Embed Size (px)
Citation preview
Journal of Plastic, Reconstructive & Aesthetic Surgery (2011) 64, 671e676
Reconstruction of trochanteric pressure sores withpedicled anterolateral thigh myocutaneous flaps
Chih-Hsin Wang, Shih-Yi Chen, Ju-Peng Fu, Niann-Tzyy Dai,Shao-Liang Chen, Tim-Mo Chen, Shyi-Gen Chen*
Division of Plastic Surgery, Department of Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei,Taiwan, Republic of China
Received 26 May 2010; accepted 30 August 2010
KEYWORDSAnterolateral thigh flap;Trochanteric pressuresores;Tensor fasciae latae flap
* Corresponding author. Division of PSurgery , Tri-Service General Hospital,Road, Nei-Hu 114, Taipei, Taiwan, Re87927195; fax: þ886 2 87927194.
E-mail address: [email protected]
1748-6815/$ - see frontmatterCrownCopyrightªdoi:10.1016/j.bjps.2010.08.042
Summary Background: To provide an alternative choice for covering trochanteric pressuresores, we report on a modified pedicle anterolateral thigh (ALT) myocutaneous flap basedon the descending branch of the lateral circumflex femoral artery.Methods: From August 2007 to January 2010, 20 consecutive patients (10 men and 10 women)underwent 21 pedicled ALT myocutaneous flaps for reconstruction of trochanteric pressuresores. The flap was designed and elevated, resembling the ALT perforator flap including partof the vastus lateralis muscle but without skeletonisation of the perforators.Results: The mean age of patients was 79.4 years (range: 46e103). The mean follow-up periodwas 13.9 months (range: 3e32). The flaps were 8e21 cm long and 5e11 cm wide. All flapshealed without major complications. All donor sites were closed primarily without skin graftingand showed good aesthetic results. No recurrence was observed.Conclusions: This modified design of pedicled ALT myocutaneous flap without skeletonisationof perforators is a reliable and easily harvested flap for reconstruction of trochanteric pressuresores with limited morbidity.Crown Copyright ª 2010 Published by Elsevier Ltd on behalf of British Association of Plastic,Reconstructive and Aesthetic Surgeons. All rights reserved.
Pressure sores are common conditions with an estimatedprevalence of 3e10% among hospitalised patients, and upto 25e33% in nursing homes. The principles of treatment of
lastic Surgery, Department ofNo. 325, Sec. 2, Cheng-Kungpublic of China. Tel.: þ886 2
et.net (S.-G. Chen).
2010Publishedby Elsevier Ltd onbehalf of
pressure ulcers include control of the underlying causes,reducing pressure, friction and shear forces, correctingnutritional deficits, managing bacterial contamination,optimising local wound care and surgical reconstruction.Trochanteric pressure sores develop in patients who lie inthe lateral position, especially in those with significantflexion contracture. Kimata et al.1 first described the use ofthe anterolateral thigh (ALT) flap as a pedicled flap forperineal reconstruction. In our institute, Chen and Tzeng2
have applied the proximal pedicled ALT thigh flap in the
BritishAssociation of Plastic, Reconstructive andAesthetic Surgeons. All rights reserved.
672 C.-H. Wang et al.
reconstruction of trochanteric defects, including traumaand osteomyelitis. We found that it is a reliable andversatile flap but that the perforator dissection is tediousand time consuming. We now have modified and simplifiedthe pedicled ALT perforator flap into a myocutaneous flapfor covering trochanteric pressure sores. Myocutaneousflaps provide good blood supply and bulky padding, and areeffective in treating infected wounds. It contains thecutaneous portion of ALT and part of the vastus lateralismuscle and does not require the skeletonisation of perfo-rators. The advantage of this method is that it allows quickand easy harvesting of the ALT flap and maintains thetensor fasciae latae (TFL) as a reserve in case the pressuresore recurs.
Patients and methods
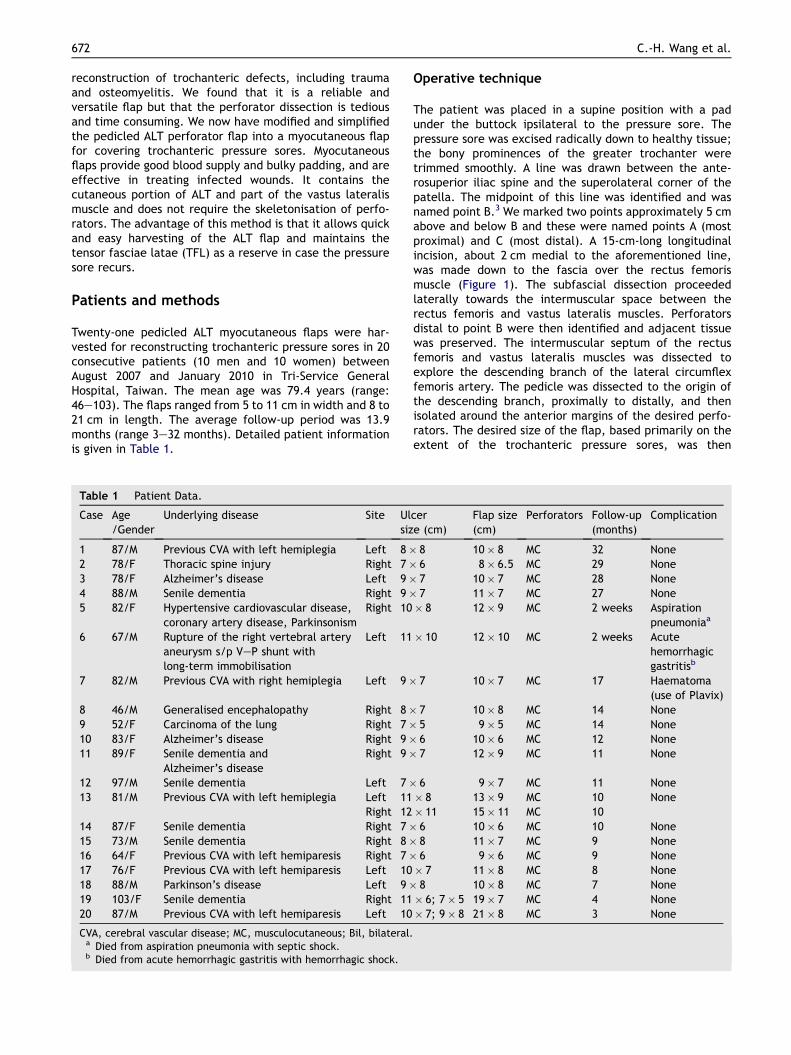
Twenty-one pedicled ALT myocutaneous flaps were har-vested for reconstructing trochanteric pressure sores in 20consecutive patients (10 men and 10 women) betweenAugust 2007 and January 2010 in Tri-Service GeneralHospital, Taiwan. The mean age was 79.4 years (range:46e103). The flaps ranged from 5 to 11 cm in width and 8 to21 cm in length. The average follow-up period was 13.9months (range 3e32 months). Detailed patient informationis given in Table 1.
Table 1 Patient Data.
Case Age/Gender
Underlying disease Site Ulsiz
1 87/M Previous CVA with left hemiplegia Left 8�2 78/F Thoracic spine injury Right 7�3 78/F Alzheimer’s disease Left 9�4 88/M Senile dementia Right 9�5 82/F Hypertensive cardiovascular disease,
coronary artery disease, ParkinsonismRight 10
6 67/M Rupture of the right vertebral arteryaneurysm s/p VeP shunt withlong-term immobilisation
Left 11
7 82/M Previous CVA with right hemiplegia Left 9�
8 46/M Generalised encephalopathy Right 8�9 52/F Carcinoma of the lung Right 7�10 83/F Alzheimer’s disease Right 9�11 89/F Senile dementia and
Alzheimer’s diseaseRight 9�
12 97/M Senile dementia Left 7�13 81/M Previous CVA with left hemiplegia Left 11
Right 1214 87/F Senile dementia Right 7�15 73/M Senile dementia Right 8�16 64/F Previous CVA with left hemiparesis Right 7�17 76/F Previous CVA with left hemiparesis Left 1018 88/M Parkinson’s disease Left 9�19 103/F Senile dementia Right 1120 87/M Previous CVA with left hemiparesis Left 10
CVA, cerebral vascular disease; MC, musculocutaneous; Bil, bilateral.a Died from aspiration pneumonia with septic shock.b Died from acute hemorrhagic gastritis with hemorrhagic shock.
Operative technique
The patient was placed in a supine position with a padunder the buttock ipsilateral to the pressure sore. Thepressure sore was excised radically down to healthy tissue;the bony prominences of the greater trochanter weretrimmed smoothly. A line was drawn between the ante-rosuperior iliac spine and the superolateral corner of thepatella. The midpoint of this line was identified and wasnamed point B.3 We marked two points approximately 5 cmabove and below B and these were named points A (mostproximal) and C (most distal). A 15-cm-long longitudinalincision, about 2 cm medial to the aforementioned line,was made down to the fascia over the rectus femorismuscle (Figure 1). The subfascial dissection proceededlaterally towards the intermuscular space between therectus femoris and vastus lateralis muscles. Perforatorsdistal to point B were then identified and adjacent tissuewas preserved. The intermuscular septum of the rectusfemoris and vastus lateralis muscles was dissected toexplore the descending branch of the lateral circumflexfemoris artery. The pedicle was dissected to the origin ofthe descending branch, proximally to distally, and thenisolated around the anterior margins of the desired perfo-rators. The desired size of the flap, based primarily on theextent of the trochanteric pressure sores, was then
cere (cm)
Flap size(cm)
Perforators Follow-up(months)
Complication
8 10� 8 MC 32 None6 8� 6.5 MC 29 None7 10� 7 MC 28 None7 11� 7 MC 27 None� 8 12� 9 MC 2 weeks Aspiration
pneumoniaa
� 10 12� 10 MC 2 weeks Acutehemorrhagicgastritisb
7 10� 7 MC 17 Haematoma(use of Plavix)
7 10� 8 MC 14 None5 9� 5 MC 14 None6 10� 6 MC 12 None7 12� 9 MC 11 None
6 9� 7 MC 11 None� 8 13� 9 MC 10 None� 11 15� 11 MC 106 10� 6 MC 10 None8 11� 7 MC 9 None6 9� 6 MC 9 None� 7 11� 8 MC 8 None8 10� 8 MC 7 None� 6; 7� 5 19� 7 MC 4 None� 7; 9� 8 21� 8 MC 3 None

Figure 1 Flap marking (Case 19) and schematic drawing offlap elevation. ASIS, anterosuperior iliac spine; P, superolateralcorner of the patella; the midpoint between ASIS and P namedpoint B; approximately 5 cm apart and named points A (mostproximal) and C (most distal); DB, descending branch of thelateral circumflex femoral artery (LCF); TB, transverse branch;AB, ascending branch; FA, femoral artery; shaded zone,designed flap area.
Reconstruction of trochanteric pressure sores 673
marked, with the perforators kept distal to point B. Theremainder of the flap was then incised. Cautery is recom-mended for flap harvest because it is time saving andcauses less bleeding and also because there is no need for
Figure 2 A. Preoperative appearance of the left trochanteric prespressure sore. C. Appearance of the left hip and aesthetically inD. Compared with the left trochanteric pressure sore, the right trocfasciae lata flap. This showed an unsightly scar with a poor flap co
intramuscular dissection of the perforators. To ensureprimary closure of the donor site and fill out the ulcerspace, the amount of vastus lateralis was harvested morethan the width of the skin paddle (Figure 3C). In our series,the flap size measured 5e11 cm in width and 8e21 cm inlength (always take at least 5 cm of muscle). The proximalcut of the muscle was about one to two proximal toperforators and the distal cut was bevelled to the distalportion of skin paddle. The flap was inset into thetrochanteric defect through a subcutaneous tunnel in thelateral thigh or via a tunnel beneath the TFL. The pediclewas laid over the vastus lateralis muscle during trans-position and a small portion of that muscle beneath thepedicle was excised, if needed, to avoid compression of thepedicle. Care was taken not to injure the ascending branchof the lateral circumflex femoris artery to preserve the TFLflap for subsequent reconstruction of any recurrence of thetrochanteric pressure sores. After adequate haemostasis,the donor site was closed primarily with a drain placement.
Results
There were one or two cutaneous perforators included inthese 21 consecutive pedicled ALT myocutaneous flaps. Allwere located distal to point B and most were adjacent topoint C. All of the perforators were musculocutaneous withsmall (<0.5 mm) vascular diameters. These perforatorswere identified and transferred with the vastus lateralismuscle without skeletonisation. The length of the pedicleranged from 12 to 16 cm according to each patient’s height,
sure sore. B. Preoperative appearance of the right trochantericconspicuous scar of the donor site 16 months after surgery.hanteric pressure sore was reconstructed with a pedicled tensorntour, and the patient could not extend the right knee.
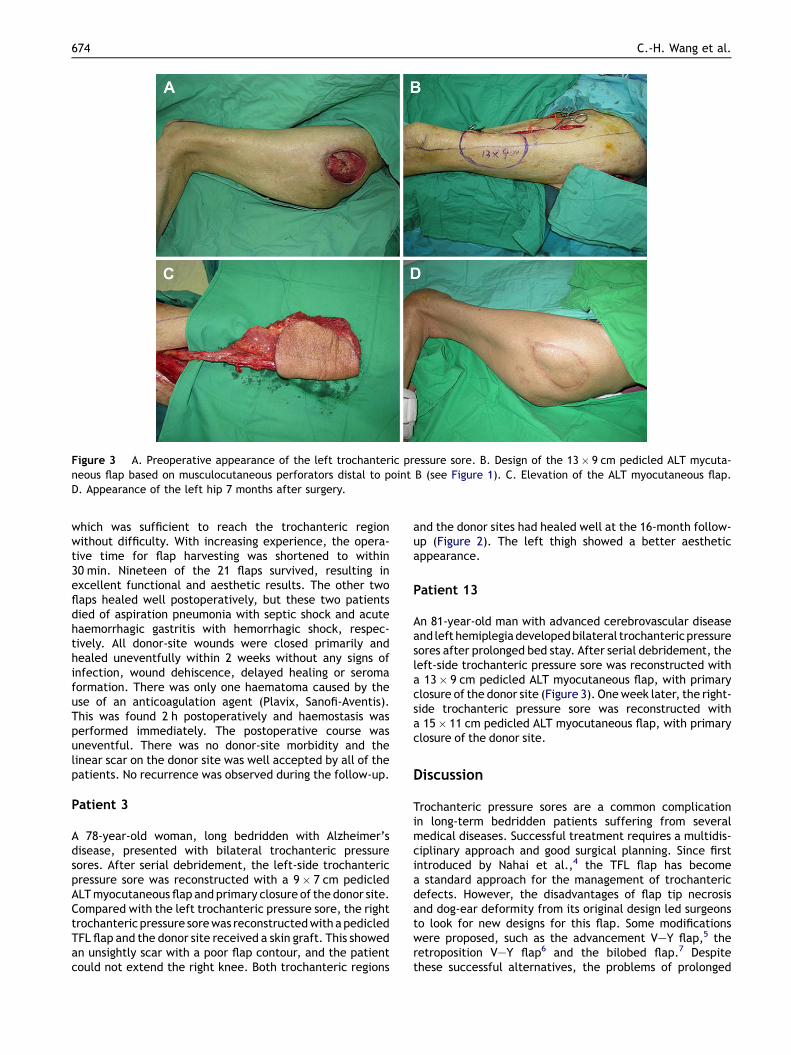
Figure 3 A. Preoperative appearance of the left trochanteric pressure sore. B. Design of the 13� 9 cm pedicled ALT mycuta-neous flap based on musculocutaneous perforators distal to point B (see Figure 1). C. Elevation of the ALT myocutaneous flap.D. Appearance of the left hip 7 months after surgery.
674 C.-H. Wang et al.
which was sufficient to reach the trochanteric regionwithout difficulty. With increasing experience, the opera-tive time for flap harvesting was shortened to within30 min. Nineteen of the 21 flaps survived, resulting inexcellent functional and aesthetic results. The other twoflaps healed well postoperatively, but these two patientsdied of aspiration pneumonia with septic shock and acutehaemorrhagic gastritis with hemorrhagic shock, respec-tively. All donor-site wounds were closed primarily andhealed uneventfully within 2 weeks without any signs ofinfection, wound dehiscence, delayed healing or seromaformation. There was only one haematoma caused by theuse of an anticoagulation agent (Plavix, Sanofi-Aventis).This was found 2 h postoperatively and haemostasis wasperformed immediately. The postoperative course wasuneventful. There was no donor-site morbidity and thelinear scar on the donor site was well accepted by all of thepatients. No recurrence was observed during the follow-up.
Patient 3
A 78-year-old woman, long bedridden with Alzheimer’sdisease, presented with bilateral trochanteric pressuresores. After serial debridement, the left-side trochantericpressure sore was reconstructed with a 9� 7 cm pedicledALTmyocutaneous flap and primary closure of the donor site.Compared with the left trochanteric pressure sore, the righttrochanteric pressure sorewas reconstructedwithapedicledTFL flap and the donor site received a skin graft. This showedan unsightly scar with a poor flap contour, and the patientcould not extend the right knee. Both trochanteric regions
and the donor sites had healed well at the 16-month follow-up (Figure 2). The left thigh showed a better aestheticappearance.
Patient 13
An 81-year-old man with advanced cerebrovascular diseaseand left hemiplegiadevelopedbilateral trochantericpressuresores after prolonged bed stay. After serial debridement, theleft-side trochanteric pressure sore was reconstructed witha 13� 9 cm pedicled ALT myocutaneous flap, with primaryclosure of the donor site (Figure 3). Oneweek later, the right-side trochanteric pressure sore was reconstructed witha 15� 11 cm pedicled ALT myocutaneous flap, with primaryclosure of the donor site.
Discussion
Trochanteric pressure sores are a common complicationin long-term bedridden patients suffering from severalmedical diseases. Successful treatment requires a multidis-ciplinary approach and good surgical planning. Since firstintroduced by Nahai et al.,4 the TFL flap has becomea standard approach for the management of trochantericdefects. However, the disadvantages of flap tip necrosisand dog-ear deformity from its original design led surgeonsto look for new designs for this flap. Some modificationswere proposed, such as the advancement VeY flap,5 theretroposition VeY flap6 and the bilobed flap.7 Despitethese successful alternatives, the problems of prolonged

Reconstruction of trochanteric pressure sores 675
operative time and unaesthetic scars remained. Recurrentrates of up to 80% have been observed with the treatmentof trochanteric pressure sores using myocutaneous flapsbased on the TFL.8
The primary consideration in the surgical treatment oftrochanteric pressure sores is the need to fill skin and soft-tissue losses, and coverage of the greater trochanter witha durable, well-perfused musculocutaneous flap. Thepedicled ALT myocutaneous flap is excellent for thispurpose. The ALT flap has been used successfully asa pedicled flap, primarily for reconstructing the groin andabdominal wall.9,10 Luo et al. successfully reconstructeda large perineal wound with a pedicled flap measuring20� 8 cm. The vastus lateralis, rectus femoris and TFLmuscles can also be combined to form compositae chimericflaps if the volume or other attributes of the muscle aredesirable.1,11 However, there are only a few reports in theliterature about the use of the ALT for reconstructing thetrochanteric region.2,12,13 We modified reported operativetechniques3,11,14 to simplify flap elevation and shorten thelearning curve among trainee surgeons. We found that thissurgical method achieves easy harvesting, obviates theneed for intramuscular dissection and offers a longerpedicle to both increase the arc of rotation and easilyachieve primary closure of the donor site.
The surgical approach was used to cover 21 trochantericpressure sores in 20 successive patients. It provided goodaesthetic coverage and durability while preserving theascending branch of the lateral circumflex femoral artery.This method preserves the conventional TFL flap ifa recurrent pressure sore should develop. In addition toa good cosmetic effect, the myocutaneous flap providesbetter vascularity and padding than does the conventionalTFL flap, and can be used to fill up potential dead space inthe trochanteric region.
Good nursing care and proper patient instruction arecritical to postoperative success. The patients are posi-tioned in such a manner to avoid pressure on the operativesite, with turning every 2 h. There was no recurrence duringthe follow-up period. The flap has a longer vascular pedicleand can reach the trochanteric region without difficulty. Itcan provide a larger skin paddle, which provides for thetension-free reconstruction of a larger trochanteric pres-sure sore compared with the TFL flap, and donor sites canbe closed primarily even if the width of the flap is morethan 8 cm.14 Kuo et al. have shown that functionalimpairment of the thigh donor site is minimal in cases inwhich a muscular part of the vastus lateralis is taken, as inthe myocutaneous flap transfer.15 Because of theseadvantages, we consider that the ALT myocutaneous flap issuitable for reconstructing trochanteric pressure sores as itprovides good coverage and durability.
Although the perforators can exhibit considerableanatomical variation, the dissection technique required forthe ALT flap has become well established. Variations occurin vascular anatomy, which include its course (muscu-locutaneous or septocutaneous) and origin (the descendingbranch of the lateral circumflex femoral or the profundafemoris artery). In reported literature,11,14,16,17 mostperforators were musculocutaneous, ranging from 74% to90% of flaps.The long vascular pedicle and lack of restric-tion to the arc of rotation are keys to the successful
transposition of the flap for reconstructing the trochantericregion. It is desirable to use the most distal one forobtaining the longest pedicle, as suggested by Kimataet al.17 Yu3 reported that the use of more distal perforatorsprovided longer pedicles, but the majority of perforatorswere musculocutaneous and small. To attain longer pedi-cles and easy, fast and safe harvesting of the flap, weintroduced a modified strategy to simplify flap elevationand shorten the learning curve among trainee surgeons(Figure 1). The flap can be raised in less than half an hourwith substantial experience, and detection of the perfora-tors using Doppler mapping might not be necessary. Weiet al.11 found the perforator to be absent in only 0.89% ofhundreds of cases in the extensive experience in Taiwan.All our patients had musculocutaneous perforators distal topoint B with small diameters (<0.5 mm) and flaps wereraised successfully in all patients.
In conclusion, our method for coverage of trochantericpressure sores offers the following advantages. It offersa longer pedicle with no restriction of the arc of rotation. Itgives easy, quick and safe surgical procedure as the tediousintramuscular dissection of the perforators for the cuta-neous skin paddle can be avoided. Most patients requiringcoverage do not, however, need the muscle function lostfrom sacrifice of a portion of the vastus lateralis muscle. Itincreases the possibility of primary closure of donor site togain an aesthetically inconspicuous curvilinear scar. Thisflap preserves the TFL flap for subsequent reconstruction ofany recurrence of trochanteric sores. This pedicled ALTmyocutaneous flap provides a large cutaneous island, withversatile applications and a reliable blood supply. It isa good alternative for covering trochanteric pressure sores.
References
1. Kimata Y, Uchiyarna K, Ebihara S, et al. Anatomic variationsand technical problems of the anterolateral thigh flap: A reportof 74 cases. Plast Reconstr Surg. 1998;102:1517e23.
2. Tzeng YS, Yu CC, Chou TD, et al. Proximal pedicled antero-lateral thigh flap for reconstruction of trochanteric defect. AnnPlast Surg 2008;61:79e82.
3. Yu P. Characteristics of the anterolateral thigh flap ina Western population and its application in head and neckreconstruction. Head Neck. 2004;26:759e69.
4. Nahai F, Silverton JS, Hill HL, et al. The tensor fasciae lataemusculocutaneous flap. Ann Plast Surg 1978;1:372e9.
5. Paletta CE, Freedman B, Shehadi SI. The V-Y tensor fasciaelatae musculocutaneous flap. Plast Reconstr Surg. 1989;83:852e7.
6. Siddiqui A, Wiedrich T, Lewis V. Tensor fasciae latae VeY ret-roposition myocutaneous flap: clinical experience. Ann PlastSurg. 1993;31:313.
7. Lynch SM. The bilobed tensor fasciae latae myocutaneous flap.Plast Reconstr Surg. 1981;67:796.
8. Evans GR, Dufresne CR, Manson PN. Surgical correction ofpressure ulcers in an urban center: is it efficacious? Adv WoundCare. 1994;7:40.
9. Luo S, Raffoul W, Piaget F, et al. Anterolateral thigh fas-ciocutaneous flap in the difficult perineogenital reconstruc-tion. Plast Reconstr Surg. 2000;105:171e3.
10. Celik N, Wei FC, Lin CH, et al. Technique and strategy inanterolateral thigh perforator flap surgery, based on an anal-ysis of 15 complete and partial failures in 439 cases. PlastReconstr Surg 2002;109:2211e6.
676 C.-H. Wang et al.
11. Wei FC, Jain V, Celik N, et al. Have we found an ideal softtissue flap? an experience with 672 anterolateral thigh flaps.Plast Reconstr Surg. 2002;109:2219e30.
12. Gravvanis AI, Tsoutsos DA, Karakitsos D, et al. Application ofthe pedicled anterolateral thigh flap to defects from the pelvisto the knee. Microsurgery 2006;26:432e8.
13. Hallock GG. The proximal pedicled anterolateral thigh flap forlower limb coverage. Ann Plast Surg. 2005;55:466e9.
14. Shieh SJ, Chiu HY, Yu JC, et al. Free anterolateral thigh flap forreconstruction of head and neck defects following cancerablation. Plast Reconstr Surg 2000;105:2349e60.
15. Kuo YR, Jeng SF, Kuo MH, et al. Free anterolateral thigh flap forextremity reconstruction: clinical experience and functionalassessment of donor site. Plast Reconstr Surg 2001;107:1766e71.
16. Wolff KD, Grundmann A. The free vastus lateralis flap: ananatomic study with case reports. Plast Reconstr Surg. 1992;89:469e75.
17. Kimata Y, Uchiyama K, Ebihara S, et al. Versatility of thefree anterolateral thigh flap for reconstruction of head andneck defects. Arch Otolaryngol Head Neck Surg 1997;123:1325e31.





























