Embed Size (px)
Citation preview
70 Practical PAIN MANAGEMENT, July/August 2007
Prolotherapy is a method of injectiontreatment designed to stimulatehealing.1 Many musculoskeletal in-
juries and pain syndromes lend them-selves to prolotherapy treatment includ-ing low back and neck pain, chronicsprains and/or strains, whiplash injuries,
tennis and golfer’s elbow, knee, ankle,shoulder or other joint pain, chronic ten-donitis/ tendonosis, and musculoskeletalpain related to osteoarthritis. Prolothera-py works by raising growth factor levels oreffectiveness to promote tissue repair orgrowth.2 It can be used years after the ini-
tial pain or problem began, as long as thepatient is healthy.
This month’s article focuses on the useof prolotherapy for knee pain and in-juries, including ligament and meniscalinjuries, tendonitis and tendonosis,patellofemoral syndrome, and os-teoarthritis pain including degenerativejoint disease.
Prolotherapy Mechanism of Action Review Prolotherapy works by causing a tempo-rary, low grade inflammation at the site ofligament or tendon weakness (fibro-os-seous junction), “tricking” the body intoinitialing a new healing cascade. Inflam-mation activates fibroblasts to the area,which synthesize precursors to mature col-lagen, reinforcing connective tissue.2 Thisinflammatory stimulus raises the level ofgrowth factors to resume or initiate a newconnective tissue repair sequence to com-plete one which had prematurely abortedor never started.2 Prolotherapy is alsoknown as “regenerative injection therapy(RIT),” “non-surgical tendon, ligament,and joint reconstruction” or “growth fac-tor stimulation injection therapy.”
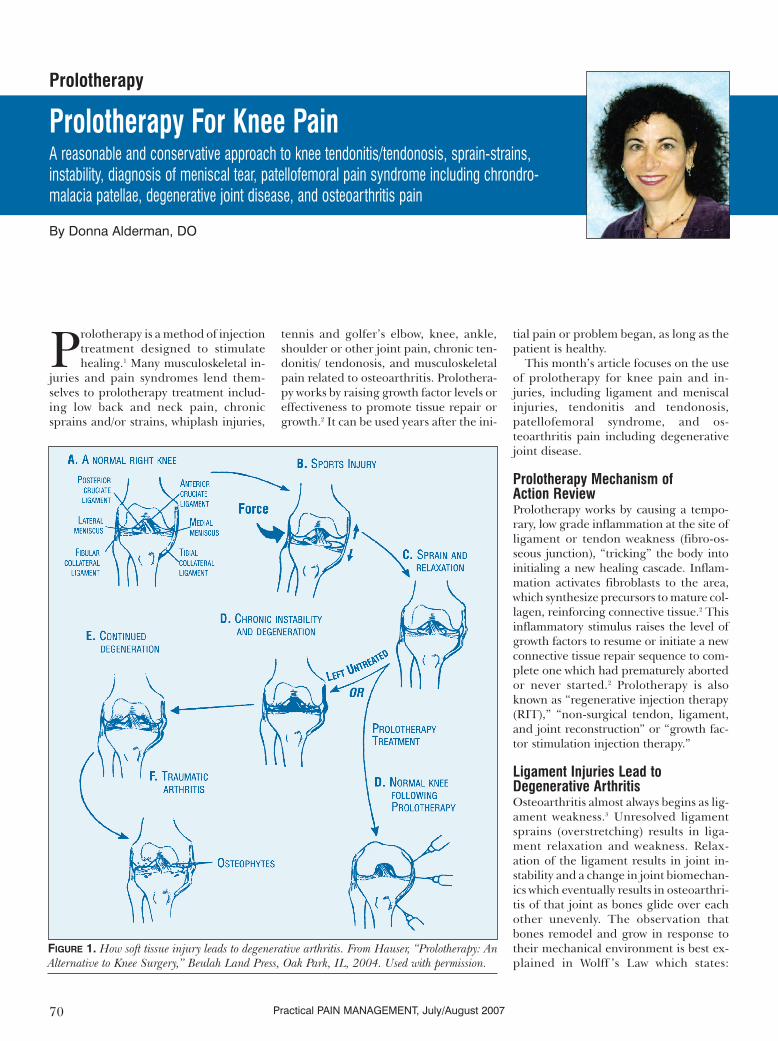
Ligament Injuries Lead to Degenerative ArthritisOsteoarthritis almost always begins as lig-ament weakness.3 Unresolved ligamentsprains (overstretching) results in liga-ment relaxation and weakness. Relax-ation of the ligament results in joint in-stability and a change in joint biomechan-ics which eventually results in osteoarthri-tis of that joint as bones glide over eachother unevenly. The observation thatbones remodel and grow in response totheir mechanical environment is best ex-plained in Wolff ’s Law which states:
Prolotherapy
By Donna Alderman, DO
Prolotherapy For Knee PainA reasonable and conservative approach to knee tendonitis/tendonosis, sprain-strains,instability, diagnosis of meniscal tear, patellofemoral pain syndrome including chrondro-malacia patellae, degenerative joint disease, and osteoarthritis pain
FIGURE 1. How soft tissue injury leads to degenerative arthritis. From Hauser, “Prolotherapy: AnAlternative to Knee Surgery,” Beulah Land Press, Oak Park, IL, 2004. Used with permission.
“Bones respond to stress by making newbone.”4 Tendon injuries, if unresolved,over a long period of time also have aninfluence on joint biomechanics and cancontribute to the development of os-teoarthritis.
This has been well demonstrated in themedical literature. One study of femalesoccer players who had sustained knee lig-ament injuries showed a very high per-centage with knee osteoarthritis 12 yearslater.5 Another study, published in SportsMedicine, observed the increased inci-dence of osteoarthritis with individualswho engaged in certain sports. These in-cluded wrestlers, boxers, baseball pitch-ers, football players, ballet dancers, soc-cer players, weightlifters, cricket players,and gymnasts.6 Postgraduate Medicine re-ports in its investigation of the causes ofhuman arthritis:
“There is no question that trauma andmechanical stress on the joint lead to thedevelopment of osteoarthritis.”7
Even in veterinary medicine, it is well-established that ligament sprains favor thedevelopment of osteoarthritis in animals.8
If ligament and tendon injuries arestimulated to heal, biomechanics can berestored and the downward progression ofdegenerative changes can be prevented orstopped. Prolotherapy can, therefore, beseen as a method to prevent or stop thearthritic process because it strengthensthe joint and thus ends the need for theknee or other treated joint, to grow boneor form bone spurs9 (see Figure 1).
Prolotherapy for Patients with Degenerative ArthritisProlotherapy has been used successfullyeven after the diagnosis of osteoarthritisand degenerative joint disease. This maybe because of its ability to strengthen theexisting intact, but weakened, ligamen-tous and tendinous structures. There isalso some clinical evidence that prolother-apy may help to regenerate cartilage.Reeves and Hassanein in Kansas City in-vestigated prolotherapy in degenerativeosteoarthritis with and without ACL laxi-ty. In their double blind, placebo-con-trolled study, enrolled patients had eithergrade 2, or more, joint narrowing orgrade 2, or more, osteophytic change. Inaddition to subjective indexes such as vi-sual analogue scale for pain, swelling, andfrequency of leg buckling, objective go-niometric flexion measurements as well asradiographic measures of joint narrowing
and osteophytosis were taken before andafter prolotherapy. Arthrometric meas-urements of ACL laxity were also done.The study concluded that prolotherapytreatment resulted in clinically and statis-tically significant improvements in kneeosteoarthritis. Preliminary blinded radi-ographic readings (1-year) demonstratedimprovement in several measures of os-teoarthritic severity. ACL laxity, whenpresent, also improved.10
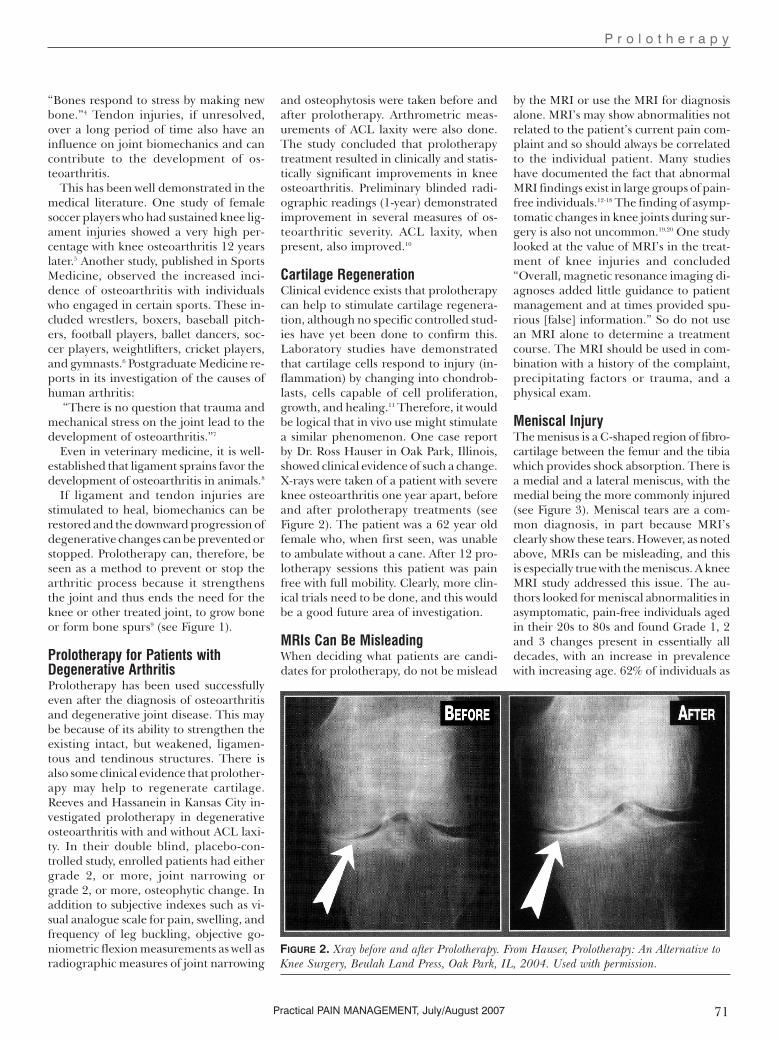
Cartilage RegenerationClinical evidence exists that prolotherapycan help to stimulate cartilage regenera-tion, although no specific controlled stud-ies have yet been done to confirm this.Laboratory studies have demonstratedthat cartilage cells respond to injury (in-flammation) by changing into chondrob-lasts, cells capable of cell proliferation,growth, and healing.11 Therefore, it wouldbe logical that in vivo use might stimulatea similar phenomenon. One case reportby Dr. Ross Hauser in Oak Park, Illinois,showed clinical evidence of such a change.X-rays were taken of a patient with severeknee osteoarthritis one year apart, beforeand after prolotherapy treatments (seeFigure 2). The patient was a 62 year oldfemale who, when first seen, was unableto ambulate without a cane. After 12 pro-lotherapy sessions this patient was painfree with full mobility. Clearly, more clin-ical trials need to be done, and this wouldbe a good future area of investigation.
MRIs Can Be MisleadingWhen deciding what patients are candi-dates for prolotherapy, do not be mislead
by the MRI or use the MRI for diagnosisalone. MRI’s may show abnormalities notrelated to the patient’s current pain com-plaint and so should always be correlatedto the individual patient. Many studieshave documented the fact that abnormalMRI findings exist in large groups of pain-free individuals.12-18 The finding of asymp-tomatic changes in knee joints during sur-gery is also not uncommon.19,20 One studylooked at the value of MRI’s in the treat-ment of knee injuries and concluded“Overall, magnetic resonance imaging di-agnoses added little guidance to patientmanagement and at times provided spu-rious [false] information.” So do not usean MRI alone to determine a treatmentcourse. The MRI should be used in com-bination with a history of the complaint,precipitating factors or trauma, and aphysical exam.
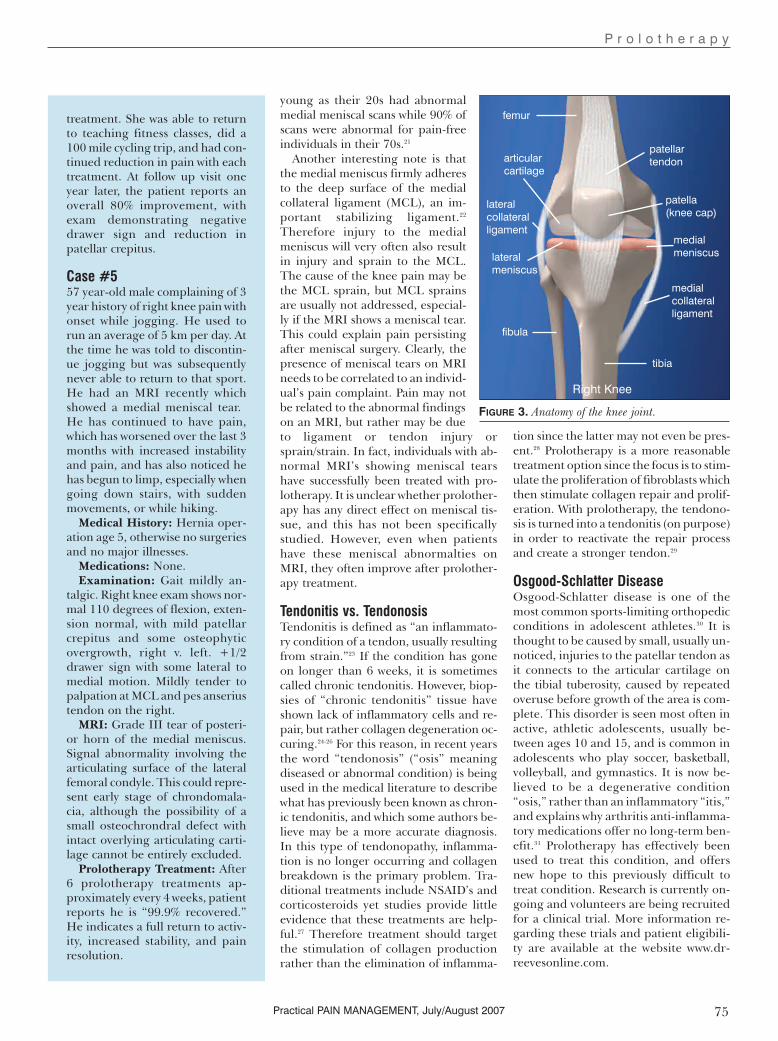
Meniscal InjuryThe menisus is a C-shaped region of fibro-cartilage between the femur and the tibiawhich provides shock absorption. There isa medial and a lateral meniscus, with themedial being the more commonly injured(see Figure 3). Meniscal tears are a com-mon diagnosis, in part because MRI’sclearly show these tears. However, as notedabove, MRIs can be misleading, and thisis especially true with the meniscus. A kneeMRI study addressed this issue. The au-thors looked for meniscal abnormalities inasymptomatic, pain-free individuals agedin their 20s to 80s and found Grade 1, 2and 3 changes present in essentially alldecades, with an increase in prevalencewith increasing age. 62% of individuals as
P r o l o t h e r a p y
71Practical PAIN MANAGEMENT, July/August 2007
FIGURE 2. Xray before and after Prolotherapy. From Hauser, Prolotherapy: An Alternative toKnee Surgery, Beulah Land Press, Oak Park, IL, 2004. Used with permission.
P r o l o t h e r a p y
74 Practical PAIN MANAGEMENT, July/August 2007
Case Reports
Case #151 year-old cameraman complaining of left knee pain for 6months which began after a two foot fall from an unstableriser at work. Two weeks after this injury, the patient was run-ning, as was his routine, and began to notice discomfort inhis left knee. Discontinuing running helped but, while at hisdaughter’s soccer game, he ran after a ball and a week laterbegan to have the same pain recur in his knee and has per-sisted. He feels the pain in the medial aspect of his kneewhen going up and down stairs, worse going up, and alsowhen walking. NSAIDs have not helped. He has been toldhe has a torn meniscus and arthritis causing his pain.
Medical History: No major surgeries or medical issues.Review of Systems: No complaints other than seasonal al-
lergies.Medications: ClaritinPhysical Exam: Left knee slightly swollen as compared to
left, but without erythema or deformity. Flexion to 110 de-grees, with restricted extension secondary to apparent Bak-ers cyst. Mild crepitus present. +1/2 drawer sign with later-al to medial motion present. Negative McMurray’s. Tender-ness present at the medial collateral ligament and pesanserius tendons.
MRI: 1. Mild tricompartmental osteoarthritis with carti-lage loss most severe in the lateral facet and trochlea; 2. Com-plex grade III signal in the posterior horn of the medialmeniscus and body compatible with tearing; 3. Mild anteri-or cruciate ligament sprain as well as a grade I medial col-lateral ligament sprain. Meniscocapsular separation cannotbe excluded as the edema is most intense adjacent to themeniscus; 4. Small joint effusion and small lobulatedpopliteal cyst.
Prolotherapy Treatment: After 5 prolotherapy treatmentsone month apart, the patient reported 90% improvement.At the patient’s followup visit and treatment 3 months later,he reported continued improvement, now 95%, and reportsno pain with return to regular exercise. At one year followup, the patient reports continued stability and activity.
Case #263 year-old male, public relations executive, with 20 year his-tory of left knee pain on and off, status post 2 knee athro-scopic surgeries which gave him only short-term relief. Overthe past few years, he states the pain has worsened and re-cently exacerbated with a lifting injury. He has taken NSAIDssuch as Bextra which temporarily help, and followed theRICE protocol (rest, ice, compression, elevation), but thepain has continued. He has stiffness and difficulty gettingup from seated to standing position, and trouble going downstairs. He has been told he has cartilage degeneration andneeds a knee replacement.
Medical History and Review of Symptoms: Tonsils outas a child and measles at age 30. No health issues except el-evated blood pressure, on medication.
Medications: Aspirin, Cozaar, Effexor, Bextra prn.Examination: Valgus deformity, left greater than right.
Flexion is restricted at 90 degrees of flexion with restrictedextension of 10 degrees from flat. There is mild swelling butno erythema. Tenderness to palpation at the medial collat-eral ligament and pes anserious tendon. +1/2 drawer signand negative McMurray.
Prolotherapy Treatment: After 10 prolotherapy treat-ments one month apart, the patient felt he was 85% im-proved and was no longer considering a knee replacement.He reported far less pain under load and resting, better flex-ibility, walking down stairs easily, and no stiffness when get-ting up from sitting or after driving. At 2-1/2 year follow-up, he had continued stability with range of motion onlymildly restricted in extension and with full range of motionin flexion.
Case #314 year-old male with anterior knee pain for one year afterbeing active in several sports for many years, including bas-ketball, football, soccer and baseball. No prior known trau-ma. He states he was diagnosed with Osgood-Schlatter dis-ease and was told there was nothing he could do about it.The patient wakes up in the morning with the pain and itlasts throughout the day and has prevented him from par-ticipating in his usual sports. Subsequently, he dropped outof all his athletic activities and is not currently active in anysport yet still experiences daily pain.
Medical History and Review of Systems: NegativeMedications: NoneExamination: Enlargement of the tibial tuberosity with
tenderness to palpation at the patellar tendon insertion onthe tuberosity bilaterally. Rest of exam within normal limits.
Prolotherapy Treatment: After one treatment to the rightknee and three treatments to the left knee at 3 to 4 week in-tervals, patient states he is 95-100% better in both knees, andback to full sports activity. He reports he can now “do any-thing.” Followup at 1 and 2 years showed stable improve-ment with continued full return to all sports.
Case #432 year-old female, former Olympic Taekwondo competitor,with history of right knee pain for three years, status postACL reconstruction (patella technique) with partial medialmenisectomy. The patient’s pain returned 1 year later andshe underwent arthroscopic debriding which confirmeddamage to her articular cartilage. This provided only tem-porary relief. She has done rehab exercise on her own butdespite this, over the last year, medial knee pain has returnedand is now persistent and fairly constant. The pain is aggra-vated by walking and activity.
Medical History and Review of Systems: Healthy, nohealth issues or complaints.
Medications: NoneExam: Right knee: patellar tracking deficit and crepitus.
+2 drawer sign. Range of motion within normal limits. Neg-ative McMurray. Tender to palpation at MCL, patellar ten-don and pes anserious tendon insertion.
Prolotherapy Treatment: The patient was given six treat-ments on her right knee, approximately every 4 weeks. Shefelt immediate reduction in her pain starting with the first
P r o l o t h e r a p y
75Practical PAIN MANAGEMENT, July/August 2007
young as their 20s had abnormalmedial meniscal scans while 90% ofscans were abnormal for pain-freeindividuals in their 70s.21
Another interesting note is thatthe medial meniscus firmly adheresto the deep surface of the medialcollateral ligament (MCL), an im-portant stabilizing ligament.22
Therefore injury to the medialmeniscus will very often also resultin injury and sprain to the MCL.The cause of the knee pain may bethe MCL sprain, but MCL sprainsare usually not addressed, especial-ly if the MRI shows a meniscal tear.This could explain pain persistingafter meniscal surgery. Clearly, thepresence of meniscal tears on MRIneeds to be correlated to an individ-ual’s pain complaint. Pain may notbe related to the abnormal findingson an MRI, but rather may be dueto ligament or tendon injury orsprain/strain. In fact, individuals with ab-normal MRI’s showing meniscal tearshave successfully been treated with pro-lotherapy. It is unclear whether prolother-apy has any direct effect on meniscal tis-sue, and this has not been specificallystudied. However, even when patientshave these meniscal abnormalties onMRI, they often improve after prolother-apy treatment.
Tendonitis vs. TendonosisTendonitis is defined as “an inflammato-ry condition of a tendon, usually resultingfrom strain.”23 If the condition has goneon longer than 6 weeks, it is sometimescalled chronic tendonitis. However, biop-sies of “chronic tendonitis” tissue haveshown lack of inflammatory cells and re-pair, but rather collagen degeneration oc-curing.24-26 For this reason, in recent yearsthe word “tendonosis” (“osis” meaningdiseased or abnormal condition) is beingused in the medical literature to describewhat has previously been known as chron-ic tendonitis, and which some authors be-lieve may be a more accurate diagnosis.In this type of tendonopathy, inflamma-tion is no longer occurring and collagenbreakdown is the primary problem. Tra-ditional treatments include NSAID’s andcorticosteroids yet studies provide littleevidence that these treatments are help-ful.27 Therefore treatment should targetthe stimulation of collagen productionrather than the elimination of inflamma-
tion since the latter may not even be pres-ent.28 Prolotherapy is a more reasonabletreatment option since the focus is to stim-ulate the proliferation of fibroblasts whichthen stimulate collagen repair and prolif-eration. With prolotherapy, the tendono-sis is turned into a tendonitis (on purpose)in order to reactivate the repair processand create a stronger tendon.29
Osgood-Schlatter DiseaseOsgood-Schlatter disease is one of themost common sports-limiting orthopedicconditions in adolescent athletes.30 It isthought to be caused by small, usually un-noticed, injuries to the patellar tendon asit connects to the articular cartilage onthe tibial tuberosity, caused by repeatedoveruse before growth of the area is com-plete. This disorder is seen most often inactive, athletic adolescents, usually be-tween ages 10 and 15, and is common inadolescents who play soccer, basketball,volleyball, and gymnastics. It is now be-lieved to be a degenerative condition“osis,” rather than an inflammatory “itis,”and explains why arthritis anti-inflamma-tory medications offer no long-term ben-efit.31 Prolotherapy has effectively beenused to treat this condition, and offersnew hope to this previously difficult totreat condition. Research is currently on-going and volunteers are being recruitedfor a clinical trial. More information re-garding these trials and patient eligibili-ty are available at the website www.dr-reevesonline.com.
treatment. She was able to returnto teaching fitness classes, did a100 mile cycling trip, and had con-tinued reduction in pain with eachtreatment. At follow up visit oneyear later, the patient reports anoverall 80% improvement, withexam demonstrating negativedrawer sign and reduction inpatellar crepitus.
Case #557 year-old male complaining of 3year history of right knee pain withonset while jogging. He used torun an average of 5 km per day. Atthe time he was told to discontin-ue jogging but was subsequentlynever able to return to that sport.He had an MRI recently whichshowed a medial meniscal tear.He has continued to have pain,which has worsened over the last 3months with increased instabilityand pain, and has also noticed hehas begun to limp, especially whengoing down stairs, with suddenmovements, or while hiking.
Medical History: Hernia oper-ation age 5, otherwise no surgeriesand no major illnesses.
Medications: None.Examination: Gait mildly an-
talgic. Right knee exam shows nor-mal 110 degrees of flexion, exten-sion normal, with mild patellarcrepitus and some osteophyticovergrowth, right v. left. +1/2drawer sign with some lateral tomedial motion. Mildly tender topalpation at MCL and pes anseriustendon on the right.
MRI: Grade III tear of posteri-or horn of the medial meniscus.Signal abnormality involving thearticulating surface of the lateralfemoral condyle. This could repre-sent early stage of chrondomala-cia, although the possibility of asmall osteochrondral defect withintact overlying articulating carti-lage cannot be entirely excluded.
Prolotherapy Treatment: After6 prolotherapy treatments ap-proximately every 4 weeks, patientreports he is “99.9% recovered.”He indicates a full return to activ-ity, increased stability, and painresolution.
FIGURE 3. Anatomy of the knee joint.
patellartendonarticular
cartilage
medialmeniscuslateral
meniscus
lateralcollateralligament
medialcollateralligament
Right Knee
femur
fibula
tibia
patella(knee cap)

P r o l o t h e r a p y
76 Practical PAIN MANAGEMENT, July/August 2007
Anterior Cruciate Ligament Injury The Anterior Cruciate Ligament (ACL) isan important ligament for anterior-pos-terior stability of the knee. An estimated200,000 ACL-related injuries occur annu-ally in the United States,32 with the high-est incidence in those who participate inpivoting sports such as soccer, volleyball,and basketball. Thirty percent of these in-juries are a result of direct contact with anobject or another player, while 70% do notinvolve direct contact and the basic injurymechanism may be elusive.33 Risk factors
include activities involving deceleration,pivoting, awkward landings, shoe-surfaceinteractions, and other mechanical envi-ronmental factors.34 While ACL injuriesare a very common knee injury, they oftendo not heal well. This is because the bloodsupply is from within the ligament itself,not from around it, and when the liga-ment is torn the blood supply is common-ly disrupted during the injury.35 If the ACLis completely ruptured, surgery is need-ed. However, for partial ACL injury, pro-lotherapy is a reasonable treatment op-tion and should be considered prior tosurgery. As discussed above, Reeves et al.demonstrated the effectiveness of pro-lotherapy for ACL laxity.36 MRI studieshave not been shown to be as accurate asone might think in the differentiation ofcomplete and partial ACL tears,37 there-fore correlation between history, physicalexam, and MRI is important in determin-ing who is a candidate for prolotherapy.
Medial Collateral SprainThe medal collateral ligament (MCL)(also called tibial collateral ligament) is animportant stabilizing ligament of theknee. The MCL sprain is a common in-jury, especially in sports but this injury canalso occur in the non-athlete. The classi-cal mechanism of a medial collateral lig-ament is a force hitting the lateral aspectof a partly flexed and externally rotatedknee38—such as would occur with a socceror football player who receives a kick orblow at the outer side of a weight-bearing
knee.39 The patient experiences a crackand feels a sudden pain at the inner as-pect of the knee. Most of the pain disap-pears relatively quickly and, at first, theknee is not swollen. However, increasingpain and swelling starts after a few hours.By the next day, the patient can hardlystand. This improves over a period of timeand, after 2 to 3 months, should be com-pletely resolved. If any residual pain ex-ists, the ligament has likely been perma-nently lengthened, resulting in an unsta-ble knee.40 As discussed above, leaving an
unstable ligament will result in a changein biomechanics and development of os-teoarthritis. Prolotherapy can be used inthis situation to repair the overstretchedligament and stimulate healing so thatstability is restored.
Coronary Ligament SprainThese small, but very important, liga-ments hold the outside edge of the menis-cus to the tibial plateau. They are verycommonly injured but mostly go undiag-nosed because the localization of the painand nature of the onset resemble a menis-cus lesion or a sprain of the medial collat-eral ligament.41 These injuries can be ef-fectively treated with prolotherapy.
Pes Anserinus TendonitisThe pes anserinus group of tendons at-tach at the medial knee and are a verycommon area of injury and source of painin all age groups. The pes anserinus is thecombined tendon insertions of three mus-cles (sartorius, gracilis, and semitendi-nous) at the anteromedial aspect of theproximal tibia. This tendonitis is some-times misdiagnosed as pes anserinus bur-sitis, however bursitis in this location israre.42 Pes anserinus tendonitis is verycommon in older individuals, and may re-main after knee replacement surgery. Pesanserinus tendonitis is easily treated withprolotherapy.
Patellar TendonopathyTenonditis around the patella is a typical
overuse injury in sports such as volleyball,basketball, cycling, and high-jump.43
Three possible sites exist: the upper bor-der (suprapatellar), the apex, which is theclassical “jumper’s knee” (infrapatellar),and at either side of the patella (tendonitisof the quadriceps expansion).44 Patienthistory typically includes localized pain atthe front of the knee during or after ex-ertion. In severe cases, there is pain at restwith less severe cases exhibiting onlyminor pain after exercise. The patient alsostates that walking upstairs or getting upfrom a chair is painful.45 Physical exam isusually normal. MRI diagnosis is not veryhelpful in this diagnosis and adds littleguidance to patient management.46,47
Patellar tendonitis can progress to ten-donosis and make its management morerecalcitrant. Again, prolotherapy can beeffective in treating this tendonitis/ten-donosis.
Patellofemoral Pain Syndrome (Pfps)Patellofemoral pain is the most commoncause of anterior knee pain,48 usually pre-senting with vague symptoms of pain“in,” “under,” or “behind” the patella orin the peri-patellar area. Symptoms areexacerbated by activities such as running,descending stairs, and squatting, as wellas prolonged sitting with the knee in aflexed position (“theatre sign”). Twenty-five percent of the population, at somestage in their lives, suffer from this con-dition.49 Despite this, there is little agree-ment on the terminology, etiology, ortreatment. The term “chrondromalaciapatellae” is sometimes used, but is nowreserved for a small subset of anteriorknee pain with documented softening ofthe patellar articular cartilage.50 There islittle evidence to support the use of kneebraces or NSAIDs51 in PFPS. This condi-tion has been successfully treated withprolotherapy.
Typical Treatment CourseThe average number of prolotherapytreatments needed is 4 to 6, with some pa-tients needing more and some patientsless. Individuals with more severe degen-erative changes may require more treat-ments while teenagers often require less.Patients who have been on anti-inflamma-tories prior to starting treatment may re-quire additional treatments before im-provement is noted. If no improvementwhatsoever is noted by the patient after 3to 4 treatments, there should be a re-eval-
“If the ACL is completely ruptured, surgery is needed. Howev-
er, for partial ACL injury, prolotherapy is a reasonable treatment
option and should be considered prior to surgery.”

uation for any interfering factors such aspoor sleep, diet, continued aggravatingactivities, illness, or use of medicationsthat may prevent healing. If indicated, thepatient should be considered for referralfor complimentary modalities, radiologi-cal studies, or surgical consult.
ContraindicationsActive infection, cancer, non-reduced dis-locations, or known allergy to any pro-lotherapy ingredients are contraindica-tions to treatment, as is any known under-lying illness which would interfere withhealing. Acute gout or rheumatoid arthri-tis in the knee joint are also contraindica-tions. Relative contraindications includecurrent and long term use of high dosesof narcotics as these medications canlower the immune response. Current useof systemic corticosteroids or NSAIDS arealso relative contraindications as these arecounter-productive to the inflammatoryhealing process.
ConclusionProlotherapy is a reasonable and conser-vative approach to knee tendonitis/ten-donosis, knee sprain-strains, knee insta-bility, diagnosis of meniscal tear,patellofemoral pain syndrome includingchrondromalacia patellae, as well as de-generative joint disease and osteoarthri-tis pain. Since prolotherapy is a treatmentmodality that provides a long term solu-tion rather than just palliation, it shouldbe considered in appropriate patientsprior to long term narcotic therapy or sur-gical intervention. n
Donna Alderman, DO is a graduate of West-ern University of Health Sciences, College ofOsteopathic Medicine of the Pacific, inPomona, California, with undergraduate de-gree from Cornell University in Ithaca, NY. Shehas extensive training in Prolotherapy and hasbeen using Prolotherapy in her practice for tenyears. Dr. Alderman is the Medical Director ofHemwall Family Medical Centers in Califor-nia and can be reached through her websitewww.prolotherapy.com.
References1. Hackett GS, Hemwall GA, and Montgomery GA.Ligament and Tendon Relaxation Treated by Prolother-apy. Fifth Edition. (1956 First Edition Charles C.Thomas, Publisher). Gustav A. Hemwall, Publisher.Institute in Basic Life Principles. Oak Brook, IL. 1991.2. Reeves KD. Prolotherapy: Basic Science, ClinicalStudies, and Technique. In Lennard TA (Ed) Pain Pro-cedures in Clinical Practice 2nd Ed. Hanley and Bel-fus. Philadelphia. 2000. 172-190.
3. Hauser R. Prolotherapy: An Alternative to KneeSurgery. Beulah Land Press. Oak Park, IL. 2004. p 83.4. Cervoni TD et al. Recognizing upper-extremitystress lesions. The Physician and Sportsmedicine.August 1997. (25):8.5. Lohmander LS, Ostenberg A, Englund M, and RoosH. High prevalence of knee osteoarthritis, pain andfunctional limitations in female soccer players twelveyears after anterior cruciate ligament injury. Arthritis &Rheumatism. October 2004. 50(10):3142-3152.6. Panush R. Recreational activities and degenerativejoint disease. Sports Medicine. January 1994. 17:1-5.7. Morehead K and Sack K. Osteoarthritis: What ther-apies for this disease of many causes? PostgraduateMedicine. November 2003. pp 12-17.8. Farrow CS and Newton CD. “Ligamentous Injury(Sprain)” in Textbook of Small Animal Orthopaedics.International Veterinary Information Service. Ithaca,NY. 1985. 9. Hauser R. Prolotherapy: An Alternative to KneeSurgery. Beulah Land Press. Oak Park, IL. 2004. p 62.10. Reeves KD and Hassanein K. Randomizedprospective double-blind placebo-controlled study ofdextrose prolotherapy for knee osteoarthritis with orwithout ACL laxity. Alternative Therapies. March 2000.6(2):68-80.11. Mankin H. The response of articular cartilage tomechanical injury. Journal of Bone and Joint Surgery.1982. 64A:460.12. Ombregt L, Bisschop P, and ter Veer HJ. A Sys-tem of Orthopaedic Medicine, 2nd Edition. ChurchillLivingstone. 2003. p 59.13. MacRae DL. Asymptomatic intervertebral discprotrusion. Acta Radiologica. 1956. pp 46-49.14. Hitselberger WE and Whitten RM. Abnormal myel-ograms in asymptomatic patients. Journal of Neuro-surgery. 1968. 28:204.15. Wiesel SW et al. A study of computer-assisted to-mography: 1. The incidence of positive CAT scans inan asymptomatic group of patients. Spine. 1984. 9:549-551.16. Powell MC et al. Prevalence of lumbar disc de-generation observed by magnetic resonance insymptomless woman. Lancet. 1986; 13:1366-1367.17. Boden SD et al. Abnormal magnetic resonancescans of the lumbar spine in asymptomatic subjects.Journal of Bone and Joint Surgery 1990. 72A:503-408.18. Kaplan PA. MR imaging of the normal shoulder:variants and pitfalls. Radiology. 1992. 184:519-524.19. Jerosch J, Castro WH, and Assheuer J. Age relat-ed magnetic resonance imagaing morphology of themenisci in asymptomatic individuals. Archives of Or-thopedic Trauma Surgery. 1996. 115(3-4); 199-202.20. LaPrade RF et al. The prevalence of abnormalmagnetic resonance imaging findings in asympto-matic knees. With correlation of magnetic resonanceimaging to arthroscopic findings in symptomaticknees. American Journal of Sports Medicine. 1994.22(6):739-745.21. Kormick J, Trefelner E, McCarthy S et al. Meniscalabnormalities in the asymptomatic population at MRImaging. Radiology. 1990. 177:463-465.22. Moore K and Dalley A. Clinically Oriented Anatomy,Fifth Edition. Lippincott Williams & Wilkins. 2006. p 688.23. Mosby’s Medical Dictionary, Elsevier Saunders. 2006.24. Astrom M and Rausing A. Chronic Achillestendinopathy: a survey of surgical and histopatholog-ic findings. Clin Orthop. July 1995. 316:151-164.25. Khan KM, Bonar F, Desmond PM et al. Patellartendinosis (jumper’s knee); findings at histopatholog-ic examination, US and MR imaging. Victorian Insti-tute of Sport Tendon Study Group. Radiology. 1996.200(3):821-827.26. Khan KM, Cook JL, Bonar F et al. Histopathologyof common teninopathies: update and implicationsfor clinical managements. Sports Medicine. 1999.27(6):393-408.
27. Almekinders LC and Temple JD. Etiology, diagnosisand treatment of tendonosis: an analysis of the literature.Medicine & Science in Sports and Exercise. 1998. 30(8).28. Khan KM, Cook JL, Taunton JE, and Bonar F.Overuse Tendonosis, Not Tendonitis. The Physicianand Sportsmedicine. May 2000. 28(5).29. Hauser R. Prolotherapy: An Alternative to KneeSurgery. Beulah Land Press. Oak Park, IL. 2004. p 92.30. Ross MD, Villard D. Disability of college-agedmen with a history of Osgood-Schlatter disease. J.Strength Cond. Res. 2003. 17(4):659-663, cited inReeves KD et al. Study seeks treatment to keep ath-letes in the game. Biomechanics. April 15, 2006.31. Kader D, Saxena A, Movin T et al. Achillestendinopathy: some aspects of basic science andclinical management. British Journal of Sports Medi-cine. 2002. 36(4):239-249, cited in Reeves, KD et al.Study seeks treatment to keep athletes in the game,Biomechanics. April 15, 2006.32. www.emedicine.com/sports/TOPIC9.HTM. Lastvisited 7/9/07.33. Griffin LY, Agel J, Albohm MJ et al. NoncontactAnterior Cruciate Ligament Injuries: Risk Factors andPrevention Strategies. Journal of the American Acad-emy of Orthopeaedic Surgeons. May/June 2000.8(3):141-150.34. Ibid. 35. Rowley D. The Musculoskeletal System. Chap-man & Hall Medical. 1997. New York, NY. p 73, citedin Hauser R. Prolo Your Sports Injuries Away. BeulahLand Press, Oak Park, IL. 2001. p 281.36. Reeves KD and Hassanein K. Randomizedprospective double-blind placebo-controlled study ofdextrose prolotherapy for knee osteoarthritis with orwithout ACL laxity. Alternative Therapies. March 2000.6(2):68-80.37. Stoller D. Magnetic Resonance Imaging in Or-thopaedics and Sports Medicine. Second Edition.Philadelphia, PA. Lippincott-Raven. 1997. p 330.38. Hull ML, Berns GS, Verma H, and Patterson HA.Strain in the medial collateral ligament of the humanknee under single and combined loads. J Biome-chanics. 1996. 26(2):199-206.39. Reider B. Medial collateral ligament injuries in ath-letes. Sports Medicine. 1996. 21(2):147-156.40. Ibid ref 12: Ombregt L, Bisschop P, and ter VeerHJ. p 1103.41. Ibid ref 12: Ombregt L, Bisschop P, and ter VeerHJ. p 1108.42. Hauser R. Prolotherapy: An Alternative to KneeSurgery. Beulah Land Press. Oak Park, IL. 2004. p 103.43. Ibid ref 12: Ombregt L, Bisschop P, and ter VeerHJ. p 1132.44. Cyriax JH. Textbook of Orthopaedic Medicine,Volume 1. Diagnosis of Soft Tissue Lesions, 8th edn.Balliere Tindall, London. 1982.45. Ibid ref 12: Ombregt L, Bisschop P, and ter VeerHJ. p 1132.46. Shalaby M and Almekinders LC. Patellar ten-donitis: the significance of magnetic resonance imag-ing findings. American Journal of Sports Medicine.1999. 27(3):345-349. 47. Stanitski CL. Correlation of Arthroscopic and Clin-ical Examinations With Magnetic Resonance ImagingFindings of Injured Knees in Children and Adoles-cents. American J of Sports Medicine. 1998. 26:2-6.48. Burton M and Drezner J. Lower extremity overuseinjuries in women. Women’s Health in Primary Care.October 2006. p 15-32.49. Fulkerson J and Hungerford D. Disorders of thePatellofemoral Joint, 2nd ed. Williams & Wilkins. Balti-more. 1990.50. Dixit S, Burton M, and Mines B. Management ofPatellofemoral Pain Syndrome. American FamilyPhysician. January 2007. 75(2):194-202.51. Ibid.
P r o l o t h e r a p y
79Practical PAIN MANAGEMENT, July/August 2007





























