Embed Size (px)
Citation preview
ORIGINAL PAPER
Pulse Pressure, Arterial Compliance and Wave Reflection UnderDifferential Vasoactive and Mechanical Loading
John K-J. Li • Ying Zhu • Pamela S. Geipel
Published online: 10 December 2010
� Springer Science+Business Media, LLC 2010
Abstract Similar pulse pressure increases and flow
reductions have been reported by many investigators,
despite dissimilar forms of arterial loading applied.
Increased vascular load is most commonly observed due to
mechanical and vasoactive interventions. The present study
intended to differentiate the hemodynamic contributions of
these two forms of arterial loading at closely matched
blood pressure levels. To accomplish this, proximal aortic
characteristic impedance (Zo), total arterial compliance
(C), peripheral vascular resistance (Rs) and time-domain
resolved forward (Pf) and reflected (Pr) waves were
obtained in six anesthetized, thoracotomized and ventilated
dogs. Acute loading was accomplished by brief descending
thoracic aorta (DTA) occlusion or by intravenous bolus
infusion of methoxamine (MTX:5 mg/ml) Systolic pres-
sure increases were matched to a similar extent. Results
showed that pulse pressures were drastically increased,
reflecting large increases in wave reflections and decreases
in arterial compliances. Changes in Zo, Rs and C were
quantitatively different between the two forms of loading.
DTA occlusion primarily increased Zo and Rs with a con-
currently large reduction in C. MTX infusion significantly
increased small vessel Rs to the same extent as DTA
occlusion, but with a slight decrease in C secondary to an
increase in pressure, with Zo unchanged. Examination of
dynamic loading showed similar increases in reflection
coefficients, but Pf and Pr were qualitatively different. We
conclude that vasoactive methoxamine infusion provides
primarily an increased resistive load, while mechanical
DTA occlusion provides an increased complex load to the
left ventricle. These loads also occur earlier and variably
during ventricular ejection.
Keywords Ventricular afterload � Arterial compliance �Pulse pressure � Wave reflection � Methoxamine infusion �Aortic occlusion
Introduction
The afterload which opposes ventricular ejection is an
important hemodynamic quantity. Changing afterload
affects the ventricle’s function as a pump and alters pulse
transmission characteristics in the arterial system (Li 2000).
Thus, it is important to be able to quantify this load and
differentiate its various contributors.
The complexity of this afterload is attributed to the dif-
ferences in the geometric and elastic properties of arteries at
differing anatomic sites and the varied extent of vasoactiv-
ities of the vascular beds. These become clear from mea-
surements of hemodynamic parameters such as pressure,
flow, and diameter. To understand the behavior of the entire
arterial tree from these measurements, however, requires
considerable effort. Thus, models of the arterial system have
been proposed to identify features of the tree. The three-
element windkessel model has been widely used, because of
its simplicity and its reasonable approximation to the input
impedance of the arterial system (Noordergraaf 1978).
Input impedance is an important determinant of ven-
tricular afterload (e.g. Li 2004). Changes in this impedance
alter the matching characteristics between the ventricle
and the arterial system. The present investigation examines
how the different components of input impedance, namely,
the characteristic impedance (Zo), arterial compliance (C)
J. K-J.Li (&) � Y. Zhu � P. S. Geipel
Cardiovascular Engineering Lab, Department of Biomedical
Engineering, Rutgers University, 599 Taylor Rd, Piscataway,
NJ 08854, USA
e-mail: [email protected]
123
Cardiovasc Eng (2010) 10:170–175
DOI 10.1007/s10558-010-9107-y

and peripheral resistance (Rs), contribute to this load
during acute pressure loading induced mechanically with
descending thoracic aorta (DTA) occlusion and vasoac-
tively with methoxamine infusion, and to see how these
changes modify the pressure and flow waveforms in terms
of their forward and reflected components.
Methods
Theoretical Analysis
For the time domain identification of the three-element
windkessel model parameters, the peripheral resistance can
be obtained as mean aortic pressure (P) to mean aortic flow
(Q) to a good approximation. The diastolic aortic pressure
decay constant, s, can be calculated from a monoexpo-
nential fit to the sampled points of the aortic pressure decay
from end-systole (Pes) to end-diastole (Pd) during the dia-
stolic period (td), such that
Pd ¼ Pese�td=s ð1Þ
and since
s ¼ RSC ð2Þ
the compliance can be easily calculated. Finally the
characteristic impedance Zo can be estimated from the
early ejection phase of systole, as before (Li 1986; Lucas
et al. 1988),
Zo ¼ P� Pdð Þ=Q ð3Þ
where Pd is the aortic diastolic pressure. Measured pressure
and flow waveforms in the arterial tree can be considered
as the sum of their forward (f), and their reflected
(r) pressure (P) and flow (Q) waves, i.e.
P ¼ Pf þ Pr ð4Þ
Q ¼ Qf þ Qr ð5Þ
The ratio of reflected wave to the forward wave defines the
reflection coefficient,
C ¼ Pr
Pf¼ �Qr
Qfð6Þ
The negative sign indicates that reflected pressure and flow
are 180� out of phase or that an increase in reflected pressure
wave decreases flow. The forward and reflected components
of pressure can be resolved according to the relations,
Pf ¼ Pþ QZoð Þ=2 ð7Þ
Pr ¼ P� QZoð Þ=2 ð8Þ
These expressions permit the subsequent resolution of the
forward and reflected waveforms (Li 1986, 2000; Geipel
and Li 1987).
Animal Experiment
Experiments were performed on six mongrel dogs. The
dogs were of either sex and of body weights between 20 to
25 kg. Each animal was anaesthetized with 30 mg/kg
Nembutal and placed on a respirator. A left thoracotomy
was performed at the fifth intercostal space to expose the
heart and the great vessels. The ascending aorta was iso-
lated for placement of a cuff-type electromagnetic flow
probe for measurement of aortic flow. A catheter-tip
pressure transducer was advanced from the femoral artery
to the immediate vicinity of the flow probe for simulta-
neous measurement of aortic pressure. A standard lead
electrocardiogram (ECG) was also recorded. The fre-
quency response of the pressure transducer was flat to well
beyond 100 Hz. The flowmeter output low-pass filter was
3 dB down at 100 Hz. At this setting the amplitude
response was flat to within ± 5% to 30 Hz with a linear
phase shift. The flow probes were statistically calibrated
against known volume flow rates in excised vessels.
Simultaneous recordings of aortic pressure, flow and
ECG were made on a four channel recorder and subse-
quently sampled at 10 ms intervals for computer analysis.
Protocol
The steady state signals prior to interventions were used to
serve as control signals. Mechanical loading was accom-
plished by a brief total occlusion (10 s) of the descending
thoracic aorta (DTA) at approximately 3–5 cm distal to the
aortic arch by a hemostat. The signals normally returned to
control within 30 s after release. The occlusion was repe-
ated after 5 min. When the control level was again estab-
lished, vasoactve loading began via intravenous bolus
infusion of methoxamine (5 mg/ml). The dose was chosen
such that systolic pressure increases were about the same as
during DTA occlusion. This was necessary for later com-
parative analysis of mechanical and vasoactive loadings at
matched blood pressure levels. The peak steady state
response was recorded.
Data Analysis
Recorded pressure and flow waveforms were sampled at
10 ms intervals. In the time domain, Zo was obtained from
the average of the instantaneous ratios of aortic pressure to
flow during the first 60 ms of ejection. The diastolic por-
tion of the aortic pressure was fitted to a mono-exponential
(correlation coefficient r [ 0.93) to obtain the pressure
decay time constant, s, so that arterial compliance, C, could
be computed.
Once the forward and reflected waves were resolved
from Eqs. (7) and (8) above, they were input to a discrete
Cardiovasc Eng (2010) 10:170–175 171
123
Fourier program to obtain harmonic moduli and phases for
the calculation of the reflection coefficient for the first five
harmonics.
All data were pooled and statistical analysis was per-
formed to determine the level of significance (t-test).
Results
Hemodynamic results were tabulated as seen in Table 1,
listing the mean values and the standard deviations of the
measured variables, including heart rates, systolic, diastolic,
and mean aortic blood pressures and mean aortic blood
flows at control, during mechanical loading via descending
aortic occlusion and vasoactive loading via methoxamine
infusion. No significant difference was found among the
heart rates, but pressures increased significantly during both
forms of pressure loading, as expected. The extent of the
systolic pressure increases as designed was about the same
level for the occlusion and methoxamine cases.
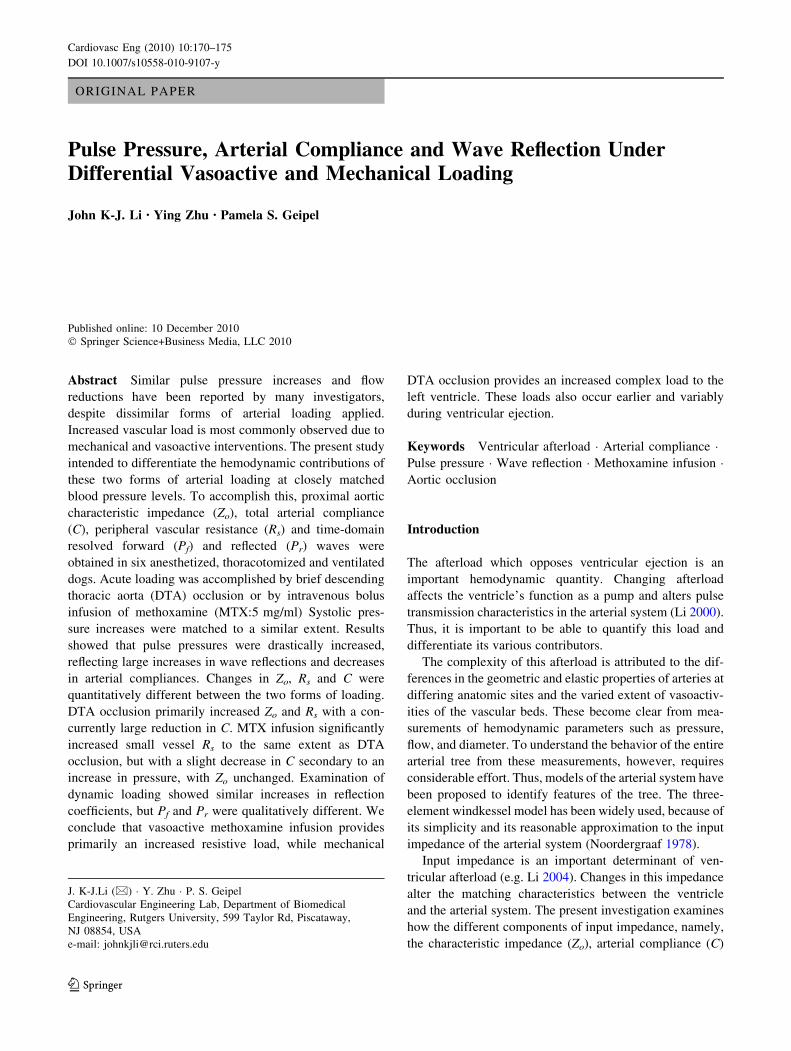
Typical waveforms of the analyzed signals are presented in
Fig. 1. DTA occlusion shows an elevated pulse pressure and a
distinctive dicrotic notch in the pressure wave and a reduced
flow compared to its control (Table 1). MTX exhibits a slow
rise to a high peak pressure, which occurs late in systole, and a
large pulse pressure. Flow is slightly decreased in MTX than
in control (Table 1). There is however, distinctive differences
in the waveforms and the resolved components between DTA
occlusion and MTX infusion, despite their similar responses.
This is seen from Table 2.
The time domain identified model parameters, i.e. Zo,
C and Rs are summarized in Table 2. Both mechanically
and vasoactively induced pressure loading increased Rs,
and decreased C. C was significantly decreased as com-
pared to control during DTA occlusion, but much less so
during the methoxamine infusion. The extent of decrease in
C was different between the two forms of ventricular
loading. Zo was increased during DTA occlusion, but
unchanged during MTX infusion.
The forward and reflected pressure waves are also
shown in Fig. 1. The forward pressure peaks in mid systole
and is larger in magnitude during DTA occlusion. The
reflected pressure also peaks in mid systole, but slightly
later, and is also larger than control. Time to peak reflected
pressure is shorter than in control. The forward pressure
during MTX also increased in magnitude. The reflected
pressure is considerably larger and oscillates with a sec-
ondary peak in late systole. In contrast, control Pf peaks
earlier in systole and falls off more gradually, while Pr
peaks at late systole and does not dip.
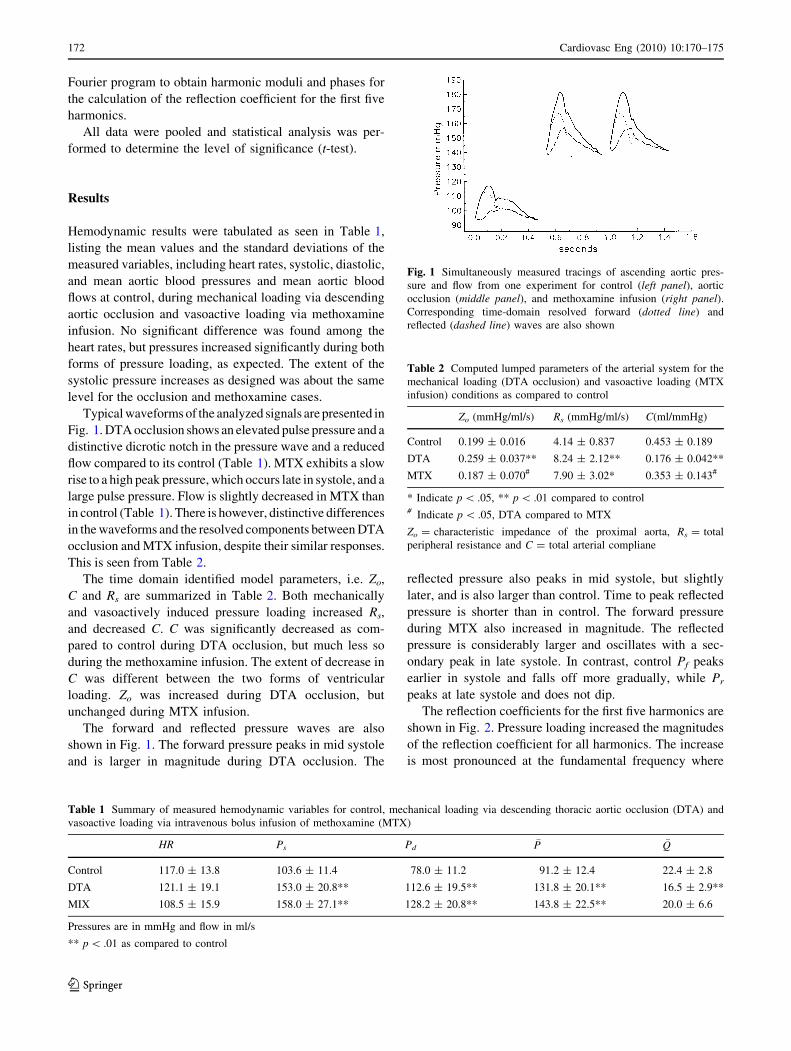
The reflection coefficients for the first five harmonics are
shown in Fig. 2. Pressure loading increased the magnitudes
of the reflection coefficient for all harmonics. The increase
is most pronounced at the fundamental frequency where
Table 1 Summary of measured hemodynamic variables for control, mechanical loading via descending thoracic aortic occlusion (DTA) and
vasoactive loading via intravenous bolus infusion of methoxamine (MTX)
HR Ps Pd�P �Q
Control 117.0 ± 13.8 103.6 ± 11.4 78.0 ± 11.2 91.2 ± 12.4 22.4 ± 2.8
DTA 121.1 ± 19.1 153.0 ± 20.8** 112.6 ± 19.5** 131.8 ± 20.1** 16.5 ± 2.9**
MIX 108.5 ± 15.9 158.0 ± 27.1** 128.2 ± 20.8** 143.8 ± 22.5** 20.0 ± 6.6
Pressures are in mmHg and flow in ml/s
** p \ .01 as compared to control
Fig. 1 Simultaneously measured tracings of ascending aortic pres-
sure and flow from one experiment for control (left panel), aortic
occlusion (middle panel), and methoxamine infusion (right panel).Corresponding time-domain resolved forward (dotted line) and
reflected (dashed line) waves are also shown
Table 2 Computed lumped parameters of the arterial system for the
mechanical loading (DTA occlusion) and vasoactive loading (MTX
infusion) conditions as compared to control
Zo (mmHg/ml/s) Rs (mmHg/ml/s) C(ml/mmHg)
Control 0.199 ± 0.016 4.14 ± 0.837 0.453 ± 0.189
DTA 0.259 ± 0.037** 8.24 ± 2.12** 0.176 ± 0.042**
MTX 0.187 ± 0.070# 7.90 ± 3.02* 0.353 ± 0.143#
* Indicate p \ .05, ** p \ .01 compared to control# Indicate p \ .05, DTA compared to MTX
Zo = characteristic impedance of the proximal aorta, Rs = total
peripheral resistance and C = total arterial compliane
172 Cardiovasc Eng (2010) 10:170–175
123
the mean reflection coefficients of 0.77, 0.68 and 0.39 were
found for MTX, DTA and control respectively. At higher
frequencies, the reflection coefficients remain large and are
more oscillatory as compared to control. These frequency
domain findings correspond to the time domain changes.
Discussion
Cardiac muscle shortening is dependent on its preload and
afterload (Braunwald 1977; Du et al. 2001; Li 2004). These
loads have opposite effects: increased preload alone
increases shortening, as dictated by the Starling’s law of
the heart; increased afterload alone however, decreases
muscle shortening, as suggested by the Hill’s equation.
Thus, just what kind of afterload the ventricle ejects against
has been of considerable interest.
Input impedance of the systemic arterial tree is an
important determinant of afterload (Pepine et al. 1979;
Gundel et al. 1981; Murgo et al. 1981). We have investigated
the contributions of its components to the load facing the
ventricular ejection, during mechanical loading and during
vasoactive loading. There are several means for altering the
load to cardiac ejection. These can be from mechanical,
neural or pharmacological interventions. The present
investigation differentiates the mechanical and pharmaco-
logical means of pressure loading the left ventricle.
Methoxamine, a vasopressor, can raise blood pressure to
a great extent (Imai et al. 1961). It acts primarily on small
vessels in a distributed manner. It is a preferential alpha
one agonist, constricting the arterioles and capacitance
vessels (Zandberg et al. 1984). Its action causes unfavor-
able hemodynamic effects by altering impedance match-
ing, primarily through increased peripheral resistance.
Although the compliance is decreased, it is not statistically
significantly different from control. The decrease in arterial
compliance is secondary to an increase in pressure.
Significantly increased pulse pressure is indicative of
reduced compliance, particularly an increase in systolic
blood pressure, as observed in systolic hypertension (Ber-
ger and Li 1990; Li et al. 1994; Li 2000; Safar and Laurent
2003). The inverse relationship between pulse pressure and
arterial compliance has been studied by several investiga-
tors (e.g. Ferguson and Randall 1986; Stergiopoulos et al.
1999). Drastically elevated mean blood pressures, as
observed here during loading, would alter such relation-
ship. The determinants of pulse pressure are many, not all
attributed to the arterial system through the interplay of
arterial compliance and peripheral resistance. As pressure
and flow are generated by the heart, cardiac contraction is
also a main contributing factor. Compliance, as we have
noted previously, is a function of arterial pressure (e.g.
Randall 1982; Li and Zhu 1994). Such pressure-dependent
compliance changes can be more accurately quantified with
a nonlinear arterial system model (Li et al. 1990; Matonick
and Li 2001) and should be further explored. The main
effects of mechanical loading of the ventricle through
descending aortic occlusion are regional, residing primarily
in the aorta (Stokland et al. 1980). Aortic characteristic
impedance increased considerably, with a large concurrent
decrease in arterial compliance. Since a large portion of the
systemic arterial compliance is in the aorta, the site of
occlusion will determine the level of ventricular loading, as
found by other investigators (Van den Bos et al. 1976).
These two methods of raising aortic blood pressure have
been used as experimental models of acute hypertension.
Our findings could clarify the hemodynamic mechanisms
promoting this diseased state. Both form of loading have
consistently produced increased systolic and diastolic
blood pressures, or the so called combined hypertension.
The increases in peripheral resistance are about the same in
the two forms of loading (99% for DTA occlusion and 91%
for MTX infusion). But only in DTA occlusion cases, the
compliance is decreased significantly, by about 61%. This
may be due to the fact that arterial compliances normally
contributed by the aorta and systemic arteries distal to the
DTA occlusion site were effectively removed. In isolated
systolic hypertension (Li et al. 2007) which occurs pre-
dominantly in the elderly, a systolic pressure greater than
165 mmHg and a diastolic pressure of about normal, a
large decrease in compliance (greater than 75%) and a
smaller but significant increase in peripheral resistance
(about than 25%) are found (Berger and Li 1990).
It is clear from the present study that the left ventricle
faces an increased steady state load, mainly from the
periphery, i.e. small resistance and capacitance vessels
during ejection in the methoxamine induced hypertension
cases. Whereas, the ventricle faces a changing complex
load, i.e. increased aortic characteristic impedance,
decreased large vessel compliance and increased peripheral
Fig. 2 Reflection coefficients as a function of frequency. Both
descending aortic occlusion (DTA; circle) and methoxamine infusion
(MTX; triangle) increased the coefficients for all harmonics. Notice
the much more pronounced oscillations during loading
Cardiovasc Eng (2010) 10:170–175 173
123

resistance during mechanical loading through descending
aortic occlusion.
The increased wave reflections during the ejection period
in general decrease ventricular outflow. This is particularly
true in the case of DTA occlusion; flow is significantly
decreased by about 26%. This decrease was only about 11%,
and statistically insignificant during methoxamine infusion,
despite similar increases in peripheral resistance. This sug-
gests that pressure loading that alters both components of the
complex load is perhaps more detrimental to ventricular
function. Since aortic pressure serves as the coronary perfu-
sion pressure, particularly during diastole (Li 2000), whether
increased aortic pressure due to the two types of loading may
lead to differential coronary flow (Ohtsuka et al. 1987) or its
resistance-compliance behavior (Liao and Li 2005) is unclear.
The magnitude of the reflected pulse waves increased by
about 2fold during the interventions. Since wave reflections
are energetically wasteful (Li 1989), such increases, espe-
cially during the ejection phase, have the effects of
retarding flow. The reflection coefficients remain high at
high frequencies, indicating that the local reflections at
aortic branching junctions are large, due to large mis-
matching of characteristic impedances of branching vessels
(Li et al. 1984). The forward components are also increased
during loading, reflecting the changing cardiac state.
Ventricular performance under such circumstances can be
evaluated from its load sensitivity, as we have shown
previously (Geipel et al. 1989).
Afterload reduction with vasodilator therapy is still a
popular means of treating cardiovascular diseases (Cohn
and Franciosa 1977; Pepine et al. 1979; Gundel et al. 1981;
Yin et al. 1983; Brin and Yin 1984; Vogt et al. 1988; Li
2000), particularly the hypertensive. It is thus important to
be able to differentiate this load and reduce its magnitude by
either decreasing wave reflections, or selectively improving
large vessel compliance and decreasing peripheral resis-
tance, or both.
Conclusion
Arterial load reduction with drug therapy and by surgical
means are still popular means of treating vascular diseases.
The present investigation provided a means and differenti-
ated the hemodynamic mechanism of the increased load due
to mechanical or vasoactive alterations. Unloading should
then be accompanied by either appropriately decreasing
wave reflections, or selectively improving large vessel
compliance and decreasing peripheral resistance or both.
Acknowledgments This work was supported in part by a grant from
the American Heart Association and New Jersey Commission on
Spinal Cord Research.
References
Berger DS, Li JK-J. Concurrent compliance reduction and increased
peripheral resistance in the manifestation of isolated systolic
hypertension. Am J Cardiol. 1990;65:67–71.
Braunwald E. Determinants and assessment of cardiac function.
N Engl J Med. 1977;296:86–9.
Brin KP, Yin FCP. Effect of nitroprusside on wave reflections in
patients with heart failure. Ann Biomed Eng. 1984;12:135–50.
Cohn JN, Franciosa JA. Vasodilator therapy of cardiac failure. N Engl
J Med. 1977;297:254–8.
Du FY, Chen X-L, Drzewiecki G, Li JK-J, Kedem J. Hypervolemia
improves global and local function and efficiency in postische-
mic myocardium. Clin Exp Pharmacol Physiol. 2001;28:630–6.
Ferguson JJ III, Randall OS. Hemodynamic correlates of arterial
compliance. Cathet Cardiovasc Diagn. 1986;12:376–80.
Geipel PS, Li JK-J. Assessing wave reflections in the systemic arterial
tree. In: Proc. IEEE 9th Ann. Conf. Eng. Med. Biol. 1987.
p. 880–1.
Geipel PS, Li JK-J, Laskey WK, Noordergraaf A. Ventricular
performance evaluated from load sensitivity. In: Proc. 9th. Int.
Cardiovasc. System Dynamics Conf. 1989. p. 309–12.
Gundel W, Cherry G, Rajagopalan B, Tan L-B, Lee G, Schultz D.
Aortic input impedance in man: acute response to vasodilator
drugs. Circulation. 1981;63:1305–14.
Imai S, Shigei T, Hashimoto K. Cardiac actions of methoxamine. Circ
Res. 1961;9:552–60.
Li JK-J. Dynamics of the vascular system. Singapore: World
Scientific Publishing Co; 2004.
Li JK-J. The arterial circulation: physical principles and clinical
applications. Totowa: Humana Press; 2000.
Li JK-J, Melbin J, Noordergraaf A. Directional disparity of pulse
wave reflections in dog arteries. Am J Physiol. 1984;247:H95–9.
Li JK-J. Time domain resolution of forward and reflected waves in the
aorta. IEEE Trans Biomed Eng. 1986;BME-33:783–5.
Li JK-J. Increased arterial pulse wave reflections and pulsatile energy
loss in acute hypertension. Angiology J Vasc Dis. 1989;40:730–5.
Li JK-J, Cui T, Drzewiecki G. A nonlinear model of the arterial
system incorporating a pressure-dependent compliance. IEEE
Trans. Biomed. Eng., 1990;BME-37:673–8.
Li JK-J, Zhu Y. Arterial compliance and its pressure-dependence in
hypertension and vasodilation. Angiology J Vasc Dis. 1994;45:113–7.
Li JK-J, Zhu Y, Drzewiecki G. Pulse pressure is a significant
determinant of arterial compliance in hypertension and vasodi-
lation. Circulation. 1994;90:I166.
Li JK-J, Zhu Y, O’Hara D, Khaw K. Allometric hemodynamic
analysis of isolated systolic hypertension and aging. Cardiovasc
Eng. 2007;7:135–9.
Liao J, Li JK-J. Modeling of the coronary circulatory system.
Cardiovasc Eng. 2005;5:141–50.
Lucas CL, Wilcox BR, Henry GW. Comparison of time domain
algorithms for estimating aortic characteristic impedance in
humans. IEEE Trans Biomed Eng. 1988;35:62–7.
Matonick JP, Li JK-J. Pressure-dependent and frequency domain
characteristics of systemic arterial compliance. Cardiovasc Eng.
2001;1:21–30.
Murgo JP, Westerhof N, Giolma JP, Altobelli S. Manipulation of
ascending aorta pressure and flow wave reflections with the
valsalva maneuver: relationship to input impedance. Circulation.
1981;63:122–32.
Noordergraaf A. Circulatory system dynamics. New York: Academic
Press; 1978.
Ohtsuka S, Kakihana M, Sugishita Y, Ito I. Effects on the rise in
aortic pressure on coronary flow reserve in dogs. Jpn Heart J.
1987;28:403–11.
174 Cardiovasc Eng (2010) 10:170–175
123

Pepine CJ, Nichols WW, Curry RC, Conti R. Aortic input impedance
during nitroprusside infusion. J Clin Invest. 1979;64:643–54.
Randall OS. Effect of arterial compliance on systolic blood pressure
and cardiac function. Clin Exp Hypertens Theory Pract. 1982;
4(7):1045–57.
Safar ME, Laurent P. Pulse pressure and arterial stiffness in rats:
comparison with humans. Am J Physiol. 2003;285:H1363–9.
Stergiopoulos N, Segers P, Westerhof N. Use of pulse pressure
method for estimating total arterial compliance in vivo. Am J
Physiol. 1999;276:H424–8.
Stokland O, Miller MM, Ilebekk A, Kiil F. Mechanism of hemody-
namic responses to occlusion of the descending thoracic aorta.
Am J Physiol. 1980;238:H423–9.
Van den Bos GC, Westerhof N, Elzinga G, Sipkema P. Reflection in
the systemic arterial arterial system effects of aortic and carotid
occlusion. Cardiovasc Res. 1976;10:565–73.
Vogt A, Neuhaus K-L, Kreuzer H. Pathophysiologic arguments for
vasodilators in heart failure. Cardiovasc Drugs Ther. 1988;2:
647–51.
Yin FCP, Guzman PA, Brin KP, Maughan WL, Brinker JA, Traill
TA, Weiss JL, Weisfeldt ML. Effect of nitroprusside on
hydraulic vascular loads on the right and left ventricle of
patients with heart failure. Circulation. 1983;67:1330–9.
Zandberg P, Timmermans PBMWM, van Zwieten PA. Hemodynamic
profiles of methoxamine and B-HT933 in spinalized ganglion-
blocked dogs. J Cardiovasc Pharmacol. 1984;6:256–62.
Cardiovasc Eng (2010) 10:170–175 175
123






![Terlipressin versus other vasoactive drugs for hepatorenal ...[Intervention Review] Terlipressin versus other vasoactive drugs for hepatorenal syndrome Mads Israelsen 1, Aleksander](https://img.dokumen.tips/doc/110x75/60a7d279a5295c2888291ae4/terlipressin-versus-other-vasoactive-drugs-for-hepatorenal-intervention-review.jpg)






















