Embed Size (px)
Citation preview

British Journal of Pkufrc Sugrry (I 989). 42, 5 12-S I6 ,% 1989 The Trustees of Brmsh Association of Plastic Surgeons
Reconstruction of the lower leg and foot with the reverse pedicled posterior tibia1 fasciocutaneous flap
G. HONG, K. STEFFENS and F. B. WANG
Service of Surgery of the Hand, Department of Orthopaedic Surgery, Tongji University Medical School, Wuhan, China, and Department of Orthopaedic Surgery, University of Essen Medical School, Federal Republic of Germany
Summary-The use of reverse flow island flaps for reconstructive surgery in the distal leg and foot represents an alternative to free flap transfer. This paper reports on the use of a reverse pedicled posterior tibia1 artery flap in four patients. The flap can reach any part of the foot.
The use of “reverse flow island flaps” in the distal lower leg and foot is comparatively recent. Only a few cases in which this principle has been used have been described, but it appears to offer a reliable alternative to microvascular free transfer of tissue.
Reverse flow island flaps have so far been based on the peroneal artery (Donski and Fogdestam, 1983 ; Yoshimura et al., 1984) and the anterior tibia1 artery (Wee, 1986; Morrison and Shen, 1987). The venous return in reverse flow island flaps was studied in detail by Torii et al. (1987). At the same time, they reported on a case of partial and one of total necrosis of an anterior tibia1 reverse flow island flap and expressed scepticism about the use of this type of flap.
The use of the posterior tibia1 artery fasciocuta- neous flap is not new. Okada et al. (1984) trans- planted such a flap microvascularly to an arm and Landra (1984) used one as a reverse flap and included the soleus muscle. Amarante et al. (1986) reported on a fasciocutaneous flap which was nourished by two perforating vessels from the posterior tibia1 artery 4 and 6.5 cm proximal to the medial malleolus. In the technique used by Amar- ante the flap was turned together with a small skin bridge. There was no ligation of the posterior tibia1 artery.
According to our preliminary experience in four cases in which a reverse pedicled posterior tibia1 fasciocutaneous flap was used, we consider such a bridge of skin unnecessary and it has the following disadvantages :
- Turning of the flap is partially impaired. ~ A larger defect results at the donor site.
- The posterior tibia1 nerve is Iocated directly deep to the grafted secondary defect.
Due to the restriction caused by the limited length of the perforating vessels, reconstruction of lateral and more distal areas of the foot is impossible with Amarante’s flap. We have extended the use of this flap in four cases by dividing the posterior tibia1 vessels proximal to the perforators, converting it into a reverse flow island flap.
Material and methods
E_xpforation of anatomical details by means ofpost- mortem dissections
We studied the vascular anatomy of the area by post-mortem dissection of 22 lower extremities. The findings can be summarised as follows :
- The posterior tibia1 artery constantly had two perforating cutaneous arteries located at an average distance of 4.3 cm and 6.9 cm above the medial malleolus.
- The posterior tibia1 artery is accompanied by two venae comitantes in which valves can be demonstrated.
- By means of dissection under a microscope, numerous communicating branches can be shown between the venae comitantes.
Considerations and investigations preceding surgery
It is essential that the presence of an alternative blood supply to the foot is known before the posterior tibia1 artery is divided. Simple palpation is insufficient since it cannot determine the direction
512
RECONSTRUCTION WITH THE REVERSE PEDICLED POSTERIOR TIBIAL FASCIOCUTANEOUS FLAP 513
of the blood flow, and proximal lesions of the blood vessels resulting in retrograde flow can remain unnoticed. Doppler investigation (Steffens et al., 1987) allows reliable exclusion of a proximally located lesion in the vessels. The interruption of the posterior tibia1 artery necessary during surgery can be simulated to a large extent by a technique similar to the Allen test in which the posterior tibia1 artery is compressed manually and the patient told to move his toes for several minutes. In doubtful cases angiography is also carried out.
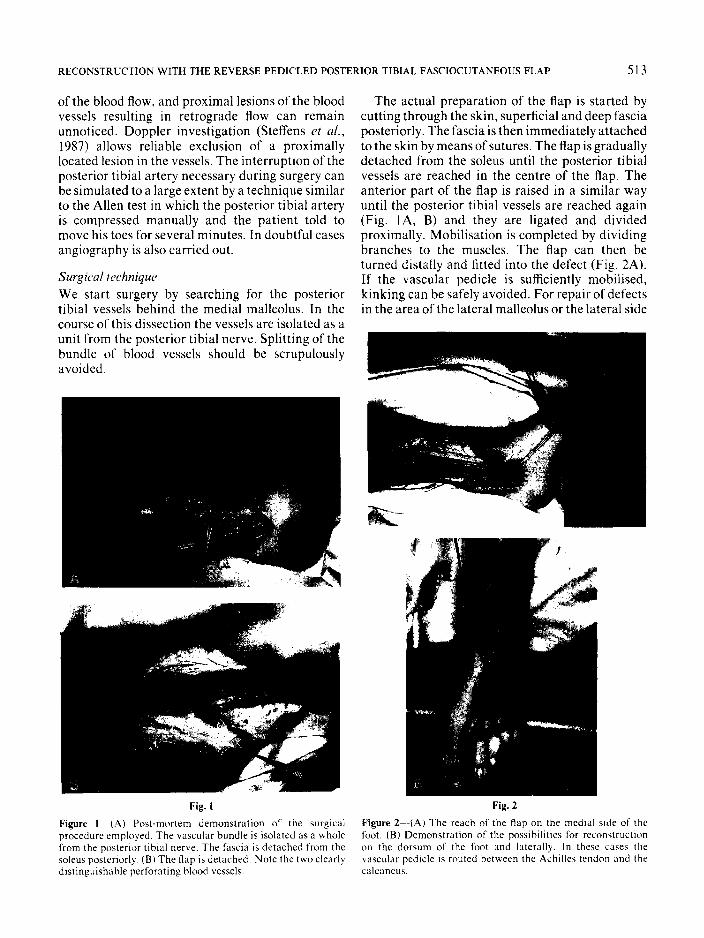
We start surgery by searching for the posterior tibia1 vessels behind the medial malleolus. In the course of this dissection the vessels are isolated as a unit from the posterior tibia1 nerve. Splitting of the bundle of blood vessels should be scrupulously avoided.
Fig. 1
Figure 1 (4) Post-mortem demonstration of the surgical procedure employed. The vascular bundle is isolated as a whole from the posterior tibia] nerve. The fascia is detached from the soleus posteriorly. (Bl The flap is detached. Note the two clearly distinguishable perforating hlood vessels.
The actual preparation of the flap is started by cutting through the skin, superficial and deep fascia posteriorly. The fascia is then immediately attached to the skin by means of sutures. The flap is gradually detached from the soleus until the posterior tibia1 vessels are reached in the centre of the flap. The anterior part of the flap is raised in a similar way until the posterior tibia1 vessels are reached again (Fig. lA, B) and they are ligated and divided proximally. Mobilisation is completed by dividing branches to the muscles. The flap can then be turned distally and fitted into the defect (Fig. 2A). If the vascular pedicle is sufficiently mobilised, kinking can be safely avoided. For repair of defects in the area of the lateral malleolus or the lateral side
Fig. 2
Figure 2--(A) The reach of the flap on the medial side of the foot. (Bl Demonstration of the possibilities for reconstruction on the dorsum of the foot and laterally. In these cases the vascular pedicle is routed between the Achilles tendon and the calcaneus.

514 BRITISH JOURNAL OF PLASTIC SURGERY
of the foot, the flap inlcuding the pedicle can be routed between the calcaneus and Achilles tendon. This passage offers sufficient clearance and there is no danger of compression of the vascular pedicle (Fig. 2B).
After the flap has been sutured into the defect, the skin overlying the posterior tibia1 nerve can be closed again.
Results
The technique has been used in four patients between October 1985 and November 1986. In two of them the defect was located on the lateral part of the foot. No complications were encountered during or after surgery in any of the cases. In each patient the flap healed completely in its new site. Following surgery, all flaps initially showed a slight bluish discolouration which disappeared completely be- tween 4 and 7 days later.
Illustrative case reports
Case I (Fig. 3) A 2%year-old female patient suffered a severe crushing injury of the medial side of the middle of her left foot. As a consequence of heavy scarring, the big toe was constantly flexed which impaired walking considerably. Earlier split skin grafting had not resulted in significant improvement.
The scarred area was completely excised. including part of the abductor hallucis muscle which was fibrosed. The considerable defect which resulted was repaired by means of a reverse pedicled posterior tibia1 fasciocuta- neous flap.
Following surgery, the flap and the grafted donor site healed without problems. A stable result was obtained and the patient is now able to walk normally, wearing slightly oversized ordinary commercial footwear.
Case Z (Fig. 4) A 24-year-old male patient presented with an ulcer due to pressure on the lateral side of the heel following severe
Fig. 3
Figure ~--CUSP I (A) The scar and flap outlined. (B) The scar emsed and raised. (C)The result 3 weeks after surgery

RECONSTRUCTION WITH THE REVERSE PEDICLED POSTERIOR TIBIAL FASCIOCUTANEOUS FLAP 515
Figure 4-Cast* 2. (A) Ulcer due to pressure over the lateral heel. (B) The flap outlined. The pivot point has been selected to allow passage of the flap and its vascular pedicle between the Achilles tendon and the calcaneus to reach the lateral defect without kinking. (C) Result I2 weeks after surgery. (D) Appearance of the donor site 12 weeks after surgery.
multiple trauma. After excision. the defect was recon- structed with a posterior tibia1 artery flap. The vascular pedicle of the flap was turned laterally and passed between the calcaneus and Achilles tendon.
After surgery the ankle joint was immobilised for 3 weeks. The flap healed without problems.
Discussion
The use of reverse flow flaps for reconstructive surgery in the distal leg and foot offers several obvious advantages; in particular, the surgical
procedures are comparatively simple and no micro- vascular anastomoses are needed. However, the need to sacrifice an important artery in the leg constitutes a potentially serious disadvantage. Other disadvantages, shared with most flaps in the area, are the secondary defect in the leg, with an obvious contour deformity, and the lack of sensa- tion.
The flap described by Amarante et ul. (1986) avoids the disadvantage of dividing one of the main arteries but the reach of this very interesting flap is limited to the heel and ankle. The indications for it

516 BRITISH JOURNAL OF PLASTIC SURGERY
overlap those of the calcaneal and dorsalis pedis island flaps.
It is possible to make the pivot point of the pedicled reverse flow posterior tibia1 artery flap up to 2-3 cm distal to the medial malleolus so that this long and mobile flap can reach almost all parts of the foot and close quite large defects. In our series the largest flap had a length of 15 cm and a width of 7 cm. However, Okada et al. (1984) have reported transplanting a posterior tibia1 free flap 22 cm x 9 cm.
Because of the relatively few number of cases, it is not yet possible to decide whether the reversed posterior tibial, the peroneal or the anterior tibia1 flap is the most reliable. In our experience dissection of the posterior tibia1 flap is significantly easier than raising either of the other two types, and another advantage is that it can be used on both sides of the foot.
A serious drawback of all reverse flow flaps is the ligation of one of the main arteries to the foot and it is therefore important that other less radical techniques, such as the calcaneus or flexor digito- rum brevis flaps, be considered first when recon- struction of a defect in this area is being planned.
Up to now we have performed this method only on patients under the age of 40 years. However, we believe that it is also applicable to older patients because of its advantages compared to microvas- cular transfer. In our opinion, its simple dissection and great versatility will lead to many uses for the reverse flow posterior tibia1 fasciocutaneous flap.
fasciocutaneous flap from the sural region. Scurufino~~iun Journal of Plastic and Reconstructice Surgery, 17, 19 I.
Landra, A. P. (1984). Q.E.D. flaps (? demonstrandum, disputan- dum or deprecandum): three useful axial pattern flaps in tropical African surgery. British JournalqfPIastic Surger?,. 37. 580.
Morrison, W. A. and Shen, T. Y. (1987). Anterior tibia1 artery flap: anatomy and case report. British Journal qf Plastic Surgery. 40,230.
Okada, T., Yasuda, Y., Kitamaya, Y. and Tsukada, S. (1984). Salvage of an arm by means of a free cutaneous flap based on the posterior tibia1 artery. Journal qf Reconstructire Microsur- gery, 1,25.
Steffens, K., Grtibmeyer, H. and Eren, S. (1987). Alleinige Doppler-Sonographie zue praoperativen Planung freier Lap- pentransplantationen. Handchirurgie. Mikrochirurgie. Plas- tische Chirurgie, 19. 284.
Torii, S.. Namiki, Y. and Mori, R. (1987). Reverse-flow island flap: clinical report and venous drainage. Plastic and Recon- structiee Surgery, 79. 600.
Wee, J. T. K. (1986). Reconstruction of the lower leg and foot with the reverse-pedicled anterior tibia1 flap: preliminary report of a new fasciocutaneous flap. British Journal ofPlastic Surger.v. 39. 327.
Yoshimura, M., Imura, S., Shimamura, K., Yamauchi, S. and Nomura, S. (1984). Peroneal flap for reconstruction in the extremity: preliminary report. Plastic and Reconstructive Surger?,, 74,402.
The Authors
Guangxiang Hong, MD, Professor. Service of Surgery of the Hand. Department oforthopaedic Surgery, Tongji University Medical School, Xiehe Clinic. Wuhan, People’s Republic of China.
Kurt Steffens, MD, Department of Orthopaedic Surgery, University of Essen Medical School, Essen.
F. B. Wang, MD, Service of Surgery of the Hand, Tongji University Medical School.
Requests for reprints to: Dr Kurt Steffens, Abteilung fur Hand-
References und.Rheumachfirurgie, Orthopadische Universitltskiinik Essen, im Evaneelischen Krankenhaus Essen-Werden. Pattberestrasse
Amarante, J., Costa, H., Reis, J. and Soares, R. (1986). A new I-3. D-4:00 Essen 16, Federal Republic of Germany. u distally based fasciocutaneous flap of the leg. British Journal ofPlastic Surgery, 39,338. Paper received 1 I April 1988.
Donski, P. K. and Fogdestam, J. (1983). Distally based Accepted 17 January 1989 after revision.