Embed Size (px)
Citation preview
A11GAGA ABSTRACTS GASTROENTEROLOGY Vol. 118, No.4
table 1
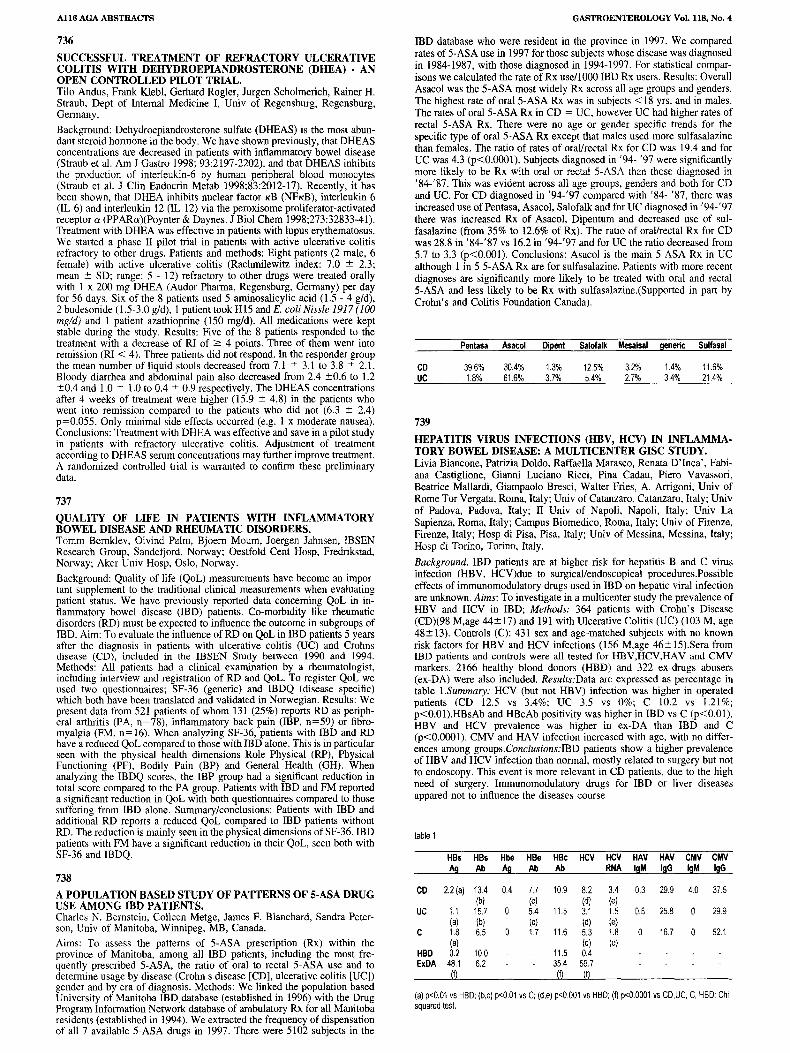
HBs HBs Hbe HBe HBc HCV HCV HAV HAV CMV CMVAg Ab Ag Ab Ab RNA IgM IgG IgM IgG
CD 2.2(al 134 0.4 7.7 10.9 8.2 34 0.3 29.9 40 37.5(b) (e) (dJ (e)
UC 1.1 15.7 0 5.4 115 3.1 15 0.6 25.8 0 29.9(a) (b) (e) (d) (e)
C 1.8 6.5 17 11.6 5.3 18 16.7 52.1(a) (d) (e)
HBD 02 10.0 11.5 0.4ExDA 48.1 6.2 354 59.7
m m (f)
(a)p<0.01 vsHBD; (b,c) p<0.01 vsC;(d,e) p<0.001 vsHBD; (f)p<O.0001 vsCD,UC, C,HBD; Chisquared test.
IBD database who were resident in the province in 1997. We comparedrates of 5-ASA use in 1997 for those subjects whose disease was diagnosedin 1984-1987, with those diagnosed in 1994-1997. For statistical comparisons we calculated the rate of Rx use/1OooIBD Rx users. Results: OverallAsacol was the 5-ASA most widely Rx across all age groups and genders.The highest rate of oral 5-ASA Rx was in subjects < 18 yrs, and in males.The rates of oral 5-ASA Rx in CD = UC, however UC had higher rates ofrectal 5-ASA Rx. There were no age or gender specific trends for thespecific type of oral 5-ASA Rx except that males used more sulfasalazinethan females. The ratio of rates of oral/rectal Rx for CD was 19.4 and forUC was 4.3 (p<O.OOOI). Subjects diagnosed in '94- '97 were significantlymore likely to be Rx with oral or rectal 5-ASA than those diagnosed in'84-'87. This was evident across all age groups, genders and both for CDand Uc. For CD diagnosed in '94-'97 compared with '84- '87, there wasincreased use of Pentasa, Asacol, Salofalk and for UC diagnosed in '94-'97there was increased Rx of Asacol, Dipentum and decreased use of sulfasalazine (from 35% to 12.6% of Rx). The ratio of oral/rectal Rx for CDwas 28.8 in '84-'87 vs 16.2 in '94-'97 and for UC the ratio decreased from5.7 to 3.3 (p<O.OOI). Conclusions: Asacol is the main 5-ASA Rx in UCalthough 1 in 5 5-ASA Rx are for sulfasalazine. Patients with more recentdiagnoses are significantly more likely to be treated with oral and rectal5-ASA and less likely to be Rx with sulfasalazine.(Supported in part byCrohn's and Colitis Foundation Canada).
739HEPATITIS VIRUS INFECTIONS (HBV, HCV) IN INFLAMMATORY BOWEL DISEASE: A MULTICENTER GISC STUDY.Livia Biancone, Patrizia Doldo, Raffaella Marasco, Renata D'Inca', Fabiana Castiglione, Gianni Luciano Ricci, Pina Cadau, Piero Vavassori,Beatrice Mallardi, Giampaolo Bresci, Walter Fries, A. Arrigoni, Univ ofRome Tor Vergata, Roma, Italy; Univ of Catanzaro, Catanzaro, Italy; Univof Padova, Padova, Italy; II Univ of Napoli, Napoli, Italy; Univ LaSapienza, Roma, Italy; Campus Biomedico, Roma, Italy; Univ of Firenze,Firenze, Italy; Hosp di Pisa, Pisa, Italy; Univ of Messina, Messina, Italy;Hosp di Torino, Torino, Italy.
Background. IBD patients are at higher risk for hepatitis Band C virusinfection (HBV, HCV)due to surgicallendoscopical procedures.Possibleeffects of immunomodulatory drugs used in IBD on hepatic viral infectionare unknown. Aims: To investigate in a multicenter study the prevalence ofHEV and HCV in IBD; Methods: 364 patients with Crohn's Disease(CD)(98 M,age 44± 17) and 191 with Ulcerative Colitis (UC) (103 M, age48± 13). Controls (C): 431 sex and age-matched subjects with no knownrisk factors for HBV and HCV infections (156 M,age 46± 15).Sera fromIBD patients and controls were all tested for HEV,HCV,HAV and CMVmarkers. 2166 healthy blood donors (HBD) and 322 ex-drugs abusers(ex-DA) were also included. Results:Data are expressed as percentage intable I.Summary: HCV (but not HBV) infection was higher in operatedpatients (CD 12.5 vs 3.4%; UC 3.5 vs 0%; C 10.2 vs 1.21%;p<O.OI).HBsAb and HBeAb positivity was higher in IBD vs C (p<O.OI).HBV and HCV prevalence was higher in ex-DA than IBD and C(p<O.OOOI). CMV and HAV infection increased with age, with no differences among groups.Conclusions:IBD patients show a higher prevalenceof HBV and HCV infection than normal, mostly related to surgery but notto endoscopy. This event is more relevant in CD patients, due to the highneed of surgery. Immunomodulatory drugs for IBD or liver diseasesappared not to influence the diseases course.
Pentasa Asacol Dipent Salofalk Mesalsal generic Sulfasal
11.6%21.4%
1.4%3.4%
3.2%2.7%
12.5%5.4%
1.3%3.7%
30.4%61.6%
39.6%1.8%
CDUC
736
SUCCESSFUL TREATMENT OF REFRACTORY ULCERATIVECOLITIS WITH DEHYDROEPIANDROSTERONE (DHEA) • ANOPEN CONTROLLED PILOT TRIAL.Tilo Andus, Frank Klebl, Gerhard Rogier, Jurgen Scholmerich, Rainer H.Straub, Dept of Internal Medicine I, Univ of Regensburg, Regensburg,Germany.
Background: Dehydroepiandrosterone sulfate (DHEAS) is the most abundant steroid hormone in the body. We have shown previously, that DHEASconcentrations are decreased in patients with inflammatory bowel disease(Straub et al. Am J Gastro 1998; 93:2197-2202), and that DHEAS inhibitsthe production of interleukin-6 by human peripheral blood monocytes(Straub et al. J Clin Endocrin Metab 1998;83:2012-17). Recently, it hasbeen shown, that DHEA inhibits nuclear factor KB (NFKB), interleukin 6(IL-6) and interleukin 12 (IL-12) via the peroxisome proliferator-activatedreceptor a (PPARa)(Poynter & Daynes. J BioI Chern 1998;273:32833-41).Treatment with DHEA was effective in patients with lupus erythematosus.We started a phase II pilot trial in patients with active ulcerative colitisrefractory to other drugs. Patients and methods: Eight patients (2 male, 6female) with active ulcerative colitis (Rachmilewitz index: 7.0 ± 2.3;mean ± SD; range: 5 - 12) refractory to other drugs were treated orallywith 1 x 200 mg DHEA (Audor Pharma, Regensburg, Germany) per dayfor 56 days. Six of the 8 patients used 5-arninosalicylic acid (1.5 - 4 g/d),2 budesonide (1.5-3.0 g/d), I patient took H15 and E. coli Nissle 1917 (lOamgld) and I patient azathioprine (150 mg/d). All medications were keptstable during the study. Results: Five of the 8 patients responded to thetreatment with a decrease of RI of 2: 4 points. Three of them went intoremission (RI < 4). Three patients did not respond. In the responder groupthe mean number of liquid stools decreased from 7.1 ± 3.1 to 3.8 ± 2.1.Bloody diarrhea and abdominal pain also decreased from 2.4 ±0.6 to 1.2±0.4 and 1.0 ± 1.0 to 0.4 ± 0.9 respectively. The DHEAS concentrationsafter 4 weeks of treatment were higher (15.9 ± 4.8) in the patients whowent into remission compared to the patients who did not (6.3 ± 2.4)p=0.055. Only minimal side effects occurred (e.g. 1 x moderate nausea).Conclusions: Treatment with DHEA was effective and save in a pilot studyin patients with refractory ulcerative colitis. Adjustment of treatmentaccording to DHEAS serum concentrations may further improve treatment.A randomized controlled trial is warranted to confirm these preliminarydata.
737QUALITY OF LIFE IN PATIENTS WITH INFLAMMATORYBOWEL DISEASE AND RHEUMATIC DISORDERS.Tomm Bemklev, Oivind Palm, Bjoern Mourn, Joergen Jahnsen, IBSENResearch Group, Sandefjord, Norway; Oestfold Cent Hosp, Fredrikstad,Norway; Aker Univ Hosp, Oslo, Norway.
Background: Quality of life (QoL) measurements have become an important supplement to the traditional clinical measurements when evaluatingpatient status. We have previously reported data concerning QoL in inflammatory bowel disease (IBD) patients. Co-morbidity like rheumaticdisorders (RD) must be expected to influence the outcome in subgroups ofIBD. Aim: To evaluate the influence ofRD on QoL in IBD patients 5 yearsafter the diagnosis in patients with ulcerative colitis (UC) and Crohnsdisease (CD), included in the IBSEN Study between 1990 and 1994.Methods: All patients had a clinical examination by a rheumatologist,including interview and registration of RD and QoL. To register QoL weused two questionnaires; SF-36 (generic) and IBDQ (disease specific)which both have been translated and validated in Norwegian. Results: Wepresent data from 521 patients of whom 131 (25%) reports RD as peripheral arthritis (PA, n=78), inflammatory back pain (IBP, n=59) or fibromyalgia (FM, n=16). When analyzing SF-36, patients with IBD and RDhave a reduced QoL compared to those with IBD alone. This is in particularseen with the physical health dimensions Role Physical (RP), PhysicalFunctioning (PF), Bodily Pain (BP) and General Health (GH). Whenanalyzing the IBDQ scores, the IBP group had a significant reduction intotal score compared to the PA group. Patients with IBD and FM reporteda significant reduction in QoL with both questionnaires compared to thosesuffering from IBD alone. Summary/conclusions: Patients with IBD andadditional RD reports a reduced QoL compared to IBD patients withoutRD. The reduction is mainly seen in the physical dimensions of SF-36. IBDpatients with PM have a significant reduction in their QoL, seen both withSF-36 and IBDQ.
738A POPULATION BASED STUDY OF PATTERNS OF 5-ASA DRUGUSE AMONG IBD PATIENTS.Charles N. Bernstein, Colleen Metge, James F. Blanchard, Sandra Peterson, Univ of Manitoba, Winnipeg, MB, Canada.
Aims: To assess the patterns of 5-ASA prescription (Rx) within theprovince of Manitoba, among all IBD patients, including the most frequently prescribed 5-ASA, the ratio of oral to rectal 5-ASA use and todetermine usage by disease (Crohn s disease [CD], ulcerative colitis [UC])gender and by era of diagnosis. Methods: We linked the population basedUniversity of Manitoba IBD,database (established in 1996) with the DrugProgram Information Network database of ambulatory Rx for all Manitobaresidents (established in 1994). We extracted the frequency of dispensationof all 7 available 5-ASA drugs in 1997. There were 5102 subjects in the













