Embed Size (px)
Citation preview
PSYCHIATRIC COMORBITY IN AUTISMTeresita M. Amay, M.D.
Diplomate
American Board of Psychiatry and Neurology
PSYCHIATRIC COMORBIDITY IN AUTISMANXIETY
DEPRESSION
BIPOLAR MOOD DISORDER

ANXIETY
University of Amsterdam Study 40% of children with ASD had at least 1 comorbid anxiety disorder
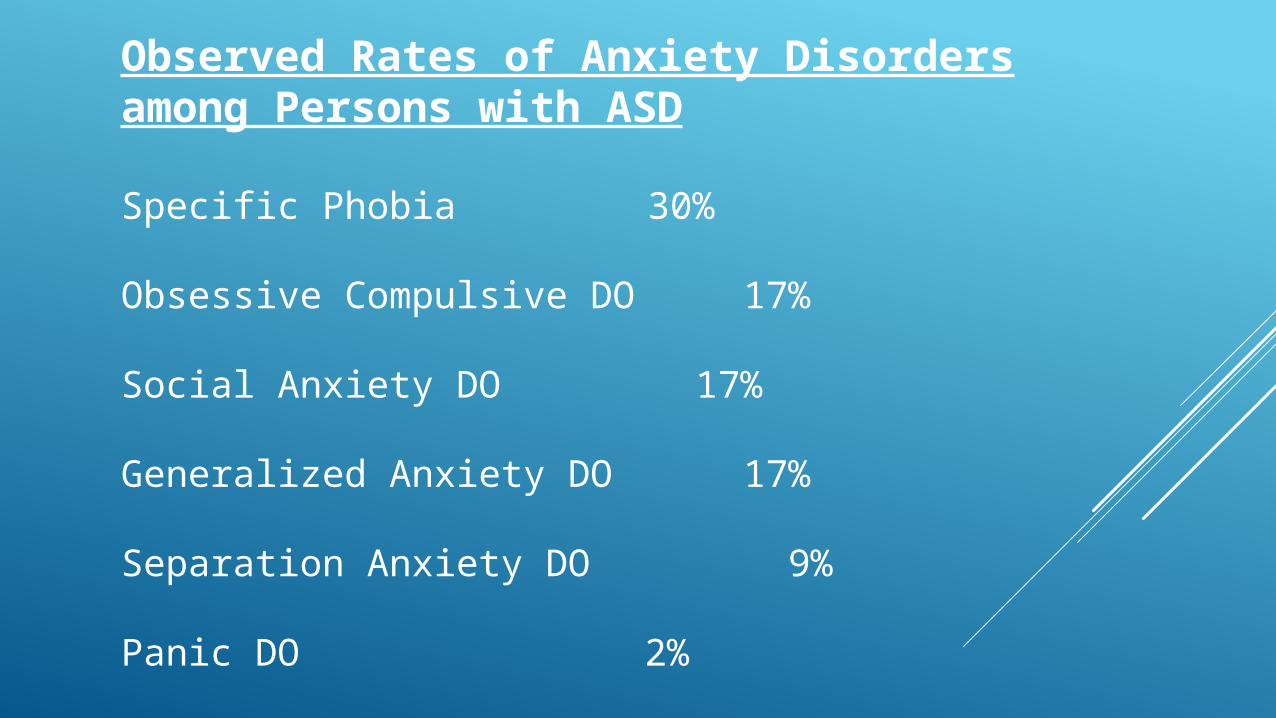
Observed Rates of Anxiety Disorders among Persons with ASD
Specific Phobia 30%
Obsessive Compulsive DO 17%
Social Anxiety DO 17%
Generalized Anxiety DO 17%
Separation Anxiety DO 9%
Panic DO 2%
DSM IV TR: Generalized Anxiety Disorder Excessive anxiety and worry (apprehensive expectation) Person finds it difficult to control worry.
The anxiety and worry are associated with 3 (or more) of the following six symptoms: 1. restlessness or feeling keyed up or on edge 2. being easily fatigued 3. difficulty concentrating or mind going blank 4. irritability 5. muscle tension 6. sleep disturbance (difficulty falling or staying asleep or restless unsatisfying sleep)
Obsessive Compulsive Disorder symptoms are similar to repetitive and stereotyped behaviors seen in ASD.
Symptoms more severe in ASD than non-ASD
TREATMENT:
For higher functioning individual Cognitive Behavior Therapy (CBT)
For severe symptoms: medication + CBT
For lower functioning individual: medication

DEPRESSION
Symptoms of depression seen in general population and ASD
-sadness-apathy-anhedonia-loss of interest-decrease self care-psychomotor retardation
In general clinicians rely on patients’ self- report; this makes it difficult to assess depression in the ASD population
Symptoms of depression can be manifested in poor sleep, ability to concentrate, and in communication through facial expression or intonation.
These are easily masked by symptoms of autism.
Symptoms that may be present but not frequently seen:- Feeling of worthlessness- Guilt
Other possible depressive symptoms more specific to or common in ASD- Irritability- Agitation- Increase social withdrawal- Change in character or obsession- Increase in compulsive behavior
For Individuals with co-morbid cognitive disability, depression can be manifested through:
- Increase in self injury- Regression of adaptive skills
Presentation of depression
Depends on age, level of intelligence and verbal skills.
TREATMENTFor mild to moderate symptoms and higher functioning- Cognitive Behavior Treatment (CBT)
For severe symptoms - CBT + Medications
For ASD patient with co-morbid cognitive disability – Medications
BIPOLAR MOOD DISORDER
Prevalence of Bipolar Disorder (BD) in adults with ASD ranges from 6% to 27%
Usual onset in adolescence Characterized by atypical presentation, making identification difficult.
Family history of affective disorder very important
Clinical features often diagnosed as Schizophrenia because of the atypical presentation.
One key factor in differentiating bipolar disorder is to look carefully at when the symptoms appear and how long they last.
Manic episodes in adult ASD are characterized by mixed features such as irritability, unstable and dysphoric mood, hostility, restlessness, anxiety, perplexity, aggression, violent behavior and insomnia.
Uncommon are euphoric mood, elation and jocularity.
Psychotic symptoms may be so prominent that other manic symptoms remain unrecognized.
Bizarre thought contents vs. odd thinking, bizarre ideas and idiosyncratic views are common among ASD individuals.
Important in making the diagnosis is an accurate clinical interview, and use of assessment instruments for mood symptoms.
The presence of a family history of BD in first degree relatives, special abilities, anxiety and or multiple psychiatric co-morbidities and co-morbid Tourette’s Syndrome are other important indicators of bipolarity.
TREATMENT: Mood stabilizers
Lithium: Predictors of favorable response are -
Family history of BDSevere hyperactivity unresponsive to stimulantsCyclical pattern of behavioral changesIrritabilityEnduring outbursts of laughterSubjective dizzinessPresence of at least some BD diagnostic criteria
Valproate
Several reports suggests efficacy in symptoms of irritability, dysphoria and anxiety.
Favorable effects in ASD patients with Mental Retardation, typical and atypical BD including rapid cycling.
Oxcarbazepine + low dose second generation antipsychotic
ATYPICAL ANTIPSYCHOTIC OR SECOND GENERATION ANTIPSYCHOTIC MEDICATIONS
RisperidoneEffective in reducing repetitive, aggressive and impulsive behaviors and improving
some aspects of sociality
Side effects: Extrapyramidal symptoms, Tardive Dyskinesia, weight gain, drowsiness and elevated prolactin level.
Aripiprazole
Effective in reducing irritability, self-injury and temper tantrums.
Well tolerated
Side Effects: weight gain, elevated prolactin, dose-dependent sedation and drooling/increased salivation. EPS and Tardive Dyskinesia are not negligible.
References:
NADD Bulletin Volume X Number 6 Article 1Bipolar Spectrum Disorder with Comorbid Spectrum Disorders Jay A Salpekar, MD, Peter Daniolos, MD, The George Washington
University School of Medicine
Journal of Affective DisordersBipolar Disorder in Adults with Asperger’s SyndromeA Systematic ReviewGiulia Vannucchi, Gabriele Masi, Cristina Toni, Dell’OssoAndreas Erfurth, Giulio Perugi
The National Autistic Society Depression and its measurement in the verbal adolescents and adultswith autism spectrum disorderKatherine Gotham, Kathryn Unruth and Catherine Lord
References:
DSM IV TR APA Publishing
Indiana Resource for AutismAnxiety and Autism Spectrum DisordersAnn Merrill