Embed Size (px)
Citation preview
1054 I.J. Radiation Oncology • Biology • Physics May 1988, Volume 14, Number 5
2. "The analysis included patients improperly assigned to treatment
Response: Fifty-five patients were assigned to radiation therapy. Three patients refused radiation therapy and demanded surgery. These three patients, as they received surgery, were analyzed as if they were random- ized to receive surgery. Forty-two patients were randomized to receive radical surgery. Four patients refused radical surgery and demanded ra- diation. These four patients who received radiation were analyzed as if they had been randomized to radiation therapy. Thus the two populations which were ultimately randomized were the 55 who were randomized to radiation therapy, minus the three who demanded surgery, plus the four randomized to surgery who demanded radiation for a total of 56. The number for radical surgery are calculated as follows: 42 minus 4 plus 3 for a total of 41. The statistician for the study debated as to whether the patients who were randomized to one treatment but who received another should be analyzed according to their randomization or analyzed by their t reatment received. The decision was made to analyze by the treatment received since the study was to examine the relative impact of the two treatments rather than the relative impact of the randomization assignment.
3. "There were unacceptable deletions from the surgical arm."
Response. • Local recurrence did not constitute failure in this study. Patients who received radiation who had biopsy proven persistent disease after definitive radiation therapy, were not identified as failures.
4. "'There was an unacceptabh, rate o f lost patients."
Response: Further follow-up at 80 months continued to demonstrate relative benefit of surgery over radiation.
5. "'The input of the uro-oncology group radiation therapy committee
Response• • The protocol did not require blind biopsies of patients ran- domized to surgery to determine whether or not local disease was present. It does not seem proper to blindly biopsy patients following radical surgery when they can be adequately monitored by digital examination for local recurrent disease. Furthermore, local disease did not constitute failure.
6. "The endpoint selected was inappropriate to evaluate t h e . . . "
Response." The use of first evidence of disease recurrence has become an accepted modality for evaluating impact of treatment designed for control of early stage disease. As first evidence of distant disease recurrence was equivalently applied to both treatment groups, to deny that the endpoint selected was inappropriate serves only to support the bias of the radio- therapist.
7. "The rate of metastasis in the radiation group was c o n s i s t e n t . . . "
Response•" One can only state that the volume of diseasc was equivalent in both the radiation therapy arm and the radical prostatectomy arm. It is interesting that a later publication from this same cooperative group that examined the impact of radiation therapy vs. no treatment for node negative stage disease indicated that the failure rates were equivalent in both the actively treated by radiation therapy arm and the arm that did not receive treatment but which was observed only (Paulson, D. F., Hodge, G. B. Jr., Hinshaw, W. and Uro-Oncology Research Group: Radiation therapy vs. delayed androgen deprivation for stage C carcinoma of the prostate. J Urol 131: 901-902, 1984). These studies would indicate that the reported impact of radiation may be nothing other than the observed natural history of node negative Stage T3 adenocarcinoma of the prostate.
8. "The results obtained with the surgical group are similar o r . . . "
Response: The studies referred to in reference 6 are studies in which the patients were selected retrospectively to optimize their treatment response. Similarly selected patients who underwent radical surgery demonstrate a benefit to radical surgery greater than that achieved in the randomized arm. This only serves to confirm that retrospective analysis of a patient population can produce treatment results equivalent to the bias of the authors.
9..','Morbidity was not reported in this study which is quoted a s . . . "
Response: Morbidity was not analyzed.
DAVID F. PAULSON, M.D. Div. of Urologic Surgery Duke University Med. Ctr. Durham, NC 27710
RADIOBIOLOGICAL IMPLICATIONS OF FRACTIONATED L O W DOSE RATE IRRADIATION
To the Editor." Recently, Pierquin and coworkers 5 presented updated results from a trial on low dose rate (LDR) irradiation of the oropharynx. 4 In this trial a comparison was made between conventional high dose rate (HDR) fractionated irradiation (45 Gy given as 25 fractions in 35 days, followed at day 40 by a boost of 25 Gy in 18 fractions), and frac- tionated LDR irradiation (also 45 Gy, but now given as 7 fractions of 6-7 Gy at approximately 1 Gy/hr in 10 days, again followed at day 40 by a LDR boost of 25 Gy in 4 fractions). Their main finding was that less recurrences and more late normal-tissue damage were seen in the patients treated with LDR than in the group treated with conventional HDR radiotherapy.
In this note we present radiobiological considerations, based upon the linear-quadratic (LQ) model,l which may explain some of these results, and highlight a potential danger from this sort of LDR treatment. This seems appropriate, because Pierquin et al. 4"5 touch only lightly on the radiobiological differences between the two treatment modalities. Frac- tionated LDR irradiation as used by Pierquin et al. 4'5 has two conflicting characteristics. On the one hand LDR irradiation can be regarded as the limit of hyperfractionation, and hence it should preferentially spare tissues with low a/fl ratios (late responding normal tissue or NT), compared to tissues with high a/fl values ( tumor tissue or TT). On the other hand, a fractionated LDR treatment can also be considered as consisting of large
CO
Q) U]
0 ID
0 >
4~ C) Q]
q-
Q]
100.
50
25 HDR f r a c t i o n s /
(~/ /J = 10 Gy
0 ' ' o : 4 . . . . . ' ' . . . . . 1'o
r e p a k r h a l f t i m e (h)
200
150 ul o 1:3
> 100 -,--I
r..) 4 - -
4- 50
0 0 .1
7 LDR f r a c t i o n s /
= 1 o Gy
' 0 : 4 . . . . . ' ' , i . . . . .
r e p a i r h a l f t - ~ m e (h)
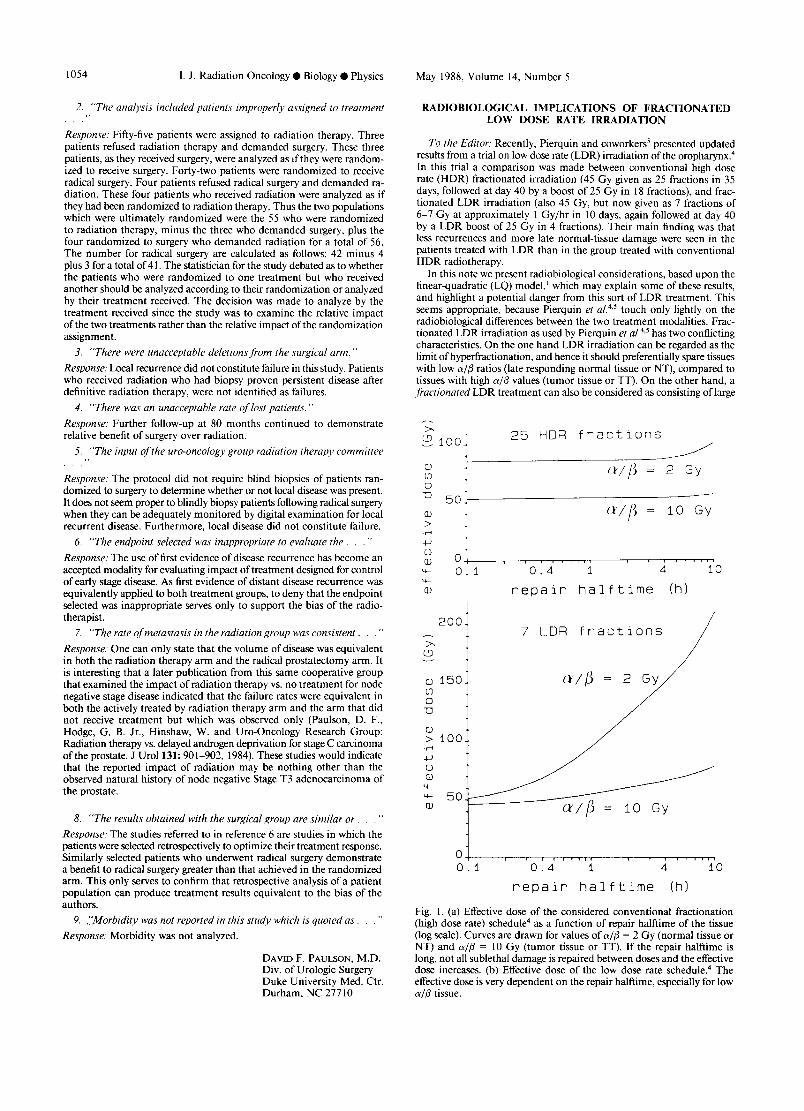
Fig. I. (a) Effective dose of the considered conventional fractionation (high dose rate) schedule 4 as a function of repair halftime of the tissue (log scale). Curves are drawn for values ofa /B = 2 Gy (normal tissue or NT) and a/~ = l0 Gy (tumor tissue or TT). If the repair halftime is long, not all sublethal damage is repaired between doses and the effective dose increases. (b) Effective dose of the low dose rate schedule. 4 The effective dose is very dependent on the repair halftime, especially for low ~/3 tissue.
Correspondence 1055
fractions (7 fractions of 6.4 Gy in the considered case), which would tend to increase, preferentially, damage to low a i r tissues. This apparent contradiction disappears if the rate o f repair of sublethal damage (SLD) is taken into account. If the repair process is very slow, the LDR fractions are equivalent to large H D R fractions, because the sublethal damage is hardly repaired during an L DR session. If the repair process is very fast, however, in comparison to the length of the L DR session, the effect of LDR irradiation resembles that of a hyperfractionated treatment, because all inflicted SLD is repaired almost instantaneously. We have quantitated these remarks and applied them to the trial of Pierquin et al. The approach of Dale 2'3 has been used to compare the relative effectiveness of LDR and conventional H D R fractionation. To simplify the calculation we have discussed only the initial 45-Gy treatment. The conclusions from our calculations are also valid for the total irradiation schemes including the successive boosts. Two types of tissue are considered, characterized by a/fl = 2 Gy (late responding NT) and a/fl = 10 Gy (TT), respectively. Qualitatively similar results would be obtained if other values for a/fl were assumed, as long as the a/fl ratio of the T T is larger than the one of the NT. Note that, the effectiveness of the different treatment modalities depends strongly on the rates of repair of SLD in NT and TT. The little quantitative information that is available on halftimes of repair suggests values of around 0.8 hr for early responding (high a/fl) NT and of around 1.4 hr for late responding (low a/fl) NT. s
The Effective Dose (ED) of the conventionally fractionated H D R treatment is given in the LQ model by:
ED = D(1 + d/(a/fl)), (1)
where D is the total dose and d the dose per fraction. For 45 Gy in 25 fractions 4 this amounts to ED = 85.5 Gy for a/fl = 2 Gy (NT) and ED = 53.1 Gy for c~/fl = 10 Gy (TT). This equation is only valid if the halftime of repair (Tu2) of SLD is much shorter than the time between successive fractions (24 hr in this case). If for a certain tissue Tt/2 is longer than, say, 6 hr, not all SLD inflicted during a fraction is repaired before the next fraction is given and the Effective Dose becomes higher. 3'7 Figure la shows the variation of ED as a function of T~/2 both for NT (a/fl = 2 Gy) and for TT (a/f l = 10 Gy). For damage to late responding tissue, ED lies between 85.5 Gy for Tu2 = 0.1 hr and 99.9 Gy for Tu2 = 10 hr, whereas for tumor the range of values is smaller.
The Effective Dose ED corresponding to fractionated LDR treat- ment is2:
ED = D{ 1 + (2R/lz)(fl/a)[1 - { 1 - exp(-u.T)}/(u.T)]}, (2)
~2.0 o
> .4 1.5 43 0 G.)
O0 >
-r"4
4 ~ 0 5 © •
a.l £..
0 . 0 0 1
pat io L D R / H D ~
' ' 0 ' . 4 . . . . . ] ' ~ . . . . . ~'o
PepaiP halftime fhl
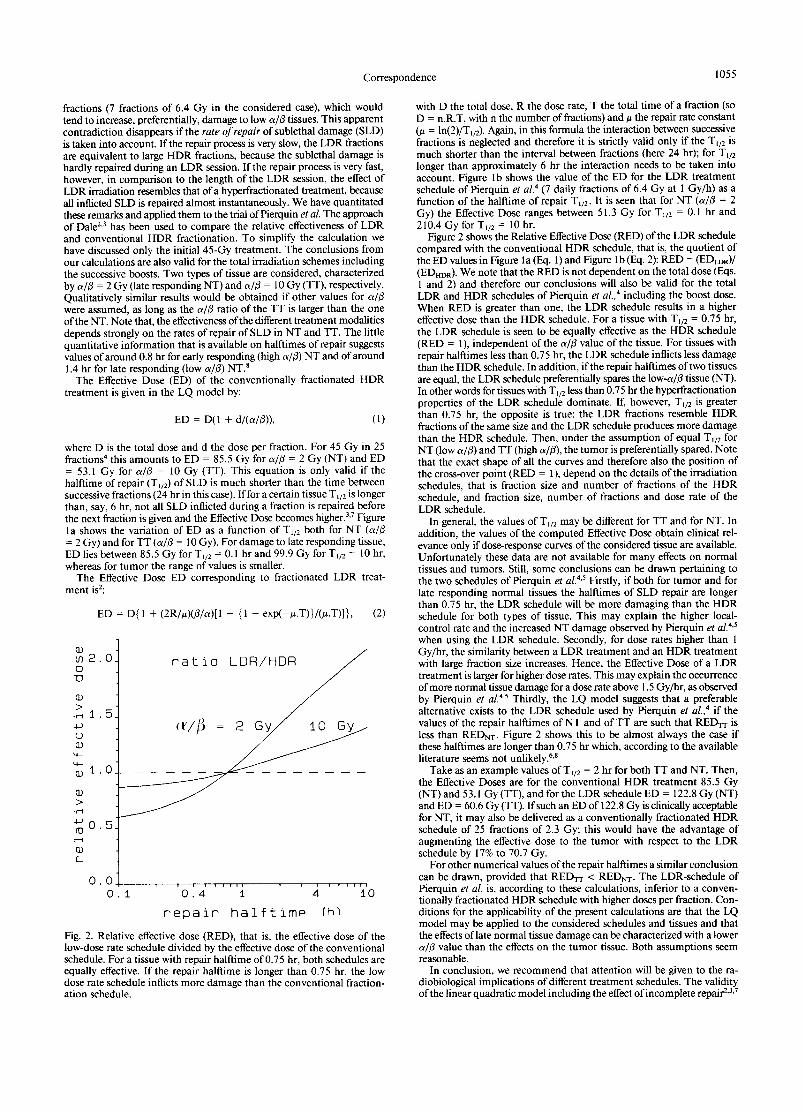
Fig. 2. Relative effective dose (RED), that is, the effective dose of the low-dose rate schedule divided by the effective dose of the conventional schedule. For a tissue with repair halflime of 0.75 hr, both schedules are equally effective. If the repair halftime is longer than 0.75 hr, the low dose rate schedule inflicts more damage than the conventional fraction- ation schedule.
with D the total dose, R the dose rate, T the total t ime of a fraction (so D = n.R.T, with n the number of fractions) and u the repair rate constant (# = ln(2)/Tu2 ). Again, in this formula the interaction between successive fractions is neglected and therefore it is strictly valid only if the Tt/2 is much shorter than the interval between fractions (here 24 hr); for T~/2 longer than approximately 6 hr the interaction needs to be taken into account. Figure lb shows the value of the ED for the LDR treatment schedule of Pierquin et aL 4 (7 daily fractions of 6.4 Gy at 1 Gy/h) as a function of the halftime of repair T,/2. It is seen that for NT (a/fl = 2 Gy) the Effective Dose ranges between 51.3 Gy for Tu2 = 0.1 hr and 210.4 Gy for Tu2 = 10 hr.
Figure 2 shows the Relative Effective Dose (RED) of the LDR schedule compared with the conventional H D R schedule, that is, the quotient of the ED values in Figure la (Eq. 1) and Figure lb (Eq. 2): RED = (EI~DR)/ (EDHDR)- We note that the RED is not dependent on the total dose (Eqs. 1 and 2) and therefore our conclusions will also be valid for the total LDR and H D R schedules of Pierquin et al., 4 including the boost dose. When RED is greater than one, the LDR schedule results in a higher effective dose than the H D R schedule. For a tissue with Tu2 = 0.75 hr, the LDR schedule is seen to be equally effective as the H D R schedule (RED = 1), independent of the a/fl value of the tissue. For tissues with repair halftimes less than 0.75 hr, the LDR schedule inflicts less damage than the H D R schedule. In addition, if the repair halftimes of two tissues are equal, the LDR schedule preferentially spares the low-a/fl tissue (NT). In other words for tissues with Tl/2 less than 0.75 hr the hyperfractionation properties of the LDR schedule dominate. If, however, Tu2 is greater than 0.75 hr, the opposite is true: the LDR fractions resemble H D R fractions of the same size and the LDR schedule produces more damage than the HDR schedule. Then, under the assumption of equal T,/2 for NT (low a i r ) and TT (high air) , the tumor is preferentially spared. Note that the exact shape of all the curves and therefore also the position of the cross-over point (RED = 1), depend on the details of the irradiation schedules, that is fraction size and number of fractions of the H D R schedule, and fraction size, number of fractions and dose rate of the LDR schedule.
In general, the values of T~/2 may be different for TT and for NT. In addition, the values of the computed Effective Dose obtain clinical rel- evance only if dose-response curves of the considered tissue are available. Unfortunately these data are not available for many effects on normal tissues and tumors. Still, some conclusions can be drawn pertaining to the two schedules of Pierquin et al. 4'5 Firstly, if both for tumor and for late responding normal tissues the halftimes of SLD repair are longer than 0.75 hr, the LDR schedule will be more damaging than the H D R schedule for both types of tissue. This may explain the higher local- control rate and the increased NT damage observed by Pierquin et a[. 4"5 when using the LDR schedule. Secondly, for dose rates higher than 1 Gy/hr, the similarity between a LDR treatment and an H D R treatment with large fraction size increases. Hence, the Effective Dose of a LDR treatment is larger for higher dose rates. This may explain the occurrence of more normal tissue damage for a dose rate above 1.5 Gy/hr, as observed by Pierquin et al. 4'5 Thirdly, the LQ model suggests that a preferable alternative exists to the LDR schedule used by Pierquin et al., 4 if the values of the repair halftimes of NT and of TT are such that REDrr is less than REDNT. Figure 2 shows this to be almost always the case if these halftimes are longer than 0.75 hr which, according to the available literature seems not unlikely. 6'8
Take as an example values ofTu2 = 2 hr for both TT and NT. Then, the Effective Doses are for the conventional H D R treatment 85.5 Gy (NT) and 53.1 Gy (TT), and for the LDR schedule ED = 122.8 Gy (NT) and ED = 60.6 Gy (TT). If such an ED of 122.8 Gy is clinically acceptable for NT, it may also be delivered as a conventionally fractionated H D R schedule of 25 fractions of 2.3 Gy; this would have the advantage of augmenting the effective dose to the tumor with respect to the LDR schedule by 17% to 70.7 Gy.
For other numerical values of the repair halftimes a similar conclusion can be drawn, provided that REDrr < REDrcr. The LDR-schedule of Pierquin et al. is, according to these calculations, inferior to a conven- tionally fractionated H D R schedule with higher doses per fraction. Con- ditions for the applicability of the present calculations are that the LQ model may be applied to the considered schedules and tissues and that the effects of late normal tissue damage can be characterized with a lower a/fl value than the effects on the tumor tissue. Both assumptions seem reasonable.
In conclusion, we recommend that attention will be given to the ra- diobiological implications of different treatment schedules. The validity of the linear quadratic model including the effect of incomplete repair 2'3'7

1056 I .J . Radiation Oncology • Biology • Physics May 1988, Volume 14, Number 5
is still under discussion, but this model can adequately describe many data sets and would therefore seem sufficiently mature to be consulted if trials concerning fractionation are under development. The importance of such considerations is indicated by our calculations showing the po- tential dangers of overdosing late reacting normal tissues with some LDR schedules. However, more knowledge on the repair halftimes of sublethal damage in irradiated tissues is badly needed to make more definitive statements.
ROEL W. DEBOER, PH.D. Joos V. LEBESQUE, PH.D., M.D. Department of Radiotherapy The Netherlands Cancer Institute (Antoni van Leeuwenhoek Huis) Plesmanlaan 121 1066 CX Amsterdam The Netherlands
1. Barendsen, G.W.: Dose fractionation, dose rate and iso-effect rela- tionships for normal tissue responses. Int. J. Radiat. Oncol. BioL Phys. 8: 1981-1997, 1982.
2. Dale, R.G.: The application of the linear-quadratic dose-effect equa- tion to fractionated and protracted radiotherapy. Br. Z RadioL 58: 515-528, 1985.
3. Dale, R.G.: The application of the linear-quadratic model to frac- tionated radiotherapy when there is incomplete normal tissue re- covery between fractions, and possible implications for treatments involving multiple fractions per day. Br. ,L Radiol. 59: 919-927, 1986.
4. Pierquin, B., Calitchi, E., Mazeron, J.J., Le Bourgeois, J.P., Leung, S.: A comparison between low dose rate radiotherapy and conven- tionally fractionated irradiation in moderately extensive cancers of the oropharynx. Int. J. Radiat. Oncol. BioL Phys. 11:431-439, 1985.
5. Pierquin, B., Calitchi, E., Mazeron, J.J., Le Bourgeois, J.P., Leung, S.: Update on low dose rate irradiation for cancer of the oropharynx- May 1986. Int. J. Radiat. OncoL Biol. Phys. 13: 259-261, 1987.
6. Rojas, A., Joiner, M.C., Ninis, J., Johns, H.: The influence of dose per fraction on the repair kinetics of tumors and normal tissues in mice (Abstr.). 6th Annual Meeting of the Eur. Soc. Therap. Radiol. Oncol. Lisboa 1987. (ESTRO) p. 12 1987.
7. Thames, H.D.: An 'incomplete-repair ' model for survival after frac- tionated and cont inuous irradiations. Int. Z Radiat. Biol. 47: 319- 339, 1985.
8. Thames, H.D., Hendry, J.H.: Fractionation in Radiotherapy, Chapter 3.4. London, Taylor and Francis. 1987.
The final judgement could only arise from a continuation of a clinical trial with an adjustment of the total dose aiming at matching for the two regimens one of the two effects of importance.
BERNARD PIERQUIN JEAN JACQUES MAZERON Dept. de Carcinologie Centre Hospitalo-Universitaire Henri Mondor 51, Avenue du Marrchal de Lattre de Tassigny 94000 Creteil France
TOXICITY AND A M I O D A R O N E
To the Editor: We were interested to read the correspondence from Demange et al., ~ describing acute mucosal toxicity in a patient receiving local radiotherapy while taking Amiodarone. We would like to describe a similar case.
A 77-year old man presented with a variably differentiated squamous cell carcinoma of the tonsil with cervical lymphadenopathy. After re- ceiving 26 Gy in 2 Gy daily fractions, (conventional 6°Co therapy) he developed severe mucositis. Such reactions have only been observed in our department at much higher doses. We were unable to find a cause for such a reaction.
After 8 days' rest there had been no improvement. The only medication he had been taking during his treatment was Amiodarone 200 mgms daily which he had been on for 1 year for myocardial dysrythmia. We decided to stop the Amiodarone and after 4 days his mouth had much improved. Radiotherapy was restarted to a total of 60 Gy with no further problems.
Amiodarone is being prescribed with increasing frequency for myo- cardial dysrhythmia, consequently the number of radiotherapy patients receiving Amiodarone is rising. It is therefore important that a possible radiosensitization is recognized in these patients and great care taken.
C. TOPHAM, FRCR J. BRIERLEY, M.Sc., MRCP H. TOMLINSON, M.P.S. The Regional Centre for Radiotherapy and Oncology Southwest Surrey Health Authority St. Luke's Hospital Warren Road Guildford Surrey GU 13NT England
R E B UT T AL
To the Editor: In their correspondence, R. W. DEBOER and J. g . LEBESQUE develop some theoretical calculations on radiobiological implications of fractionated low dose rate irradiation, about our paper ("Update on low dose rate irradiation for cancer of the Oropha rynx" - - Int. J. Radiat. Oncol. 13- -259-261- -1987) .
The main finding of our clinical study was that less recurrences and more late normal-tissue damage were seen in the patients treated with LDR than in the group treated with conventional H D R radiotherapy. The straight forward conclusion is that the L DR regimen was much more efficient (84% of local control for LDR, versus 39% for HDR) than the H D R regimen for the cure rate. On the other hand, the normal tissue damage is more important with L DR (16% of necrosis for LDR versus 0% for HDR). No absolute conclusion can be drawn on the differential effect between the two types of tissues.
Theoretical computation suggested either no differential effect or some differential effect on one direction or the other, depending on the values ascribed to the radiobiological parameters which are accessible. The computat ion made by R. W. DEBOER and J. V. LEBESQUE is based on a simple modal taking only into account the amoun t of SLD repair (a/13 parameters) and the kinetics of the repair (T½ parameter).
The differences in overall t ime of the first part of the t reatment (45 Gy in IO d. for LDR and in 35 d. for HDR) has not been considered. In our opinion, the total duration of the protraction is a major factor. We appreciate the value of the theoretical computat ion in the analysis of the clinical results. However we doubt that they allow a definitive statement of the relative therapeutic merits of the two regimens compared in our study.
1. Demange, L., Marechal, F., Nguyen, T.D.: Could amiodarone in- crease acute cutaneous and mucosal toxicity of radiotherapy? Int. ~L Radiat. Oncol. Biol. Phys. 13: 289, 1987.
BLOOD F L O W VALUES
To the Editor. Recently, Groebe et at. ~ published a manuscript dis- cussing the suitability of dividing heated tissue into temperature equiv- alent zones for estimation of tissue blood flow from thermal clearance curves. The authors disagree with our previously published data 2 de- scribing a mathematical model which divides tissue into a series of tem- perature equivalent zones for prediction of blood flow during the cooling of tissue. They raised a point that selection of the number of zones is arbitrary and that any blood flow can be achieved by selection of a dif- ferent number of zones. In our model we used radioactive microspheres to calculate the number of isothermal zones for this specific geometry.
The authors are correct with their conclusion that the perfusion rates change as a function of the number of isothermal zones. We believe that they are incorrect in their conclusion that the model is inappropriate for use. We have done, and are continuing to do, studies which compare blood flow values calculated from mathematical models with blood flow values calculated by other techniques (radioactive microspheres, laser doppler flowimetry, etc.). We are continuing to develop this model which is more predictive of the type of thermal decay seen in tissue. One thing is clear; the thermal washout in tissue is not a pure exponential function.
The main point that the authors make is, as the number of zones increase, the temperature in the center of the heated volume will not decrease with time during the thermal washout period. They state that,





























