Embed Size (px)
Citation preview

British Journalof Urology (1991), 61 ,434443 0 1991 British Journal of Urology
Case Reports
Prostate Carcinoma Metastatic to the Male Breast
F. J. ALLEN and D. J. J. VAN VELDEN, Departmentsof Urology and Pathology. University of Stellenbosch. Tygerberg, Sooth Africa
Case Report A.S. was referred to this department in September 1988 with metastatic prostate carcinoma. Two years previously he had presented elsewhere with abdominal pain and weight loss. Cervical lymphadenopathy was noted and biopsy revealed poorly differentiated adenocarcinoma in the lymph nodes. Computed tomography at that time revealed retroperitoneal lymphadenopathy and the pa- tient received chemotherapy. Three months later sclerotic bone metastases were noted, a diagnosis of prostatic carcinoma was made and the patient was treated with stilboestrol with a good response. In May 1988 he was
seen by the Radiotherapy Department at this hospital with severe bone pain and was treated by half-body irradiation, again with a reasonable response. At this stage he stopped using stilboestrol. When seen by us he complained of weight loss, pain, enlarged lymph nodes and painful enlarged breasts. On examination he was cachexic and cervical and axillary lymphadenopathy was noted. There was also marked bilateral gynaecomastia which was stony hard in consistency. Rectal examination revealed a small clinically benign prostate. Total acid phosphatase was raised at 324.2 u/l (normal range 4.8- 13.5) with a prostatic fraction of 272.7 u/l (normal < 3.7). Alkaline phosphatase was 235 u/l (normal range 30-85) and lactate dehydrogenase 662 u/l (normal range 100- 350). A radioisotope bone scan revealed multiple metas- tases. Bilateral orchiectomy was performed together with biopsy of the unusually hard gynaecomastia under local anaesthesia.
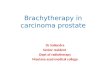
Histology revealed male breast tissue invaded by poorly differentiated adenocarcinoma cells which stained positively for both prostatic acid phosphatase and prostate specific antigen (PSA) using immunohistochem- ical staining with polyclonal antibodies (Fig.).
Despite the reintroduction of hormonal treatment the patient deteriorated rapidly and died 3 months later (December, 1988).
Fig. Two normal breast ducts and numerous carcinoma cells staining positively for PSA. ( x 400).
434

CASE REPORTS 435
Comment
Prostate carcinoma is classically associated with osseous or lymphatic metastases, but unusual sites of metastases have been reported and immunohis- tochemical staining techniques have proved valua- ble in localisation of metastatic adenocarcinoma to a prostatic origin (Venable et al., 1983). Metastatic prostate carcinoma to the breast is uncommon and although proof of the prostatic origin has been lacking in most early reports, Naritoku and Taylor (1 983) reported 2 cases where immunocytochemical demonstration of PSA and prostatic acid phospha- tase were performed. Most of the earlier cases have been associated with diffuse metastatic disease and the patients were on oestrogen treatment when the breast malignancy was discovered (Drelichman et a/., 1980). One can only speculate as to whether gynaecomastia associated with oestrogens, by in- creasing local blood supply, encourages metastases to this site.
References Drelichman, A., Amer, M., Pontes, E. etal. (1980). Carcinoma of
the prostate metastatic to breast. Urology, 16,250-255. Naritoku, W. Y. and Taylor, C. R. (1983). Immunohistologic
diagnosis of 2 cases of metastatic prostate cancer to breast. J . Urol., 130, 365-361.
Venable, D. D., Hastings, D. and Misra, R. P. (1983). Unusual metastatic patterns of prostate adenocarcinoma. J . Urol., 130, 980-985.
Requests for reprints to: F. J . Allen, Department of Urology, Faculty of Medicine, University of Stellenbosch, P.O. Box 63, Tygerberg 7505, Republic of South Africa.
An Unusual Case of Bladder Perforation
E. L. VAN THILLO, Department of Urology, University Hospital of St Pieter, Leuven, Belgium
Case Report A 53-year-old male presented with several episodes of lower urinary tract infection despite appropriate anti- biotic therapy.
Eleven years previously he had survived an anterior wall myocardial infarction and 5 years previously an automatic defibrillator had been implanted after episodes of severe ventricular arrhythmia; 3 years previously the defibrillator had been replaced with an automatic
cardioverter-defibrillator which was implanted into a previous left abdominal pocket. Since the patient showed no arrhythmia during several Holter monitor recordings, the defibrillator was deactivated.
Intravenous urography was performed because of the persistent urinary tract infection and this suggested the presence of defibrillator leads within the bladder. This was confirmed by cystoscopy.
We extracted the defibrillator and sutured the urinary bladder. The leads were left properly fixed into the rectus muscle. The patient’s clinical course was uneventful.
Comment
In a series of 112 patients receiving this implant this complication did not occur (Mirowski, 1985) and in our patient it was due to pressure necrosis with perforation of the roof of the bladder.
Reference Mirowski, M. (1985). The automatic implantable cardioverter-
defibrillator: an overview. J . Am. CON. Cardiol., 6,461-466.
Requests for reprints to: E. L. Van Thillo, Department of Urology, University Hospital of St Pieter, Brusselsestraat 69, 3000 Leuven, Belgium.
Combination of Chemolysis and Extracorporeal Shock Wave Lithotripsy in Cystine Urolithiasis
H. VANDEURSEN and L. BAERT, Department of Urology, University Hospital of St Pieter, Leuven, Belgium
Extracorporeal shock wave lithotripsy (ESWL) and endoscopic contact lithotripsy have failed to disin- tegrate cystine calculi (Dretler, 1988) but the newer extracorporeal lithotriptors cause fragmentation of cystine stones and, when combined with intensive chemolysis, accelerate dissolution by increasing the contact surface for chemolytic agents (Schmeller et al., 1984).
Case Report A 50-year-old female presented with left colicky pain. A right nephrectomy had been performed previously be- cause of pyonephrosis due to an infected staghorn stone and analysis confirmed it was composed of cystine. Despite preventive medical treatment, a left staghorn stone recurred within 6 years.