Embed Size (px)
Citation preview
1
International Journal of Medical and Dental Case Reports (2018), Article ID 170618, 3 Pages
C A S E R E P O R T
Prosthodontic management of an adolescent with ectodermal dysplasia and skeletal Class III malocclusion: A clinical reportPravin Eknath Raipure, Ravindra Shivdas Pawar, Rahul Shyamrao Kulkarni
Department of Prosthodontics, Nair Hospital Dental College, Mumbai, Maharashtra, India
AbstractOral manifestations of ectodermal dysplasia (ED) include complete or partial hypodontia, anodontia, impacted teeth, loss of occlusal vertical dimension, protuberant lips, malformed and widely spaced teeth, and underdeveloped alveolar ridges. Dental defects associated with this syndrome can cause esthetic, functional, and psychosocial problems. Patients with EDs often present a significant treatment challenge for the restorative dentist owing to the multitude of oral manifestations. This clinical report describes the prosthodontic management of an adolescent with ED using overlay complete denture and ceramometal fixed dental prostheses.
Keywords: Anodontia, complete mouth rehabilitation, ectodermal dysplasia, overlay dentures
Correspondence Pravin Eknath Raipure, Department of Prosthodontics, Nair Hospital Dental College, Mumbai, Maharashtra, India. E-mail: [email protected]
Received 18 May 2018; Accepted 20 June 2018
doi: 10.15713/ins.ijmdcr.91
How to cite this article: Raipure PE, Pawar RS, Kulkarni RS. Prosthodontic management of an adolescent with ectodermal dysplasia and skeletal Class III malocclusion: A clinical report. Int J Med Dent Case Rep 2018;5:0-0.
Introduction
Ectodermal dysplasias (EDs) comprise a large group of congenital developmental disorders of at least two ectoderm-derived structures, such as eccrine sweat glands, teeth, hair, skin, and nails.[1] EDs exhibit cross-related recessive, autosomal dominant, and autosomal recessive patterns of inheritance.[1,2] Congenital malformations of ED include missing or malformed teeth, sparse hair, defective nails, and absence of sweat glands. The syndrome type may often be accompanied by deafness, skeletal anomalies, mental retardation, ichthyosis, palmoplantar keratoderma, eye abnormalities, facial deformities, clefts of the palate and the lip, and other systemic findings.[3,4] Oral anomalies include complete or partial hypodontia, anodontia, impacted teeth, loss of occlusal vertical dimension, protuberant lips, malformed and widely spaced teeth, and underdeveloped alveolar ridges. Dental defects associated with this syndrome can cause esthetic, functional, and psychosocial problems.[5] Patients with EDs often present a significant treatment challenge for the restorative dentist owing to multitude of oral manifestations. Age of the patient is an important factor during treatment planning of patients with ED since restorative options may vary according to chronological and skeletal age of the patients. This clinical report describes prosthodontic management of an adolescent with ED
using overlay complete denture and ceramometal fixed dental prostheses (FDPs).
Case Report
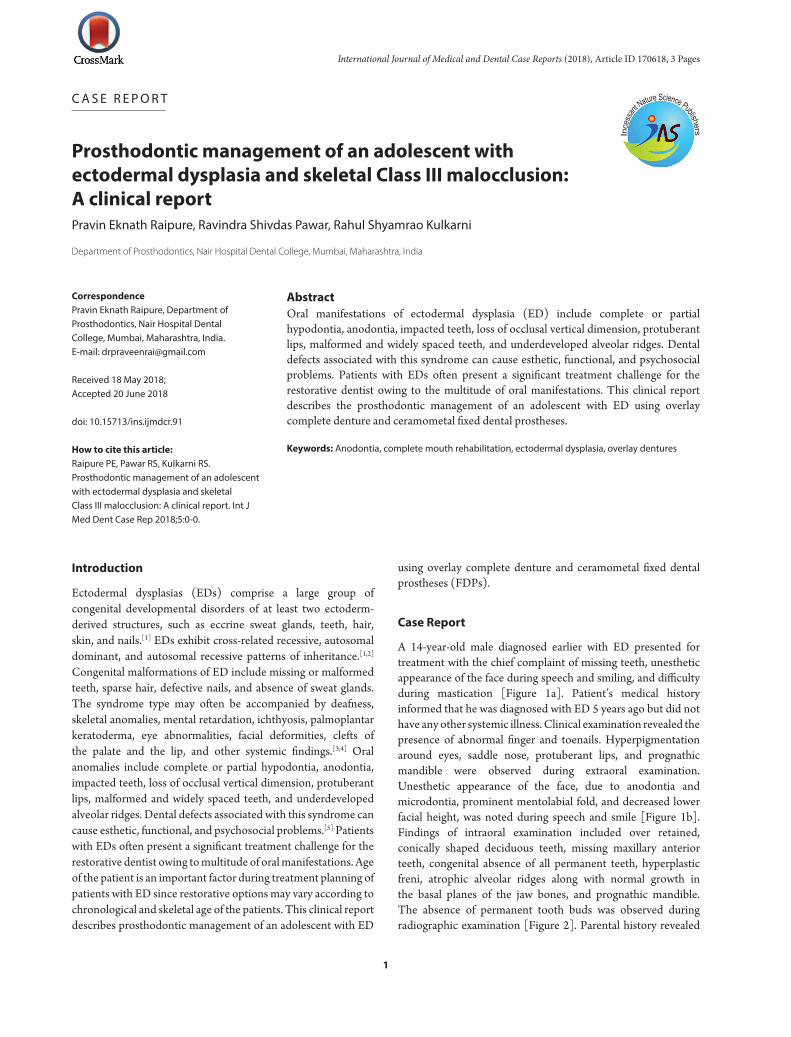
A 14-year-old male diagnosed earlier with ED presented for treatment with the chief complaint of missing teeth, unesthetic appearance of the face during speech and smiling, and difficulty during mastication [Figure 1a]. Patient’s medical history informed that he was diagnosed with ED 5 years ago but did not have any other systemic illness. Clinical examination revealed the presence of abnormal finger and toenails. Hyperpigmentation around eyes, saddle nose, protuberant lips, and prognathic mandible were observed during extraoral examination. Unesthetic appearance of the face, due to anodontia and microdontia, prominent mentolabial fold, and decreased lower facial height, was noted during speech and smile [Figure 1b]. Findings of intraoral examination included over retained, conically shaped deciduous teeth, missing maxillary anterior teeth, congenital absence of all permanent teeth, hyperplastic freni, atrophic alveolar ridges along with normal growth in the basal planes of the jaw bones, and prognathic mandible. The absence of permanent tooth buds was observed during radiographic examination [Figure 2]. Parental history revealed
Raipure, et al. Prosthodontic management of an adolescent with ectodermal dysplasia
2
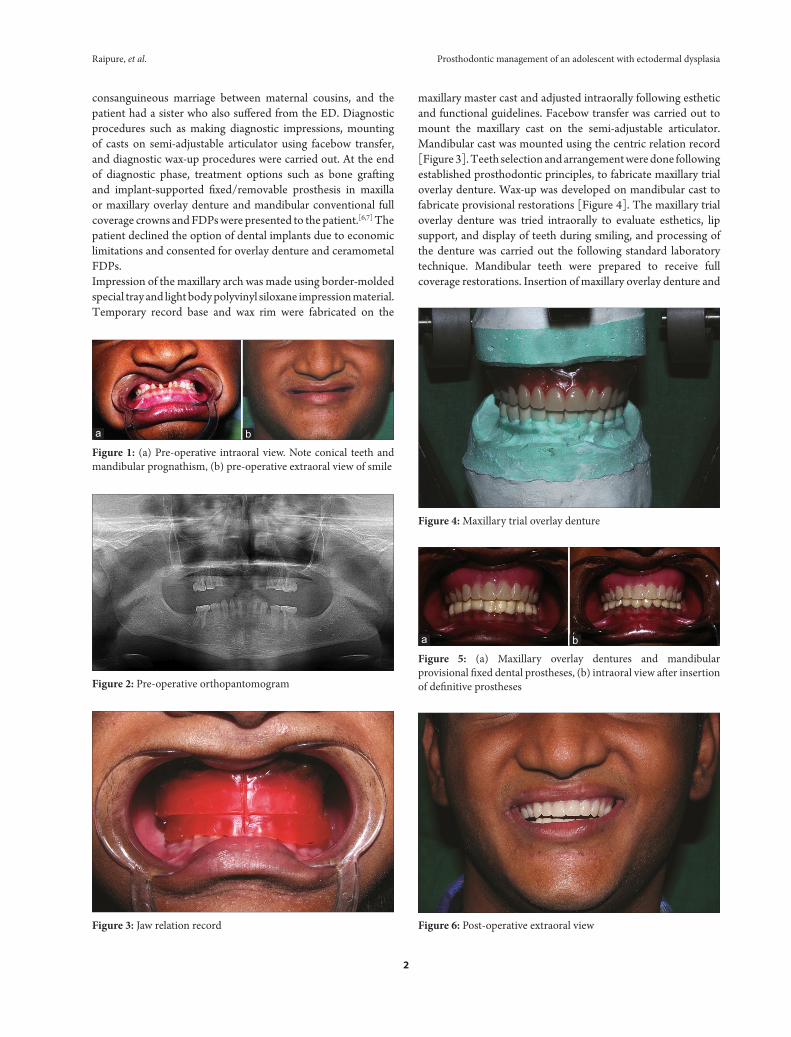
maxillary master cast and adjusted intraorally following esthetic and functional guidelines. Facebow transfer was carried out to mount the maxillary cast on the semi-adjustable articulator. Mandibular cast was mounted using the centric relation record [Figure 3]. Teeth selection and arrangement were done following established prosthodontic principles, to fabricate maxillary trial overlay denture. Wax-up was developed on mandibular cast to fabricate provisional restorations [Figure 4]. The maxillary trial overlay denture was tried intraorally to evaluate esthetics, lip support, and display of teeth during smiling, and processing of the denture was carried out the following standard laboratory technique. Mandibular teeth were prepared to receive full coverage restorations. Insertion of maxillary overlay denture and
Figure 2: Pre-operative orthopantomogram
Figure 3: Jaw relation record
Figure 4: Maxillary trial overlay denture
consanguineous marriage between maternal cousins, and the patient had a sister who also suffered from the ED. Diagnostic procedures such as making diagnostic impressions, mounting of casts on semi-adjustable articulator using facebow transfer, and diagnostic wax-up procedures were carried out. At the end of diagnostic phase, treatment options such as bone grafting and implant-supported fixed/removable prosthesis in maxilla or maxillary overlay denture and mandibular conventional full coverage crowns and FDPs were presented to the patient.[6,7] The patient declined the option of dental implants due to economic limitations and consented for overlay denture and ceramometal FDPs.Impression of the maxillary arch was made using border-molded special tray and light body polyvinyl siloxane impression material. Temporary record base and wax rim were fabricated on the
Figure 6: Post-operative extraoral view
Figure 5: (a) Maxillary overlay dentures and mandibular provisional fixed dental prostheses, (b) intraoral view after insertion of definitive prostheses
ba
Figure 1: (a) Pre-operative intraoral view. Note conical teeth and mandibular prognathism, (b) pre-operative extraoral view of smile
ba

Prosthodontic management of an adolescent with ectodermal dysplasia Raipure, et al.
3
cementation of mandibular provisional heat-polymerized FDPs were carried out [Figure 5a]. The patient wore the provisional restorations for 3 months and was evaluated periodically. During the evaluation period, the patient’s anterior speaking space and function were assessed. The muscles of mastication and the temporomandibular joint were evaluated for clinical signs of discomfort, and it was observed that the patient was asymptomatic and comfortable during this period. Final tooth modifications and gingival retraction were carried out in the mandibular arch, and impression was recorded in polyvinyl siloxane impression material using putty wash technique. Definitive cast was obtained by pouring impression in Type IV dental stone. Bite registration was made using provisional FDPs and occlusal registration material in sections. Individual ceramometal crowns and FDPs were fabricated for mandibular teeth and cemented using zinc phosphate cement [Figure 5b]. Written instructions were provided to the patient regarding maintenance and use of overlay denture. The patient recall visits were scheduled at every 3 months for a period of 1 year, during which an improvement in esthetics, speech, function, and socializing was noted [Figure 8].
Discussion
Prosthetic rehabilitation of patients with ED presents special challenges to the dental profession, and a multidisciplinary approach involving pedodontist, orthodontist, oral surgeon, and prosthodontist is often necessary.[5] It is advantageous if the treatment commences during childhood, since an opportunity to use growth-adapted measures exists in the planning of dental treatment. Due to the lack of teeth and deviant facial and dental appearance, these cases may experience social and psychosocial problems. Furthermore, the need for treatment varies at different ages and requires continuous planning in close cooperation with the patient and family throughout the years of childhood and adolescence.[5] Prosthodontic treatment for adolescent ED cases usually comprises of providing interim partial dentures, conventional complete dentures, overlay dentures, or fixed prostheses such as conventional FDPs and dental implants.[6,7] Dental implant prostheses represent the best alternative since they help to preserve the alveolar bone.[5] In regions of tooth agenesis, the buccolingual width of the alveolar process is often insufficient, which may be an indication for bone augmentation procedures.
Autotransplantation of the second or third molars to the premolar region in patients with both premolar missing also has been shown to have a good prognosis.[5] In the present case, alternative treatment plan could have been the surgical augmentation maxillary alveolar bone and implant therapy.[6,7] However, these options were ruled out by the patient due to financial constraints. Hence, conventional overlay dentures and FDPs were prescribed. The overlay denture needs to be remade periodically in this patient to match his maxillary skeletal and facial growth. The patient was advised to follow denture hygiene instructions, use fluoride mouthwash, and brush twice a day following proper technique to achieve long-term favorable prognosis. The patient’s esthetic and functional expectations were satisfied, and he did not have sensitivity or pain after the treatment.
Summary
This clinical report demonstrates that overlay dentures and conventional FDPs can be a favorable and economic method of the treatment for ED patients. For the patient described, the treatment improved esthetics, oral function, and social confidence.
References
1. Trzeciak WH, Koczorowski R. Molecular basis of hypohidrotic ectodermal dysplasia: An update. J Appl Genet 2016;57:51-61.
2. Rad AS, Siadat H, Monzavi A, Mangoli AA. Full mouth rehabilitation of a hypohidrotic ectodermal dysplasia patient with dental implants: A clinical report. J Prosthodont 2007;16:209-13.
3. Vieira KA, Teixeira MS, Guirado CG, Gaviäo MB. Prosthodontic treatment of hypohidrotic ectodermal dysplasia with complete anodontia: Case report. Quint Int 2007;38:75-80.
4. Tarjan I, Gabris K, Rozsa N. Early prosthetic treatment of patients with ectodermal dysplasia: A clinical report. J Prosthet Dent 2005;93:419-24.
5. Bergendal B. Prosthetic habilitation of a young patient with hypohidrotic ectodermal dysplasia and oligodontia: A case report of 20 years of treatment. Int J Prosthodont 2001;14:471-9.
6. Kramer FJ, Baethge C, Tschernitschek H. Implants in children with ectodermal dysplasia: A case report and literature review. Clin Oral Impl Res 2007;18:140-6.
7. Sweeney IP, Ferguson JW, Heggie AA, Lucas JO. Treatment outcomes for adolescent ectodermal dysplasia patients treated with dental implants. Int J Paed Dent 2005;15:241-8.




























