Embed Size (px)
Citation preview

Progressive Septal and Palatal Perforation Secondary to Intranascd Cocaine Abuse
B S Gendeh, MS (ORL-HNS),"B J Ferguson, MD, FACS,** J T Johnson, MD, FACS,** S Kapadia,*"* MD, FACPath, *Department of Otorhinolaryngology- Head and Neck Surgery, Faculty of Medicine, Hospital National University of Malaysia, Jalan Tenteram, Bandar Tun Razak, 56000 Kuala Lumpur, **Department of Otolaryngology, The Eye and Ear Institute, Suite 500, 200 Lothrop Street, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA,'H* Department of Pathology, Presbyterian Hospital, 200 Lothrop Street, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA
*The Author was a Fulbright Scholar to the University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA for 1997.
Cocaine (benzylmethylecyonine) is used in its pure form for "snorting" and the more volatile "free-base" form is used for smoking. Cocaine, a derivative of the leaves of Erythroxylon coca was long used by the Indian natives in Peru. However, it was not until 1855 that cocaine was isolated from the coca leaves. An estimated 30 million Americans have used cocaine and 6 million are compulsive users with a frequency of snorting amounting to once a month. Approximately, one in five American high school students have used cocaine before graduation. At one time, the cost of cocaine served as a barrier to its widespread use. However, with increasing availability and decreased cost, its use has escalated in
Med J Malaysia Vol 53 No 4 Dec 1998
the United States. The intranasal route, "snorting", is the most common route of administration. Users typically inhale the drug at 10 to 45 minutes intervals over a period lasting several days or longer. The cocaine is detoxified by the liver and plasma cholinesterase to water soluble metabolites which are excreted in the unne.
Septal perforation from intranasal cocaine abuse was first reported by Owens in 1912. Subsequently, several reports of septal perforations among heavy abusers appeared in the literature. Repeated episodes of vasoconstriction and subsequent ischaemia due to
frequent cocaine snorting may cause septal perforation. However, palatal destruction is rare with four reported cases in the literature 1.2.3,4 An estimated 4.5% of
435

CASE REPORT
addicts using intranasal cocaine suffer nasal and sinus complications. These range from nasal crusting, epistaxis and anaesthesia to large septal perforations.
A 44 year American female tobacco smoker had snuffed cocaine for several years. She reported snuffing cocaine since her college days and had stopped using cocaine approximately four months prior to presentation. She presented with a two year history of nasal blockage and a five month history of fluid regurgitating through the nostril. The patient was noted to have an obvious saddled nose deformity (Figure 1). Nasal endoscopic
fig, 1: lcder(!Ji view of Sl«:iddled fll)~e deformity
436
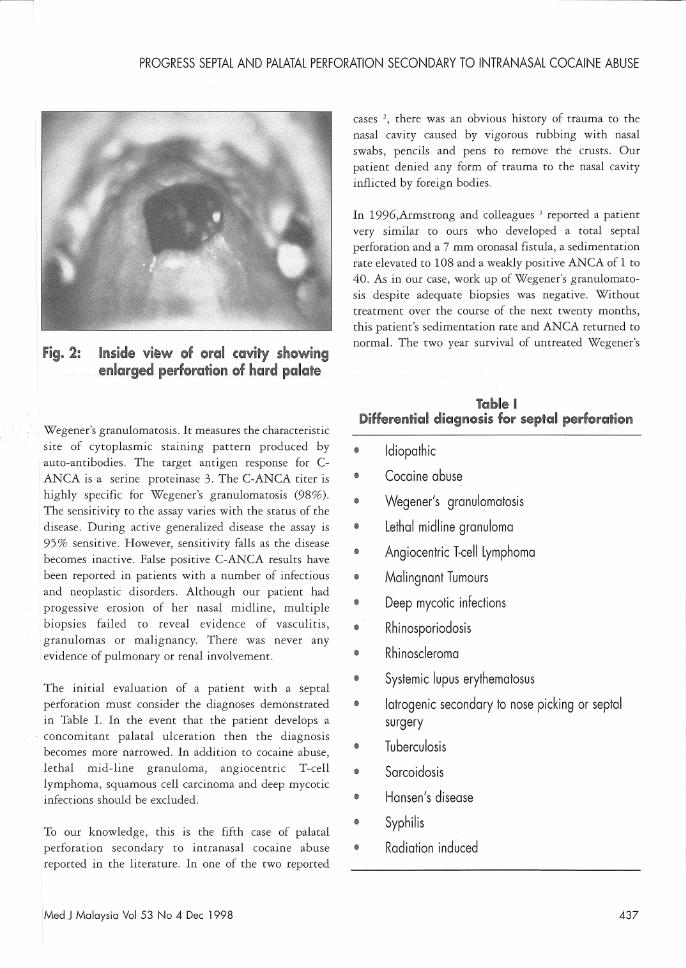
examination revealed a subtotal perforation involving the cartilaginous and bony septum with decreased sensation and extensive crusting. Examination of the oral cavity revealed a fistula in the hard palate which was in the midline and measuring 18mm in diameter. Biopsies from the edge of the septal perforation and palatal perforation showed only acute and chronic inflammation with necrosis but no evidence of vasculitis, granuloma or malignancy. Medical management of the patient's nasal problems consisted of oral Augmentin 500 mg tid, regular debridement of nasal crusts and daily douches of saline combined with gentamicin (80mg per 500ml of saline, lOcc each per day). Over the course of the next year, the perforation slowly enlarged (Figure 2). The patient claimed no further use of cocaine. Urine analysis for traces of cocaine was negative. Crusting of the nose became an increasing problem and cultures repeatedly grew coagulase positive staphylococcus.
The laboratory investigations performed then revealed a weakly positive C-ANCA(1: 40 titer), a normal anti-nuclear antibody (ANA- less than 1:40 titer), a normal rheumatoid factor (RF- less than 15 IU/ml), the sedimentation rate was 28mm per hour (Westergreen Method), platelets were elevated at (653,000/ en mm) and CBC revealed a WBC of 10.7 per cu mm, FTA absorption was non-reactive and HIV test was negative.
The pathophysiologic mechanism by which cocaine induces a delayed palatal perforation is unclear. The short term effect of cocaine is to block sodium channels and interfere with the generation of nerve impulses and thus produce anaesthesia. Vasoconstriction occurs because re-uptake of nor-epinephrine and epinephrine is inhibited. Direct contraction of vascular smooth muscle independent of sympathetic nerve activity has also been demonstrated. The profound vasoconstriction incurred with cocaine use leads to ischaemia, ulceration and perforation. In the interim, stasis of mucociliary clearance, crusting and bacterial colonization may occur which can result in atrophic changes in the mucosal lining. The falsely positive C-ANCA led to a dilemma in establishing the exact diagnosis in this patient. C-ANCA is the most important ancillary assay in
Med J Malaysia Vol 53 No 4 Dec 1998
PROGRESS SEPTAL AND PALATAL PERFORATION SECONDARY TO INTRANASAL COCAINE ABUSE
Fig. 2: Inside vi~w @f oral cavity showing enlarged pel'f@ra~ion of hard palate
Wegener's granulomatosis. It measures the characteristic site of cytoplasmic staining pattern produced by auto-antibodies. The target antigen response for CANCA is a serine proteinase 3. The C-ANCA titer is highly specific for Wegener's granulomatosis (98%). The sensitivity to the assay varies with the status of the disease. During active generalized disease the assay is 95% sensitive. However, sensitivity falls as the disease becomes inactive. False positive C-ANCA results have been reported in patients with a number of infectious and neoplastic disorders. Although our patient had progessive erosion of her nasal midline, multiple biopsies failed to reveal evidence of vasculitis,
'granulomas or malignancy. There was never any evidence of pulmonary or renal involvement.
The initial evaluation of a patient with a septal perforation must consider the diagnoses demonstrated in Table I. In the event that the patient develops a concomitant palatal ulceration then the diagnosis becomes more narrowed. In addition to cocaine abuse, lethal mid-line granuloma, angiocentric T-cell lymphoma, squamous cell carcinoma and deep mycotic infections should be excluded.
To our knowledge, this is the fifth case of palatal perforation secondary to intranasal cocaine abuse reported in the literature. In one of the two reported
Med J Malaysia Vol 53 No 4 Dec 1998
cases 2, there was an obvious history of trauma to the nasal cavity caused by vigorous rubbing with nasal swabs, pencils and pens to remove the crusts. Our patient denied any form of trauma to the nasal cavity inflicted by foreign bodies.
In 1996,Armstrong and colleagues 3 reported a patient very similar to ours who developed a total septal perforation and a 7 mm oronasal fistula, a sedimentation rate elevated to 108 and a weakly positive ANCA of 1 to 40. As in our case, work up of Wegener's granulomatosis despite adequate biopsies was negative. \JVithout treatment over the course of the next twenty months, this patient's sedimentation rate and ANCA returned ro normal. The two year survival of untreated Wegener's
Table I Differential diagnosis for §eptal perforation
@ Idiopathic
ill Cocaine abuse
iI Wegener's granulomatosis
I) Lethal midline granuloma
@ Angiocentric T-cell Lymphoma
@ Malingnant Tumours
@ Deep mycotic infections
@ Rhinosporiodosis
Ii Rhinoscleroma
~ Systemic lupus erythematosus
il Iatrogenic secondary to nose picking or septal surgery
!I Tuberculosis
@ Sarcoidosis
® Hansen's disease
" Syphilis
<!l Radiation induced
437

CASE REPORT
granulomatosis is only 10% which our patient has outlived.
Kuriloff and Kimmelman1 reported a patient whose septal perforation progressed to hard palate involvement with an oronasal fistula. None of the patients had ANCA's performed in their review.
A C-ANCA positive result in a setting of septal perforation and oronasal fistula immediately raises ones suspicion for Wegener's granulomatosis. One should also pursue a history of cocaine abuse specifically with these patients since this may account for similar findings. Biopsies of the affected tissue should be taken
1. Gates GM, Jabs AD, Hugo NE. Perforation of hard palate associated with cocaine abuse. Annals of Plastic
Surgery 1991; 26(5): 446-68.
2. Sas try RC, Lee D, Har-el G. Palatal perforation from
cocaine abuse. Orolaryngology Head and Neck
Surgery 1997; 116: 565-66.
438
regardless of history in order to determine whether the patient has Wegener's granulomatosis.
The authors wish to acknowledge Professor Eugene N .. Myers, Chairman of the Department of Otolaryngology, The Eye and Ear Institute, University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, USA, for permission to publish this data. The first author was a Malaysian Fulbright Scholar to University of Pittsburgh Medical Center, Pittsburgh, Pennsylvania, United States of America for 1997.
3. Armstrong M, Shikani AH. Nasal septal necrosis
mimicking Wegener's granulomatosis in a cocaine
abuser. ENT Journal 1996; 75(9): 623-26.
4. Kuriloff DB, Kimmelman CH. Osteocartilaginous
necrosis of the sinonasal tract following cocaine
abuse. Laryngoscope 1989; 99: 918-24.
Med J Malaysia Vol 53 No 4 Dec 1998





























