Embed Size (px)
Citation preview
SURGICAL ONCOLOGY AND RECONSTRUCTION
Rec
De
Un
Reconstruction of Through-and-ThroughCheek Defects With Folded Free
Anterolateral Thigh Flaps
eived
partme
iversity
*Reside
yResidezAssocixAssocijjAssoc{Reside#Reside
**Profes
yyProfe
Zhi-Min Liu, MD,* Di Wu, MD,y Xue-Kui Liu, MD, PhD,z Wei-Wei Liu, MD, PhD,xHao Li, MD, PhD,jj Quan Li, MD,{ Xin-Rui Zhang, MD,# Zong-Yuan Zeng, MD,**
and Zhu-Ming Guo, MDyy
Purpose: The purpose of this study was to assess the clinical application and therapeutic efficacy ofthrough-and-through cheek defects reconstructed with folded anterolateral thigh (ALT) flaps.
Patients and Methods: From January 2009 to May 2012, 10 patients with through-and-through cheek
defects resulting from resection of cheek tumor underwent reconstruction with the folded ALT flap at Sun
Yat-Sen University Cancer Center, Guangzhou, China. Surgical procedures in harvesting the ALT flap, as
well as the surgical anatomy, are described, and the success rate is reported.
Results: All ALT flaps were fasciocutaneous flaps. One patient with a thrombotic event required opera-
tive exploration in the perioperative period. All 10 flaps were based on a single perforator for reconstruc-
tion of defects. In all 10 cases, the donor site was closed primarily for the ALT flap, leaving only a linear scar
that was inconspicuous with normal clothing, and the thigh had no functional deficit.
Conclusions: The free ALT flap has good pliability and can be folded for the reconstruction of both the
inner and outer lining of through-and-through cheek defects. This flap presents good functional results at
the recipient site with the additional advantages of minimal donor-site morbidity, a very acceptable
esthetic result, and a high level of patient satisfaction.Crown Copyright � 2013 Published by Elsevier Inc on behalf of the American Association of Oral and
Maxillofacial Surgeons. All rights reserved
J Oral Maxillofac Surg 71:960-964, 2013
The reconstruction of substantial defects of the cheek
after tumor resection has always been a challenging
problem because of their extremely visible location,
as well as limited local tissue supply. In addition, the
cheek abuts several structures of expressive function,
such as the eyes, mouth, and local facial musculature.To achieve satisfactory functional and esthetic results,
reconstruction of such defects requires careful 3D res-
toration of all missing components, adequate texture
matching, and functional restoration. Several tech-
niques have been developed to reconstruct cheek de-
from State Key Laboratory of Oncology in South China,
nt of Head and Neck Surgery, Cancer Center, Sun Yat-Sen
, Guangzhou, China.
nt.
nt.
ate Professor (Attending Doctor).
ate Professor (Attending Doctor).
iate Professor (Attending Doctor).
nt.
nt.
sor (Attending Doctor).
ssor (Attending Doctor).
960
fects after surgery, to restore function and cosmesis.
The free radial forearm flap and the pectoralismajor my-
ocutaneous flap (PMMF)were themost commonly used
soft tissues for reconstruction of cheek defects.1-3
However, these yielded a series ofwell-knowndisadvan-
tages, especially related to donor-area complications.4,5
The anterolateral thigh (ALT) flap was originally de-
scribed by Song et al6 in 1984 as a septocutaneous flap
based on the descending branch of the lateral circum-
flex artery. Kimata et al7 first described the use of this
flap for the reconstruction of head and neck defects. In
Zhi-Min Liu, MD, and Di Wu, MD, contributed equally to this
work.
Supported by grants from the Natural Science Foundation of
Guangdong Province.
Address correspondence and reprint requests to Dr Liu: Depart-
ment of Head and Neck Surgery, Cancer Center, Sun Yat-Sen Univer-
sity, Guangdong, 510060, China; e-mail: [email protected]
Crown Copyright � 2013 Published by Elsevier Inc on behalf of the American
Association of Oral and Maxillofacial Surgeons. All rights reserved
0278-2391/12/01573-X$36.00/0
http://dx.doi.org/10.1016/j.joms.2012.10.022
LIU ET AL 961
the meantime, the ALT flap has become one of the pre-
ferred donor flaps for head and neck reconstruction.
Researchers have reported that the failure rate with
the free ALT flap was lower than 2%, and they
concluded that the free ALT flap could replace most
other flaps for soft tissue reconstruction, because of its
versatility in design, long pedicle with a suitable vessel
diameter, and low donor-site morbidity.8,9 Given theseadvantages, the ALT flap has gained worldwide
popularity over other flaps and today is the workhorse
in many centers.8-10 However, this flap has not
become particularly popular for the reconstruction of
through-and-through cheek defects. Researchers have
reported that the radical forearm flap is a highly suitable
flap and themost commonly used flap in reconstruction
of through-and-through cheek defects.3,11
The purpose of this article is to describe our prelim-
inary experience with the folded ALT flap, which was
exclusively used for the reconstruction of through-
and-through cheek defects.
Patients and Methods
Because of the retrospective nature of this study, it
was granted an exemption in writing by the University
of Sun Yat-Sen Institutional Review Board, Guang-
zhou, China.
From January 2009 to May 2012, 10 patients with
through-and-through cheek defects due to tumor re-
section underwent reconstruction with the foldedALT flap (Fig 1) at Sun Yat-Sen University Cancer Cen-
ter. There were 8 male and 2 female patients. The me-
dian age of patients was 56 years (range, 28-70 years).
All 10 patients hadmalignant oral tumors. Clinical stag-
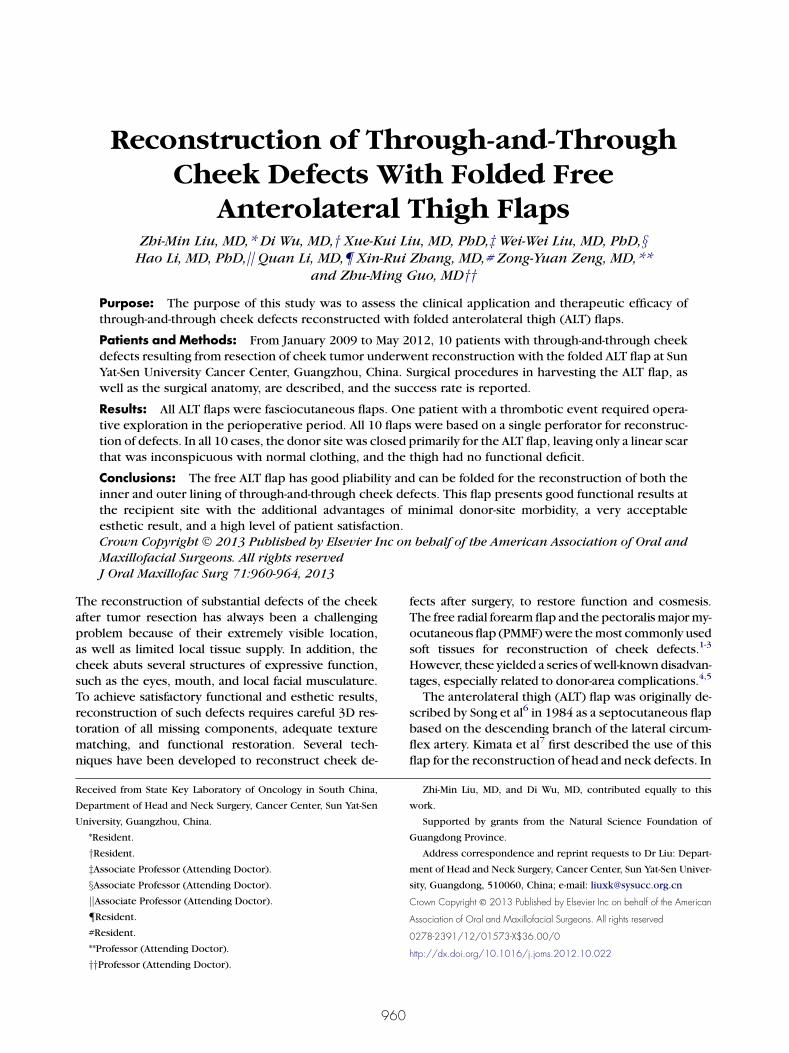
FIGURE 1. The lesion was completely excis
Liu et al. Through-and-Through Cheek Defect. J Oral Maxillofac Surg 20
ingwas performed according to the 2002 International
Union Against Cancer TNM Classification of Malignant
Tumors. Of the patients, 6 had previously untreated
disease whereas the remaining 4 had recurrent disease
at presentation.
SURGICAL TECHNIQUE
Flap Technique
The patient was in the supine position with a slight
medial rotation of the ipsilateral thigh. The anterior su-
perior iliac spine and the superolateral border of the
patella were identified and marked. A line was drawn
between the 2 points, which was the iliopatellar
line; the midpoint of this line was determined; anda skin paddle was drawn by use of this as a center
point. The iliopatellar line and the body surface projec-
tion line of the descending branch of the lateral cir-
cumflex femoral artery were marked. An incision
line was designed along the interior side of the iliopa-
tellar line. The skin and fascia lata were incised. The
skin flap was developed to the lateral side of the rectus
femoris muscle under the fascia lata. The flap waspulled by several sutures to expose the interface be-
tween the flap and the vastus lateralis muscle. The per-
forator was dissected carefully in the vastus lateralis
muscle. Mosquito hemostat forceps were used to deli-
cately dissect and explore the perforators penetrating
the fascia lata along the interface (Fig 2).
Insertion and Reconstruction
Theflapswere folded toprovide intraoralmucosal lin-
ing, aswell as the facial side of the cheek. The flap’s edge
closer to the perforator was first anchored to stabilize
the perforator and avoid any kinks and compressions.
ed (through-and-through cheek defect).
13.
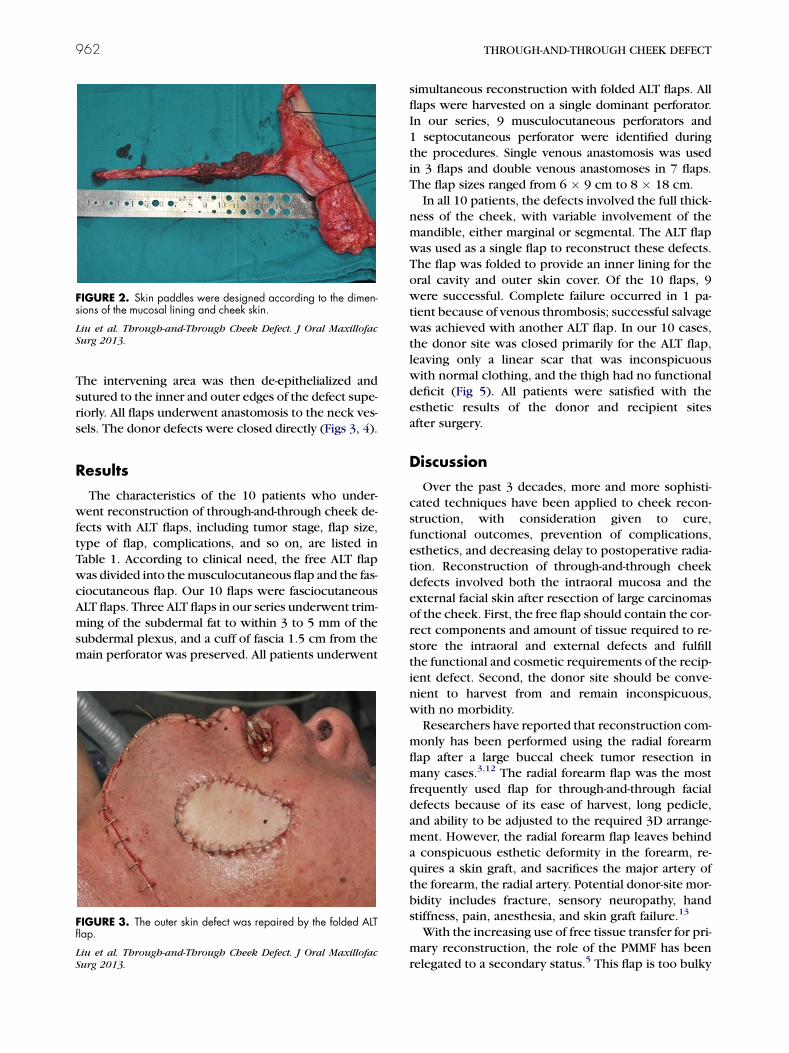
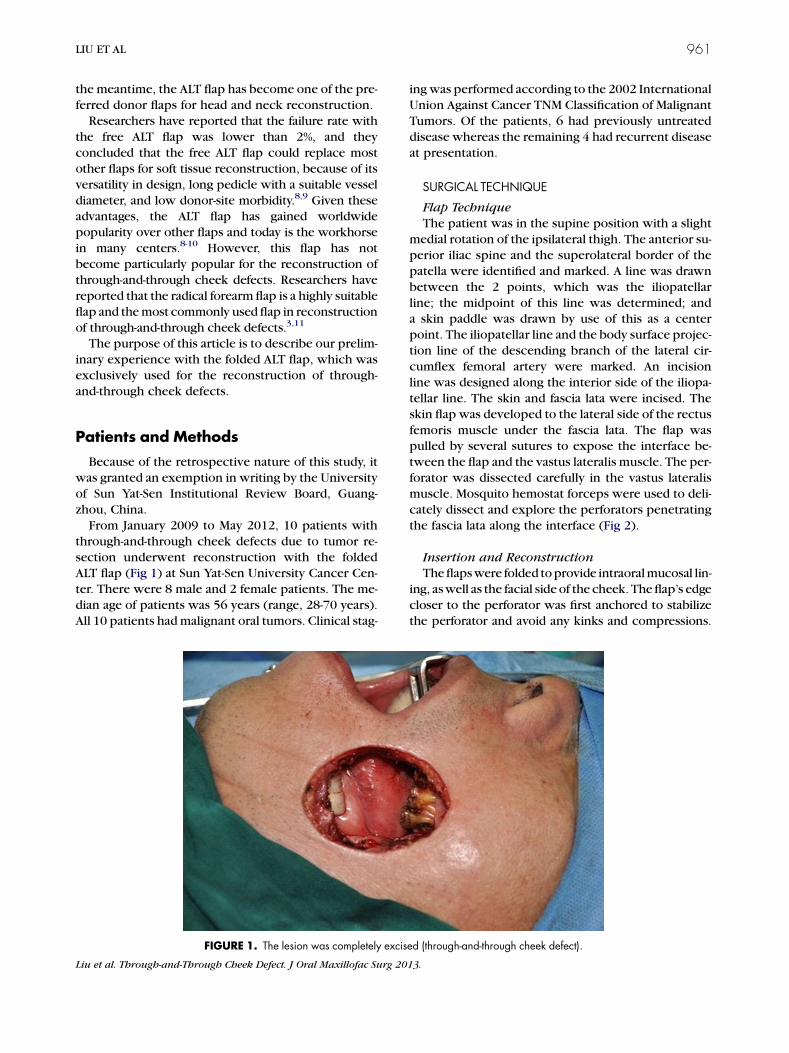
FIGURE 2. Skin paddles were designed according to the dimen-sions of the mucosal lining and cheek skin.
Liu et al. Through-and-Through Cheek Defect. J Oral Maxillofac
Surg 2013.
962 THROUGH-AND-THROUGH CHEEK DEFECT
The intervening area was then de-epithelialized and
sutured to the inner and outer edges of the defect supe-
riorly. All flaps underwent anastomosis to the neck ves-
sels. The donor defects were closed directly (Figs 3, 4).
Results
The characteristics of the 10 patients who under-went reconstruction of through-and-through cheek de-
fects with ALT flaps, including tumor stage, flap size,
type of flap, complications, and so on, are listed in
Table 1. According to clinical need, the free ALT flap
was divided into themusculocutaneous flap and the fas-
ciocutaneous flap. Our 10 flaps were fasciocutaneous
ALT flaps. Three ALT flaps in our series underwent trim-
ming of the subdermal fat to within 3 to 5 mm of thesubdermal plexus, and a cuff of fascia 1.5 cm from the
main perforator was preserved. All patients underwent
FIGURE 3. The outer skin defect was repaired by the folded ALTflap.
Liu et al. Through-and-Through Cheek Defect. J Oral Maxillofac
Surg 2013.
simultaneous reconstruction with folded ALT flaps. All
flaps were harvested on a single dominant perforator.
In our series, 9 musculocutaneous perforators and
1 septocutaneous perforator were identified during
the procedures. Single venous anastomosis was used
in 3 flaps and double venous anastomoses in 7 flaps.
The flap sizes ranged from 6 � 9 cm to 8 � 18 cm.
In all 10 patients, the defects involved the full thick-ness of the cheek, with variable involvement of the
mandible, either marginal or segmental. The ALT flap
was used as a single flap to reconstruct these defects.
The flap was folded to provide an inner lining for the
oral cavity and outer skin cover. Of the 10 flaps, 9
were successful. Complete failure occurred in 1 pa-
tient because of venous thrombosis; successful salvage
was achieved with another ALT flap. In our 10 cases,the donor site was closed primarily for the ALT flap,
leaving only a linear scar that was inconspicuous
with normal clothing, and the thigh had no functional
deficit (Fig 5). All patients were satisfied with the
esthetic results of the donor and recipient sites
after surgery.
Discussion
Over the past 3 decades, more and more sophisti-
cated techniques have been applied to cheek recon-
struction, with consideration given to cure,functional outcomes, prevention of complications,
esthetics, and decreasing delay to postoperative radia-
tion. Reconstruction of through-and-through cheek
defects involved both the intraoral mucosa and the
external facial skin after resection of large carcinomas
of the cheek. First, the free flap should contain the cor-
rect components and amount of tissue required to re-
store the intraoral and external defects and fulfillthe functional and cosmetic requirements of the recip-
ient defect. Second, the donor site should be conve-
nient to harvest from and remain inconspicuous,
with no morbidity.
Researchers have reported that reconstruction com-
monly has been performed using the radial forearm
flap after a large buccal cheek tumor resection in
many cases.3,12 The radial forearm flap was the mostfrequently used flap for through-and-through facial
defects because of its ease of harvest, long pedicle,
and ability to be adjusted to the required 3D arrange-
ment. However, the radial forearm flap leaves behind
a conspicuous esthetic deformity in the forearm, re-
quires a skin graft, and sacrifices the major artery of
the forearm, the radial artery. Potential donor-site mor-
bidity includes fracture, sensory neuropathy, handstiffness, pain, anesthesia, and skin graft failure.13
With the increasing use of free tissue transfer for pri-
mary reconstruction, the role of the PMMF has been
relegated to a secondary status.5 This flap is too bulky
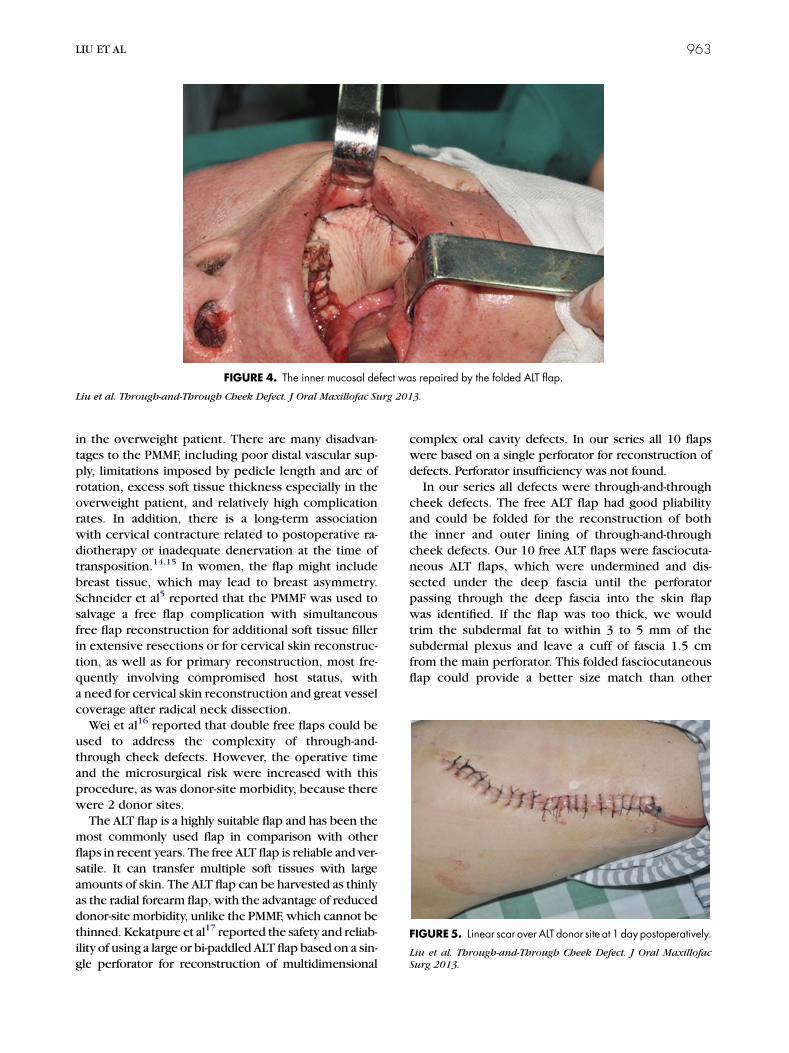
FIGURE 4. The inner mucosal defect was repaired by the folded ALT flap.
Liu et al. Through-and-Through Cheek Defect. J Oral Maxillofac Surg 2013.
FIGURE5. Linear scar over ALT donor site at 1 day postoperatively.
Liu et al. Through-and-Through Cheek Defect. J Oral Maxillofac
Surg 2013.
LIU ET AL 963
in the overweight patient. There are many disadvan-
tages to the PMMF, including poor distal vascular sup-
ply, limitations imposed by pedicle length and arc of
rotation, excess soft tissue thickness especially in the
overweight patient, and relatively high complicationrates. In addition, there is a long-term association
with cervical contracture related to postoperative ra-
diotherapy or inadequate denervation at the time of
transposition.14,15 In women, the flap might include
breast tissue, which may lead to breast asymmetry.
Schneider et al5 reported that the PMMF was used to
salvage a free flap complication with simultaneous
free flap reconstruction for additional soft tissue fillerin extensive resections or for cervical skin reconstruc-
tion, as well as for primary reconstruction, most fre-
quently involving compromised host status, with
a need for cervical skin reconstruction and great vessel
coverage after radical neck dissection.
Wei et al16 reported that double free flaps could be
used to address the complexity of through-and-
through cheek defects. However, the operative timeand the microsurgical risk were increased with this
procedure, as was donor-site morbidity, because there
were 2 donor sites.
The ALT flap is a highly suitable flap and has been the
most commonly used flap in comparison with other
flaps in recent years. The free ALT flap is reliable and ver-
satile. It can transfer multiple soft tissues with large
amounts of skin. The ALT flap can be harvested as thinlyas the radial forearm flap, with the advantage of reduced
donor-site morbidity, unlike the PMMF, which cannot be
thinned. Kekatpure et al17 reported the safety and reliab-
ility of using a large or bi-paddled ALT flap based on a sin-
gle perforator for reconstruction of multidimensional
complex oral cavity defects. In our series all 10 flaps
were based on a single perforator for reconstruction of
defects. Perforator insufficiency was not found.
In our series all defects were through-and-through
cheek defects. The free ALT flap had good pliabilityand could be folded for the reconstruction of both
the inner and outer lining of through-and-through
cheek defects. Our 10 free ALT flaps were fasciocuta-
neous ALT flaps, which were undermined and dis-
sected under the deep fascia until the perforator
passing through the deep fascia into the skin flap
was identified. If the flap was too thick, we would
trim the subdermal fat to within 3 to 5 mm of thesubdermal plexus and leave a cuff of fascia 1.5 cm
from the main perforator. This folded fasciocutaneous
flap could provide a better size match than other

964 THROUGH-AND-THROUGH CHEEK DEFECT
flaps for the reconstruction of through-and-through
cheek defects, at the same time leading to better
functional and esthetic results. The corner of the
mouth was preserved in our 10 cases, if it was in-
vaded and excised. The two skin islanded of the chi-
meric ALT flap should be well designed to form
a corner of the mouth.18 We believe that the chimeric
ALT flap, which was complex or often not necessaryin reconstruction of through-and-through cheek de-
fects without involving the corner of the mouth,
could lead to the risk of impairment of circulation
or direct injury to the perforating vessel.
One of the primary advantages of the ALT flap is the
reduced donor-site morbidity. Kuo et al19 reported ob-
jectively, using a kinetic communicator machine, that
patients who underwent myocutaneous ALT flap pro-cedures showed minimal weakness of the donor site
with long-term follow-up. In our 10 cases, all donor
sites were closed directly without any difficulty and
the wounds healed uneventfully.
All in all, the most important aspect of the folded
ALT flap in reconstruction of through-and-through
cheek defects lies in its versatility in design and com-
position, as well as low donor-site morbidity. Thefree ALT flap is also relatively safe and easy to harvest;
moreover, it can be harvested with a skin paddle as
large as possible and provides a longer pedicle length.
The operations for tumor resection and flap harvest
can be simultaneously performed, unlike scapular, par-
ascapular, and latissimus dorsi flap harvest, shortening
the operative time.8,20
The free ALTflaphas goodpliability and can be foldedfor the reconstruction of both the inner and outer lining
of through-and-through cheek defects. This flap pre-
sents good functional results at the recipient site, with
the additional advantages of minimal donor-site morbid-
ity, a very acceptable esthetic result, and a high level of
patient satisfaction. The free ALT flap is now considered
to be aworkhorse in our center in the reconstruction of
through-and-through cheek defects.
References
1. Heller L, Cole P, Kaufman Y: Cheek reconstruction: Currentconcepts in managing facial soft tissue loss. Semin Plast Surg22:294, 2008
2. Kroll SS, Evans GR, Goldberg D, et al: A comparison of resourcecosts for head and neck reconstruction with free and pectoralismajor flaps. Plast Reconstr Surg 99:1282, 1997
3. Yokoo S, Tahara S, Tsuji Y, et al: Functional and aesthetic recon-struction of full-thickness cheek, oral commissure and vermil-ion. J Craniomaxillofac Surg 29:344, 2001
4. Gupta M, Allen M, Corsten M: Reduction of donor site morbidityin the radial forearm free flap by use of topical tissue expanders.J Otolaryngol Head Neck Surg 38:628, 2009
5. Schneider DS, Wu V, Wax MK: Indications for pedicled pec-toralis major flap in a free tissue transfer practice. Head Neck34:1106, 2012
6. Song YG, Chen GZ, Song YL: The free thigh flap: A new free flapconcept based on the septocutaneous artery. Br J Plast Surg 37:149, 1984
7. Kimata Y, Uchiyama K, Ebihara S, et al: Versatility of the free an-terolateral thigh flap for reconstruction of head and neck de-fects. Arch Otolaryngol Head Neck Surg 123:1325, 1997
8. Sun G, Lu M, Tang E, et al: Clinical application of freeanterolateral thigh flap in the reconstruction of intraoraldefects. Oral Surg Oral Med Oral Pathol Oral Radiol Endod112:34, 2011
9. Wei FC, Jain V, Celik N, et al: Have we found an ideal soft-tissueflap? An experience with 672 anterolateral thigh flaps. Plast Re-constr Surg 109:2219, 2002
10. Lutz BS,Wei FC:Microsurgical workhorse flaps in head and neckreconstruction. Clin Plast Surg 32:421, 2005
11. Kang SH, Nam W, Cha IH, et al: Double continuous radial fore-arm flap for the reconstruction of full-thickness buccal cheek de-fect. J Plast Reconstr Aesthet Surg 62:e95, 2009
12. Disa JJ, Liew S, Cordeiro PG: Soft-tissue reconstruction of theface using the folded/multiple skin island radial forearm freeflap. Ann Plast Surg 47:612, 2001
13. Richardson D, Fisher SE, Vaughan ED, et al: Radial forearm flapdonor-site complications and morbidity: A prospective study.Plast Reconstr Surg 99:109, 1997
14. Maisel RH, Liston SL, Adams GL: Complications of pectoralismyocutaneous flaps. Laryngoscope 93:928, 1983
15. Liu R, Gullane P, Brown D, et al: Pectoralis major myocutaneouspedicled flap in head and neck reconstruction: Retrospective re-view of indications and results in 244 consecutive cases at theToronto General Hospital. J Otolaryngol 30:34, 2001
16. Wei FC, Demirkan F, Chen HC, et al: Double free flaps in recon-struction of extensive composite mandibular defects in headand neck cancer. Plast Reconstr Surg 103:39, 1999
17. Kekatpure VD, Trivedi NP, Shetkar G: Single perforator basedanterolateral thigh flap for reconstruction of large compositedefects of oral cavity. Oral Oncol 47:517, 2011
18. Liu WW, Yang AK, Ou YD: The harvesting and insetting ofa chimeric anterolateral thigh flap to reconstruct throughand through cheek defects. Int J Oral Maxillofac Surg 40:1421, 2011
19. Kuo YR, Jeng SF, Kuo MH, et al: Free anterolateral thigh flapfor extremity reconstruction: Clinical experience and func-tional assessment of donor site. Plast Reconstr Surg 107:1766, 2001
20. Valentini V, Cassoni A, Marianetti TM, et al: Anterolateral thighflap for the reconstruction of head and neck defects: Alternativeor replacement of the radial forearm flap? J Craniofac Surg 19:1148, 2008





























