Embed Size (px)
Citation preview
o
crvsoccamb
otosbb
Proximal Hamstring Syndrome:Repair and Ischial BursectomyCarlos A. Guanche, MD
The increase in analyzing hip intra-articular injuries has led to an exponential understandingof the diagnosis and treatment of many injuries and pathologies around the hip. Previously,many of these conditions were either undertreated or treated with open surgical proce-dures. This chapter details 1 evolving technique that allows for the endoscopic manage-ment of proximal hamstring tears and chronic ischial bursitis. Until now, these have beenmanaged exclusively with much larger open approaches. This procedure allows for com-plete exposure of the posterior aspect of the hip in a safe minimally invasive manner, whileaddressing the various pathologies.Oper Tech Sports Med 20:333-339 © 2012 Elsevier Inc. All rights reserved.
KEYWORDS hamstring tear, ischial bursitis, hamstring syndrome
eanrtTc
dppcdas
With the evolution of hip arthroscopy has come theendoscopic management of several pathologies previ-
usly treated with more invasive open approaches.1,2 Thetechnique described in this chapter is another such evolu-tion. Hamstring injuries are common and can affect all levelsof athletes.3-7 There is a continuum of hamstring injuries thatan range from musculotendinous strains to avulsion inju-ies.3,4 Most hamstring strains do not require surgical inter-ention and resolve with a variety of modalities and rest.3-7 Inome situations, chronic pain can occur at the hamstringrigin either due to a partial or complete tear or due tohronic ischial bursitis. The technique described in thishapter is one that allows for the treatment and evaluation ofll of these injuries in an endoscopic manner, with a mini-um of risk and a maximum of diagnostic evaluation capa-
ility.The hamstring complex originates from the ischial tuber-
sity and inserts distally below the knee on the proximalibia, with the exception of the short head of the biceps fem-ris. The tibial branch of the sciatic nerve innervates theemitendinosus and semimembranosus, and the peronealranch of the sciatic nerve innervates the long head of theiceps femoris.5
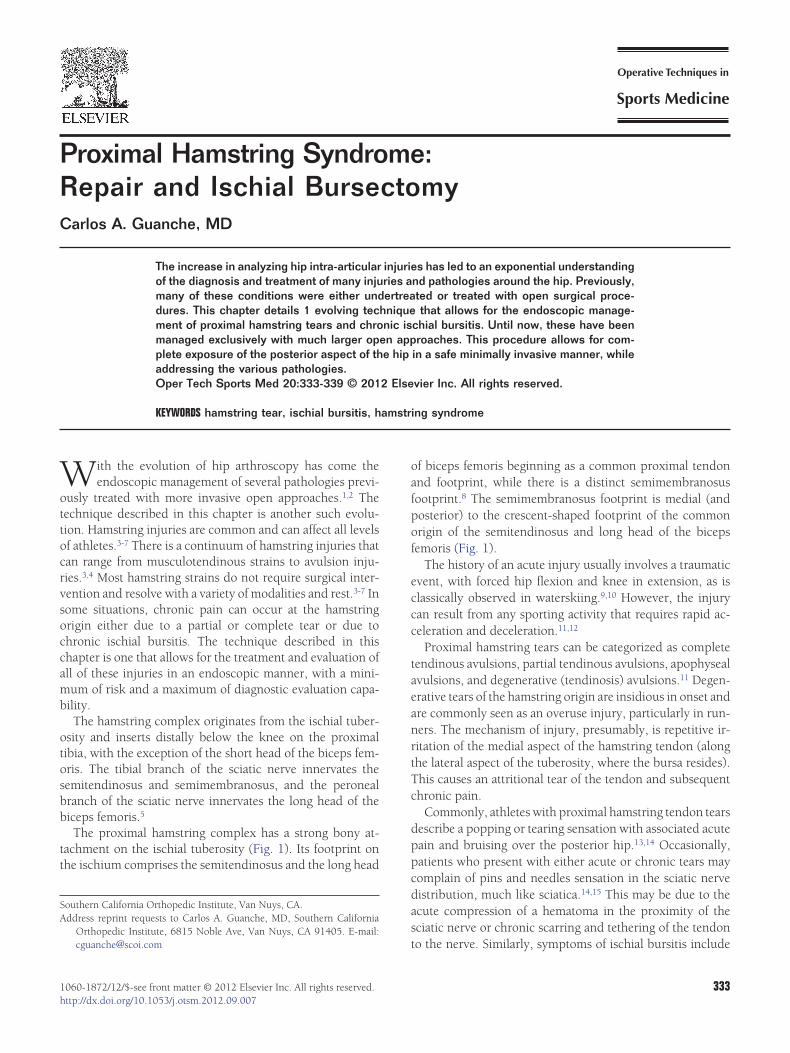
The proximal hamstring complex has a strong bony at-tachment on the ischial tuberosity (Fig. 1). Its footprint onthe ischium comprises the semitendinosus and the long head
Southern California Orthopedic Institute, Van Nuys, CA.Address reprint requests to Carlos A. Guanche, MD, Southern California
Orthopedic Institute, 6815 Noble Ave, Van Nuys, CA 91405. E-mail:
[email protected]1060-1872/12/$-see front matter © 2012 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1053/j.otsm.2012.09.007
of biceps femoris beginning as a common proximal tendonand footprint, while there is a distinct semimembranosusfootprint.8 The semimembranosus footprint is medial (andposterior) to the crescent-shaped footprint of the commonorigin of the semitendinosus and long head of the bicepsfemoris (Fig. 1).
The history of an acute injury usually involves a traumaticevent, with forced hip flexion and knee in extension, as isclassically observed in waterskiing.9,10 However, the injurycan result from any sporting activity that requires rapid ac-celeration and deceleration.11,12
Proximal hamstring tears can be categorized as completetendinous avulsions, partial tendinous avulsions, apophysealavulsions, and degenerative (tendinosis) avulsions.11 Degen-rative tears of the hamstring origin are insidious in onset andre commonly seen as an overuse injury, particularly in run-ers. The mechanism of injury, presumably, is repetitive ir-itation of the medial aspect of the hamstring tendon (alonghe lateral aspect of the tuberosity, where the bursa resides).his causes an attritional tear of the tendon and subsequenthronic pain.
Commonly, athletes with proximal hamstring tendon tearsescribe a popping or tearing sensation with associated acuteain and bruising over the posterior hip.13,14 Occasionally,atients who present with either acute or chronic tears mayomplain of pins and needles sensation in the sciatic nerveistribution, much like sciatica.14,15 This may be due to thecute compression of a hematoma in the proximity of theciatic nerve or chronic scarring and tethering of the tendon
o the nerve. Similarly, symptoms of ischial bursitis include333
nTn
mpsiucp
334 C.A. Guanche
buttock pain or hip pain and localized tenderness overlyingthe ischial tuberosity. Additional symptoms of chronic ischialbursitis may also include tingling in the buttocks that spreadsdown the leg.14
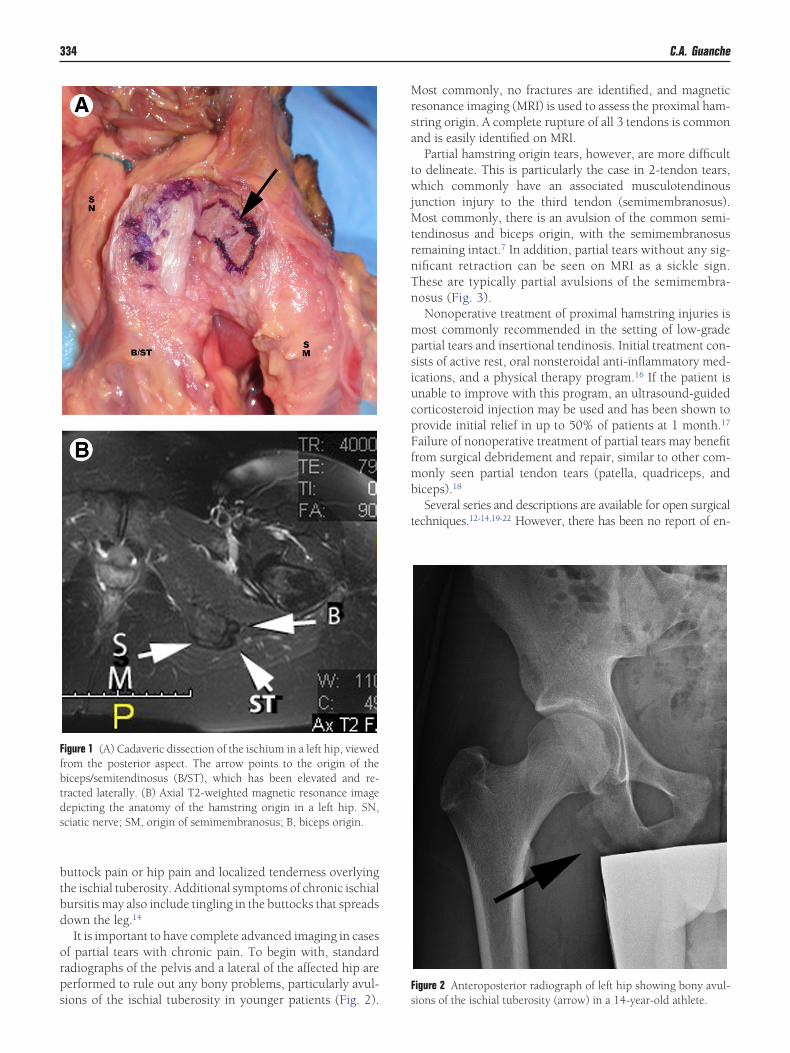
It is important to have complete advanced imaging in casesof partial tears with chronic pain. To begin with, standardradiographs of the pelvis and a lateral of the affected hip areperformed to rule out any bony problems, particularly avul-
Figure 1 (A) Cadaveric dissection of the ischium in a left hip, viewedfrom the posterior aspect. The arrow points to the origin of thebiceps/semitendinosus (B/ST), which has been elevated and re-tracted laterally. (B) Axial T2-weighted magnetic resonance imagedepicting the anatomy of the hamstring origin in a left hip. SN,sciatic nerve; SM, origin of semimembranosus; B, biceps origin.
sions of the ischial tuberosity in younger patients (Fig. 2).
Most commonly, no fractures are identified, and magneticresonance imaging (MRI) is used to assess the proximal ham-string origin. A complete rupture of all 3 tendons is commonand is easily identified on MRI.
Partial hamstring origin tears, however, are more difficultto delineate. This is particularly the case in 2-tendon tears,which commonly have an associated musculotendinousjunction injury to the third tendon (semimembranosus).Most commonly, there is an avulsion of the common semi-tendinosus and biceps origin, with the semimembranosusremaining intact.7 In addition, partial tears without any sig-
ificant retraction can be seen on MRI as a sickle sign.hese are typically partial avulsions of the semimembra-osus (Fig. 3).Nonoperative treatment of proximal hamstring injuries isost commonly recommended in the setting of low-gradeartial tears and insertional tendinosis. Initial treatment con-ists of active rest, oral nonsteroidal anti-inflammatory med-cations, and a physical therapy program.16 If the patient isnable to improve with this program, an ultrasound-guidedorticosteroid injection may be used and has been shown torovide initial relief in up to 50% of patients at 1 month.17
Failure of nonoperative treatment of partial tears may benefitfrom surgical debridement and repair, similar to other com-monly seen partial tendon tears (patella, quadriceps, andbiceps).18
Several series and descriptions are available for open surgicaltechniques.12-14,19-22 However, there has been no report of en-
Figure 2 Anteroposterior radiograph of left hip showing bony avul-
sions of the ischial tuberosity (arrow) in a 14-year-old athlete.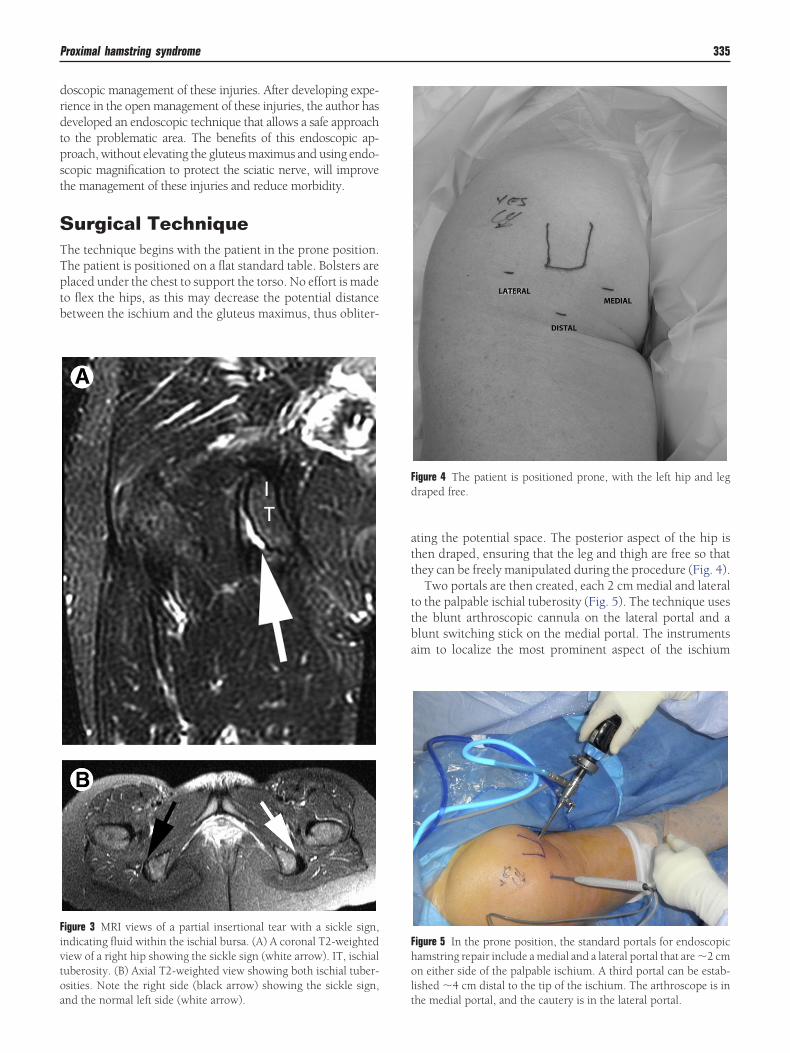
Proximal hamstring syndrome 335
doscopic management of these injuries. After developing expe-rience in the open management of these injuries, the author hasdeveloped an endoscopic technique that allows a safe approachto the problematic area. The benefits of this endoscopic ap-proach, without elevating the gluteus maximus and using endo-scopic magnification to protect the sciatic nerve, will improvethe management of these injuries and reduce morbidity.
Surgical TechniqueThe technique begins with the patient in the prone position.The patient is positioned on a flat standard table. Bolsters areplaced under the chest to support the torso. No effort is madeto flex the hips, as this may decrease the potential distancebetween the ischium and the gluteus maximus, thus obliter-
Figure 3 MRI views of a partial insertional tear with a sickle sign,indicating fluid within the ischial bursa. (A) A coronal T2-weightedview of a right hip showing the sickle sign (white arrow). IT, ischialtuberosity. (B) Axial T2-weighted view showing both ischial tuber-osities. Note the right side (black arrow) showing the sickle sign,
and the normal left side (white arrow).ating the potential space. The posterior aspect of the hip isthen draped, ensuring that the leg and thigh are free so thatthey can be freely manipulated during the procedure (Fig. 4).
Two portals are then created, each 2 cm medial and lateralto the palpable ischial tuberosity (Fig. 5). The technique usesthe blunt arthroscopic cannula on the lateral portal and ablunt switching stick on the medial portal. The instrumentsaim to localize the most prominent aspect of the ischium
Figure 4 The patient is positioned prone, with the left hip and legdraped free.
Figure 5 In the prone position, the standard portals for endoscopichamstring repair include a medial and a lateral portal that are �2 cmon either side of the palpable ischium. A third portal can be estab-lished �4 cm distal to the tip of the ischium. The arthroscope is in
the medial portal, and the cautery is in the lateral portal.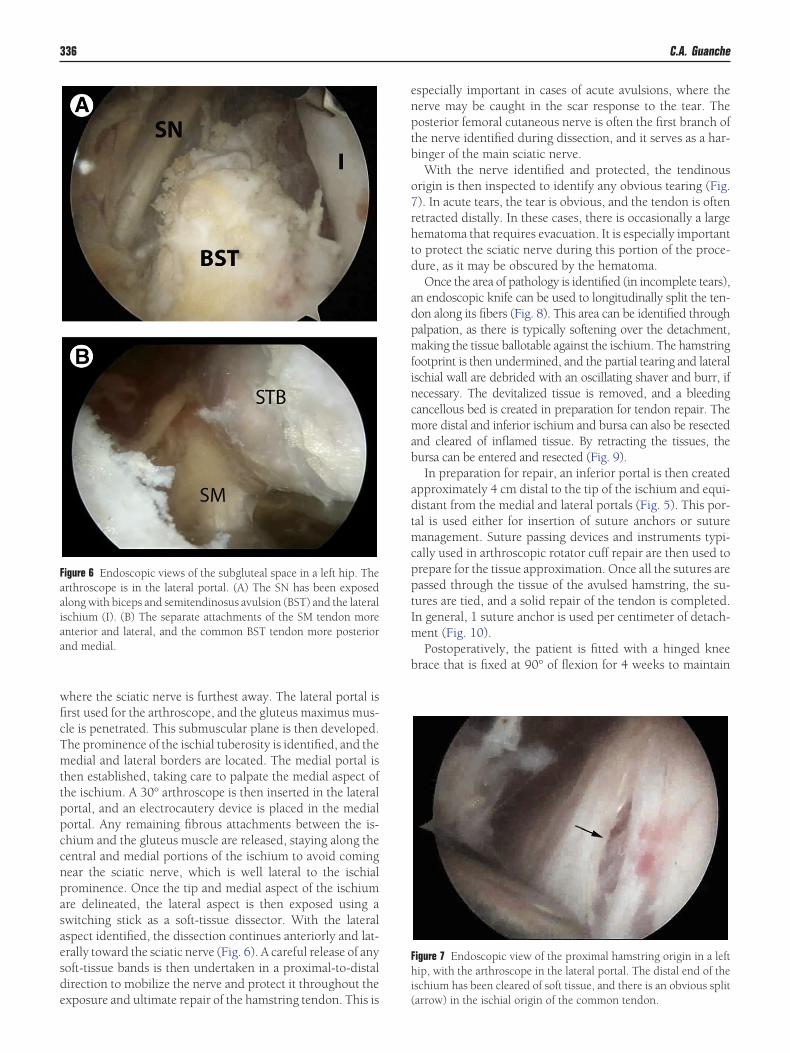
aaiaa
336 C.A. Guanche
where the sciatic nerve is furthest away. The lateral portal isfirst used for the arthroscope, and the gluteus maximus mus-cle is penetrated. This submuscular plane is then developed.The prominence of the ischial tuberosity is identified, and themedial and lateral borders are located. The medial portal isthen established, taking care to palpate the medial aspect ofthe ischium. A 30° arthroscope is then inserted in the lateralportal, and an electrocautery device is placed in the medialportal. Any remaining fibrous attachments between the is-chium and the gluteus muscle are released, staying along thecentral and medial portions of the ischium to avoid comingnear the sciatic nerve, which is well lateral to the ischialprominence. Once the tip and medial aspect of the ischiumare delineated, the lateral aspect is then exposed using aswitching stick as a soft-tissue dissector. With the lateralaspect identified, the dissection continues anteriorly and lat-erally toward the sciatic nerve (Fig. 6). A careful release of anysoft-tissue bands is then undertaken in a proximal-to-distaldirection to mobilize the nerve and protect it throughout the
Figure 6 Endoscopic views of the subgluteal space in a left hip. Therthroscope is in the lateral portal. (A) The SN has been exposedlong with biceps and semitendinosus avulsion (BST) and the lateralschium (I). (B) The separate attachments of the SM tendon morenterior and lateral, and the common BST tendon more posteriornd medial.
exposure and ultimate repair of the hamstring tendon. This is
especially important in cases of acute avulsions, where thenerve may be caught in the scar response to the tear. Theposterior femoral cutaneous nerve is often the first branch ofthe nerve identified during dissection, and it serves as a har-binger of the main sciatic nerve.
With the nerve identified and protected, the tendinousorigin is then inspected to identify any obvious tearing (Fig.7). In acute tears, the tear is obvious, and the tendon is oftenretracted distally. In these cases, there is occasionally a largehematoma that requires evacuation. It is especially importantto protect the sciatic nerve during this portion of the proce-dure, as it may be obscured by the hematoma.
Once the area of pathology is identified (in incomplete tears),an endoscopic knife can be used to longitudinally split the ten-don along its fibers (Fig. 8). This area can be identified throughpalpation, as there is typically softening over the detachment,making the tissue ballotable against the ischium. The hamstringfootprint is then undermined, and the partial tearing and lateralischial wall are debrided with an oscillating shaver and burr, ifnecessary. The devitalized tissue is removed, and a bleedingcancellous bed is created in preparation for tendon repair. Themore distal and inferior ischium and bursa can also be resectedand cleared of inflamed tissue. By retracting the tissues, thebursa can be entered and resected (Fig. 9).
In preparation for repair, an inferior portal is then createdapproximately 4 cm distal to the tip of the ischium and equi-distant from the medial and lateral portals (Fig. 5). This por-tal is used either for insertion of suture anchors or suturemanagement. Suture passing devices and instruments typi-cally used in arthroscopic rotator cuff repair are then used toprepare for the tissue approximation. Once all the sutures arepassed through the tissue of the avulsed hamstring, the su-tures are tied, and a solid repair of the tendon is completed.In general, 1 suture anchor is used per centimeter of detach-ment (Fig. 10).
Postoperatively, the patient is fitted with a hinged kneebrace that is fixed at 90° of flexion for 4 weeks to maintain
Figure 7 Endoscopic view of the proximal hamstring origin in a lefthip, with the arthroscope in the lateral portal. The distal end of theischium has been cleared of soft tissue, and there is an obvious split
(arrow) in the ischial origin of the common tendon.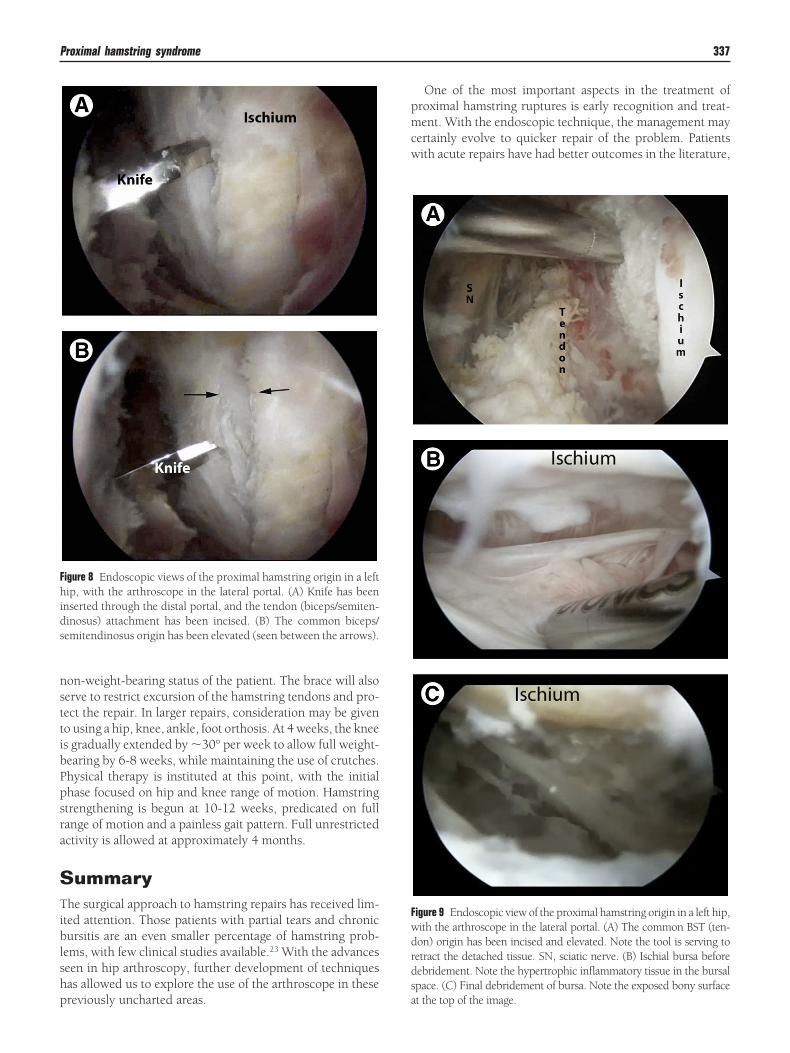
shp
pmcw
Proximal hamstring syndrome 337
non-weight-bearing status of the patient. The brace will alsoserve to restrict excursion of the hamstring tendons and pro-tect the repair. In larger repairs, consideration may be givento using a hip, knee, ankle, foot orthosis. At 4 weeks, the kneeis gradually extended by �30° per week to allow full weight-bearing by 6-8 weeks, while maintaining the use of crutches.Physical therapy is instituted at this point, with the initialphase focused on hip and knee range of motion. Hamstringstrengthening is begun at 10-12 weeks, predicated on fullrange of motion and a painless gait pattern. Full unrestrictedactivity is allowed at approximately 4 months.
SummaryThe surgical approach to hamstring repairs has received lim-ited attention. Those patients with partial tears and chronicbursitis are an even smaller percentage of hamstring prob-lems, with few clinical studies available.23 With the advanceseen in hip arthroscopy, further development of techniquesas allowed us to explore the use of the arthroscope in these
Figure 8 Endoscopic views of the proximal hamstring origin in a lefthip, with the arthroscope in the lateral portal. (A) Knife has beeninserted through the distal portal, and the tendon (biceps/semiten-dinosus) attachment has been incised. (B) The common biceps/semitendinosus origin has been elevated (seen between the arrows).
reviously uncharted areas.
One of the most important aspects in the treatment ofroximal hamstring ruptures is early recognition and treat-ent. With the endoscopic technique, the management may
ertainly evolve to quicker repair of the problem. Patientsith acute repairs have had better outcomes in the literature,
Figure 9 Endoscopic view of the proximal hamstring origin in a left hip,with the arthroscope in the lateral portal. (A) The common BST (ten-don) origin has been incised and elevated. Note the tool is serving toretract the detached tissue. SN, sciatic nerve. (B) Ischial bursa beforedebridement. Note the hypertrophic inflammatory tissue in the bursalspace. (C) Final debridement of bursa. Note the exposed bony surface
at the top of the image.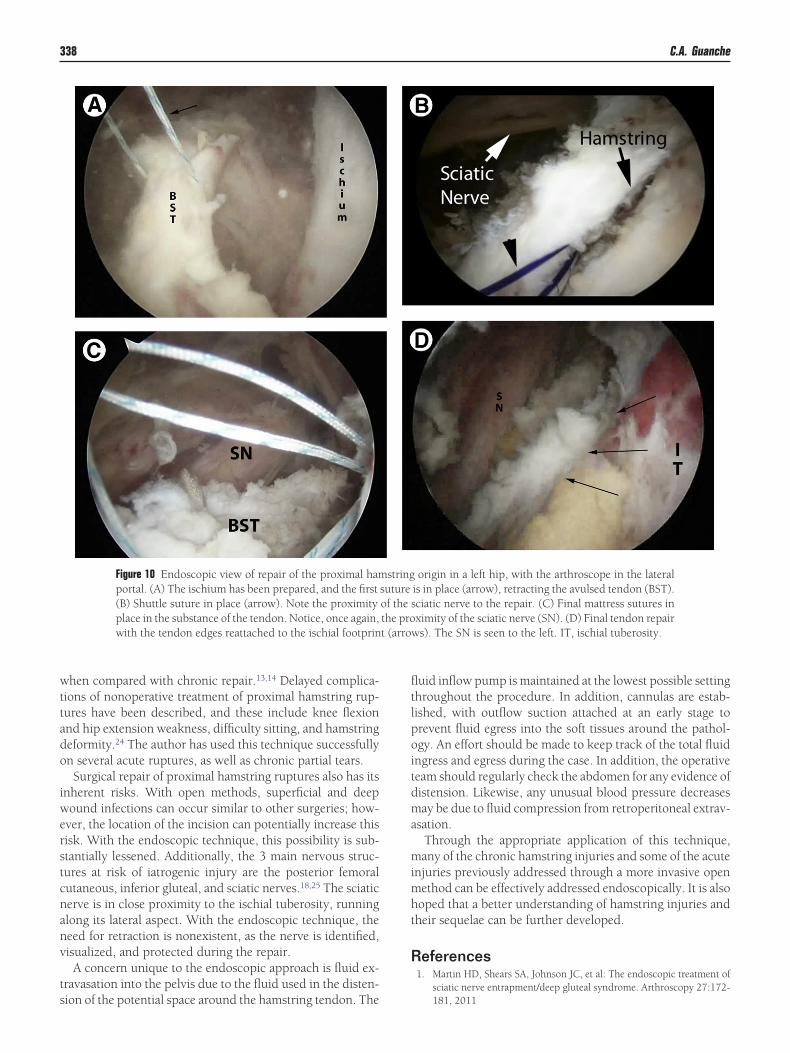
o
iwerstc
t (arro
338 C.A. Guanche
when compared with chronic repair.13,14 Delayed complica-tions of nonoperative treatment of proximal hamstring rup-tures have been described, and these include knee flexionand hip extension weakness, difficulty sitting, and hamstringdeformity.24 The author has used this technique successfullyn several acute ruptures, as well as chronic partial tears.Surgical repair of proximal hamstring ruptures also has its
nherent risks. With open methods, superficial and deepound infections can occur similar to other surgeries; how-
ver, the location of the incision can potentially increase thisisk. With the endoscopic technique, this possibility is sub-tantially lessened. Additionally, the 3 main nervous struc-ures at risk of iatrogenic injury are the posterior femoralutaneous, inferior gluteal, and sciatic nerves.18,25 The sciatic
nerve is in close proximity to the ischial tuberosity, runningalong its lateral aspect. With the endoscopic technique, theneed for retraction is nonexistent, as the nerve is identified,visualized, and protected during the repair.
A concern unique to the endoscopic approach is fluid ex-travasation into the pelvis due to the fluid used in the disten-
Figure 10 Endoscopic view of repair of the proximal hamportal. (A) The ischium has been prepared, and the first(B) Shuttle suture in place (arrow). Note the proximityplace in the substance of the tendon. Notice, once again,with the tendon edges reattached to the ischial footprin
sion of the potential space around the hamstring tendon. The
fluid inflow pump is maintained at the lowest possible settingthroughout the procedure. In addition, cannulas are estab-lished, with outflow suction attached at an early stage toprevent fluid egress into the soft tissues around the pathol-ogy. An effort should be made to keep track of the total fluidingress and egress during the case. In addition, the operativeteam should regularly check the abdomen for any evidence ofdistension. Likewise, any unusual blood pressure decreasesmay be due to fluid compression from retroperitoneal extrav-asation.
Through the appropriate application of this technique,many of the chronic hamstring injuries and some of the acuteinjuries previously addressed through a more invasive openmethod can be effectively addressed endoscopically. It is alsohoped that a better understanding of hamstring injuries andtheir sequelae can be further developed.
References1. Martin HD, Shears SA, Johnson JC, et al: The endoscopic treatment of
sciatic nerve entrapment/deep gluteal syndrome. Arthroscopy 27:172-
origin in a left hip, with the arthroscope in the lateralis in place (arrow), retracting the avulsed tendon (BST).sciatic nerve to the repair. (C) Final mattress sutures inximity of the sciatic nerve (SN). (D) Final tendon repair
ws). The SN is seen to the left. IT, ischial tuberosity.
stringsutureof thethe pro
181, 2011

Proximal hamstring syndrome 339
2. Byrd JWT, Polkowski G, Jones KS: Endoscopic management of thesnapping iliopsoas tendon. Arthroscopy e18, 2009
3. Drez DD, DeLee JC, Miller MD (eds): Orthopaedic Sports Medicine:Principles and Practice, Vol 2. Philadelphia, Saunders, 2003, pp 1481-1523
4. Clanton TO, Coupe KJ: Hamstring strains in athletes: Diagnosis andtreatment. J Am Acad Orthop Surg 6:237-248, 1998
5. Garrett WE Jr: Muscle strain injuries. Am J Sports Med 24:S2-S8, 1996,(6 suppl)
6. Garrett WE Jr, Rich FR, Nikolaou PK, et al: Computed tomography ofhamstring muscle strains. Med Sci Sports Exerc 21:506-514, 1989
7. Elliott MC, Zarins B, Powell JW, et al: Hamstring muscle strains inprofessional football players: A 10-year review. Am J Sports Med 39:843-850, 2011
8. Miller SL, Gill J, Webb GR: The proximal origin of the hamstrings andsurrounding anatomy encountered during repair. A cadaveric study.J Bone Joint Surg Am 89:44-48, 2007
9. Blasier RB, Morawa LG: Complete rupture of the hamstring origin froma water skiing injury. Am J Sports Med 18:435-437, 1990
10. Orava S, Kujala UM: Rupture of the ischial origin of the hamstringmuscles. Am J Sports Med 23:702-705, 1995
11. Klingele KE, Sallay PI: Surgical repair of complete proximal hamstringtendon rupture. Am J Sports Med 30:742-747, 2002
12. Mica L, Schwaller A, Stoupis C, et al: Avulsion of the hamstring musclegroup: A follow-up of 6 adult non-athletes with early operative treat-ment: A brief report. World J Surg 33:1605-1610, 2009
13. Sallay PI, Ballard G, Hamersly S, et al: Subjective and functional out-comes following surgical repair of complete ruptures of the proximalhamstring complex. Orthopedics 31:1092-1096, 2008
14. Sarimo J, Lempainen L, Mattila K, et al: Complete proximal hamstring
avulsions: A series of 41 patients with operative treatment. Am J SportsMed 36:1110-1115, 2008
15. Konan S, Haddad F: Successful return to high level sports followingearly surgical repair of complete tears of the proximal hamstring ten-dons. Int Orthop 34:119-123, 2010
16. Mendiguchia J, Brughelli M: A return-to-sport algorithm for acute ham-string injuries. Phys Ther Sport 12:2-14, 2011
17. Zissen MH, Wallace G, Stevens KJ, et al: High hamstring tendinopathy:MRI and ultrasound imaging and therapeutic efficacy of percutaneouscorticosteroid injection. AJR Am J Roentgenol 195:993-998, 2010
18. Lempainen L, Sarimo J, Mattila K, et al: Proximal hamstring tendinopa-thy: Results of surgical management and histopathologic findings. Am JSports Med 37:727-734, 2009
19. Chakravarthy J, Ramisetty N, Pimpalnerkar A, et al: Surgical repair ofcomplete proximal hamstring tendon ruptures in water skiers and bullriders: A report of four cases and review of the literature. Br J SportsMed 39:569-572, 2005
20. Cross MJ, Vandersluis R, Wood D, et al: Surgical repair of chroniccomplete hamstring tendon rupture in the adult patient. Am J SportsMed 26:785-788, 1998
21. Cohen S, Bradley J: Acute proximal hamstring rupture. J Am AcadOrthop Surg 15:350-355, 2007
22. Birmingham P, Muller M, Wickiewicz T, et al: Functional outcome afterrepair of proximal hamstring avulsions. J Bone Joint Surg Am 93:1819-1826, 2011
23. Harris JD, Griesser MJ, Best TM, et al: Treatment of proximal hamstringruptures—A systematic review. Int J Sports Med 32:490-495, 2011
24. Puranen J, Orava S: The hamstring syndrome. A new diagnosis ofgluteal sciatic pain. Am J Sports Med 16:517-521, 1988
25. Lempainen L, Sarimo J, Heikkilä J, et al: Surgical treatment of partialtears of the proximal origin of the hamstring muscles. Br J Sports Med
40:688-691, 2006




























