Embed Size (px)
Citation preview
1
Clinical Policy Title: Radioembolization and chemoembolization for liver cancer
and other indications
Clinical Policy Number: 05.02.09
Effective Date: February 1, 2016
Initial Review Date: November 18, 2015
Most Recent Review Date: February 15, 2017
Next Review Date: February 2018
Related policies:
None.
ABOUT THIS POLICY: Keystone First has developed clinical policies to assist with making coverage determinations. Keystone First’s clinical policies are based on guidelines from established industry sources, such as the Centers for Medicare & Medicaid Services (CMS), state regulatory agencies, the American Medical Association (AMA), medical specialty professional societies, and peer-reviewed professional literature. These clinical policies along with other sources, such as plan benefits and state and federal laws and regulatory requirements, including any state- or plan-specific definition of “medically necessary,” and the specific facts of the particular situation are considered by Keystone First when making coverage determinations. In the event of conflict between this clinical policy and plan benefits and/or state or federal laws and/or regulatory requirements, the plan benefits and/or state and federal laws and/or regulatory requirements shall control. Keystone First’s clinical policies are for informational purposes only and not intended as medical advice or to direct treatment. Physicians and other health care providers are solely responsible for the treatment decisions for their patients. Keystone First’s clinical policies are reflective of evidence-based medicine at the time of review. As medical science evolves, Keystone First will update its clinical policies as necessary. Keystone First’s clinical policies are not guarantees of payment.
Coverage policy
Keystone First considers the use of radioembolization to be clinically proven and, therefore, medically
necessary to treat cancer in the liver in the following instances:
Inoperable or unresectable primary hepatic cancer (i.e., hepatocellular carcinoma [HCC]).
Colorectal cancer with exclusively liver metastases.
Neuroendocrine tumors, such as octreotide-resistant carcinoid tumors or refractory
pancreatic neuroendocrine tumors (PNETs), which have spread to the liver.
Ocular melanoma that has spread to the liver when rendered in the context of an
investigational review board (IRB)-approved clinical trial protocol.
Cholangiocarcinoma (i.e., cholangiocellular carcinoma [CCC]) that has spread to the liver
when rendered in the context of an IRB-approved clinical trial protocol.
Liver tumors too large for surgery to shrink them to allow surgical removal.
Policy contains:
Transarterial embolization.
Radioembolization.
Chemoembolization.
Hepatocellular carcinoma.
2
Cancers in the liver that cannot be removed surgically and are not responsive to systemic
chemotherapy.
Preoperative treatment of liver cancer prior to orthotopic liver transplant (OTL).
Keystone First considers the use of chemoembolization to be clinically proven and, therefore, medically
necessary to treat cancer in the liver in the following instances:
• Inoperable or unresectable primary hepatic cancer (i.e., HCC).
• Neuroendocrine tumors, such as octreotide-resistant carcinoid tumors or refractory PNETs,
which have spread to the liver.
• Gastrointestinal stromal tumors (GIST) refractory to tyrosine kinase inhibitor therapy that
have spread to the liver.
• Ocular melanoma that has spread to the liver when rendered in the context of an IRB-
approved clinical trial protocol.
• Cholangiocarcinoma (i.e., CCC) that has spread to the liver when rendered in the context of
an IRB-approved clinical trial protocol.
• Preoperative treatment of liver cancer prior to OTL.
• Postoperative treatment of recurrent liver cancer after OTL.
Limitations:
Keystone First considers the use of radioembolization and chemoembolization to be investigational and,
therefore, not medically necessary in the following instances:
Ocular melanoma metastatic to liver and primary cholangiocarcinoma except when part of
an IRB-approved clinical trial protocol.
Breast cancer, lung cancer or other cancers except as indicated above or when part of an
IRB-approved clinical trial protocol.
Tumors ≤3 cm are optimally treated with ablation. Lesions between 3 to 5 cm may be
treated using combination embolization and ablation as long as tumor location is favorable.
Unresectable/inoperable lesions > five cm should be treated using arterial embolic
approaches.
In patients with early stage hepatocellular carcinoma (HCC) who are not candidates for liver
resection or transplant, radiofrequency ablation (RFA) is considered the best therapeutic
choice.
RFA is the recommended procedure for ≥3 unresectable colorectal liver metastases confined
to the liver.
Neuroendocrine tumors have been shown to respond favorably to somatostatin analogs;
however, refractory disease may become apparent in time and require additional therapy
(e.g., RFA).

3
Note: The criteria of tumor >5 cm or no more than three lesions in the liver are the indications for
surgery for HCC and do not pertain to the treatments of radioembolization and chemoembolization
addressed by this policy.
Alternative covered services:
Surgical resection of liver cancer.
Liver transplantation.
Somatostatin-analog treatment of endocrine-active hepatic metastases.
Chemotherapy of liver cancer.
Radiotherapy of liver cancer.
Background
The American Cancer Society estimates there were 35,660 new cases (25,510 in men and 10,150 in
women) of primary liver cancer and intrahepatic bile duct cancer diagnosed in the United States in 2015.
An average man's lifetime risk of getting liver or intrahepatic bile duct cancer is about one in 81, while
an average woman's risk is about one in 196. Most cases occur in people with certain risk factors (male
gender, Asian or Pacific Island descent, use of anabolic steroids, cigarette smoking, prior hepatitis B or
hepatitis C infection, cirrhosis, obesity, diabetes mellitus, various inherited conditions such as hereditary
hemochromatosis, and toxins such as aflatoxins, arsenic, and vinyl chloride). The average age at
diagnosis of liver cancer is 63 years.
Angiography of the hepatic circulation can be used to show the arteries that supply blood to a liver
cancer, which can help doctors plan treatment for liver cancer, and can also be used to guide some
types of non-surgical treatment, such as embolization (a procedure that injects substances to try to
block or reduce the blood flow to cancer cells in the liver). Angiography may be done with a
computerized tomography (CT) scanner (CT angiography) or a magnetic resonance imaging (MRI)
scanner (magnetic resonance [MR] angiography) instead of x-ray angiography because they can give
information about the blood vessels in the liver without the need for a catheter in the artery.
Formal staging systems, such as the American Joint Committee on Cancer (AJCC) TNM system, are
helpful to get an idea about a patient's prognosis and to help determine the most appropriate
treatment. This staging system is based on the results of the physical exam, imaging, and other tests to
assess the patient for three key pieces of information: 1) T describes the number and size of the primary
tumors, measured in centimeters, and whether the cancer has grown into nearby blood vessels or
organs; 2) N describes the extent of spread to nearby (regional) lymph nodes, and 3) M indicates
whether the cancer has metastasized to other parts of the body. But for treatment purposes, doctors
often classify liver cancers more simply, based on whether or not they can be entirely cut out (resected).

4
Potentially resectable or transplantable cancers are cancers that can be completely removed by surgery
or treated with liver transplant with a patient is healthy enough to tolerate the surgery. This would
include patients who do not have cirrhosis or other serious medical problems. If all of the cancer in the
liver is successfully removed, the overall five-year survival rate is over 50 percent. For people with early-
stage liver cancers who have a liver transplant, the five-year survival rate is in the range of 60 – 70
percent. Unfortunately, only a small number of patients with liver cancer present in this group.
Inoperable with only local disease implies that the cancer is small enough and in the right place to be
removed but the patient is not healthy enough for surgery (e.g., liver cancer in the presence of severe
cirrhosis) and surgery to remove the cancer might not leave enough liver to sustain life. Unresectable
cancers are those cancers that have not spread to the lymph nodes or distant organs but cannot be
completely removed by surgery. This includes cancers that have grown throughout the liver such that
they cannot be safely removed due to proximity to the great vessels or the bile ducts. There is potential
for use of embolization in treatment of large unresectable cancers to reduce their size sufficiently to
make resection feasible.
Advanced (metastatic) cancers are those that have spread to lymph nodes or other organs. Most
advanced liver cancers cannot be successfully treated with surgery. Embolization is an option for some
patients with tumors that cannot be removed by surgery. It can be used for tumors that are too large
(usually larger than five centimeters across) to be treated with ablation (a treatment that kills tumor
cells without removing them).
Finally, there is the case of a primary tumor elsewhere that has metastasized to the liver (e.g., colorectal
cancer). When these metastases threaten liver function and life it is possible to treat them with selective
arterial embolization and adjuvant intrahepatic radiotherapy or chemotherapy.
Embolization does reduce some of the blood supply to the normal liver tissue, so it may not be a good
option for those patients whose liver has been damaged by disease (i.e., hepatitis or cirrhosis). This type
of treatment typically does not require a hospital stay.
Searches
Keystone First searched PubMed and the databases of:
• UK National Health Services Center for Reviews and Dissemination.
• Agency for Healthcare Research and Quality’s National Guideline Clearinghouse and other
evidence-based practice centers.
• The Centers for Medicare & Medicaid Services (CMS).
We conducted searches on December 26, 2016. Searched terms were: "radioembolization (MeSH),"
"chemoembolization (MeSH)" and "liver cancer."
We included:
5
• Systematic reviews, which pool results from multiple studies to achieve larger sample sizes
and greater precision of effect estimation than in smaller primary studies. Systematic
reviews use predetermined transparent methods to minimize bias, effectively treating the
review as a scientific endeavor, and are thus rated highest in evidence-grading hierarchies.
• Guidelines based on systematic reviews.
• Economic analyses, such as cost-effectiveness, and benefit or utility studies (but not simple
cost studies), reporting both costs and outcomes — sometimes referred to as efficiency
studies — which also rank near the top of evidence hierarchies.
Findings
Arterial embolization is also known as trans-arterial embolization (TAE). In this procedure a catheter is
introduced into the femoral artery and threaded up into the hepatic artery in the liver. Once the
catheter is in place, small occlusive materials (e.g., Gel-foam® coil) are injected into the artery to plug it
up.
Radioembolization technique combines embolization with radiation therapy and is sometimes known as
trans-arterial radioembolization (TARE). In the United States, this is done by introducing small beads
called “microspheres” (i.e., TheraSphere® and SIR-Spheres®) that are embedded with a radioactive
isotope (yttrium-90 or Y-90) into the hepatic artery. The radio-infused beads lodge in the blood vessels
near the tumor, where they give off small amounts of radiation to the tumor site for several days. The
radiation travels a very short distance, so its effects are limited mainly to the tumor.
Radioembolization is used predominantly to treat cancer in the liver. The disease may take one of two
forms: 1) primary hepatic cancer (i.e., HCC), and 2) cancer that has metastasized to the liver from a
primary tumor elsewhere (e.g., colorectal cancer). Metastatic colorectal cancer to the liver and primary
HCC are the cancers most often considered for radioembolization treatment.
Lau (2012) reported the results of an expert panel convened to assess radioembolization as therapy for
HCC. The panel noted a number of variables in the outcome of treatment, such as the findings of
imaging of the tumor and its vasculature, tumor and uninvolved liver characteristics, previous therapies,
and localization of the microsphere infusion. There was consensus that radioembolization can improve
the clinical outcomes for selected patients with inoperable liver cancer.
Sangro (2011) in a systematic review of results from eight European medical centers found
radioembolization was effective in increasing survival of advanced HCC, demonstrating a median overall
survival of 12.8 months. The authors noted that survival varied significantly by functional status, hepatic
function, tumor burden (number of nodules) and presence or absence of extrahepatic disease. Common
adverse events were fatigue, nausea, vomiting, and abdominal pain.
In a large randomized controlled trial (RCT) of 291 patients Salem (2010) administered 526
radioembolization treatments (range one to five) to patients with HCC with response rates of 42 – 57

6
percent and overall time to progression of 7.9 months. Within this group were a limited number (n=56)
of patients with portal vein thrombosis whose survival was only 5.6 months.
A phase 2 trial of hepatic colorectal metastases treated by radioembolization (Van Hazel 2004) noted
radioembolization was more effective versus systemic chemotherapy with 5-flourouracil (5-FU) at
extending time to progression and survival. Dose of radiation was calculated based on the tumor volume
in the liver. The authors noted that a single infusion of Y-90 resulted in higher response and longer time
to progression (18.6 months versus 3.6 months) than chemotherapy with systemic 5-FUand leucovorin.
Median survival in the radioembolization group was almost two and a half years versus 18 months with
systemic chemotherapy.
Radioembolization has also been used for other forms of cancer affecting the liver, such as 1)
cholangiocarcinoma; 2) breast cancer with solely liver metastasis; 3) neuroendocrine tumors, such as
carcinoid tumors, that have spread to the liver; and 4) gastrointestinal sarcoma, a stromal tumor of the
gut also known as GIST.
A pilot study analyzing the use of Y-90 in 24 patients with biopsy-proven intrahepatic
cholangiocarcinoma (ICC) showed a favorable response to treatment and survival outcomes (Ibrahim
2008). Imaging follow-up of the study cohort demonstrated partial response in 27 percent, stable
disease in 68 percent and progression in 5 percent. Most patients (77 percent) showed >50 percent
tumor necrosis. Median overall survival was 14.9 months. Portal vein thrombosis was noted as a
particularly ominous predictive factor with patients achieving only 5.7 months of survival.
An ongoing, open clinical trial (Pitton 2013) comparing selective internal radiotherapy (SIRT) versus
transarterial chemoembolization with drug-eluting beads (DEBs) for the treatment of
cholangiocarcinoma has not yet posted results. A second clinical trial (Leyvraz 2013), also open to
enrollment, is comparing systemic sorafenib (an anti-angiogenic agent) versus radioembolizatoin with
Sir-Spheres® in the treatment of ocular melanoma.
Radioembolization for breast cancer metastases to liver was evaluated in an observational series that
demonstrated significant radiologic response, although survival benefit could not be established from
the study (Coldwell 2007). Diminished tumor volume was demonstrated in 47 percent, stable disease or
minor improvement in 47 percent and 5 percent showed no response. Survival was short in the patients
who failed to respond: median 3.6 months. Among responders the survival at 14 months was 86
percent.
Coldwell (2012) revisited this subject in a narrative review, citing evidence to support the use of
radioembolizatoin in liver metastases from neuroendocrine and breast cancers. The authors also noted
a number of other tumors (e.g., melanoma, lung) with similar radiobiologic profiles who may respond to
this treatment. They noted sufficient liver functional reserve and good patient performance status in the
absence of significant comorbidity was essential for success. Radioembolization was encouraged in

7
patients showing progression of liver metastases during treatment hiatus, in tumors that respond poorly
to chemotherapy or in treatment-refractory disease.
A systematic review (Yang 2012) of 37 RCTs inclusive of 1,575 patients examined the use of
radioembolization versus chemoembolization for unresectable neuroendocrine tumor liver metastases
(NETLM). The review examined the efficacy and safety of the use of hepatic arterial chemoembolization,
simple embolization and radioembolization and found comparable outcomes for all therapies with
regard to response to treatment, survival and toxicity. The authors noted that carcinoid had a
particularly high response rate of 67 percent versus 35 percent overall and concluded these therapies
are safe and effective in the treatment of NETLM.
A small series looked at the impact of radioembolization for GIST metastases to the peritoneum and the
liver in 11 patients failing tyrosine kinase inhibitor (TKI) therapy (Rathman 2015). Following
radioembolization three patients showed complete response, five showed partial response and one
showed stable disease. No patient showed progressive disease after radioembolization. Median survival
was 29.8 months (range, 10 – 72 months). The authors concluded that radioembolization is a safe and
effective therapy for patients with GIST liver metastases, and offered their results as a challenge to the
prevailing notion that GISTs are resistant to radiation therapy.
Radioembolization is often used in coordination with more well-established cancer treatments, such as
surgery and chemotherapy: 1) radioembolization may be used on liver tumors too large for surgery to
shrink them to allow surgical removal; and 2) chemotherapy and radioembolization may be provided in
combination to maximize the destruction of cancer cells.
In an RCT inclusive of 24 patients with advanced unresectable liver cancer or colorectal cancer
metastases to liver Cohen (2014) documented the pharmacokinetics of capecitabine in combination
with radio-embolization. Radioembolization with Y-90 resin microspheres was administered using a
sequential lobar approach with two cycles of capecitabine. The authors noted a partial response in four
patients (16.7 percent), stable disease in 17 (70.8 percent) and progression in three (12.5 percent).
Median time to progression and overall survival of the metastatic colorectal cancer cohort was 6.4 and
8.1 months, respectively.
Gulec (2013) compared radioembolization with selective arterial chemotherapy versus systemic
chemotherapy for hepatic colorectal cancer metastases. Treatment was administered with Y-90
microspheres and with contemporary standard chemotherapy for colorectal metastases to the liver.
Response to treatment was evaluated by serial fludeoxyglucose positron emission tomography and
computed tomography performed at four weeks, two to four months, and six to eight months. A
decrease in tumor size was seen in 19 of the 20 patients; however, the reduction of tumor size in the
radioembolization with selective arterial chemotherapy group was markedly greater. The authors
concluded that the chemo-radio combination produced superior objective responses compared with
systemic chemo-only treatment in a front-line treatment setting of patients with colorectal cancer liver
metastases.
8
A narrative review (Memon 2013) reported on radioembolization employed for treating patients with
unresectable HCC. The authors opined that this technique has proven useful for the majority of patients
with HCC as most of them present in advanced stage, beyond potentially curative options
(resection/liver transplantation). They also noted that radioembolization can be used in downstaging
large tumors to bring them within transplantable criteria, in patients with portal venous thrombosis due
to tumor invasion, and as palliative therapy.
Kosmider (2011) reported a series of 19 patients with unresectable liver metastases from colorectal
cancer treated with radioembolization and chemotherapy. Most (74 percent) had metastatic disease
confined to the liver. Concurrent treatment with 5-fluorourail/leucovorin (n = 7) or 5-
fluorourail/leucovorin/oxaliplatin (FOLFOX; n = 12) was started three to four days before a single
radioembolization treatment. Overall response was 84 percent. Median progression-free survival time
was 10.4 months and median overall survival time was 29.4 months.
Radioembolization can also be a treatment option for cancers in the liver that can’t be removed
surgically and are not responsive to chemotherapy. Bester (2012) retrospectively evaluated the safety
and survival of 339 patients with chemotherapy-refractory liver metastases treated with Y-90. The
median overall survival after radioembolization was 12.0 months, versus 6.3 months for a standard-care
cohort (n = 51). At three months of follow-up the incidence of serious adverse events was low. The
authors concluded radioembolization is an effective and safe treatment for patients with chemotherapy-
refractory hepatic metastases and improves overall survival in a select population of patients.
Radioembolization is generally only considered as treatment for cancers whose spread is limited to the
liver. Radioembolization is contraindicated in patients with severe liver disease where diminished
hepatic circulation may precipitate hepatic failure, or in patients with abnormal blood flow between the
liver and lungs (i.e., acquired arteriovenous malformation or shunting).
Chemoembolization, also known as transarterial chemoembolization (TACE), combines embolization
with chemotherapy. Specifically, the technique permits dearterialization of the tumor and selective
delivery of chemotherapeutic agents into the tumor's feeding vessels during angiography. Most often,
this is done by using tiny beads that give off a chemotherapy drug for the embolization. TACE can also
be done by giving chemotherapy through the catheter directly into the artery, then plugging up the
artery. Tumor ischemia raises the drug concentration compared to infusion alone and extends the
retention of the chemotherapeutic drug.
Spreafico (2015) evaluated the short-term safety and effectiveness of the new generation of 70-150 µm
drug-eluting beads (M1 DEB) in patients with hepatocellular carcinoma undergoing TACE as a primary
therapy or as a bridge to liver transplantation. A total of 45 consecutive patients underwent TACE with
M1 DEB loaded with doxorubicin (DEBDOX/M1). The mean number of TACE procedures per patient was
1.4. The objective response rate was 77.7 percent with a median time to best response of three months.
In 13 patients, DEBDOX/M1 TACE served as a bridge/down-staging to hepatectomy or liver

9
transplantation. The authors concluded that DEBDOX/M1 TACE is an effective modality of treatment
with promising results in terms of objective response rate and tumor down-staging.
In a narrative review Lencioni (2013) stated that TACE is the current standard of care for patients with
HCC and relatively preserved liver function, absence of cancer-related symptoms, and no evidence of
vascular invasion or extrahepatic spread. TACE may also be offered to patients with early-stage HCC
when surgical options or percutaneous ablation are precluded. The authors noted that in conventional
TACE, the administration of the anticancer-in-oil emulsion is followed by mechanical embolization with
either a spherical or a nonspherical embolic agent, but there is no consensus on the optimal
chemotherapeutic agents to use. Worldwide, the most popular anticancer drug for TACE of HCC is
doxorubicin. On the frequency of therapy, the authors noted that no randomized trials have been
designed to evaluate the optimal frequency of therapy; and that the safety and effectiveness of more
than four TACE procedures is unknown.
Cannon (2012) assessed the safety and effectiveness of chemoembolization with doxorubicin-eluting
doxorubicin beads (DEBDOX) in the treatment of multi-nodular (greater than or equal to 10 lesions)
HCC. At 12 months, a group of 42 patients with multi-nodular disease showed a response rate of 56
percent and median overall survival of 7.6 months. The authors concluded that DEBDOX treatment is
safe and effective when compared to historical controls and current best systemic therapy for multi-
nodular HCC.
In a narrative review of treatments for HCC, Biolato (2010) wrote “… as locoregional therapy, TACE
allows complete local tumor control of 25 – 35 percent and permits an increase of survival in patients
with HCC.” The authors also noted that percutaneous ethanol injection or radio frequency ablation as
neoadjuvant therapy prior to hepatectomy or transplantation was beneficial. The authors cited DEBs
loaded with doxorubicin and sorafenib as a further refinement of interest and recommended their
continued investigation. The authors concluded that TACE is the standard of care for treatment of
unresectable HCC.
Tokh (2010) assessed the safety, efficacy and survival among 63 patients with unresectable HCC treated
with beads loaded with doxorubicin (DOX). Median tumor size was 4.8 cm (range of 2 – 12 centimeters).
Overall, 81 percent showed tumor regression and alpha-feto protein (AFP) decreased in 79 percent of
patients with elevated levels, with a median fall of 78.5 percent. Actuarial survival was 18.2 months,
leading the authors to conclude that treatment of HCC using DEBDOX is at least equivalent, with milder
toxicity, than conventional TACE.
An RCT of 28 patients with unresectable recurrent HCC following orthotopic liver transplant (OLT)
randomized patients to lobaplatin-based chemoembolization or supportive care to assess response and
survival (Zhou 2010). Eight of the 14 patients in the chemoembolization group (57 percent) showed
partial tumor response (>30 percent reduction in tumor size), with significantly longer overall survival
compared to those who did not. No severe complications developed during follow-up in patients
receiving chemoembolization.

10
Chemoembolization has been successfully used as a palliative treatment of symptoms associated with
functioning neuroendocrine tumors (i.e., carcinoid tumors) involving the liver. It has also been utilized in
metastases to liver from GIST, and from PNETs that produce gastrin, insulin or other pancreatic
hormones.
Gupta (2003) retrospectively studied the outcomes of 81 patients with systemic chemotherapy-resistant
carcinoid metastases to liver when treated with hepatic artery embolization or chemoembolization by
evaluating the clinical and radiologic response rates, duration of response, and progression-free and
overall survival rates of these patients. Fifty patients were treated with bland hepatic artery
embolization, and 31 underwent chemoembolization. Of the 69 patients in whom radiologic response
could be evaluated, partial response was observed in 46 patients (67 percent), minimal response in six
(8.7 percent), stable disease in 11 (16 percent), and progressive disease in six (8.7 percent). The median
duration of response in the 42 patients with partial response was 17 months (range, four – 51 months).
Sixty-three percent of patients had a reduction in their tumor-related symptoms. The median
progression-free survival duration was 19 months (95 percent confidence interval, 17 – 21 months); the
probability of progression-free survival was 75 percent, 35 percent, and 11 percent at one, two, and
three years, respectively. The median overall survival time was 31 months (95 percent confidence
interval, 23 – 38 months); the survival probability was 93 percent at one year, 62 percent at two years,
and 24 percent at five years.
Cao (2012) evaluated the efficacy and safety of TACE for GIST with liver metastases after the failure of
TKI therapy. Sixty patients who were resistant and/or intolerant to prior imatinib and/or sunitinib were
eligible for the study. The patients were divided into two groups: those in the TACE group (n=22)
received TACE treatment containing 5 – 20 mL iodized oil and 40 – 80 mg doxorubicin hydrochloride and
TKI reintroduction or best supportive care, those in control group (n=38) only received TKI
reintroduction or best supportive care. In the TACE group, 12 patients (54.5 percent) achieved liver
partial response, five patients (22.7 percent) had stable disease, and five patients (22.7 percent) had
progressive disease. Disease control rate of liver metastases was 77.3 percent in the TACE group and
39.5 percent in the control group. The median overall survival in TACE group was also longer than in
control group (68.5 weeks, 95 percent CI: 57.4-79.6 vs. 25.7 weeks, 95 percent CI: 23.2-28.2) (P =
0.0001). TACE treatment significantly reduced the risk of death (hazard ratio: 0.109). Patients without
extrahepatic metastases treated with TACE had significantly better prognosis. The authors concluded
that TACE is effective and well tolerated in GIST patients with liver metastases after TKI failure, and it
may be an optional treatment for this disease.
Akahori (2013) reported the use of TACE to treat hepatic metastases of PNETs. The authors
administered cisplatin to unresectable PNET metastases with a total of 24 treatments in a small series of
five patients. There was one complete response, three partial responses and one patient whose disease
remained stable over the course of treatment and follow-up. Median survival of 36 months was
achieved without severe toxicity or adverse effect.
11
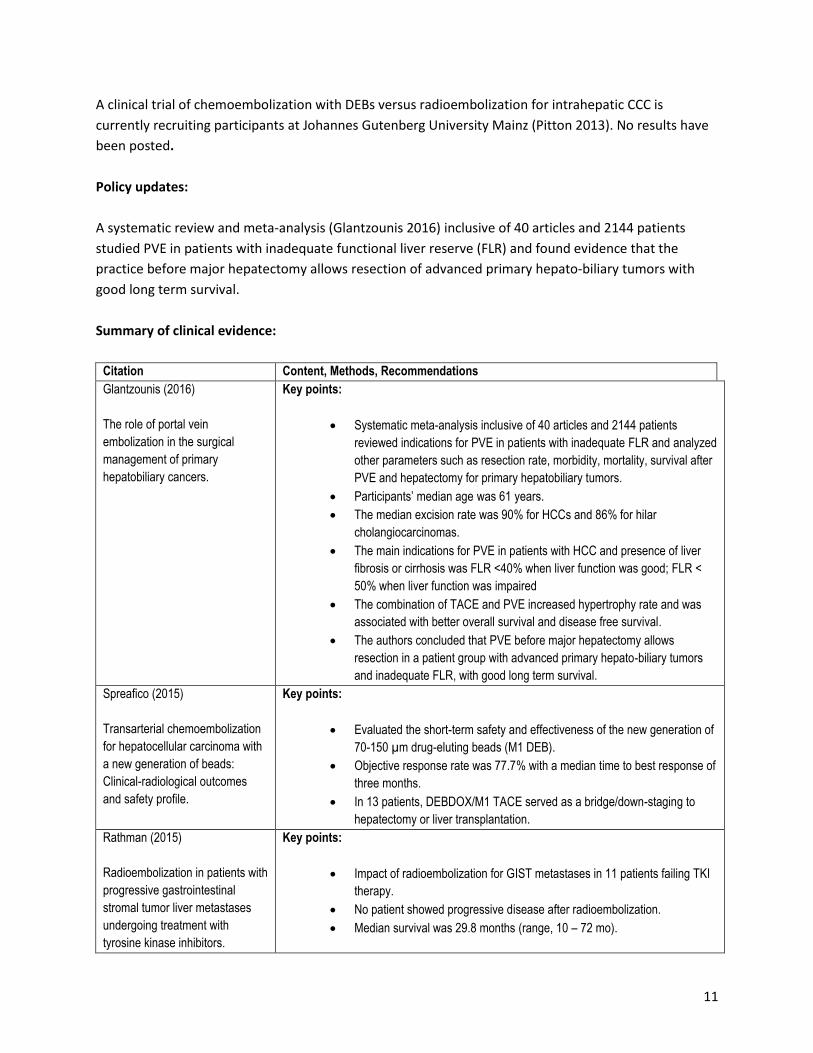
A clinical trial of chemoembolization with DEBs versus radioembolization for intrahepatic CCC is
currently recruiting participants at Johannes Gutenberg University Mainz (Pitton 2013). No results have
been posted.
Policy updates:
A systematic review and meta-analysis (Glantzounis 2016) inclusive of 40 articles and 2144 patients
studied PVE in patients with inadequate functional liver reserve (FLR) and found evidence that the
practice before major hepatectomy allows resection of advanced primary hepato-biliary tumors with
good long term survival.
Summary of clinical evidence:
Citation Content, Methods, Recommendations
Glantzounis (2016)
The role of portal vein
embolization in the surgical
management of primary
hepatobiliary cancers.
Key points:
Systematic meta-analysis inclusive of 40 articles and 2144 patients
reviewed indications for PVE in patients with inadequate FLR and analyzed
other parameters such as resection rate, morbidity, mortality, survival after
PVE and hepatectomy for primary hepatobiliary tumors.
Participants’ median age was 61 years.
The median excision rate was 90% for HCCs and 86% for hilar
cholangiocarcinomas.
The main indications for PVE in patients with HCC and presence of liver
fibrosis or cirrhosis was FLR <40% when liver function was good; FLR <
50% when liver function was impaired
The combination of TACE and PVE increased hypertrophy rate and was
associated with better overall survival and disease free survival.
The authors concluded that PVE before major hepatectomy allows
resection in a patient group with advanced primary hepato-biliary tumors
and inadequate FLR, with good long term survival.
Spreafico (2015)
Transarterial chemoembolization
for hepatocellular carcinoma with
a new generation of beads:
Clinical-radiological outcomes
and safety profile.
Key points:
Evaluated the short-term safety and effectiveness of the new generation of
70-150 µm drug-eluting beads (M1 DEB).
Objective response rate was 77.7% with a median time to best response of
three months.
In 13 patients, DEBDOX/M1 TACE served as a bridge/down-staging to
hepatectomy or liver transplantation.
Rathman (2015)
Radioembolization in patients with
progressive gastrointestinal
stromal tumor liver metastases
undergoing treatment with
tyrosine kinase inhibitors.
Key points:
Impact of radioembolization for GIST metastases in 11 patients failing TKI
therapy.
No patient showed progressive disease after radioembolization.
Median survival was 29.8 months (range, 10 – 72 mo).
12
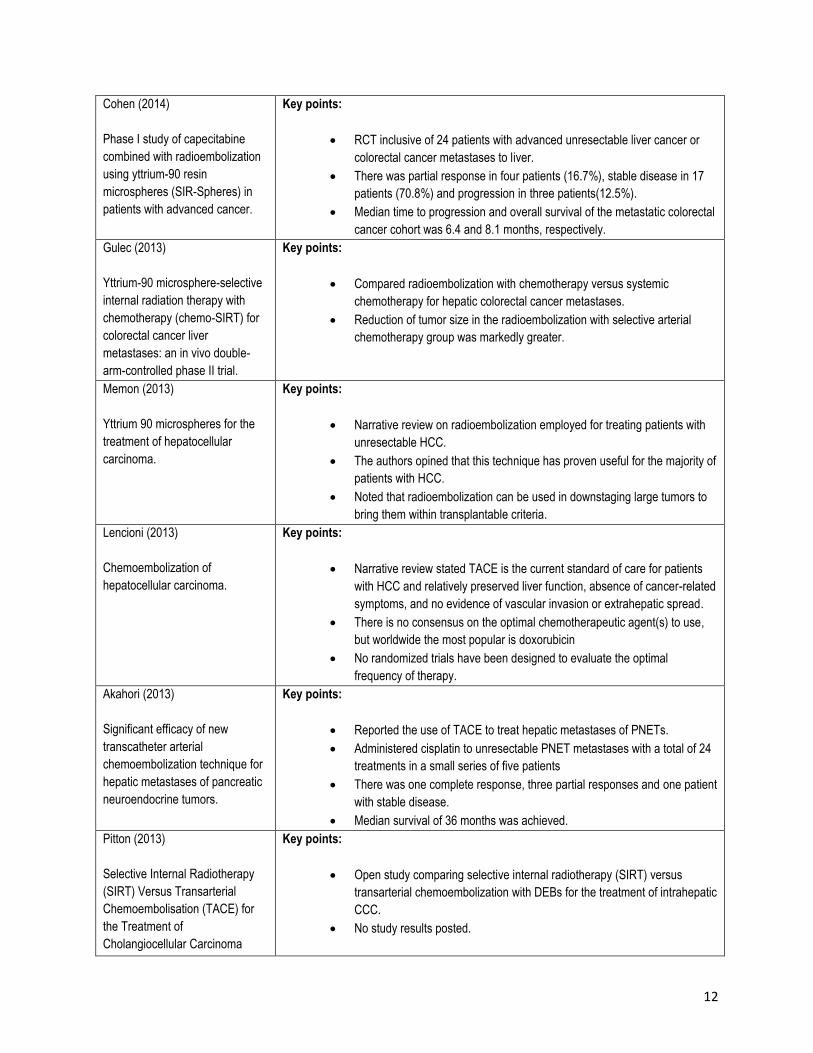
Cohen (2014)
Phase I study of capecitabine
combined with radioembolization
using yttrium-90 resin
microspheres (SIR-Spheres) in
patients with advanced cancer.
Key points:
RCT inclusive of 24 patients with advanced unresectable liver cancer or
colorectal cancer metastases to liver.
There was partial response in four patients (16.7%), stable disease in 17
patients (70.8%) and progression in three patients(12.5%).
Median time to progression and overall survival of the metastatic colorectal
cancer cohort was 6.4 and 8.1 months, respectively.
Gulec (2013)
Yttrium-90 microsphere-selective
internal radiation therapy with
chemotherapy (chemo-SIRT) for
colorectal cancer liver
metastases: an in vivo double-
arm-controlled phase II trial.
Key points:
Compared radioembolization with chemotherapy versus systemic
chemotherapy for hepatic colorectal cancer metastases.
Reduction of tumor size in the radioembolization with selective arterial
chemotherapy group was markedly greater.
Memon (2013)
Yttrium 90 microspheres for the
treatment of hepatocellular
carcinoma.
Key points:
Narrative review on radioembolization employed for treating patients with
unresectable HCC.
The authors opined that this technique has proven useful for the majority of
patients with HCC.
Noted that radioembolization can be used in downstaging large tumors to
bring them within transplantable criteria.
Lencioni (2013)
Chemoembolization of
hepatocellular carcinoma.
Key points:
Narrative review stated TACE is the current standard of care for patients
with HCC and relatively preserved liver function, absence of cancer-related
symptoms, and no evidence of vascular invasion or extrahepatic spread.
There is no consensus on the optimal chemotherapeutic agent(s) to use,
but worldwide the most popular is doxorubicin
No randomized trials have been designed to evaluate the optimal
frequency of therapy.
Akahori (2013)
Significant efficacy of new
transcatheter arterial
chemoembolization technique for
hepatic metastases of pancreatic
neuroendocrine tumors.
Key points:
Reported the use of TACE to treat hepatic metastases of PNETs.
Administered cisplatin to unresectable PNET metastases with a total of 24
treatments in a small series of five patients
There was one complete response, three partial responses and one patient
with stable disease.
Median survival of 36 months was achieved.
Pitton (2013)
Selective Internal Radiotherapy
(SIRT) Versus Transarterial
Chemoembolisation (TACE) for
the Treatment of
Cholangiocellular Carcinoma
Key points:
Open study comparing selective internal radiotherapy (SIRT) versus
transarterial chemoembolization with DEBs for the treatment of intrahepatic
CCC.
No study results posted.
13
(CCC).
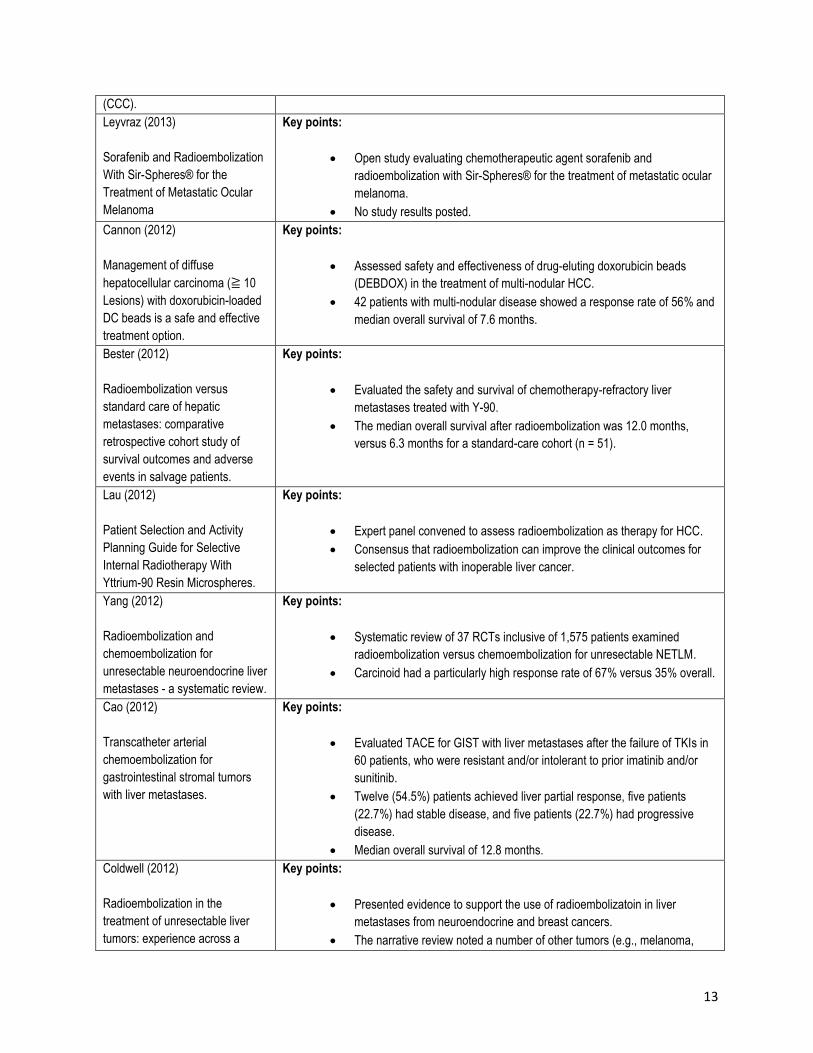
Leyvraz (2013)
Sorafenib and Radioembolization
With Sir-Spheres® for the
Treatment of Metastatic Ocular
Melanoma
Key points:
Open study evaluating chemotherapeutic agent sorafenib and
radioembolization with Sir-Spheres® for the treatment of metastatic ocular
melanoma.
No study results posted.
Cannon (2012)
Management of diffuse
hepatocellular carcinoma (≧ 10
Lesions) with doxorubicin-loaded
DC beads is a safe and effective
treatment option.
Key points:
Assessed safety and effectiveness of drug-eluting doxorubicin beads
(DEBDOX) in the treatment of multi-nodular HCC.
42 patients with multi-nodular disease showed a response rate of 56% and
median overall survival of 7.6 months.
Bester (2012)
Radioembolization versus
standard care of hepatic
metastases: comparative
retrospective cohort study of
survival outcomes and adverse
events in salvage patients.
Key points:
Evaluated the safety and survival of chemotherapy-refractory liver
metastases treated with Y-90.
The median overall survival after radioembolization was 12.0 months,
versus 6.3 months for a standard-care cohort (n = 51).
Lau (2012)
Patient Selection and Activity
Planning Guide for Selective
Internal Radiotherapy With
Yttrium-90 Resin Microspheres.
Key points:
Expert panel convened to assess radioembolization as therapy for HCC.
Consensus that radioembolization can improve the clinical outcomes for
selected patients with inoperable liver cancer.
Yang (2012)
Radioembolization and
chemoembolization for
unresectable neuroendocrine liver
metastases - a systematic review.
Key points:
Systematic review of 37 RCTs inclusive of 1,575 patients examined
radioembolization versus chemoembolization for unresectable NETLM.
Carcinoid had a particularly high response rate of 67% versus 35% overall.
Cao (2012)
Transcatheter arterial
chemoembolization for
gastrointestinal stromal tumors
with liver metastases.
Key points:
Evaluated TACE for GIST with liver metastases after the failure of TKIs in
60 patients, who were resistant and/or intolerant to prior imatinib and/or
sunitinib.
Twelve (54.5%) patients achieved liver partial response, five patients
(22.7%) had stable disease, and five patients (22.7%) had progressive
disease.
Median overall survival of 12.8 months.
Coldwell (2012)
Radioembolization in the
treatment of unresectable liver
tumors: experience across a
Key points:
Presented evidence to support the use of radioembolizatoin in liver
metastases from neuroendocrine and breast cancers.
The narrative review noted a number of other tumors (e.g., melanoma,
14
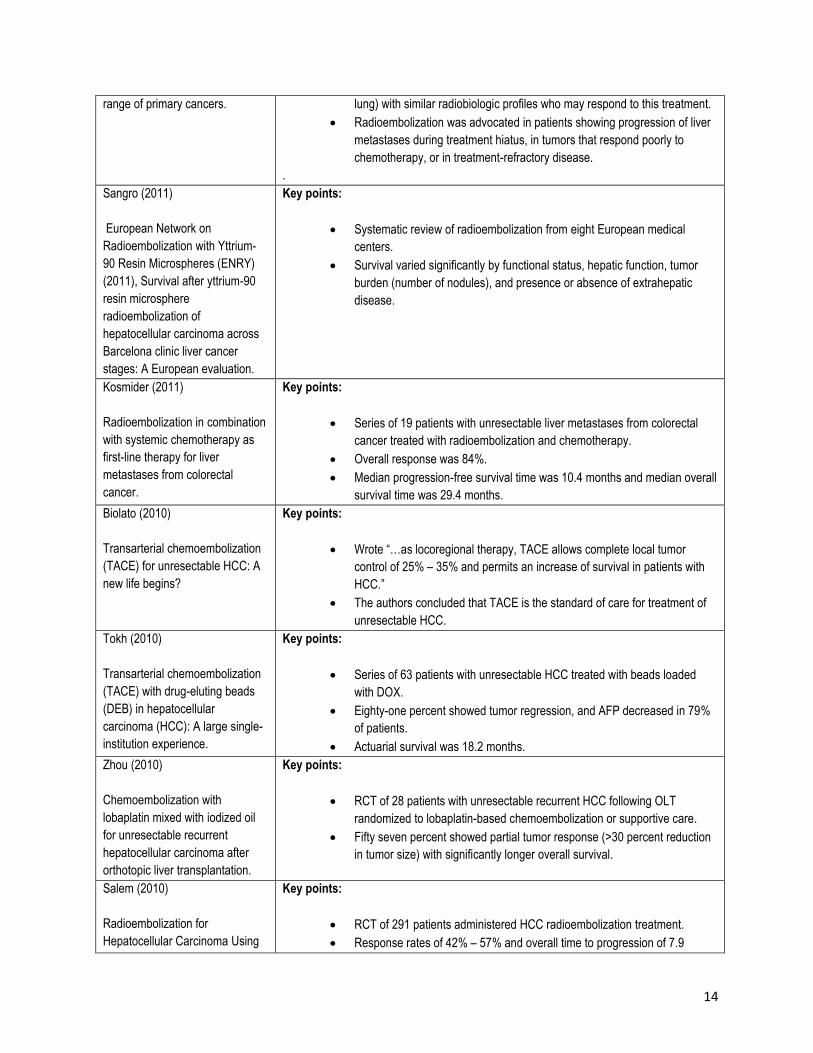
range of primary cancers.
lung) with similar radiobiologic profiles who may respond to this treatment.
Radioembolization was advocated in patients showing progression of liver
metastases during treatment hiatus, in tumors that respond poorly to
chemotherapy, or in treatment-refractory disease.
.
Sangro (2011)
European Network on
Radioembolization with Yttrium-
90 Resin Microspheres (ENRY)
(2011), Survival after yttrium-90
resin microsphere
radioembolization of
hepatocellular carcinoma across
Barcelona clinic liver cancer
stages: A European evaluation.
Key points:
Systematic review of radioembolization from eight European medical
centers.
Survival varied significantly by functional status, hepatic function, tumor
burden (number of nodules), and presence or absence of extrahepatic
disease.
Kosmider (2011)
Radioembolization in combination
with systemic chemotherapy as
first-line therapy for liver
metastases from colorectal
cancer.
Key points:
Series of 19 patients with unresectable liver metastases from colorectal
cancer treated with radioembolization and chemotherapy.
Overall response was 84%.
Median progression-free survival time was 10.4 months and median overall
survival time was 29.4 months.
Biolato (2010)
Transarterial chemoembolization
(TACE) for unresectable HCC: A
new life begins?
Key points:
Wrote “…as locoregional therapy, TACE allows complete local tumor
control of 25% – 35% and permits an increase of survival in patients with
HCC.”
The authors concluded that TACE is the standard of care for treatment of
unresectable HCC.
Tokh (2010)
Transarterial chemoembolization
(TACE) with drug-eluting beads
(DEB) in hepatocellular
carcinoma (HCC): A large single-
institution experience.
Key points:
Series of 63 patients with unresectable HCC treated with beads loaded
with DOX.
Eighty-one percent showed tumor regression, and AFP decreased in 79%
of patients.
Actuarial survival was 18.2 months.
Zhou (2010)
Chemoembolization with
lobaplatin mixed with iodized oil
for unresectable recurrent
hepatocellular carcinoma after
orthotopic liver transplantation.
Key points:
RCT of 28 patients with unresectable recurrent HCC following OLT
randomized to lobaplatin-based chemoembolization or supportive care.
Fifty seven percent showed partial tumor response (>30 percent reduction
in tumor size) with significantly longer overall survival.
Salem (2010)
Radioembolization for
Hepatocellular Carcinoma Using
Key points:
RCT of 291 patients administered HCC radioembolization treatment.
Response rates of 42% – 57% and overall time to progression of 7.9
15
Yttrium-90 Microspheres: A
Comprehensive Report of Long-
term Outcomes.
months.
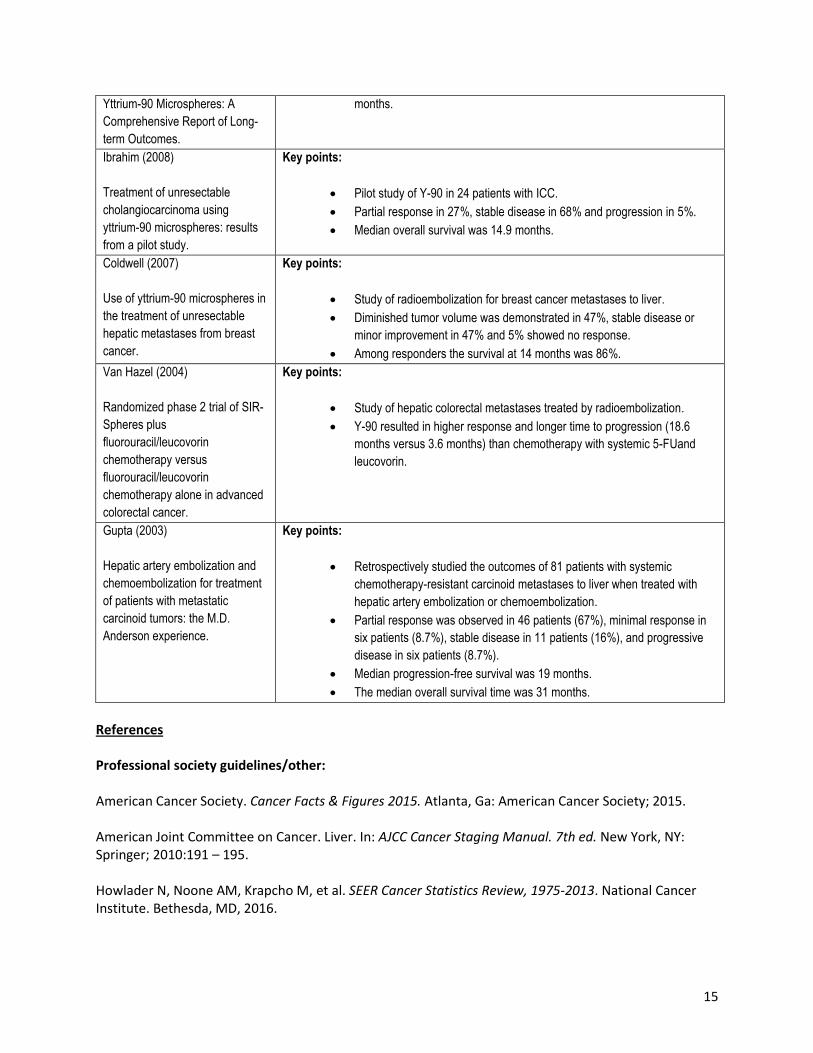
Ibrahim (2008)
Treatment of unresectable
cholangiocarcinoma using
yttrium-90 microspheres: results
from a pilot study.
Key points:
Pilot study of Y-90 in 24 patients with ICC.
Partial response in 27%, stable disease in 68% and progression in 5%.
Median overall survival was 14.9 months.
Coldwell (2007)
Use of yttrium-90 microspheres in
the treatment of unresectable
hepatic metastases from breast
cancer.
Key points:
Study of radioembolization for breast cancer metastases to liver.
Diminished tumor volume was demonstrated in 47%, stable disease or
minor improvement in 47% and 5% showed no response.
Among responders the survival at 14 months was 86%.
Van Hazel (2004)
Randomized phase 2 trial of SIR-
Spheres plus
fluorouracil/leucovorin
chemotherapy versus
fluorouracil/leucovorin
chemotherapy alone in advanced
colorectal cancer.
Key points:
Study of hepatic colorectal metastases treated by radioembolization.
Y-90 resulted in higher response and longer time to progression (18.6
months versus 3.6 months) than chemotherapy with systemic 5-FUand
leucovorin.
Gupta (2003)
Hepatic artery embolization and
chemoembolization for treatment
of patients with metastatic
carcinoid tumors: the M.D.
Anderson experience.
Key points:
Retrospectively studied the outcomes of 81 patients with systemic
chemotherapy-resistant carcinoid metastases to liver when treated with
hepatic artery embolization or chemoembolization.
Partial response was observed in 46 patients (67%), minimal response in
six patients (8.7%), stable disease in 11 patients (16%), and progressive
disease in six patients (8.7%).
Median progression-free survival was 19 months.
The median overall survival time was 31 months.
References Professional society guidelines/other: American Cancer Society. Cancer Facts & Figures 2015. Atlanta, Ga: American Cancer Society; 2015. American Joint Committee on Cancer. Liver. In: AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer; 2010:191 – 195. Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975-2013. National Cancer Institute. Bethesda, MD, 2016.

16
National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: Hepatobiliary Cancers. V.2.2014. Web site. www.nccn.org. Accessed December 26, 2016. Organ Procurement and Transplantation Network (OPTN) and Scientific Registry of Transplant Recipients (SRTR). OPTN / SRTR 2012 Annual Data Report: liver. Rockville, MD: Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation; 2012. Website. http://srtr.transplant.hrsa.gov/annual_reports/2012/pdf/03_liver_13.pdf. Accessed December 26, 2016. United States Department of Health and Human Services. The Health Consequences of Smoking — 50 Years of Progress. A Report of the Surgeon General. Website. http://www.surgeongeneral.gov/library/reports/50-years-of-progress/full-report.pdf Accessed December 26, 2016. Peer-reviewed references: Akahori T, Sho M, Tanaka T, et al. Significant efficacy of new transcatheter arterial chemoembolization technique for hepatic metastases of pancreatic neuroendocrine tumors. Anticancer Res. 2013 Aug;33(8):3355 – 8. Asnacios A, Fartoux L, Romano O, et al. Gemcitabine plus oxaliplatin (GEMOX) combined with cetuximab in patients with progressive advanced stage hepatocellular carcinoma: Results of a multicenter phase 2 study. Cancer. 2008;112:2733 – 2739. Bartlett DL, DiBisceglie AM, Dawson LA. Cancer of the liver. In: DeVita VT, Lawrence TS, Rosenberg SA, eds. DeVita, Hellman, and Rosenberg's Cancer: Principles and Practice of Oncology. 9th ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2011:997 – 1018. Bester L, Meteling B, Pocock N, Pavlakis N, Chua TC, Saxena A, et al. Radioembolization versus standard care of hepatic metastases: comparative retrospective cohort study of survival outcomes and adverse events in salvage patients. J Vasc Interv Radiol 2012;23:96 – 105. Biolato M, Marrone G, Racco S, et al. Transarterial chemoembolization (TACE) for unresectable HCC: A new life begins? Eur Rev Med Pharmacol Sci. 2010;14(4):356 – 362. Brandi G, de Rosa F, Agostini V, et al. Metronomic capecitabine in advanced hepatocellular carcinoma patients: a phase II study. Oncologist. 2013;18(12):1256 – 7. Bruix J, Tak WY, Gasbarrini A, et al. Regorafenib as second-line therapy for intermediate or advanced hepatocellular carcinoma: multicentre, open-label, phase II safety study. Eur J Cancer. 2013;49(16):3412 – 9. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42:1208 – 1230. Cannon RM, Urbano J, Kralj I, et al. Management of diffuse hepatocellular carcinoma (≧ 10 Lesions) with doxorubicin-loaded DC beads is a safe and effective treatment option. Onkologie. 2012;35(4):184 – 188.
17
Cao G, Li J, Shen L, Zhu X. Transcatheter arterial chemoembolization for gastrointestinal stromal tumors with liver metastases. World J Gastroenterol. 2012 Nov 14;18(42):6134 – 40. Cohen SJ, Konski AA, Putnam S, et al. Phase I study of capecitabine combined with radioembolization using yttrium-90 resin microspheres (SIR-Spheres) in patients with advanced cancer. Br J Cancer. 2014;111(2):265 – 271. Coldwell DM, Kennedy AS, Nutting CW.Use of yttrium-90 microspheres in the treatment of unresectable hepatic metastases from breast cancer. Int J Radiat Oncol Biol Phys. 2007 Nov 1;69(3):800 – 4. Coldwell D Sangro B, Salem R, Wasan H, Kennedy A. Radioembolization in the treatment of unresectable liver tumors: experience across a range of primary cancers. Am J Clin Oncol. 2012;35(2):167 – 77. El-Serag HB. Hepatocellular carcinoma. N Engl J Med. 2011;365:1118 – 1127. Forner A, Llovet JM, Bruix J. Hepatocellular carcinoma. Lancet. 2012;379:1245 – 1255. Glantzounis GK, Tokidis E, Basourakos SP, Ntzani EE, Lianos GD, Pentheroudakis G. The role of portal vein embolization in the surgical management of primary hepatobiliary cancers. A systematic review. Eur J Surg Oncol. 2016;0748-7983(16):30177-9. Graf H, Jüngst C, Straub G, et al. Chemoembolization combined with pravastatin improves survival in patients with hepatocellular carcinoma. Digestion. 2008;78:34 – 38. Gulec SA , Pennington K, Wheeler J, et al. Yttrium-90 microsphere-selective internal radiation therapy with chemotherapy (chemo-SIRT) for colorectal cancer liver metastases: an in vivo double-arm-controlled phase II trial. Am J Clin Oncol. 2013 Oct;36(5):455 – 60. Gupta S, Yao JC, Ahrar K, et al. Hepatic artery embolization and chemoembolization for treatment of patients with metastatic carcinoid tumors: the M.D. Anderson experience. Cancer J. 2003;9(4):261 – 7. Hassan MM, Spitz MR, Thomas MB, et al. Effect of different types of smoking and synergism with hepatitis C virus on risk of hepatocellular carcinoma in American men and women: Case-control study. Int J Cancer. 2008;123:1883 – 1891. Heo J, Reid T, Ruo L, et al. Randomized dose-finding clinical trial of oncolytic immunotherapeutic vaccinia JX-594 in liver cancer. Nat Med. 2013 Mar;19(3):329 – 336. Hoshida Y, Villanueva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med. 2008;359:1995 – 2004. Ibrahim S, Mulcahy M, Lewndowski R, et al. Treatment of unresectable cholangiocarcinoma using yttrium-90 microspheres: results from a pilot study. Cancer 2008:113:2119 – 28. Ishizuka M, Kubota K, Shimoda M, Kita J, Kato M, Park KH, Shiraki T. Effect of menatetrenone, a vitamin k2 analog, on recurrence of hepatocellular carcinoma after surgical resection: a prospective randomized controlled trial. Anticancer Res. 2012;32(12):5415 – 5420.
18
Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Canc J Clin. 2011;61:69 – 90. Lau W, Kennedy A, Kim Y, et al. Patient Selection and Activity Planning Guide for Selective Internal Radiotherapy With Yttrium-90 Resin Microspheres. Int J Rad Onc Biol Phys 2012;82(1):401 – 407 Kosmider S, Tan TH, Yip D, Dowling R, Lichtenstein M, Gibbs P.Radioembolization in combination with systemic chemotherapy as first-line therapy for liver metastases from colorectal cancer. J Vasc Interv Radiol. 2011;22(6):780 – 6. Lencioni R, Chen XP, Dagher L, Venook AP. Treatment of intermediate/advanced hepatocellular carcinoma in the clinic: How can outcomes be improved? Oncologist. 2010;15(suppl 4):42 – 52. Lencioni R, Crocetti L. Local-regional treatment of hepatocellular carcinoma. Radiology. 2012;262:43 – 58. Lencioni R, Petruzzi P, Crocetti L. Chemoembolization of hepatocellular carcinoma. Semin Intervent Radiol. 2013;30(1):3 – 11. Lewandowski RJ, Geschwind JF, Liapi E, Salem R. Transcatheter intraarterial therapies: Rationale and overview. Radiology. 2011;259:641 – 657. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378 –390. Maheshwari S, Sarraj A, Kramer J, El-Serag HB. Oral contraception and the risk of hepatocellular carcinoma. J Hepatol. 2007;47:506 – 513. Maluccio M, Covey AM, Gandhi R, et al. Comparison of survival rates after bland arterial embolization and ablation versus surgical resection for treating solitary hepatocellular carcinoma up to 7 cm. J Vasc Interv Radiol 2005;16:955 – 961. Marrero JA, Fontana RJ, Fu S, et al. Alcohol, tobacco and obesity are synergistic risk factors for hepatocellular carcinoma. J Hepatol. 2005;42:218 – 224. Memon K, Lewandowski RJ, Riaz A, Salem R. Yttrium 90 microspheres for the treatment of hepatocellular carcinoma. Recent Results Cancer Res. 2013;190:207 – 24. Miyake Y, Kobashi H, Yamamoto K. Meta-analysis: The effect of interferon on development of hepatocellular carcinoma in patients with chronic hepatitis B virus infection. J Gastroenterol. 2009;44:470 – 475. Onaca N, Davis GL, Jennings LW, Goldstein RM, Klintmalm GB. Improved results of transplantation for hepatocellular carcinoma: a report from the International Registry of Hepatic Tumors in Liver Transplantation. Liver Transpl. 2009;15(6):574 – 80.
19
Rathmann N, Diehl SJ, Dinter D, et al. Radioembolization in patients with progressive gastrointestinal stromal tumor liver metastases undergoing treatment with tyrosine kinase inhibitors. J Vasc Interv Radiol. 2015;26(2):231 – 8. Salem R, Lewandowski R, Mulcahy M, et al. Radioembolization for Hepatocellular Carcinoma Using Yttrium-90 Microspheres: A Comprehensive Report of Long-term Outcomes. Imaging and Advanced Technology. 2010;138(1), 52 – 64. Samuel M, Chow PK, Chan Shih-Yen E, Machin D, Soo KC. Neoadjuvant and adjuvant therapy for surgical resection of hepatocellular carcinoma. Cochrane Database Syst Rev. 2009;(1):CD001199. Sangro B, Carpanese L, Cianni R, et al. European Network on Radioembolization with Yttrium-90 Resin Microspheres (ENRY) (2011), Survival after yttrium-90 resin microsphere radioembolization of hepatocellular carcinoma across Barcelona clinic liver cancer stages: A European evaluation. Hepatology, 54: 868 – 878. Santoro A, Rimassa L, Borbath I, et al. Tivantinib for second-line treatment of advanced hepatocellular carcinoma: a randomised, placebo-controlled phase 2 study. Lancet Oncol. 2013;14(1):55 – 63. Shen Q, Fan J, Yang XR, et al. Serum DKK1 as a protein biomarker for the diagnosis of hepatocellular carcinoma: a large-scale, multicentre study. Lancet Oncol. 2012;13(8):817 – 826. Siegel AB, Cohen EI, Ocean A, et al. Phase II trial evaluating the clinical and biologic effects of bevacizumab in unresectable hepatocellular carcinoma. J Clin Oncol. 2008;26:2992 – 2998. Spreafico C, Cascella T, Facciorusso A, et al. Transarterial chemoembolization for hepatocellular carcinoma with a new generation of beads: Clinical-radiological outcomes and safety profile. Cardiovasc Intervent Radiol. 2015;38(1):129 – 134. Thomas MB, Morris JS, Chadha R, et al. Phase II trial of the combination of bevacizumab and erlotinib in patients who have advanced hepatocellular carcinoma. J Clin Oncol. 2009;27:843 – 850. Toh HC, Chen PJ, Carr BI, et al. Phase 2 trial of linifanib (ABT-869) in patients with unresectable or metastatic hepatocellular carcinoma. Cancer. 2013;119(2):380 – 387. Uhm JE, Park JO, Lee J, et al. A phase II study of oxaliplatin in combination with doxorubicin as first-line systemic chemotherapy in patients with inoperable hepatocellular carcinoma. Cancer Chemother Pharmacol. 2009;63:929 – 935. Van Hazel G, Blackwell A, Anderson J, et al. Randomised phase 2 trial of SIR-Spheres plus fluorouracil/leucovorin chemotherapy versus fluorouracil/leucovorin chemotherapy alone in advanced colorectal cancer. J Surg Oncol. 2004,1;88(2):78 – 85. Weber S, Jarnagin W, Duffy A, et al. Liver and bile duct cancer. In: Abeloff MD, Armitage JO, Lichter AS, Niederhuber JE. Kastan MB, McKenna WG, eds. Clinical Oncology. 4th ed. Philadelphia, Pa: Elsevier; 2008:1569 – 1579.
20
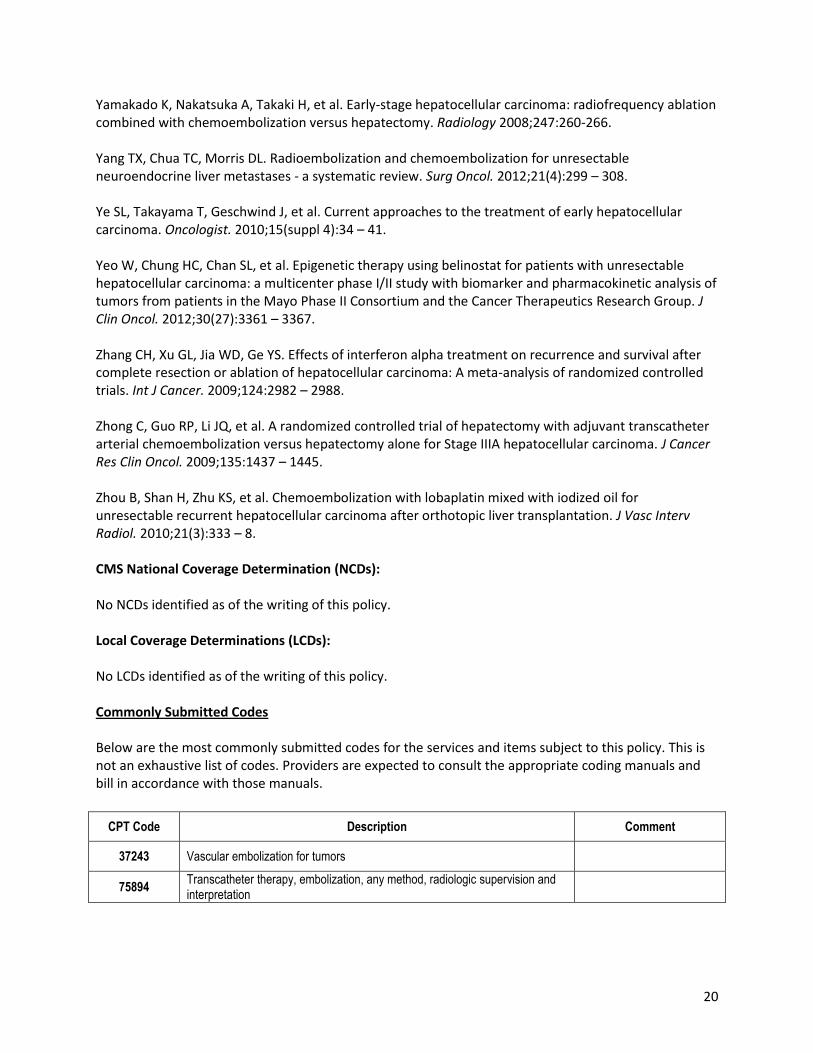
Yamakado K, Nakatsuka A, Takaki H, et al. Early-stage hepatocellular carcinoma: radiofrequency ablation combined with chemoembolization versus hepatectomy. Radiology 2008;247:260-266. Yang TX, Chua TC, Morris DL. Radioembolization and chemoembolization for unresectable neuroendocrine liver metastases - a systematic review. Surg Oncol. 2012;21(4):299 – 308. Ye SL, Takayama T, Geschwind J, et al. Current approaches to the treatment of early hepatocellular carcinoma. Oncologist. 2010;15(suppl 4):34 – 41. Yeo W, Chung HC, Chan SL, et al. Epigenetic therapy using belinostat for patients with unresectable hepatocellular carcinoma: a multicenter phase I/II study with biomarker and pharmacokinetic analysis of tumors from patients in the Mayo Phase II Consortium and the Cancer Therapeutics Research Group. J Clin Oncol. 2012;30(27):3361 – 3367. Zhang CH, Xu GL, Jia WD, Ge YS. Effects of interferon alpha treatment on recurrence and survival after complete resection or ablation of hepatocellular carcinoma: A meta-analysis of randomized controlled trials. Int J Cancer. 2009;124:2982 – 2988. Zhong C, Guo RP, Li JQ, et al. A randomized controlled trial of hepatectomy with adjuvant transcatheter arterial chemoembolization versus hepatectomy alone for Stage IIIA hepatocellular carcinoma. J Cancer Res Clin Oncol. 2009;135:1437 – 1445. Zhou B, Shan H, Zhu KS, et al. Chemoembolization with lobaplatin mixed with iodized oil for unresectable recurrent hepatocellular carcinoma after orthotopic liver transplantation. J Vasc Interv Radiol. 2010;21(3):333 – 8. CMS National Coverage Determination (NCDs): No NCDs identified as of the writing of this policy. Local Coverage Determinations (LCDs): No LCDs identified as of the writing of this policy. Commonly Submitted Codes Below are the most commonly submitted codes for the services and items subject to this policy. This is not an exhaustive list of codes. Providers are expected to consult the appropriate coding manuals and bill in accordance with those manuals.
CPT Code Description Comment
37243 Vascular embolization for tumors
75894 Transcatheter therapy, embolization, any method, radiologic supervision and interpretation
21
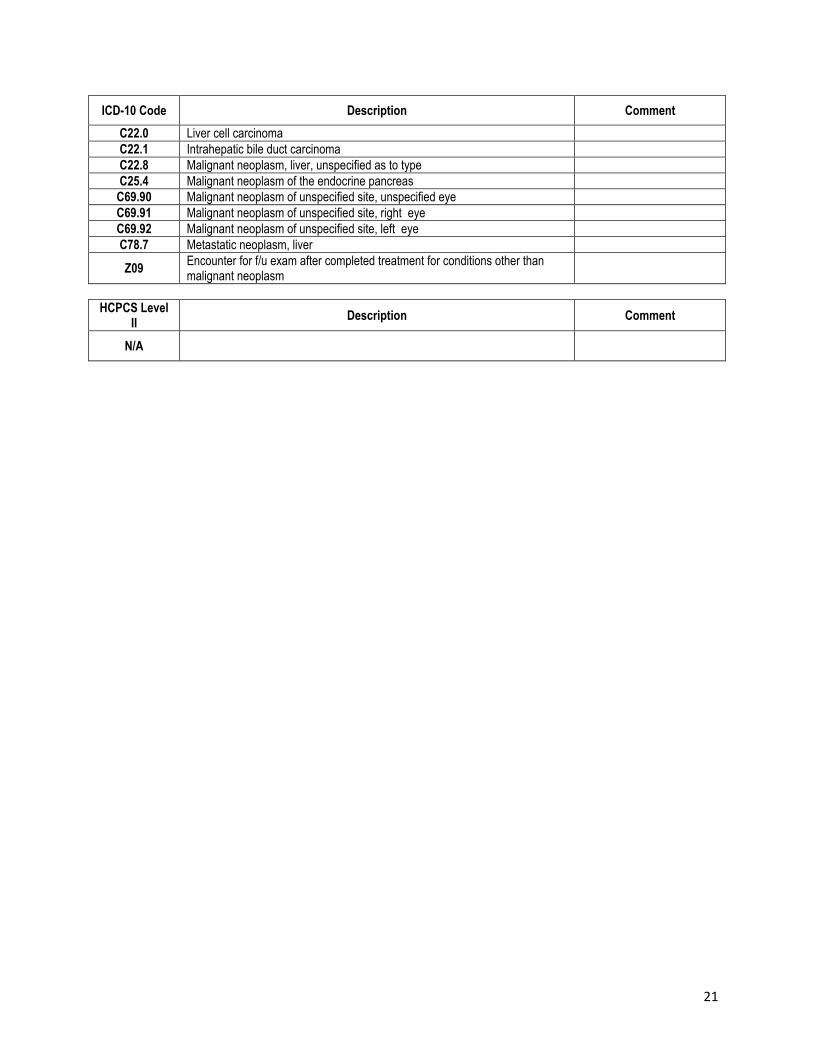
ICD-10 Code Description Comment
C22.0 Liver cell carcinoma
C22.1 Intrahepatic bile duct carcinoma
C22.8 Malignant neoplasm, liver, unspecified as to type
C25.4 Malignant neoplasm of the endocrine pancreas
C69.90 Malignant neoplasm of unspecified site, unspecified eye
C69.91 Malignant neoplasm of unspecified site, right eye
C69.92 Malignant neoplasm of unspecified site, left eye
C78.7 Metastatic neoplasm, liver
Z09 Encounter for f/u exam after completed treatment for conditions other than malignant neoplasm
HCPCS Level II
Description Comment
N/A





























