Embed Size (px)
Citation preview

Prospective Comparison of FlecainideVersus Sotalol for Immediate
Cardioversion of Atrial FibrillationJohann Reisinger, MD, Edmund Gatterer, MD, Georg Heinze, MSc, Kurt Wiesinger, MD,
Eduard Zeindlhofer, MD, Martin Gattermeier, MD, Gerhard Poelzl, MD,Horst Kratzer, MD, Anton Ebner, MD, Wolfgang Hohenwallner, MD, Kurt Lenz, MD,
Joerg Slany, MD, and Peter Kuhn, MD
This study sought to compare the efficacy and safety ofintravenous flecainide and sotalol for immediate cardio-version of atrial fibrillation. We performed a prospec-tive, randomized, single-blind, multicenter trial, includ-ing 106 hemodynamically stable patients with atrialfibrillation, stratified according to duration of the ar-rhythmia. Exclusion criteria included severely reducedleft ventricular systolic function, recent antiarrhythmictherapy, and hypokalemia. Patients were randomly as-signed to receive either intravenous flecainide or intra-venous sotalol. Trial medication was given at a dose of1.5 mg/kg body weight (maximum 150 mg). Overall,
28 of 54 patients (52%) given flecainide and 12 of 52patients (23%) given sotalol converted to sinus rhythmduring the first 2 hours after start of the infusion (p 50.003). Multivariate analysis confirmed that treatmentallocation to flecainide, an arrhythmia duration of <24hours, higher plasma magnesium level at baseline,higher age for men, and lower age for women indepen-dently increases the probability of conversion. The fre-quency of adverse effects was not significantly differentin the 2 treatment groups. Q1998 by Excerpta Medica,Inc.
(Am J Cardiol 1998;81:1450–1454)
A trial fibrillation (AF) is the most frequently en-countered arrhythmia in clinical practice. Phar-
macologic therapy is often the first means of attempt-ing reversion of AF, and several drug trials for acuteconversion of AF have included flecainide (a class ICdrug)1–7or sotalol (a class III antiarrhythmic drug withb-blocker effects).8–11However, no direct comparisonhas yet been performed. Thus, the purpose of thisprospective, randomized, single-blind trial was tocompare the efficacy and safety of flecainide andsotalol for immediate conversion of AF.
METHODSStudy patients: Patients were considered possible
candidates for entry into the study if there was sus-tained AF lasting$15 minutes to#6 months with aventricular rate$80 beats/min at rest. Patients withatrial flutter were not eligible. Exclusion criteria wereclinical signs of congestive heart failure (New YorkHeart Association functional class.II), severely re-duced left ventricular systolic function (mean left ven-tricular fractional shortening,20%), unstable anginapectoris, acute myocardial infarction within the pre-ceding 6 weeks, hypotension (systolic blood pressure
,100 mm Hg), obstructive pulmonary disease, recentantiarrhythmic therapy (treatment with antiarrhythmicagents of class I to IV within the previous 48 hours oramiodarone within the previous 6 months), any pre-viously documented conduction disturbances of morethan first-degree atrioventricular block or sick sinussyndrome (unless protected by a permanent pacemak-er), prolongation of the corrected QT (QTc) interval(.450 ms), AF lasting$48 hours without appropriateanticoagulation therapy, compromised renal function(i.e., serum creatinine.2.5 mg/dl), hepatic insuffi-ciency, uncorrected hypokalemia, flecainide or sotalolhypersensitivity, pregnancy and lactation, age,16 or.85 years, and inability or unwillingness to givewritten informed consent. The study protocol wasapproved by the institutional committees on humanresearch of the participating hospitals.
Data collection: Complete medical history, physicalexamination, routine laboratory results (including thy-roid function tests), 12-lead electrocardiogram, and anechocardiogram were obtained at baseline evaluation.Cardiac rhythm was monitored continuously and ve-nous blood samples for determination of plasma druglevels were taken 2 hours after start of the infusion.
Enrollment and drug administration: Patients wereprospectively stratified according to duration of thearrhythmia (group I:$15 minutes to#24 hours;group II:.24 hours to#7 days; group III:.7 days to#6 months). In each group patients were randomlyallocated to receive either flecainide (Aristocor, F.Joh. Kwizda, Vienna, Austria) or sotalol (Sotacor,Bristol-Myers Squibb, Vienna, Austria), which areboth approved drugs in Austria. Trial medication wasgiven by infusion over 15 minutes at a dose of
From the Departments of Internal Medicine and Laboratory Medicine,Krankenhaus Barmherzige Schwestern, Linz; Department of InternalMedicine, Krankenanstalt Rudolfstiftung, Vienna; Department of Med-ical Computer Sciences, Section of Clinical Biometrics, University ofVienna, Vienna; and Department of Internal Medicine, KrankenhausBarmherzige Brueder, Linz, Austria. This study was supported byresearch grants from F. Joh. Kwizda GmbH, and Bristol-Myers SquibbGmbH, Vienna, Austria. Manuscript received September 11, 1997;revised manuscript received and accepted February 18, 1998.
Address for reprints: Johann Reisinger, MD, Department of InternalMedicine, Krankenhaus Barmherzige Schwestern, Seilerstaette 4,A-4020 Linz, Austria.
1450 ©1998 by Excerpta Medica, Inc. 0002-9149/98/$19.00All rights reserved. PII S0002-9149(98)00223-9
1.5 mg/kg body weight (maximum 150 mg) and allpatients were monitored for 2 hours.
Study end points: The primary end point was con-version of AF to sinus rhythm within 2 hours ofstarting medication. The secondary end points werethe influence of various clinical or echocardiographicfactors on the probability of conversion, the relationbetween plasma drug levels and effectiveness, differ-ences in the frequency of adverse events, and differ-ences between the 2 drugs in slowing of the ventric-ular rate in nonconverters.
Statistics: The sample size was determined in ad-vance based on the following assumptions: With atype I error of 0.05 (2-sided), a type II error of 0.20, adifference in conversion rates between the 2 drugs of20%, and a mean conversion rate of 50%, the calcu-lated total study population was 212. An interim anal-ysis after inclusion of half of the intended sample size(i.e., 106 patients) was planned ahead in order toterminate the study earlier according to a group se-quential design by Geller and Pocock.12 Mean val-ues6 SD are given for continuous variables if nor-mally distributed, and median values are given fordata with an asymmetric distribution. Comparisons ofconversion rates between groups were made by thechi-square test and differences in continuous variableswere analyzed by means of thet test for independentsamples. The method of Kaplan and Meier13 was usedto construct estimates of the cumulative proportion ofpatients reverting to sinus rhythm in each treatmentgroup over time (BMDP Statistical Software, Version1990, Los Angeles, California) which were then com-pared by the Mantel test.14
To identify which clinical or echocardiographic fac-tors predicted conversion, a multivariate analysis(stepwise logistic regression)15 using the StatisticalAnalysis System Software Version 6.11 (SAS Insti-tute Inc., Cary, North Carolina) was performed. Oddsratios (OR) and 95% confidence intervals (CI) werecalculated with standard methods. A p value ,0.05was considered statistically significant.
RESULTSPatient characteristics: Altogether, 106 hospitalized
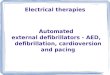
patients meeting inclusion and exclusion criteria wereenrolled into the trial (Table I). Regarding underlyingdisease, 31 patients had systemic hypertension (13with and 18 without left ventricular hypertrophy), 15had coronary artery disease (11 with prior myocardialinfarction), 10 had valvular heart disease, 2 dilatedcardiomyopathy, 3 acute pulmonary embolism, 1chronic pulmonary hypertension, 3 previously undi-agnosed hyperthyroidism, 1 sick sinus syndrome (withimplanted atrial pacemaker), and 1 patient had hadpericardectomy due to constrictive pericarditis. In 3patients AF was triggered by alcohol and in 1 patientby an atrioventricular nodal reentrant tachycardia. In 2patients AF occurred#24 hours after noncardiac sur-gery, and in 33 patients no discernible cause of AFcould be evaluated (idiopathic AF).
Response to randomized therapy: Overall, 28 of 54patients (52%; 95% CI 38% to 66%) given flecainide
and 12 of 52 patients (23%; 95% CI 13% to 37%)given sotalol converted to sinus rhythm during the first2 hours after start of the infusion (p5 0.003). Therewas a statistically significant difference in the distri-butions of the time intervals to conversion for patientstreated with flecainide and those treated with sotalol(p 5 0.0008) (Figure 1). Conversion rates of bothdrugs varied considerably depending on duration ofthe arrhythmia (Figure 2). If AF was present for#24hours, conversion to sinus rhythm was achieved in 24of 35 patients (69%) in the flecainide group and in 11of 36 (31%) in the sotalol group (p5 0.004). Theconversion rates were 4 of 9 (44%) and 1 of 6 (17%),respectively, for arrhythmia previously present for.24 hours to#7 days (p5 0.58). None of 20 patientswith AF of .7 days’ duration reverted to sinusrhythm.
Multivariate analysis (logistic regression): Multivar-iate analysis (Table II) revealed that treatment alloca-tion to flecainide, an arrhythmia duration of#24hours, higher plasma magnesium level at baseline,higher age for men and lower age for women inde-pendently increase the probability of conversion.None of the other variables, including left atrial size,
TABLE I Baseline Patient Data
Flecainide(n 5 54)
Sotalol(n 5 52)
Age (yr) 65 6 12 59 6 15Men/women 30/24 31/21Body weight (kg) 78 6 14 77 6 13Body mass index (kg/m2) 27.0 6 3.5 26.7 6 4.0Duration of atrial fibrillation (AF)
median (d)0.53 0.41
Interquartile range (d) 0.17–1.50 0.18–1.48Group I ($15 min to #24 h) 35 (65%) 36 (69%)
Duration of AF, median (h) 5.9 6.4Group II (.24 h to #7 d) 9 (17%) 6 (12%)
Duration of AF, median (h) 30.3 44.3Group III (.7 d to #6 mo) 10 (18%) 10 (19%)
Duration of AF, median (d) 55 80Recurrent atrial fibrillation 29 (54%) 33 (63%)Ventricular rate at entry
(beats/min)122 6 29 119 6 27
Systolic blood pressure (mm Hg) 133 6 22 139 6 19Diastolic blood pressure
(mm Hg)85 6 15 85 6 13
Left atrial anteroposterior size(mm)
42 6 6 40 6 9
Left atrial superior-inferior size(mm)
58 6 8 57 6 8
Reduced systolic left ventricularfunction
15 (28%) 14 (27%)
Hypertension 15 (28%) 16 (31%)Coronary artery disease 9 (17%) 6 (12%)Valvular heart disease 5 (9%) 5 (10%)Idiopathic atrial fibrillation 17 (32%) 16 (31%)Plasma potassium (mmol/L) 4.0 6 0.3 3.9 6 0.4Plasma magnesium (mmol/L) 0.86 6 0.15 0.88 6 0.14Concomitant treatment with
digoxin12 (22%) 14 (27%)
Values are expressed as mean 6 SD, median, or number (%) of patients.Reduced left ventricular systolic function was defined as a mean left ventric-
ular fractional shortening ,28%.
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/FLECAINIDE VERSUS SOTALOL FOR AF 1451

reduced left ventricular systolicfunction, idiopathic AF, recur-rent AF, or concomitant use ofdigoxin, predicted the probabil-ity of conversion.
Plasma drug levels: Meanplasma flecainide levels in pa-tients who received the drugwere 111 6 42 ng/ml, meanplasma sotalol levels were820 6 107 ng/ml. With bothdrugs the plasma levels were notsignificantly different in patientsreverting versus not reverting tosinus rhythm.
Adverse effects: Adverse ef-fects were reported in 9 of the54 flecainide-treated patients(17%) and in 10 of the 52 pa-tients receiving sotalol (19%)(p 5 NS), and included mainlyasymptomatic hypotension (5
episodes in each group) and brady-cardia (1 with flecainide and 2 withsotalol). A single episode of torsadesde pointes in conjunction with acutecongestive heart failure developedafter infusion of sotalol in a patientwith reduced left ventricular func-tion.
Changes in ventricular rate in non-converters: Among nonconverters,treatment with sotalol was associatedwith a significantly slower ventricu-lar rate than treatment with flecainide(79 6 20 vs 1046 26 beats/min;p 5 0.0001 for comparison of ven-tricular rates after 2 hours).
DISCUSSIONThis study shows that flecainide
is significantly more effective thansotalol for immediate conversion ofrecent-onset AF.
Comparison with previous studies:Flecainide has been studied in a largenumber of randomized trials foracute termination of a recent-onsetepisode of AF and was found to beequally effective as quinidine, butacting more rapidly1 and more effec-tively than verapamil,2 digoxin,3amiodarone,4 procainamide,5 andpropafenone.6 Our conversion ratefor flecainide in patients with AF of#24 hours’ duration compares fa-vorably with that recently reportedfor ibutilide.16 Randomized trialsfound sotalol as effective for conver-sion as digoxin plus disopyramide(after cardiac surgery)8 but less ef-fective than quinidine9 or digoxin
FIGURE 1. Cumulative conversion rates (%) of AF for flecainide (continuous line) and sotalol(dashed line) based on time after start of drug infusion.
FIGURE 2. Effect of arrhythmia duration on conversion rate with flecainide (solidbars) and sotalol (open bars) in AF (Group I: >15 minutes to <24 hours; Group II:>24 hours to <7 days; Group III: >7 days to <6 months).
TABLE II Predictors of Conversion (multivariate analysis)
Variable Unit OR (95% CI) p Value
Treatment allocation Flecainide/sotalol 7.32 (2.04–26.22) 0.0022Duration of atrial fibrillation #/.24 h 13.85 (2.99–64.21) 0.0008Plasma magnesium level 0.1 mmol/L 1.91 (1.21–3.00) 0.0052Age (male patients) 10 yr 4.44 (1.22–16.11) 0.0038*Age (female patients) 10 yr 0.33 (0.13–0.84)
*This p value refers to the significant interaction between age and sex. Odds ratio (OR) approximateshow much more likely a conversion would occur if a patient’s variable value was increased by the valuelisted in the unit column. For dichotomous variables such as treatment allocation, the OR with the unitflecainide/sotalol estimates how much more likely a conversion would occur in patients treated withflecainide than with sotalol.
CI 5 confidence interval, OR 5 odds ratio.
1452 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 81 JUNE 15, 1998

plus quinidine.10 The poor efficacy of sotalol in ourstudy is consistent with a recent placebo-controlledtrial11 in which sotalol was not effective for termina-tion at doses up to 1.5 mg/kg.
Possible mechanisms underlying efficacy of therapy:AF is widely believed to result from multiple reentrantcircuits.17,18 The minimum size of a circuit is relatedto the electrical wavelength (5 conduction velocity3effective refractory period). The antiarrhythmic effectof drugs on AF has been correlated with their ability toprolong the electrical wavelength,19 thereby reducingthe possible number of simultaneous wavefrontswithin the finite area of the atria until conductionfailure leads to arrhythmia termination. Flecainideslows atrial conduction and increases the atrial refrac-tory period.20 The effects on refractoriness predomi-nate as indicated by drug-induced increases in thewavelength, which are substantial even at short atrialcycle lengths as in AF. Sotalol’s ability to increase theatrial effective refractory period without changingconduction velocity21 is typical for its class III action,but the resultant effects on wavelength are reduced ascycle length decreases, paralleling its diminished ac-tions on the effective refractory period (reverse use-dependence). This property may explain the discrep-ancy between sotalol’s efficacy in preventing22,23 andits inefficacy in terminating rapid reentrant arrhyth-mias such as AF21,24 in contrast to the newer class IIIagent ibutilide, which maintains its effects on refrac-toriness even at high atrial rates.25
Duration of atrial fibrillation and efficacy of acutetherapy: Our results are consistent with the findings ofprevious drug studies which showed that the ability ofclass IC agents to terminate AF decreases with in-creasing duration of the arrhythmia.1,6 Even during thefirst days of AF, marked electrophysiologic changestake place in the atria that clearly favor the perpetua-tion of AF.26,27 The reduced conduction velocity oc-curring with long-standing AF decreases the electricalwavelength, making the arrhythmia intrinsically moreresistant; this may sensitize the tissue to conduction-slowing actions of flecainide, offsetting the increasesin refractoriness caused by the drug.
Possible role of magnesium: Similar to results of arecently published study,28 our results support theview that magnesium may play a significant role in theconversion of AF and consequently should deservefurther consideration as adjunctive therapy in thissetting.
Interaction between age and sex: This significantinteraction may be related to gender-specific differ-ences in repolarization time, which is known to begreater at the ventricular level in premenopausalwomen than in men and to equalize after meno-pause.29 This finding may also be valid at the atriallevel, thereby promoting the efficacy of antiarrhyth-mic drugs (which prolong the atrial refractory period)in women of lower age with AF.
Study limitations: Our trial did not have a placebogroup due to our concerns leaving symptomatic pa-tients untreated. The trial was only single blind, butthe primary end point of the study was not prone to
subjective assessment. The absence of a significantdifference in response in patients with AF of.24hours’ duration may be due to the small number ofpatients enrolled.
Conclusions: Conversion to sinus rhythm within 2hours by flecainide or sotalol was limited to patientswith AF of recent onset. At the doses used in thisstudy, flecainide was significantly more effective thansotalol for immediate conversion of AF. This is con-sistent with the different drug-induced changes inwavelength at rapid atrial rates. Besides treatmentallocation and arrhythmia duration, plasma magne-sium level and an interaction between age and sexwere independent predictors of conversion.
Acknowledgment: We thank Thomas Quinton,MD, Hans Keller, MD, and the staff of the intensivecare units at the participating hospitals for their sup-port and assistance in patient recruitment. We areindebted to Rodney H. Falk, MD, for critical review ofthe manuscript.
1. Borgeat A, Goy JJ, Maendly R, Kaufmann U, Grbic M, Sigwart U. Flecainideversus quinidine for cardioversion of atrial fibrillation to sinus rhythm.Am JCardiol 1986;58:496–498.2. Suttorp MJ, Kingma JH, Lie-A-Huen L, Mast EG. Intravenous flecainideversus verapamil for acute conversion of paroxysmal atrial fibrillation or flutter tosinus rhythm.Am J Cardiol1989;63:693–696.3. Wafa SS, Ward DE, Parker J, Camm AJ. Efficacy of flecainide acetate for atrialarrhythmias following coronary artery bypass grafting.Am J Cardiol1989;63:1058–1064.4. Capucci A, Lenzi T, Boriani G, Trisolini G, Binetti N, Cavazza M, Fontana G,Magnani B. Effectiveness of loading oral flecainide for converting recent-onsetatrial fibrillation to sinus rhythm in patients without organic heart disease or withonly systemic hypertension.Am J Cardiol1992;70:69–72.5. Madrid AH, Moro C, Marin-Huerta E, Mestre JL, Novo L, Costa A. Compar-ison of flecainide and procainamide in cardioversion of atrial fibrillation.EurHeart J 1993;14:1127–1131.6. Suttorp MJ, Kingma JH, Jessurun ER, Lie-A-Huen L, van Hemel NM, Lie KI.The value of class IC antiarrhythmic drugs for acute conversion of paroxysmalatrial fibrillation or flutter to sinus rhythm.J Am Coll Cardiol1990;16:1722–1727.7. Donovan KD, Power BM, Hockings BEF, Dobb GJ, Lee K-Y. Intravenousflecainide versus amiodarone for recent-onset atrial fibrillation.Am J Cardiol1995;75:693–697.8. Campell TJ, Gavaghan TP, Morgan JJ. Intravenous sotalol for the treatment ofatrial fibrillation and flutter after cardiopulmonary bypass: comparison withdisopyramide and digoxin in a randomised trial.Br Heart J 1985;54:86–90.9. Hohnloser SH, van de Loo A, Baedeker F. Efficacy and proarrhythmic hazardsof pharmacologic cardioversion of atrial fibrillation: prospective comparison ofsotalol versus quinidine.J Am Coll Cardiol1995;26:852–858.10. Halinen MO, Huttunen M, Paakkinen S, Tarssanen L. Comparison of sotalolwith digoxin-quinidine for conversion of acute atrial fibrillation to sinus rhythm(the Sotalol-Digoxin-Quinidine Trial).Am J Cardiol1995;76:495–498.11. Sung RJ, Tan HL, Karagounis L, Hanyok JJ, Falk R, Platia E, Das G, HardySA, and the Sotalol Multicenter Study Group. Intravenous sotalol for the termi-nation of supraventricular tachycardia and atrial fibrillation and flutter: a multi-center, randomized, double-blind, placebo-controlled study.Am Heart J1995;129:739–748.12. Geller NL, Pocock SJ. Interim analyses in randomized clinical trials: rami-fications and guidelines for practitioners.Biometrics1987;43:213–223.13. Kaplan EL, Meier P. Nonparametric estimation from incomplete observa-tions.J Am Stat Assoc1958;53:457–481.14. Mantel N. Evaluation of survival data and two new rank order statisticsarising in its consideration.Cancer Chemother Rep1966;50:163–170.15. Hosmer DW, Lemeshow S. Applied Logistic Regression. 1st ed. New York:John Wiley, 1989.16. Stambler BS, Wood MA, Ellenbogen KA, Perry KT, Wakefield LK,VanderLugt JT, and the Ibutilide Repeat Dose Study Investigators. Efficacy andsafety of repeated intravenous doses of ibutilide for rapid conversion of atrialflutter or fibrillation.Circulation 1996;94:1613–1621.
ARRHYTHMIAS AND CONDUCTION DISTURBANCES/FLECAINIDE VERSUS SOTALOL FOR AF 1453

17. Moe GK. On the multiple wavelet hypothesis of atrial fibrillation.Arch IntPharmacodyn Ther1962;140:183–188.18. Allessie MA, Konings K, Kirchhof CJHJ, Wijffels M. Electrophysiologicmechanisms of perpetuation of atrial fibrillation.Am J Cardiol 1996;77:10A–23A.19. Rensma PL, Allessie MA, Lammers WJEP, Bonke FIM, Schalij MJ. Lengthof excitation wave and susceptibility to reentrant atrial arrhythmias in normalconcious dogs.Circ Res1988;62:395–410.20. Wang Z, Page P, Nattel S. Mechanism of flecainide’s antiarrhythmic actionin experimental atrial fibrillation.Circ Res1992;71:271–287.21. Wang J, Bourne GW, Wang Z, Villemaire C, Talajic M, Nattel S. Compar-ative mechanisms of antiarrhythmic drug action in experimental atrial fibrillation.Importance of use-dependent effects on refractoriness.Circulation 1993;88:1030–1044.22. Juul-Moeller S, Edvardsson N, Rehnquist-Ahlberg N. Sotalol versus quini-dine for the maintenance of sinus rhythm after direct current conversion of atrialfibrillation. Circulation 1990;82:1932–1939.23. Reimold SC, Cantillon CO, Friedman PL, Antman EM. Propafenone versus
sotalol for suppression of recurrent symptomatic atrial fibrillation.Am J Cardiol1993;71:558–563.24. Hohnloser SH, Woosley RL. Sotalol.N Engl J Med1994;331:31–38.25. Naccarelli GV, Lee KS, Gibson JK, VanderLugt J. Electrophysiology andpharmacology of ibutilide.Am J Cardiol1996;78(suppl 8A):12A–16A.26. Wijffels MCEF, Kirchhof CJHJ, Dorland R, Allessie MA. Atrial fibrillationbegets atrial fibrillation. A study in awake chronically instrumented goats.Cir-culation 1995;92:1954–1968.27. Sanfilippo AJ, Abascal VM, Sheehan M, Oertel LB, Harrigan P, Hughes RA,Weyman AE. Atrial enlargement as a consequence of atrial fibrillation.Circula-tion 1990;82:792–797.28. Gullestad L, Birkeland K, Molstad P, Moen Hoyer M, Vanberg P, KjekshusJ. The effect of magnesium versus verapamil on supraventricular arrhythmias.Clin Cardiol 1993;16:429–434.29. Rautaharju PM, Zhou SH, Wong S, Calhoun HP, Berenson GS, Prineas R,Davignon A. Sex differences in the evolution of the electrocardiographic QTinterval with age.Can J Cardiol1992;8:690–695.
1454 THE AMERICAN JOURNAL OF CARDIOLOGYT VOL. 81 JUNE 15, 1998