Embed Size (px)
Citation preview
British Journal of Plastic Surgery (2000), 53, 574~577 �9 2000 The British Association of Plastic Surgeons doi: 10.1054/bjps.2000.3407
I . . , . , . . ~ P L A S T I C S U R G E R Y
Reconstruction of the Achilles tendon and overlying soft tissue using antero-lateral thigh free flap
J.-W. Lee, J.-C. Yu, S.-J. Shieh, C. Liu and J.-J. Pai
Division of Plastic Surgery, Department of Surgery, National Cheng Kung University Hospital, Tainan, Taiwan
...... i
SUMMARY Reconstruction of combined loss of the Achilles tendon and overlying soft tissue was performed using an antero-lateral thigh free flap in three patients. The cutaneous portion is used to cover the open wound, and a piece of fascia lata is utilised to replace the missing segment of the Achilles tendon. The skin defect ranged from 5 x 2.5 to 7 x 5 cm, and the tendon loss measured from 3.5 to 5.5 cm in length. All of the patients showed satisfactory functional results with a follow-up period from 3 to 9 months. The advantages of the procedure are that: it is a single-staged opera- tion; it promotes rapid healing of the tendo Achilles since the tendon substitute is well vascularised; it is adaptable to a wide range of defect sizes and shapes; it can be performed in the supine position without the need for postural change; and it can restore good contour and causes minimal morbidity at the donor site. �9 2000 The British Association of Plastic Surgeons
Keywords: Achilles tendon, antero-lateral thigh free flap.
Combined loss of the Achilles tendon and the overlying soft tissue poses a difficult reconstructive problem. A successful reconstruction must have the following prereq- uisites: skin cover that is strong enough to withstand the repetitive friction and shearing forces during walking; a soft tissue cushion that is thin enough to allow for nor- mal shoes yet thick enough to offer adequate padding and protection; and a tendon reconstruction that has the appropriate strength, durability and tension to meet the dynamic workload. The lack of suitable local tissue at this site makes the task even more of a challenge. Various innovative procedures had been evolved with favourable outcome 1-5 and the prevalence of microsurgical free flap transfer in recent years attests to its superiority as a treat- ment modality in such a complicated situation.
After over 50 cases of antero-lateral thigh free flap harvesting in our institute, it was apparent that this flap might be useful in this particular situation. The skin-fat component could provide for wound coverage, and the strong fascia lata sheet could be rolled up to replace the lost Achilles tendon segment. Reconstruction of the com- plex tissue defect could be achieved in one stage with a single piece of vascularised tissue. We report three cases, discuss the superiority of this flap and compare the dif- ferences between our method and those of others already published.
"Operative procedures
The antero-lateral thigh flap was designed to be slightly larger than the soft tissue defect and preferably located on the contralateral side. We started with marking a straight line between the anterior superior iliac spine and the lateral edge of the patellar bone. The cutaneous perfo- rator is usually located in the midportion on that line, and could be detected with preoperative Doppler audiometry. A medial incision above the rectus femoris muscle is made and deepened down to the subfascial plane. The dissection is continued underneath the deep fascia and extended laterally until the cutaneous perforator is encountered. The skin portion is then harvested by incising the perimeter of the flap, and a piece of adjoining fascia lata strip is elevated as an integral part of the transplant. We use the posterior expansion of the fascia lata to con- struct the new tendon in order to prevent inadvertent injury to the flap vessel, which is located more anteriorly.
The posterior tibial vessel is the preferred recipient because of its proximity to the wound. The fascia lata sheet is rolled up to mimic the size and shape of the Achilles tendon, and reconstruction of the latter is achieved with 2-0 prolene sutures. The vascular anasto- mosis is performed under the microscope. The open wound is covered with the skin flap, and the donor defect is closed primarily over a suction drain.
Patients and methods
From March 1999 to November 1999, we reconstructed combined loss of Achilles tendon and overlying soft tis- sue in three cases. Two of them sustained the defect after avulsion injury, and the third suffered the tissue loss as a result of wound complication following initial tendon repair.
Case reports
Case 1
A 48-year-old male high school teacher played tennis as a hobby for more than 20 years. He had experienced soreness of the right heel region for 6 months. Tendinitis of the tendo Achilles was diagnosed and kenacort injections were adminis- tered on several occasions. He sustained sudden rupture of the
574
Achilles tendon and overlying soft tissue reconstruction 575
Achilles tendon the day before admission and a primary repair of the tendon using ethibond sutures was performed.
The postoperative course was complicated by wound edge skin necrosis and soft tissue infection, with subsequent develop- ment of tendon exposure and desiccation. He was referred to our service 2 months after the incident. Further debridement was conducted and the resultant defect measured about 7 x 5 cm in extent, with segmental loss of the Achilles tendon measuring 5.5 cm in length and about 75% of the tendon.
A 9 • 6 cm antero-lateral thigh flap from the left side was harvested, with a large piece of fascia lata included within the transplant. The fascia strip was rolled into an omelette-like con- figuration and used to connect the separated ends of the Achilles tendon. An end-to-side microvascular anastomosis was made between the posterior tibialis artery and the flap pedicle vessels. A protective splint was applied for a duration of 8 weeks. The patient was then allowed to resume ordinary activi- ty on a graduated schedule. Three months after the surgery, he could walk unaided and could even stand on his toes. There was no pain, local inflammatory reaction or sinus formation around the operated site. The bulk of subcutaneous fat is exces- sive, and thinning of the flap may be considered.
Case 2
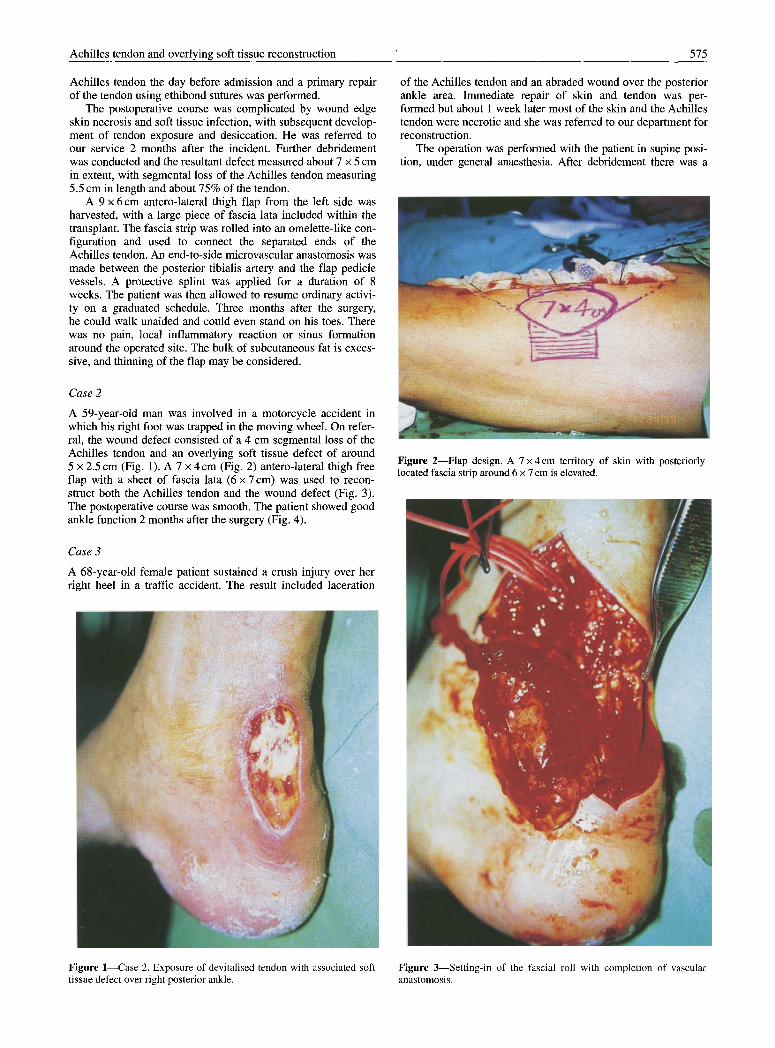
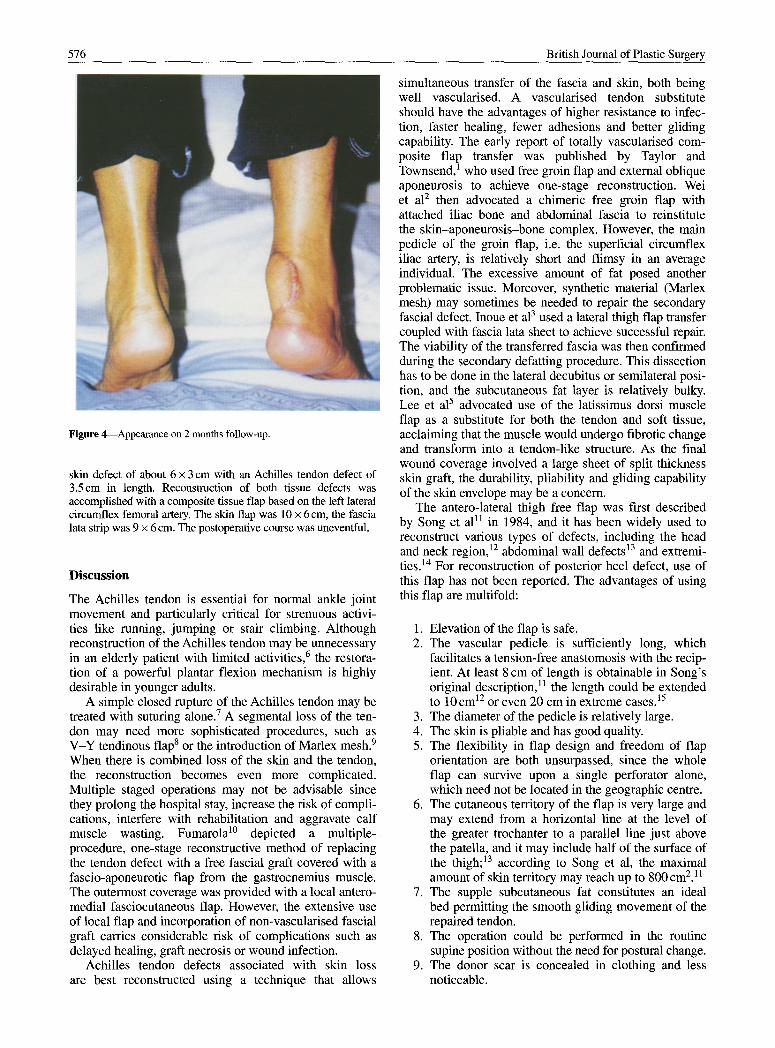
A 59-year-old man was involved in a motorcycle accident in which his right foot was trapped in the moving wheel. On refer- ral, the wound defect consisted of a 4 cm segmental loss of the Achilles tendon and an overlying soft tissue defect of around 5 • 2.5 cm (Fig. 1). A 7 • 4 c m (Fig. 2) antero-lateral thigh free flap with a sheet of fascia lata (6 • 7 cm) was used to recon- struct both the Achilles tendon and the wound defect (Fig. 3). The postoperative course was smooth. The patient showed good ankle function 2 months after the surgery (Fig. 4).
Case 3
A 68-year-old female patient sustained a crush injury over her right heel in a traffic accident. The result included laceration
of the Achilles tendon and an abraded wound over the posterior ankle area. Immediate repair of skin and tendon was per- formed but about 1 week later most of the skin and the Achilles tendon were necrotic and she was referred to our department for reconstruction.
The operation was performed with the patient in supine posi- tion, under general anaesthesia. After debridement there was a
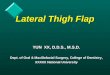
Figure 2---Flap design. A 7 x 4 cm territory of skin with posteriorly located fascia strip around 6 x 7 cm is elevated.
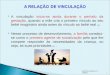
Figure 1--Case 2. Exposure of devitalised tendon with associated soft Figure 3--Setting-in of the fascial roll with completion of vascular tissue defect over right posterior ankle, anastomosis.
576 British Journal of Plastic Surgery
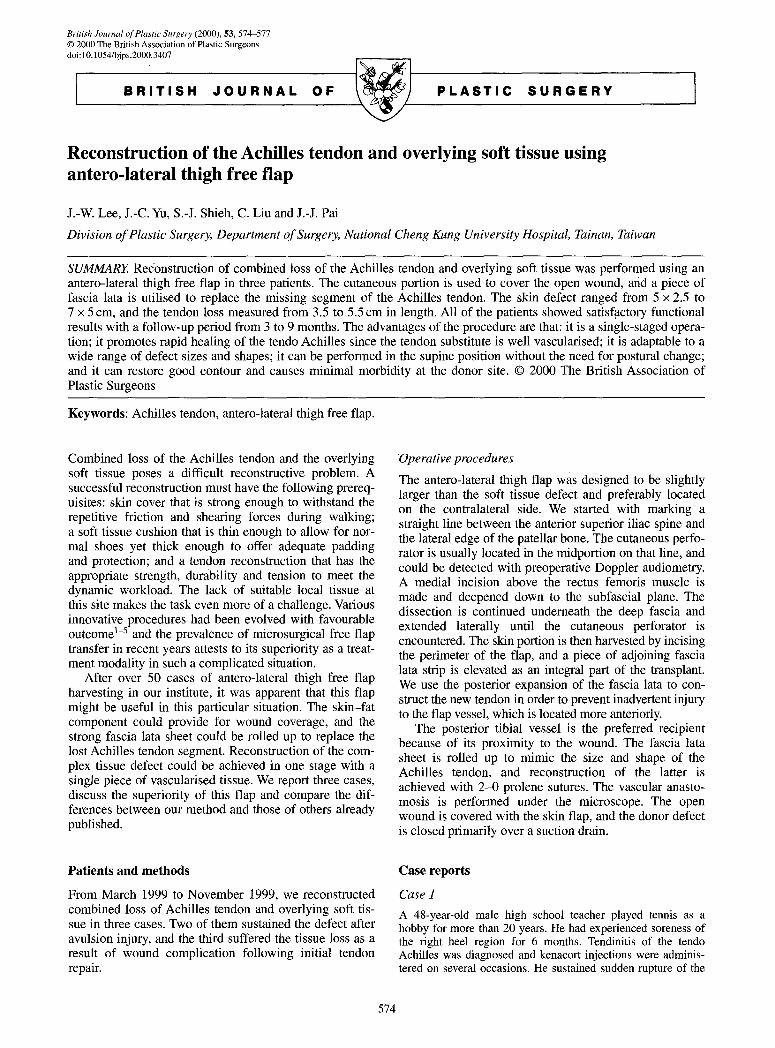
Figure 4--Appearance on 2 months follow-up.
skin defect of about 6 • 3 cm with an Achilles tendon defect of 3.5cm in length. Reconstruction of both tissue defects was accomplished with a composite tissue flap based on the left lateral circumflex femoral artery. The skin flap was 10 • 6cm, the fascia lata strip was 9 • 6 cm. The postoperative course was uneventful.
Discussion
The Achilles tendon is essential for normal ankle joint movement and particularly critical for strenuous activi- ties like running, jumping or stair climbing. Although reconstruction of the Achilles tendon may be unnecessary in an elderly patient with limited activities, 6 the restora- tion of a powerful plantar flexion mechanism is highly desirable in younger adults.
A simple closed rupture of the Achilles tendon may be treated with suturing alone. 7 A segmental loss of the ten- don may need more sophisticated procedures, such as V-Y tendinous flap s or the introduction of Marlex mesh. 9 When there is combined loss of the skin and the tendon, the reconstruction becomes even more complicated. Multiple staged operations may not be advisable since they prolong the hospital stay, increase the risk of compli- cations, interfere with rehabilitation and aggravate calf muscle wasting. Fumarola l~ depicted a multiple-. procedure, one-stage reconstructive method of replacing the tendon defect with a free fascial graft covered with a fascio-aponeurotic flap from the gastrocnemius muscle. The outermost coverage was provided with a local antero- medial fasciocutaneous flap. However, the extensive use of local flap and incorporation of non-vascularised fascial graft carries considerable risk of complications such as delayed healing, graft necrosis or wound infection.
Achilles tendon defects associated with skin loss are best reconstructed using a technique that allows
simultaneous transfer of the fascia and skin, both being well vascularised. A vascularised tendon substitute should have the advantages of higher resistance to infec- tion, faster healing, fewer adhesions and better gliding capability. The early report of totally vascularised com- posite flap transfer was published by Taylor and Townsend, 1 who used free groin flap and external oblique aponeurosis to achieve one-stage reconstruction. Wei et al 2 then advocated a chimeric free groin flap with attached iliac bone and abdominal fascia to reinstitute the skin-aponeurosis-bone complex. However, the main pedicle of the groin flap, i.e. the superficial circumflex iliac artery, is relatively short and flimsy in an average individual. The excessive amount of fat posed another problematic issue. Moreover, synthetic material (Marlex mesh) may sometimes be needed to repair the secondary fascial defect. Inoue et al 3 used a lateral thigh flap transfer coupled with fascia lata sheet to achieve successful repair. The viability of the transferred fascia was then confirmed during the secondary defatting procedure. This dissection has to be done in the lateral decubitus or semilateral posi- tion, and the subcutaneous fat layer is relatively bulky. Lee et al 5 advocated use of the latissimus dorsi muscle flap as a substitute for both the tendon and soft tissue, acclaiming that the muscle would undergo fibrotic change and transform into a tendon-like structure. As the final wound coverage involved a large sheet of split thickness skin graft, the durability, pliability and gliding capability of the skin envelope may be a concern.
The antero-lateral thigh free flap was first described by Song et a111 in 1984, and it has been widely used to reconstruct various types of defects, including the head and neck region, 12 abdominal wall defects 13 and extremi- ties. 14 For reconstruction of posterior heel defect, use of this flap has not been reported. The advantages of using this flap are multifold:
1. Elevation of the flap is safe. 2. The vascular pedicle is sufficiently long, which
facilitates a tension-free anastomosis with the recip- ient. At least 8 cm of length is obtainable in Song's original description, 11 the length could be extended to 10 cm 12 or even 20 cm in extreme cases. 15
3. The diameter of the pedicle is relatively large. 4. The skin is pliable and has good quality. 5. The flexibility in flap design and freedom of flap
orientation are both unsurpassed, since the whole flap can survive upon a single perforator alone, which need not be located in the geographic centre.
6. The cutaneous territory of the flap is very large and may extend from a horizontal line at the level of the greater trochanter to a parallel line just above the patella, and it may include half of the surface of the thigh; 13 according to Song et al, the maximal amount of skin territory may reach up to 800cm2.11
7. The supple subcutaneous fat constitutes an ideal bed permitting the smooth gliding movement of the repaired tendon.
8. The operation could be performed in the routine supine position without the need for postural change.
9. The donor scar is concealed in clothing and less noticeable.

Achilles tendon and overlying soft tissue reconstruction 577
10. The donor defect can often be closed directly. A defect up to 7cm ~4 or even 9cm wide 13 had been closed without the need of skin graft.
11. The skin flap is generally thin, or could be trimmed down to a thickness of 3--4 mm without endangering the viability of the flapJ 2,t4
12. With proper modification, it may be harvested as a chimeric flap, which can incorporate rectus femoris muscle, vastus lateralis muscle and/or fascia lata strip to reconstruct a multi-component defect.
13. The donor site stays far away from the recipient, therefore a two-team approach is feasible.
The only drawback is the variability of the vascular pedicle, and thus preoperative Doppler audiometry assess- ment is recommended.
The patients in our series made an uneventful and rapid recovery, which was instrumental in prompting an early return to a rehabilitation programme and helped to prevent further wasting of the calf muscle. This report indicates that the antero-lateral thigh flap may be a useful option in the reconstruction of compound defects in the posterior heel region.
6. Saunders DE, Hochberg J, Wittenborn W. Treatment of total loss of the Achilles tendon by skin flap cover without tendon repair. Plast Reconstr Surg 1978; 62: 708-12.
7. Kellam JF, Hunter GA, McElwain JP. Review of the operative treat- ment of Achilles tendon rupture. Clin Orthop 1985; 201: 80-3.
8. Abraham E, Pankovich AM. Neglected rupture of the Achilles ten- don: treatment by V-Y tendinous flap. J Bone Joint Surg 1975; 57A: 253-5.
9. Ozaki J, Fujiki J, Sugimoto K, Tamai S, Masuhara K. Reconstruction of neglected Achilles tendon rupture with Marlex mesh. Clin Orthop 1989; 238: 204-8.
10. Fumarola A. A one-stage reconstruction of a large defect of the tendo Achilles and the overlying skin. Br J Plast Surg 1985; 38: 403-6.
11. Song YG, Chen GZ, Song YL. The free thigh flap: a new free flap concept based on the septocutaneous artery. Br J Plast Surg 1984; 37: 149-59.
12, Koshima I, Fukuda H, Yamamoto H, Moriguchi T, Soeda S, Ohta S. Free anterolateral thigh flaps for reconstruction of head and neck defects. Plast Reconstr Surg 1993; 92: 421-30.
13. Kimata Y, Uchiyama K, Sekido M, et al. Anterolateral thigh flap for abdominal wall reconstruction. Plast Reconstr Surg 1999; 103:1191-7.
14. Kimura N, Satoh K. Consideration of a thin flap as an entity and clinical applications of the thin anterolateral thigh flap. Plast Reconstr Surg 1996; 97: 985-92.
15. Kimata Y, Uchiyama K, Ebihara S, Nakatsuka T, Harii K. Anatomic variations and technical problems of the anterolateral thigh flap: a report of 74 cases. Plast Reconstr Surg 1998; 102: 1517-23.
References
1. Taylor GI, Townsend E Composite free flap and tendon transfer: an anatomical study and a clinical technique. Br J Plast Surg 1979; 32: 170-83.
2. Wei F-C, Chen H-C, Chuang C-C, Noordhoff MS. Reconstruction of Achilles tendon and calcaneus defects with skin-aponeuro- sis-bone composite free tissue from the groin region. Plast Reconstr Surg 1988; 81: 579-87.
3. Inoue T, Tanaka I, Imai K, Hatoko M. Reconstruction of Achilles tendon using vascularised fascia lata with free lateral thigh flap. Br J Plast Surg 1990; 43: 728-31.
4. Lidman D, Nettelblad H, Berggren A, Rajan S. Reconstruction of soft tissue defects including the Achilles tendon with free neu- rovascular tensor fascia lata flap and fascia lata: case report. Scand J Plast Rec0nstr Surg 1987; 21: 213-18.
5. Lee H-B, Lew D-H, Oh S-H, et al. Simultaneous reconstruction of the Achilles tendon and soft-tissue defect using only a latissimus dorsi muscle free flap. Plast Reconstr Surg 1999; 104:111-19.
The Authors
Jing-Wei Lee MD, Instructor and Attending Plastic Surgeon Jui-Chin Yu MD, Attending Plastic Surgeon Shyh-Jou Shieh MD, Instructor and Attending Plastic Surgeon Cheng Liu MD, Attending Plastic Surgeon Jui-Jung Pal MD, Chief Resident
Division of Plastic Surgery, Department of Surgery, National Cheng Kung University Hospital, 138 Seng Li Road, Tainan 70428, Taiwan.
Correspondence to Dr Jui-Chin Yn.
Paper received 22 February 2000. Accepted 7 June 2000.