugby uniontraining but is 60 times less than that seen during professionalrugby union.19 A helmet usage rate of 99% within the injuredgroup suggests that recreational mountain bikers are aware ofthe risks of injury to the head and neck region. Of those whosehelmet shattered on impact, 68% suffered no head injury,suggesting that modern helmets afford the wearer goodprotection.
Despite the modest overall injury rate seen during the studyperiod, the reported prevalence of skeletal fracture in mountainbiking is higher than in soccer and rugby union and may be
similar to other road cycling disciplines.20 In contrast tocompetitive MTBing injury data,10 fractures were much morecommon in male recreational participants than in women.The high rate of helmet use among injured bikers precluded
any comparison of helmet users and non-users. The resultspresented here cannot confirm or refute any association betweenthe larger “Full face” helmet design and an increased risk ofcervical spine injury. The potentially protective effect of“Skater” helmets cannot easily be explained and warrantsfurther study.The results of this study suggest a potential protective effect
of body armour. In our cohort, lower limb armour protectedagainst lower limb wounding, but this effect was not replicatedwith upper limb armour use. The use of gloves offered additionalprotection.Despite the popularity of a flat pedal system among younger
MTBing enthusiasts, it was the quick-release system that wasassociated with fewer injuries. This may reflect the particularriding style of each group. Bikers using flat pedals are often saidto favour them in order to attempt more tricks and jumps, whilequick-release has traditionally been reserved for the cross-country enthusiast.Improvements in mountain bike design and technology have
led to more sophisticated and effective suspension systemoptions on modern frames. The results of this study demon-strated a protective effect of the full-suspension set-up, despitethis design reportedly allowing the biker to tackle steeper andmore technically demanding terrain.This study has limitations. We have had to rely on the accu-
racy of FC Scotland data when determining details on visitornumbers to mountain biking sites. The analysis of risk factors isdependent on a random sample being obtained by the fieldsurveys. While every effort was made to ensure this was the case(questioning 30% of the daily number of bikers, on four separateoccasions), it is accepted that our sample group may not beentirely representative of the population at risk as a whole.Some attendances at the named medical facilities may have beenmissed at triage, and there may have been a number of injuredindividuals attending for treatment out with the study area.Telephone interviews may introduce a further source of bias, butusing this method of data capture, we were able to achieve an83% response rate, with the information obtained directly fromthe injured bikers.This is the first large prospective study of recreational
mountain biking injury. We report clear associations betweenprotective equipment, bicycle design and the patterns of injuryencountered. Previous studies have reported a trend towardsserious and debilitating injury, but these results suggest thatrecreational MTBing compares favourably with many otherpopular sports.
Competing interests None.
Ethics approval This study was conducted with the approval of the Borders GeneralHospital Ethics Committee, Borders General Hospital, Melrose, Roxburghshire, TD6 9BS.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1. Forestry commission visitor surveys and counts. http://www.forestry.gov.uk/
forestry/infd-5pgazz (accessed 18 Aug 2009).2. Kronisch RL, Pfeiffer RP, Chow TK. Acute injuries in cross-country and downhill off-
road bicycle racing. Med Sci Sports Exerc 1999;28:1351e5.3. Pfeiffer RP. Off-road bicycle racing injuriesdThe NORBA Pro/Elite Category.
Clin Sports Med 1994;13:207e18.4. Kim PTW, Jangra D, Ritchie AH, et al. Mountain biking injuries requiring trauma
center admission: a 10-year regional trauma system experience. J Trauma2006;60:312e18.
278 Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from

5. Jeys LM, Cribb G, Toms AD, et al. Mountain biking injuries in rural England.Br J Sports Med 2001;35:197e9.
6. Forestry commission 7stanes phase 2 final report. http://www.7stanes.gov.uk/pdf/7stanesphase2finalreport.pdf (accessed 18 Aug 2009).
7. Chow TK, Bracker MD, Patrick K. Acute injuries from mountain biking. West J Med1993;159:145e8.
8. Pfeiffer RP, Kronisch RL. Off-road cycling injuries. An overview. Sports Med1995;19:311e25.
9. Chow TK, Kronisch RL. Mechanisms of injury in competitive off-road bicycling. WildEnviron Med 2002;13:27e30.
10. Kronisch RL, Pfeiffer RP, Chow TK, et al. Gender differences in acute mountain bikeracing injuries. Clin J Sport Med 2002;12:158e64.
11. Kronisch RL, Pfeiffer RP. Mountain biking injuries: an update. Sports Med2002;32:523e37.
12. Quigley MA, Boyce SH. Mountain biking injuries in south west Scotland: an analysisof injuries attending A&E [abstract]. British Association of Sport and ExerciseMedicine, 2005. Br J Sports Med 2005;40:90.
13. Agel J, Evans TA, Dick R, et al. Descriptive epidemiology of collegiate men’s soccerinjuries: National Collegiate Athletic Association Injury Surveillance System,1988e89 through 2002e2003. J Athl Train 2007;42:270e7.
14. Emery CA, Meeuwisse WH. Risk factors for injury in indoor compared with outdooradolescent soccer. Am J Sports Med 2006;34:1636e42.
15. Lindenfeld TN, Schmitt DJ, Hendy MP, et al. Incidence of injury in indoor soccer.Am J Sports Med 1994;22:364e71.
16. Bird YN, Waller AE, Marshall SW, et al. The New Zealand Rugby injury andperformance project. Br J Sports Med 1998;32:319e25.
17. Brogger-Jensen T, Hvass I, Bugge S. Injuries at the BMX cycling EuropeanChampionship, 1989. Br J Sports Med 1990;24:269e70.
18. Pickett W, Streight S, Simpson K, et al. Head injuries in youth soccer playerspresenting to the emergency department. Br J Sports Med 2005;39:226e31.
19. Kemp SP, Hudson Z, Brooks JH, et al. The epidemiology of head injuries in Englishprofessional rugby union. Clin J Sport Med 2008;18:227e34.
20. Gassner RJ, Hackl W, Tuli T, et al. Differential profile of facial injuries amongmountain bikers compared with bicyclists. J Trauma 1999;47:50e4.
If you need the latest information in emergency care then you need the
Emergency Medicine Journal. Packed with research, educational papers
and debate of all aspects of emergence medicine, the journal will make
sure you know everything you need to.
Informationin a hurry...
FOR MORE DETAILS ORTO SUBSCRIBE,VISITTHEWEBSITETODAY
emj.bmj.com
Emerg Med J 2011;28:274e279. doi:10.1136/emj.2009.086991 279
Original article
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from
doi: 10.1136/emj.2009.0869912010
2011 28: 274-279 originally published online July 20,Emerg Med J S A Aitken, L C Biant and Charles M Court-Brown Recreational mountain biking injuries
http://emj.bmj.com/content/28/4/274.full.htmlUpdated information and services can be found at:
These include:
References
http://emj.bmj.com/content/28/4/274.full.html#related-urlsArticle cited in:
http://emj.bmj.com/content/28/4/274.full.html#ref-list-1This article cites 18 articles, 6 of which can be accessed free at:
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(977 articles)Trauma � Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on September 30, 2014 - Published by emj.bmj.comDownloaded from