Embed Size (px)
Citation preview
Profile of Dentofacial Deformities and Multidisciplinary Management in Hong Kong and Glasgow A retrospective, observational study
Introduction Dentofacial deformity is defined as “deviations from normal facial proportions and dental relationships that are severe enough to be handicapping”,1 and causes problems aesthetically, functionally, and psychosocially, leading to malocclusion, speech problems, and clinical depression, resulting in a decreased quality of life. 2
Dentofacial deformity encompasses a wide spectrum of features and underlying skeletal problems (Table 1). Recapping its definition as being “deviations from normal facial proportion”, it is essential, then, to recognize what normal is. Yet, it has been observed that distinct differences in norm exist inter-ethnically. For example, the Chinese face, when compared to that of Caucasian’s, has a wider outer-canthal distance, wider nasal base, and more protrusive lips.3 As clinicians, during treatment planning, it is thus crucial to take the patient’s ethnicity into consideration in order to maintain the natural appearance and the ethnicity of the patients after treatment. Hence, the importance of thorough and accurate diagnosis cannot be overstressed. With modern advanced technology, diagnosis is made easier with the help of cone-beam computed tomography (CBCT), where a 3-Dimensional (3D) evaluation of the deformity can be obtained and a 3D stereolithographic model be produced to allow trial surgery.4 – 6
Due to the complexity of cases, most require a team of cross-disciplinary specialists to provide well-rounded management. Leading the team are oral and maxillofacial surgeons and orthodontists, and other members of the team may include clinical psychologists, speech and hearing therapists, prosthodontists, periodontists, restorative dentists, and other medical specialists. Different surgical approaches have been implemented for the correction of dentofacial deformities, namely orthognathic surgery and distraction osteogenesis. Orthognathic surgery has a long history, dating back to 1897. To date, it remains as the standard approach in the management of dentofacial deformities.7 Distraction osteogenesis was extended from the orthopaedics, where it was developed in 1905 for leg lengthening.8 This technique was extensively researched and applied in cases of severe jaw hypoplasia. At present, there are a number of published articles focusing on the prevalence of dentofacial deformity in different parts of the world and/or reporting on the surgical treatment modalities in the correction of dentofacial deformity.5, 9 – 17 Yet, there are few published articles that highlight the multidisciplinary team approach in patient management, or offer comparison of ethnically different patients with dentofacial deformities following corrective jaw surgeries. This study is the first of the kind to offer cross-ethnic comparison, and aims to provide a comprehensive insight into the field of dentofacial deformities by comparing patient demography (age, gender, presenting complaint), diagnostic tools used, spectrum of diagnosis, duration of treatment, disciplines involved, and surgical techniques employed between patients who sought surgical correction for their dentofacial deformities in Hong Kong and Glasgow over the past ten years.
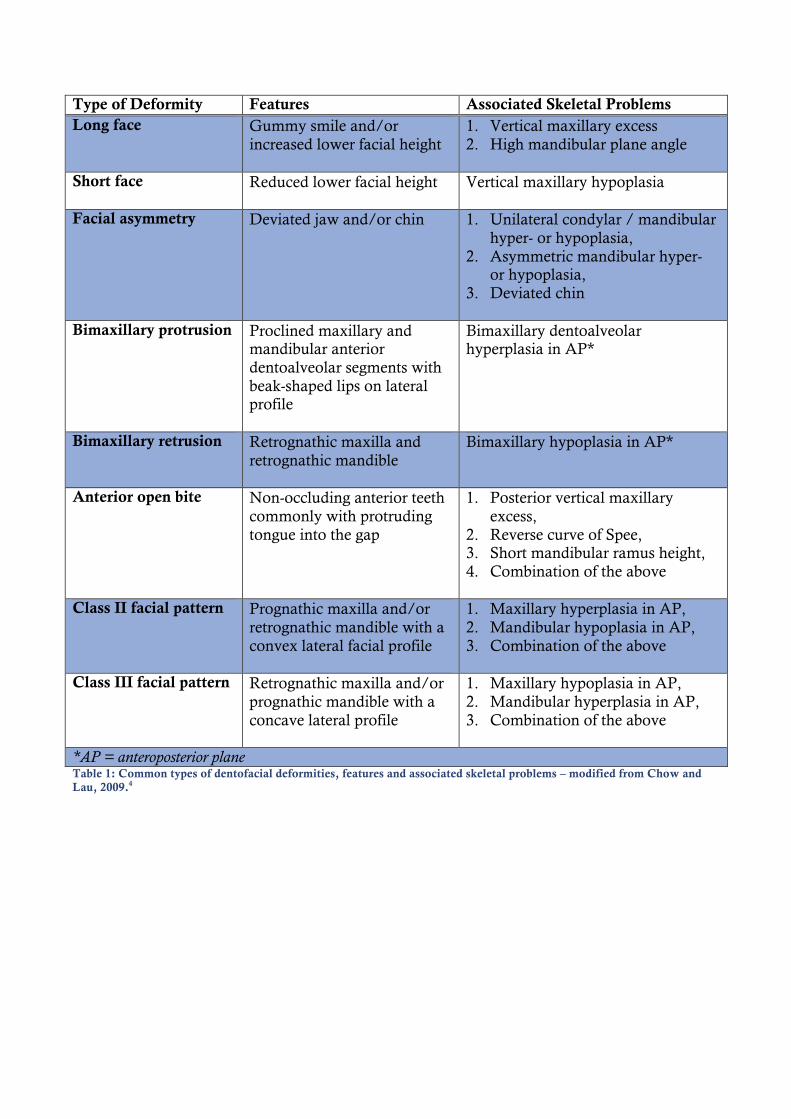
Type of Deformity Features Associated Skeletal Problems Long face Gummy smile and/or
increased lower facial height 1. Vertical maxillary excess 2. High mandibular plane angle
Short face Reduced lower facial height Vertical maxillary hypoplasia
Facial asymmetry Deviated jaw and/or chin 1. Unilateral condylar / mandibular
hyper- or hypoplasia, 2. Asymmetric mandibular hyper-
or hypoplasia, 3. Deviated chin
Bimaxillary protrusion Proclined maxillary and
mandibular anterior dentoalveolar segments with beak-shaped lips on lateral profile
Bimaxillary dentoalveolar hyperplasia in AP*
Bimaxillary retrusion Retrognathic maxilla and retrognathic mandible
Bimaxillary hypoplasia in AP*
Anterior open bite Non-occluding anterior teeth commonly with protruding tongue into the gap
1. Posterior vertical maxillary excess,
2. Reverse curve of Spee, 3. Short mandibular ramus height, 4. Combination of the above
Class II facial pattern Prognathic maxilla and/or
retrognathic mandible with a convex lateral facial profile
1. Maxillary hyperplasia in AP, 2. Mandibular hypoplasia in AP, 3. Combination of the above
Class III facial pattern Retrognathic maxilla and/or prognathic mandible with a concave lateral profile
1. Maxillary hypoplasia in AP, 2. Mandibular hyperplasia in AP, 3. Combination of the above
*AP = anteroposterior plane Table 1: Common types of dentofacial deformities, features and associated skeletal problems – modified from Chow and Lau, 2009.4
Material and Methods
Selection of Study Hospitals Two world-leading dental hospitals were selected – one in Asia and one in Europe. The Prince Philip Dental Hospital is a training hospital, working in collaboration with the Faculty of Dentistry of the University of Hong Kong. Similarly, the Glasgow Dental Hospital and School is part of the Medical School of the MVLS college of the University of Glasgow. Both dental hospitals are comparable in terms of their high reputation and standards. The multidisciplinary teams at each institute are recognized locally, nationally, and internationally for their excellent quality of care delivered to patients with dentofacial deformities. Thus, their treatment protocols can be compared. Being based in Hong Kong, the Prince Philip Dental Hospital naturally attracts mainly Chinese patients, whilst the Glasgow Dental Hospital and School, situated in Scotland, attracts predominantly Caucasian Scottish patients. This difference in ethnicity allows comparisons to be made between the two centres.
Selection of Patients Consecutive hospital records of patients with dentofacial deformities requiring surgical correction from 2003 to 2012 were obtained from the operation lists. There was no restriction on the age or the sex of the patients. Exclusion criteria included patients with cleft lip and/or palate, patients with acquired dentofacial defects, and patients who declined or did not complete treatment.
Data Collection
1. Demographics and background information The date of birth and the gender of the patients were recorded. The presenting complaints of the patients were categorized into mastication, speech, aesthetics, psychological, health-related, mal-alignment, traumatic bite, or temporomandibular joint (TMJ) problems. If any patient presented with other complaints, they were individually recorded separately. The date of referral, date of initial assessment at the Joint Orthognathic Assessment Clinic, date of commencement of orthodontic treatment, date of surgery, and date of de-bonding of the fixed orthodontic appliance were also recorded.
2. Oral and maxillofacial diagnosis The diagnosis was recorded according to the clinical notes from the initial assessment of the patient at the Joint Orthognathic Assessment Clinic. The skeletal pattern of the patient was recorded as class I, II, or III according to the basal relationship between the maxilla and the mandible. Other diagnoses that were recorded included asymmetry and open-bite. The skeletal deformities were categorized into the site of the problem, being the dentoalveolus, maxilla, mandible, mid-face, zygoma, condyle and chin together with the details of the deformity – hypo/hyperplasia, and the plane of deformity – transverse, vertical or anteroposterior.
3. Disciplines involved The different disciplines, aside from orthodontics and oral and maxillofacial surgery, which were involved in the treatment of each patient, were recorded based on the clinical notes and any referral letters found in a patient’s record. These included periodontology, restorative dentistry, prosthodontics, clinical psychology, speech and hearing, and other medical specialties.
4. Surgical treatment received These were recorded based on the finalized surgical plan formulated after assessment of the patients in the Joint Orthognathic Assessment Clinic upon the completion of the pre-surgical orthodontic treatment.
5. Pre-surgical planning records The pre-surgical planning records and radiography obtained from patients were noted according to the information provided in the clinical notes and in the imaging request folders.
Data Analysis Data was entered into the computer and analyzed using the Statistical Package for Social Sciences (SPSS) software. Chi-square test, Fisher’s exact test, Chi-square exact test, ANOVA, and student’s t-test were used with a threshold of significance set at p<0.05.
Ethics Approval This study has been approved by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (HKU/HA HKW IRB) and by the Hospital administration of the National Health Services in the Glasgow Dental Hospital and School.
Results
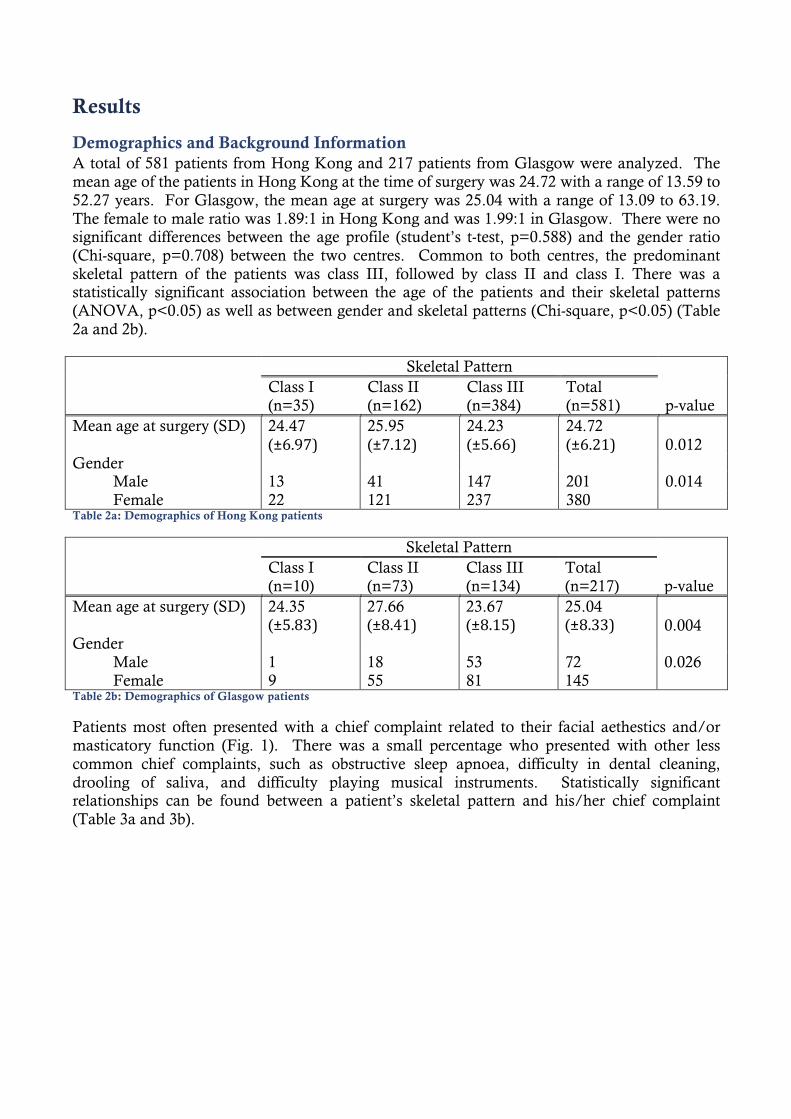
Demographics and Background Information A total of 581 patients from Hong Kong and 217 patients from Glasgow were analyzed. The mean age of the patients in Hong Kong at the time of surgery was 24.72 with a range of 13.59 to 52.27 years. For Glasgow, the mean age at surgery was 25.04 with a range of 13.09 to 63.19. The female to male ratio was 1.89:1 in Hong Kong and was 1.99:1 in Glasgow. There were no significant differences between the age profile (student’s t-test, p=0.588) and the gender ratio (Chi-square, p=0.708) between the two centres. Common to both centres, the predominant skeletal pattern of the patients was class III, followed by class II and class I. There was a statistically significant association between the age of the patients and their skeletal patterns (ANOVA, p<0.05) as well as between gender and skeletal patterns (Chi-square, p<0.05) (Table 2a and 2b). Skeletal Pattern
p-value Class I (n=35)
Class II (n=162)
Class III (n=384)
Total (n=581)
Mean age at surgery (SD) 24.47 (±6.97)
25.95 (±7.12)
24.23 (±5.66)
24.72 (±6.21) 0.012
Gender Male 13 41 147 201 0.014 Female 22 121 237 380 Table 2a: Demographics of Hong Kong patients
Skeletal Pattern
p-value Class I (n=10)
Class II (n=73)
Class III (n=134)
Total (n=217)
Mean age at surgery (SD) 24.35 (±5.83)
27.66 (±8.41)
23.67 (±8.15)
25.04 (±8.33) 0.004
Gender Male 1 18 53 72 0.026 Female 9 55 81 145 Table 2b: Demographics of Glasgow patients
Patients most often presented with a chief complaint related to their facial aethestics and/or masticatory function (Fig. 1). There was a small percentage who presented with other less common chief complaints, such as obstructive sleep apnoea, difficulty in dental cleaning, drooling of saliva, and difficulty playing musical instruments. Statistically significant relationships can be found between a patient’s skeletal pattern and his/her chief complaint (Table 3a and 3b).
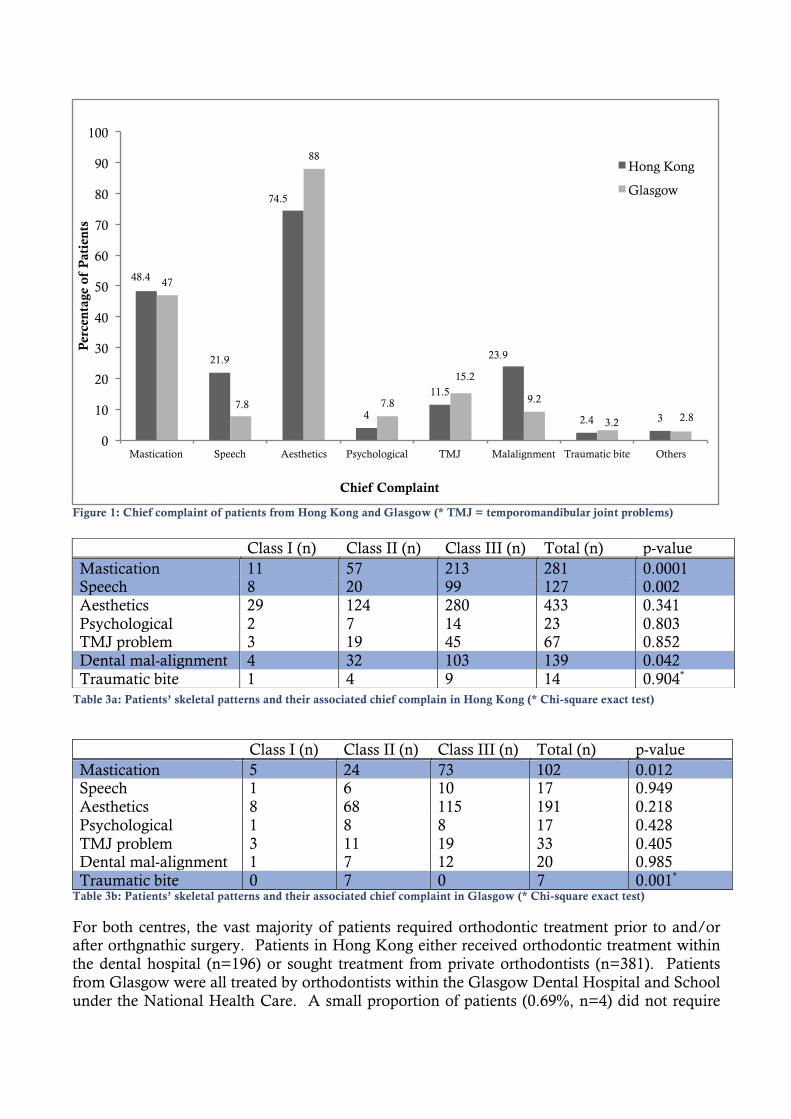
Class I (n) Class II (n) Class III (n) Total (n) p-value Mastication 5 24 73 102 0.012 Speech 1 6 10 17 0.949 Aesthetics 8 68 115 191 0.218 Psychological 1 8 8 17 0.428 TMJ problem 3 11 19 33 0.405 Dental mal-alignment 1 7 12 20 0.985 Traumatic bite 0 7 0 7 0.001*
Table 3b: Patients’ skeletal patterns and their associated chief complaint in Glasgow (* Chi-square exact test)
For both centres, the vast majority of patients required orthodontic treatment prior to and/or after orthgnathic surgery. Patients in Hong Kong either received orthodontic treatment within the dental hospital (n=196) or sought treatment from private orthodontists (n=381). Patients from Glasgow were all treated by orthodontists within the Glasgow Dental Hospital and School under the National Health Care. A small proportion of patients (0.69%, n=4) did not require
Class I (n) Class II (n) Class III (n) Total (n) p-value Mastication 11 57 213 281 0.0001 Speech 8 20 99 127 0.002 Aesthetics 29 124 280 433 0.341 Psychological 2 7 14 23 0.803 TMJ problem 3 19 45 67 0.852 Dental mal-alignment 4 32 103 139 0.042 Traumatic bite 1 4 9 14 0.904*
Table 3a: Patients’ skeletal patterns and their associated chief complain in Hong Kong (* Chi-square exact test)
48.4
21.9
74.5
4
11.5
23.9
2.4 3
47
7.8
88
7.8
15.2
9.2
3.2 2.8
0
10
20
30
40
50
60
70
80
90
100
Mastication Speech Aesthetics Psychological TMJ Malalignment Traumatic bite Others
Per
cent
age
of P
atie
nts
Chief Complaint
Hong Kong
Glasgow
Figure 1: Chief complaint of patients from Hong Kong and Glasgow (* TMJ = temporomandibular joint problems)
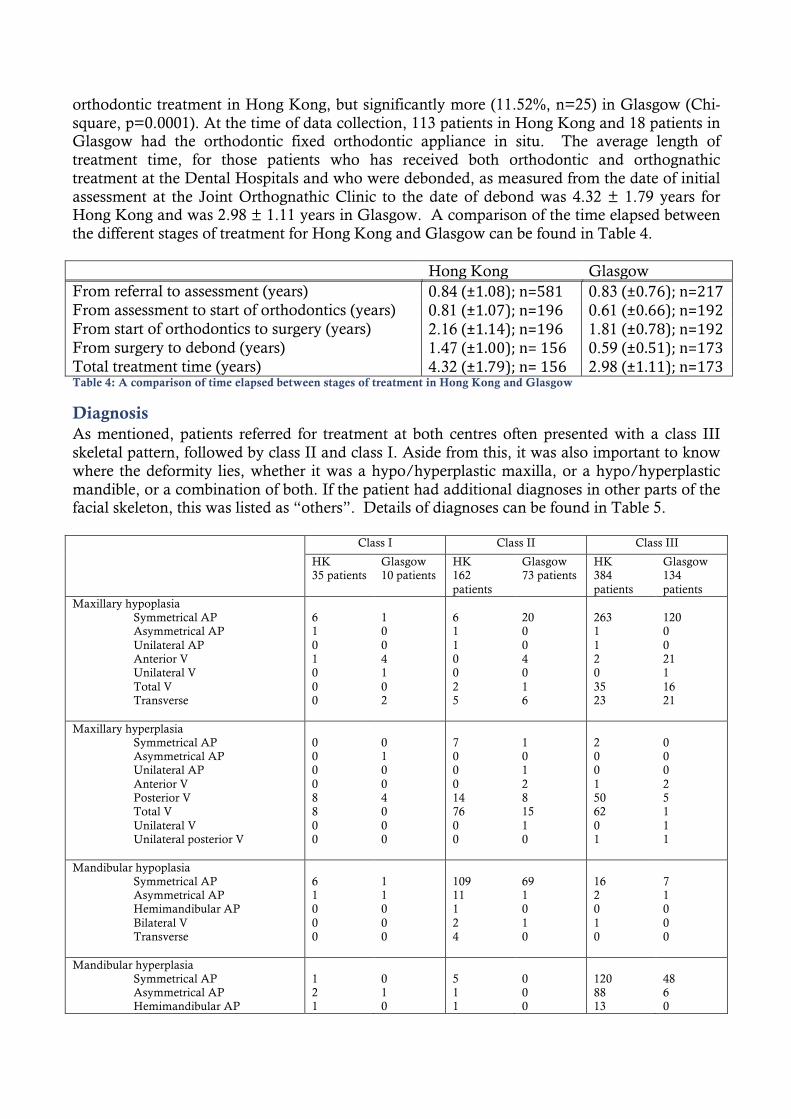
orthodontic treatment in Hong Kong, but significantly more (11.52%, n=25) in Glasgow (Chi-square, p=0.0001). At the time of data collection, 113 patients in Hong Kong and 18 patients in Glasgow had the orthodontic fixed orthodontic appliance in situ. The average length of treatment time, for those patients who has received both orthodontic and orthognathic treatment at the Dental Hospitals and who were debonded, as measured from the date of initial assessment at the Joint Orthognathic Clinic to the date of debond was 4.32 ± 1.79 years for Hong Kong and was 2.98 ± 1.11 years in Glasgow. A comparison of the time elapsed between the different stages of treatment for Hong Kong and Glasgow can be found in Table 4. Hong Kong Glasgow From referral to assessment (years) 0.84 (±1.08); n=581 0.83 (±0.76); n=217 From assessment to start of orthodontics (years) 0.81 (±1.07); n=196 0.61 (±0.66); n=192 From start of orthodontics to surgery (years) 2.16 (±1.14); n=196 1.81 (±0.78); n=192 From surgery to debond (years) 1.47 (±1.00); n= 156 0.59 (±0.51); n=173 Total treatment time (years) 4.32 (±1.79); n= 156 2.98 (±1.11); n=173 Table 4: A comparison of time elapsed between stages of treatment in Hong Kong and Glasgow
Diagnosis As mentioned, patients referred for treatment at both centres often presented with a class III skeletal pattern, followed by class II and class I. Aside from this, it was also important to know where the deformity lies, whether it was a hypo/hyperplastic maxilla, or a hypo/hyperplastic mandible, or a combination of both. If the patient had additional diagnoses in other parts of the facial skeleton, this was listed as “others”. Details of diagnoses can be found in Table 5. Class I Class II Class III
HK 35 patients
Glasgow 10 patients
HK 162 patients
Glasgow 73 patients
HK 384 patients
Glasgow 134 patients
Maxillary hypoplasia Symmetrical AP Asymmetrical AP Unilateral AP Anterior V Unilateral V Total V Transverse
6 1 0 1 0 0 0
1 0 0 4 1 0 2
6 1 1 0 0 2 5
20 0 0 4 0 1 6
263 1 1 2 0 35 23
120 0 0 21 1 16 21
Maxillary hyperplasia Symmetrical AP Asymmetrical AP Unilateral AP Anterior V Posterior V Total V Unilateral V Unilateral posterior V
0 0 0 0 8 8 0 0
0 1 0 0 4 0 0 0
7 0 0 0 14 76 0 0
1 0 1 2 8 15 1 0
2 0 0 1 50 62 0 1
0 0 0 2 5 1 1 1
Mandibular hypoplasia Symmetrical AP Asymmetrical AP Hemimandibular AP Bilateral V Transverse
6 1 0 0 0
1 1 0 0 0
109 11 1 2 4
69 1 0 1 0
16 2 0 1 0
7 1 0 0 0
Mandibular hyperplasia Symmetrical AP Asymmetrical AP Hemimandibular AP
1 2 1
0 1 0
5 1 1
0 0 0
120 88 13
48 6 0
Unilateral V Bilateral V Transverse
0 0 0
0 0 0
0 1 0
0 0 0
1 7 1
2 0 0
Bimaxillary retrusion
0 0 0 20 0 8
Dentoalveolar hypoplasia Maxilla Mandible Bimaxillary
0 1 0
0 0 0
2 3 0
0 0 0
1 2 0
0 0 0
Dentoalveolar hyperplasia Maxilla Mandible Bimaxillary
2 4 9
0 0 0
24 9 68
0 0 0
87 37 60
0 0 0
Open bite Anterior Posterior bilateral Posterior unilateral
9 0 0
6 0 0
22 0 0
10 1 0
60 0 0
12 0 3
Chin hypoplasia AP Vertical AP and vertical
8 0 1
1 0 0
99 2 3
0 1 0
22 3 1
1 0 0
Chin hyperplasia AP Vertical
0 0
0 0
2 3
1 1
8 9
0 1
Midface hypoplasia Nasomaxillary Nasomaxillary zygomatic
0 0
0 0
0 0
0 0
9 7
1 0
Zygomatic hypoplasia Bilateral AP Unilateral AP Unilateral V Bilateral transverse
0 0 0 0
1 0 0 0
1 1 0 0
2 0 0 0
3 6 1 0
21 1 0 1
Zygomatic hyperplasia Bilateral AP
0
0
0
0
1
1
Condyle Unilateral hyperplasia Unilateral hypoplasia Condylar resorption
11 0 0
1 1 0
3 0 5
0 0 0
104 0 0
6 0 0
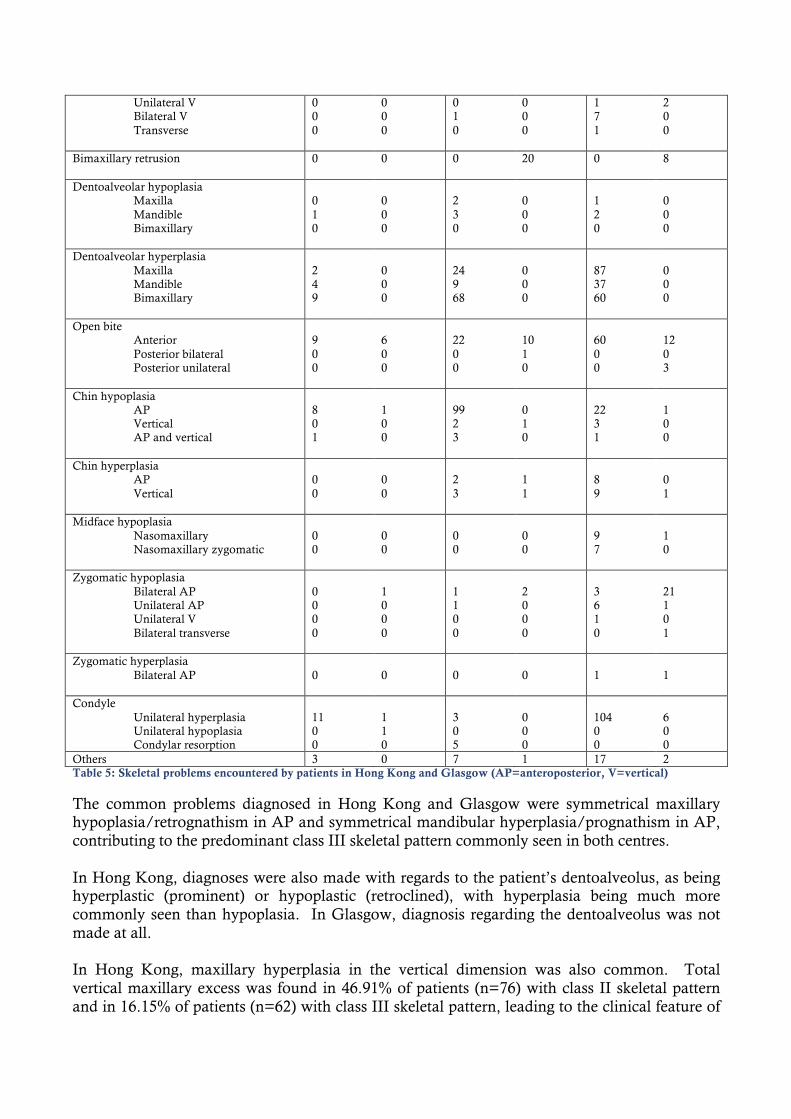
Others 3 0 7 1 17 2 Table 5: Skeletal problems encountered by patients in Hong Kong and Glasgow (AP=anteroposterior, V=vertical)
The common problems diagnosed in Hong Kong and Glasgow were symmetrical maxillary hypoplasia/retrognathism in AP and symmetrical mandibular hyperplasia/prognathism in AP, contributing to the predominant class III skeletal pattern commonly seen in both centres. In Hong Kong, diagnoses were also made with regards to the patient’s dentoalveolus, as being hyperplastic (prominent) or hypoplastic (retroclined), with hyperplasia being much more commonly seen than hypoplasia. In Glasgow, diagnosis regarding the dentoalveolus was not made at all. In Hong Kong, maxillary hyperplasia in the vertical dimension was also common. Total vertical maxillary excess was found in 46.91% of patients (n=76) with class II skeletal pattern and in 16.15% of patients (n=62) with class III skeletal pattern, leading to the clinical feature of
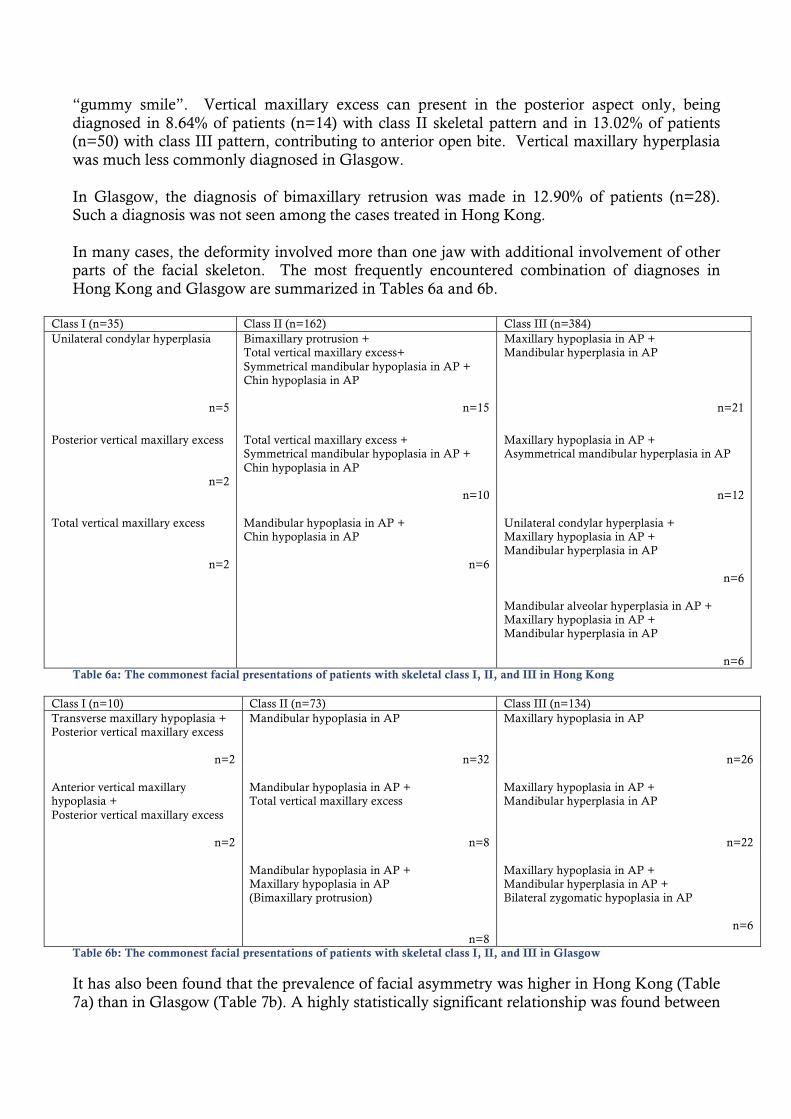
“gummy smile”. Vertical maxillary excess can present in the posterior aspect only, being diagnosed in 8.64% of patients (n=14) with class II skeletal pattern and in 13.02% of patients (n=50) with class III pattern, contributing to anterior open bite. Vertical maxillary hyperplasia was much less commonly diagnosed in Glasgow. In Glasgow, the diagnosis of bimaxillary retrusion was made in 12.90% of patients (n=28). Such a diagnosis was not seen among the cases treated in Hong Kong. In many cases, the deformity involved more than one jaw with additional involvement of other parts of the facial skeleton. The most frequently encountered combination of diagnoses in Hong Kong and Glasgow are summarized in Tables 6a and 6b.
Class I (n=35) Class II (n=162) Class III (n=384) Unilateral condylar hyperplasia
n=5
Bimaxillary protrusion + Total vertical maxillary excess+ Symmetrical mandibular hypoplasia in AP + Chin hypoplasia in AP
n=15
Maxillary hypoplasia in AP + Mandibular hyperplasia in AP
n=21
Posterior vertical maxillary excess
n=2
Total vertical maxillary excess + Symmetrical mandibular hypoplasia in AP + Chin hypoplasia in AP
n=10
Maxillary hypoplasia in AP + Asymmetrical mandibular hyperplasia in AP
n=12 Total vertical maxillary excess
n=2
Mandibular hypoplasia in AP + Chin hypoplasia in AP
n=6
Unilateral condylar hyperplasia + Maxillary hypoplasia in AP + Mandibular hyperplasia in AP
n=6
Mandibular alveolar hyperplasia in AP + Maxillary hypoplasia in AP + Mandibular hyperplasia in AP
n=6
Table 6a: The commonest facial presentations of patients with skeletal class I, II, and III in Hong Kong
Class I (n=10) Class II (n=73) Class III (n=134) Transverse maxillary hypoplasia + Posterior vertical maxillary excess
n=2
Mandibular hypoplasia in AP
n=32
Maxillary hypoplasia in AP
n=26 Anterior vertical maxillary hypoplasia + Posterior vertical maxillary excess
n=2
Mandibular hypoplasia in AP + Total vertical maxillary excess
n=8
Maxillary hypoplasia in AP + Mandibular hyperplasia in AP
n=22
Mandibular hypoplasia in AP + Maxillary hypoplasia in AP (Bimaxillary protrusion)
n=8
Maxillary hypoplasia in AP + Mandibular hyperplasia in AP + Bilateral zygomatic hypoplasia in AP
n=6
Table 6b: The commonest facial presentations of patients with skeletal class I, II, and III in Glasgow
It has also been found that the prevalence of facial asymmetry was higher in Hong Kong (Table 7a) than in Glasgow (Table 7b). A highly statistically significant relationship was found between
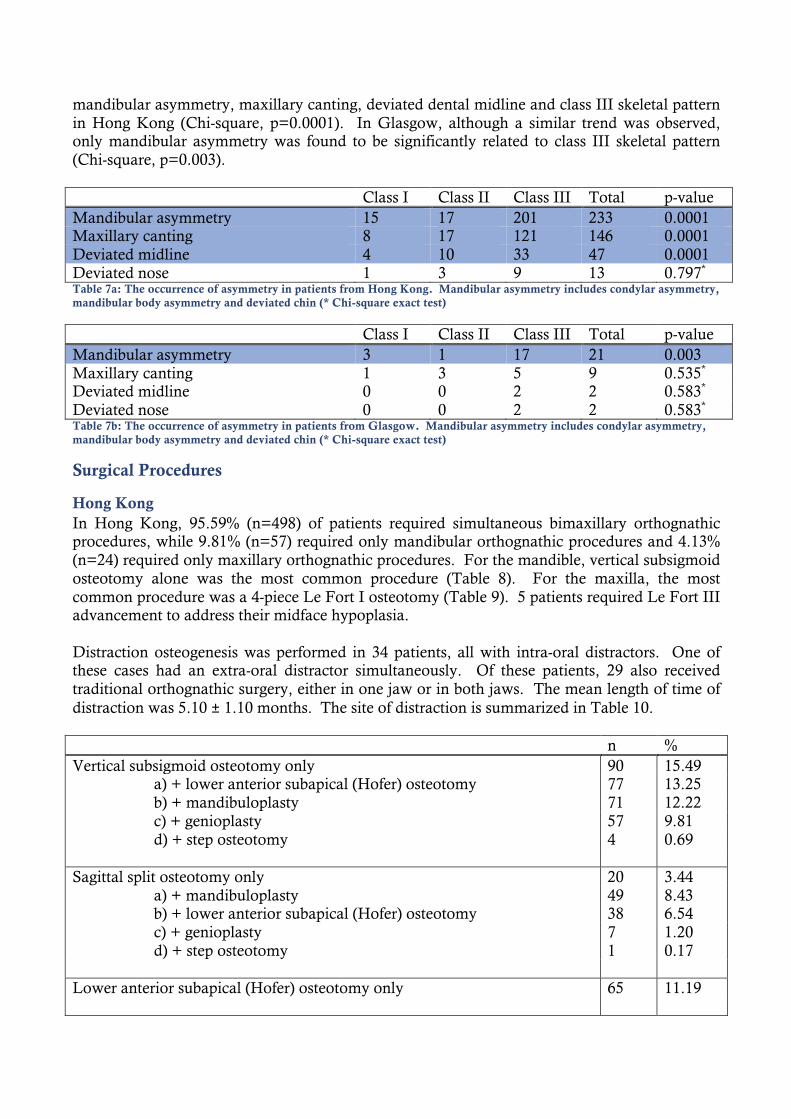
mandibular asymmetry, maxillary canting, deviated dental midline and class III skeletal pattern in Hong Kong (Chi-square, p=0.0001). In Glasgow, although a similar trend was observed, only mandibular asymmetry was found to be significantly related to class III skeletal pattern (Chi-square, p=0.003). Class I Class II Class III Total p-value Mandibular asymmetry 15 17 201 233 0.0001 Maxillary canting 8 17 121 146 0.0001 Deviated midline 4 10 33 47 0.0001 Deviated nose 1 3 9 13 0.797* Table 7a: The occurrence of asymmetry in patients from Hong Kong. Mandibular asymmetry includes condylar asymmetry, mandibular body asymmetry and deviated chin (* Chi-square exact test)
Class I Class II Class III Total p-value Mandibular asymmetry 3 1 17 21 0.003 Maxillary canting 1 3 5 9 0.535* Deviated midline 0 0 2 2 0.583* Deviated nose 0 0 2 2 0.583* Table 7b: The occurrence of asymmetry in patients from Glasgow. Mandibular asymmetry includes condylar asymmetry, mandibular body asymmetry and deviated chin (* Chi-square exact test)
Surgical Procedures
Hong Kong In Hong Kong, 95.59% (n=498) of patients required simultaneous bimaxillary orthognathic procedures, while 9.81% (n=57) required only mandibular orthognathic procedures and 4.13% (n=24) required only maxillary orthognathic procedures. For the mandible, vertical subsigmoid osteotomy alone was the most common procedure (Table 8). For the maxilla, the most common procedure was a 4-piece Le Fort I osteotomy (Table 9). 5 patients required Le Fort III advancement to address their midface hypoplasia. Distraction osteogenesis was performed in 34 patients, all with intra-oral distractors. One of these cases had an extra-oral distractor simultaneously. Of these patients, 29 also received traditional orthognathic surgery, either in one jaw or in both jaws. The mean length of time of distraction was 5.10 ± 1.10 months. The site of distraction is summarized in Table 10. n % Vertical subsigmoid osteotomy only 90 15.49 a) + lower anterior subapical (Hofer) osteotomy 77 13.25 b) + mandibuloplasty 71 12.22 c) + genioplasty 57 9.81 d) + step osteotomy 4 0.69 Sagittal split osteotomy only 20 3.44 a) + mandibuloplasty 49 8.43 b) + lower anterior subapical (Hofer) osteotomy 38 6.54 c) + genioplasty 7 1.20 d) + step osteotomy 1 0.17 Lower anterior subapical (Hofer) osteotomy only 65 11.19
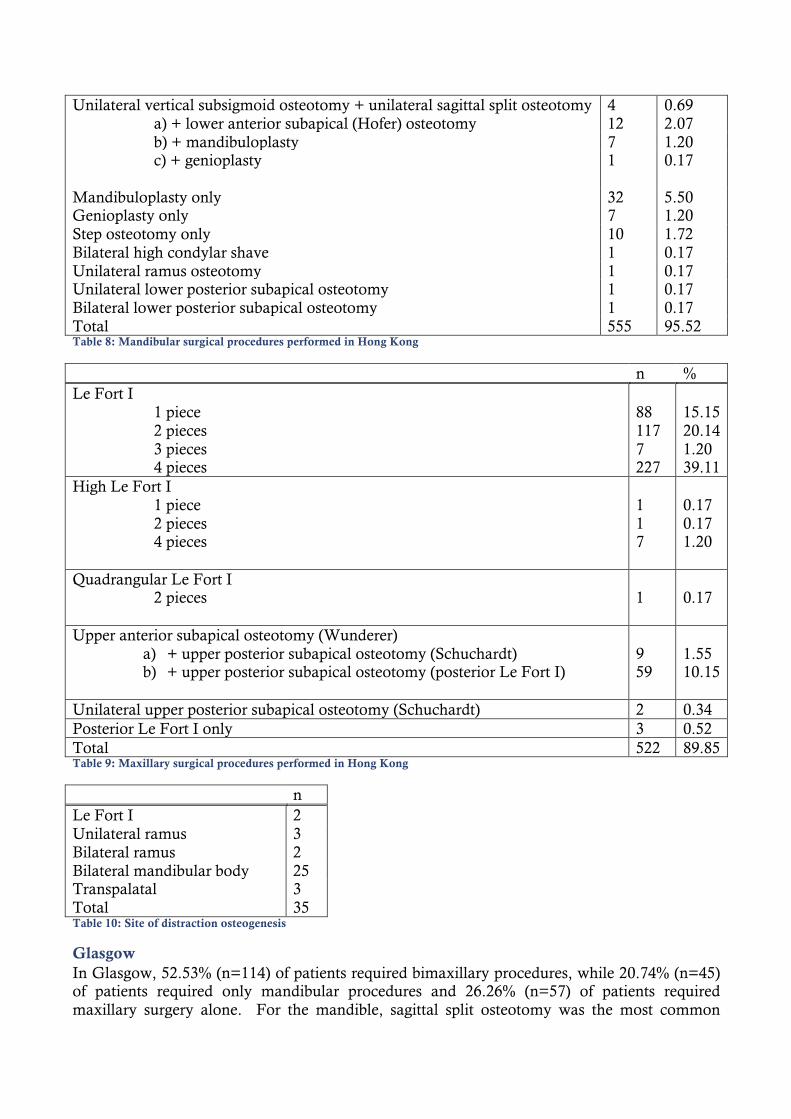
Unilateral vertical subsigmoid osteotomy + unilateral sagittal split osteotomy 4 0.69 a) + lower anterior subapical (Hofer) osteotomy 12 2.07 b) + mandibuloplasty 7 1.20 c) + genioplasty
1 0.17
Mandibuloplasty only 32 5.50 Genioplasty only 7 1.20 Step osteotomy only 10 1.72 Bilateral high condylar shave 1 0.17 Unilateral ramus osteotomy 1 0.17 Unilateral lower posterior subapical osteotomy 1 0.17 Bilateral lower posterior subapical osteotomy 1 0.17 Total 555 95.52 Table 8: Mandibular surgical procedures performed in Hong Kong
n % Le Fort I 1 piece 2 pieces 3 pieces 4 pieces
88 117 7 227
15.15 20.14 1.20 39.11
High Le Fort I 1 piece 2 pieces 4 pieces
1 1 7
0.17 0.17 1.20
Quadrangular Le Fort I 2 pieces
1
0.17
Upper anterior subapical osteotomy (Wunderer) a) + upper posterior subapical osteotomy (Schuchardt) b) + upper posterior subapical osteotomy (posterior Le Fort I)
9 59
1.55 10.15
Unilateral upper posterior subapical osteotomy (Schuchardt) 2 0.34 Posterior Le Fort I only 3 0.52 Total 522 89.85 Table 9: Maxillary surgical procedures performed in Hong Kong
n Le Fort I 2 Unilateral ramus 3 Bilateral ramus 2 Bilateral mandibular body 25 Transpalatal 3 Total 35 Table 10: Site of distraction osteogenesis
Glasgow In Glasgow, 52.53% (n=114) of patients required bimaxillary procedures, while 20.74% (n=45) of patients required only mandibular procedures and 26.26% (n=57) of patients required maxillary surgery alone. For the mandible, sagittal split osteotomy was the most common
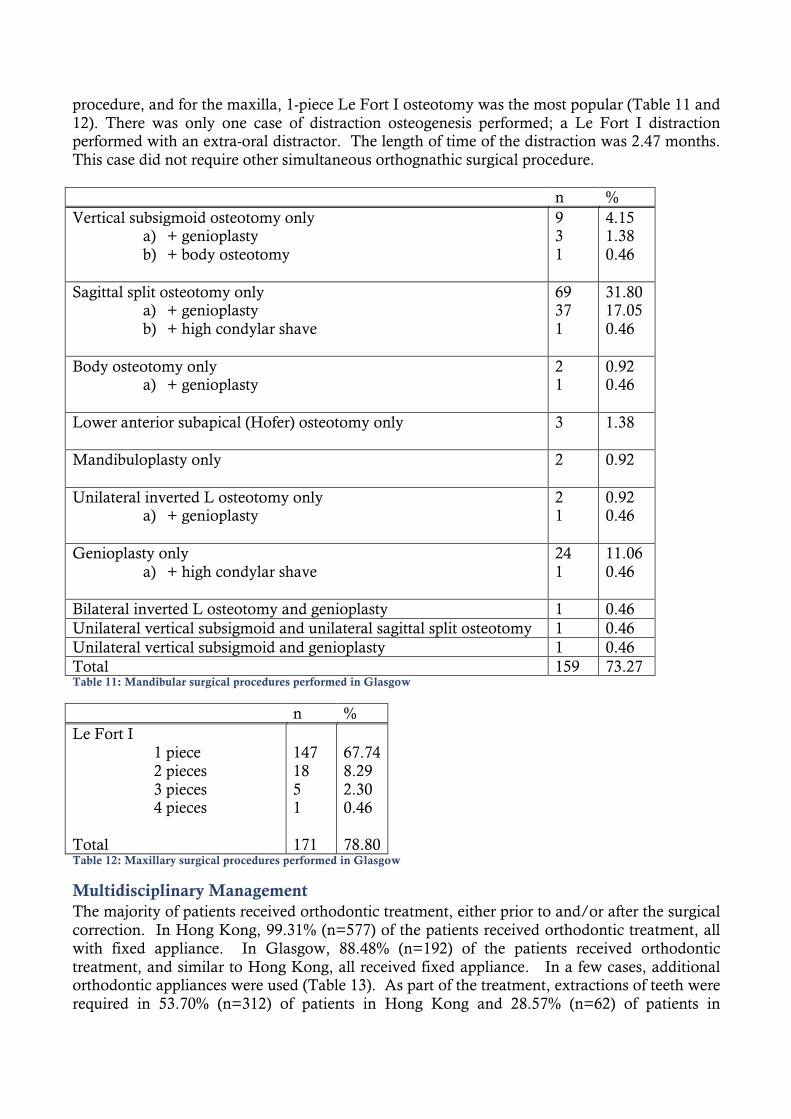
procedure, and for the maxilla, 1-piece Le Fort I osteotomy was the most popular (Table 11 and 12). There was only one case of distraction osteogenesis performed; a Le Fort I distraction performed with an extra-oral distractor. The length of time of the distraction was 2.47 months. This case did not require other simultaneous orthognathic surgical procedure. n % Vertical subsigmoid osteotomy only
a) + genioplasty b) + body osteotomy
9 3 1
4.15 1.38 0.46
Sagittal split osteotomy only a) + genioplasty b) + high condylar shave
69 37 1
31.80 17.05 0.46
Body osteotomy only a) + genioplasty
2 1
0.92 0.46
Lower anterior subapical (Hofer) osteotomy only
3
1.38
Mandibuloplasty only 2 0.92
Unilateral inverted L osteotomy only a) + genioplasty
2 1
0.92 0.46
Genioplasty only a) + high condylar shave
24 1
11.06 0.46
Bilateral inverted L osteotomy and genioplasty 1 0.46 Unilateral vertical subsigmoid and unilateral sagittal split osteotomy 1 0.46 Unilateral vertical subsigmoid and genioplasty 1 0.46 Total 159 73.27 Table 11: Mandibular surgical procedures performed in Glasgow
n % Le Fort I 1 piece 2 pieces 3 pieces 4 pieces Total
147 18 5 1 171
67.74 8.29 2.30 0.46 78.80
Table 12: Maxillary surgical procedures performed in Glasgow
Multidisciplinary Management The majority of patients received orthodontic treatment, either prior to and/or after the surgical correction. In Hong Kong, 99.31% (n=577) of the patients received orthodontic treatment, all with fixed appliance. In Glasgow, 88.48% (n=192) of the patients received orthodontic treatment, and similar to Hong Kong, all received fixed appliance. In a few cases, additional orthodontic appliances were used (Table 13). As part of the treatment, extractions of teeth were required in 53.70% (n=312) of patients in Hong Kong and 28.57% (n=62) of patients in
Glasgow. This was done either at the pre-surgical orthodontic stage or at the time of orthognathic surgery. Hong Kong (n) Glasgow (n) Quadhelix 3 4 Rapid maxillary expander 6 6 Upper removable appliance 1 2 Functional appliance 1 3 Table 13: Additional orthodontic appliances used in Hong Kong and Glasgow
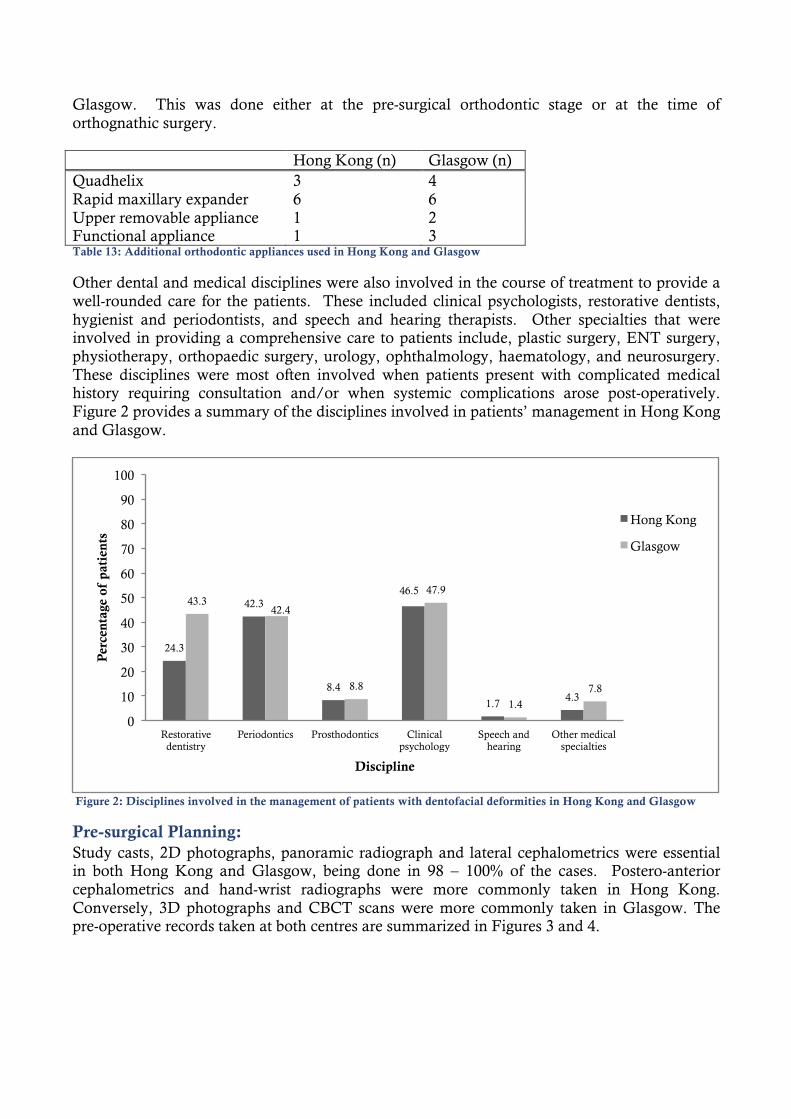
Other dental and medical disciplines were also involved in the course of treatment to provide a well-rounded care for the patients. These included clinical psychologists, restorative dentists, hygienist and periodontists, and speech and hearing therapists. Other specialties that were involved in providing a comprehensive care to patients include, plastic surgery, ENT surgery, physiotherapy, orthopaedic surgery, urology, ophthalmology, haematology, and neurosurgery. These disciplines were most often involved when patients present with complicated medical history requiring consultation and/or when systemic complications arose post-operatively. Figure 2 provides a summary of the disciplines involved in patients’ management in Hong Kong and Glasgow.
Figure 2: Disciplines involved in the management of patients with dentofacial deformities in Hong Kong and Glasgow
Pre-surgical Planning: Study casts, 2D photographs, panoramic radiograph and lateral cephalometrics were essential in both Hong Kong and Glasgow, being done in 98 – 100% of the cases. Postero-anterior cephalometrics and hand-wrist radiographs were more commonly taken in Hong Kong. Conversely, 3D photographs and CBCT scans were more commonly taken in Glasgow. The pre-operative records taken at both centres are summarized in Figures 3 and 4.
24.3
42.3
8.4
46.5
1.7 4.3
43.3 42.4
8.8
47.9
1.4
7.8
0
10
20
30
40
50
60
70
80
90
100
Restorative dentistry
Periodontics Prosthodontics Clinical psychology
Speech and hearing
Other medical specialties
Per
cent
age
of p
atie
nts
Discipline
Hong Kong
Glasgow
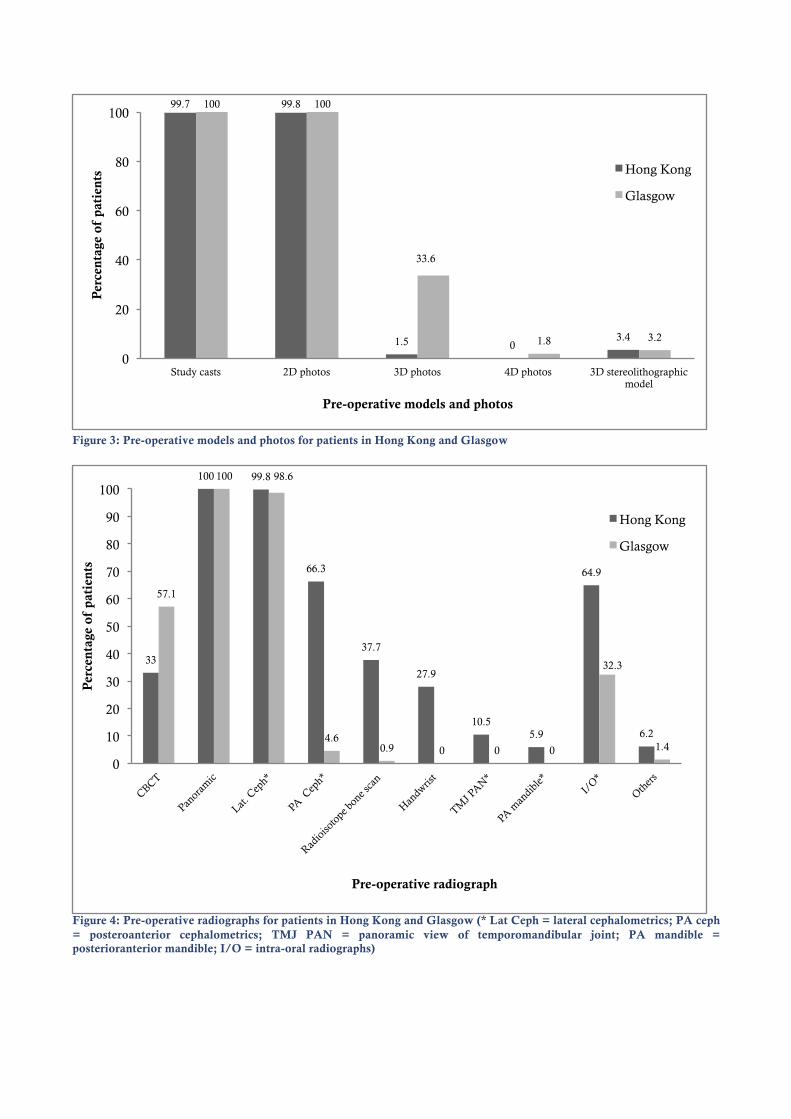
Figure 3: Pre-operative models and photos for patients in Hong Kong and Glasgow
Figure 4: Pre-operative radiographs for patients in Hong Kong and Glasgow (* Lat Ceph = lateral cephalometrics; PA ceph = posteroanterior cephalometrics; TMJ PAN = panoramic view of temporomandibular joint; PA mandible = posterioranterior mandible; I/O = intra-oral radiographs)
99.7 99.8
1.5 0 3.4
100 100
33.6
1.8 3.2
0
20
40
60
80
100
Study casts 2D photos 3D photos 4D photos 3D stereolithographic model
Per
cent
age
of p
atie
nts
Pre-operative models and photos
Hong Kong
Glasgow
33
100 99.8
66.3
37.7
27.9
10.5 5.9
64.9
6.2
57.1
100 98.6
4.6 0.9 0 0 0
32.3
1.4
0
10
20
30
40
50
60
70
80
90
100
Per
cent
age
of p
atie
nts
Pre-operative radiograph
Hong Kong
Glasgow
Discussion
Demographics Similar with other studies, the number of female patients in both Hong Kong and Glasgow outweighed that of male patients.9 – 17 This is expected as women have been reported to make use of medical services more than men,18 and females have consistently been found to perceive their body image more negatively and to express greater concerns regarding their facial features, particularly when their facial features differ greatly from those of their peers.19 The mean age of patient in Hong Kong and Glasgow was similar with that reported in various studies as being in the mid-20s.9-13, 17 It has been found that patients older than 41 years of age are less motivated to undergo surgery when compared to younger patients.20 This may be related to the greater concern with the risks of surgery in older patients versus the greater need for aesthetic improvement in the younger age group.20-22 Despite this, there is a new group of patients with dentofacial deformities over 40 year-old suffering from obstructive sleep apnoea, who may benefit from orthognathic surgery for correction of airway obstruction and this may change the age prevalence in future studies.
Diagnosis Similar to many published studies9, 10, 12, 13, 15, 17 the majority of patients seeking treatment in Hong Kong and Glasgow presented with a skeletal class III pattern. This could be due to the patients’ concern of a protruding lower jaw in class III deformity more than class II, of which the latter could be camouflaged by functional orthodontics during growth, aesthetically by a beard in males or by simply posturing the mandible forward. Coinciding with other studies, aesthetics was the most commonly cited chief complaint, suggesting that the wish for aesthetic improvement is a strong motivation for patients to proceed with orthognathic surgery.20, 23 The need for functional improvement such as mastication and speech was also significant, particularly in patients presented with a class III deformity. The reverse overjet often creates problems in mastication, where the action of incising food is impossible, and the patient relies solely on the posterior teeth for chewing. Similarly, it has been found that a class III malocclusion can distort the speech articulation.24 In Hong Kong, a high prevalence of mandibular asymmetry was found, commonly due to unilateral condylar hyperplasia or asymmetric mandibular hyperplasia. Hence, the pre-treatment diagnostic tools in Hong Kong included the prescription of Technetium-99 (Tc-99) radioactive isotope bone scan to evaluate the growth activity of the condyle, and the use of postero-anterior cephalometry. In addition to facial asymmetry, dentoalveolar hyperplasia was exclusively diagnosed in Hong Kong. This condition can occur in the maxilla, in the mandible, or in both the maxilla and the mandible, where in such cases, the diagnosis of bimaxillary protrusion is made. The prevalence of bimaxillary protrusion amongst the Asian population is high.15, 25 This is supported by the results of this study. Whilst asymmetry and dentoalveolar hyperplasia were common in Hong Kong, zygomatic hypoplasia was diagnosed more often for patients in Glasgow. This reflects one of the major differences in the acceptable facial profile between Asians and Caucasians.
Multidisciplinary Management In both centres, all patients are presented in a joint orthognathic assessment clinic, where a team of orthodontist and oral and maxillofacial surgeon assesses each patient together to discuss
his/her diagnosis and treatment plan. The same patient is presented again after pre-surgical orthodontics to assess his/her readiness for surgery and to finalize the surgical plan.
Involvement of Clinical Psychologist One major difference between Hong Kong and Glasgow is the level of involvement of clinical psychologists in the initial assessment of patients. In Glasgow, each patient is required to undergo a one-to-one clinical psychological assessment, to allow identification of cases not suitable for surgery and screening of potential psychological issues that may require professional counseling to prevent serious psychological crisis during treatment. The psychological service in Glasgow has provided support to patients during the immediate postoperative phase where adjustment and acceptance to the surgical changes was problematic. Yet, due to the much larger patient throughput, Hong Kong has adopted the use of two screening questionnaires – Brief Symptom Inventory (BSI) and Eysenck Personality Questionnaire Revised (EPQ-R) instead. Any patients with abnormal results from the above tests are subsequently referred to a dedicated clinical psychologist with PhD specialized in this field at the Clinical Psychology Department to receive detailed consultation and therapy. However, the use of screening questionnaires has some inherent limitations. For example, there is no mean of telling whether the patient is answering the questionnaire truthfully, and thus the sensitivity and specificity of the questionnaires may be challenged. As well, the patient’s psychology is a dynamic profile, with the level of anxiety increasing during pre-surgical orthodontics and climaxing in the immediate pre-operative periods26, 27 and the level of uncertainty and uneasiness peaking in the immediate post-operative periods as the patient is adjusting to the new appearance and coping with the post-operative stress. In this regard, having the patient fill out a questionnaire at any one given time pre-operatively and post-operatively may not be adequate to show the changing stress and anxiety of the patient throughout the perioperative period. This study has shown that aesthetics was the most prevalent chief complaint among patients seeking for combined orthodontic-orthognathic treatment. In fact, a study by Vulink et al. in 2008 showed that 10% of patients presented for orthognathic surgery may suffer from body dysmorphic disorder – a condition where patients become overly obsessed with their appearance without having a significant defect.28 These patients have unreal negative perception of their body image, and have unrealistic expectations of surgery. It is important for clinicians to be able to identify such patients prior to treatment to allow proper referrals to psychological or psychiatric colleagues, rather than attempting surgery. There are a number of screening questionnaires that can be used, including Body Dysmorphic Disorder Examination (BDDE) and Hospital Anxiety and Depression Scale (HADS). However, accurate result analysis of these questionnaires by non-psychiatrically trained clinicians is difficult.29 The importance of having a good liaison between oral and maxillofacial surgeons and a psychologist or psychiatrist in the multidisciplinary team approach to patients with dentofacial deformities is again highlighted.
Orthodontic Treatment In both centres, the majority of patients required both pre-surgical and post-surgical orthodontic treatment with fixed appliances to bring the dentition in line with the bony base and into functional occlusion. The length of pre-surgical orthodontics between the two teaching centres was similar, requiring approximately two years, and is comparable with that reported in other teaching centres.13 As for post-surgical orthodontic treatment, Hong Kong had a much longer time of 1.47 years as compared to 0.59 years in Glasgow and the 12 months reported by Martos Diaz et al. in 2010.13 Therefore, the average total treatment time for patients in Hong Kong was also longer. Whilst it is commonly believed that segmental osteotomy, which is highly
practiced in Hong Kong, can decrease the overall treatment time,30, 31 the results from this study showed otherwise. This may be due to the large number of patients in the orthodontic waiting list and lack of manpower, including postgraduates, coping with the large number of surgical patients, thus contributing to the longer post-surgical orthodontic treatment time in Hong Kong. This study also showed that whilst merely 0.69% of cases did not require orthodontic treatment in Hong Kong, this figure was significantly higher in Glasgow being 11.52% (Chi-square p=0.0001). This is theoretically practical if the patients present with well-aligned arches with no or minimal dentoalveolar compensation. Such patients can expect to have ideal occlusion once their skeletal problems are rectified via surgery. In reality, such cases are rare. Often, patients present with concurrent mal-alignment such as crowding and severe dentoalveolar compensation, particularly in severe skeletal class III cases. The higher number of cases without orthodontic treatment in Glasgow may reflect the difference in the profile of dental malocclusion between Hong Kong and Glasgow and the operators’ preference to accept mild dental mal-alignment in Glasgow.
Surgical Management
Surgical Planning: 2D versus 3D Since late 2008, CBCT has become part of the standard treatment planning protocol for every patient in Glasgow and the use of 3D stereo-photogrammetry is also gaining popularity, whilst in Hong Kong, the use of 2D plain radiography continues to be the standard protocol. CBCT can help to provide information critical to surgical planning, including the anatomy and the medio-lateral width of the ramus of the mandible, morphology of the inferior dental nerves, and position of roots for segmental procedures. A 3D diagnostic model can then be generated to show the morphology of the skeletal deformity, allowing surgical planning and computerized simulation surgery, resulting in higher quality outcomes and reduction in the length of surgery.32 Furthermore, the use of 3D prediction planning is of important value particularly in cases of facial asymmetry, where standard 2D CASSOS planning is limited as only the profile view of a patient is shown. In Hong Kong, where the prevalence of facial asymmetry is high, it is a surprise to see such low usage of CBCT and 3D planning in patients, and postero-anterior cephalometry was used instead. This is due to the concern of the significantly higher effective dose of radiation of CBCT when compared to conventional plain radiography,33 and its use may not be justifiable when conventional plain radiography may be adequate for diagnosis. Studies have shown limitations to the accuracy of 3D prediction planning with commercial software, such as Maxilim showing marked errors in the region of the upper lip.34 The superimposition of 3D facial photographs with CBCT images can also be technique sensitive and it is crucial to maintain the exact same facial expression for two non-simultaneous image captures. Otherwise, substantial error may be introduced. Moreover, capturing 3D facial photographs and CBCT images simultaneously also has a low feasibility, having to set-up the 3D stereo-photogrammetry instrument in front of the CBCT machine, which is both time and space consuming,35 and the practicality of performing 3D prediction planning for all patients is low due to time and space constraint. Clinical trials are ongoing. It will be interesting to compare the outcomes of treatment planned with 3D prediction with those planned with traditional 2D radiography and study models in terms of complications, operation time, patient satisfaction and cost-effectiveness.36 It is hard to critique, at this stage, the benefit of 3D planning in orthognathic surgery. Nevertheless, the use of 3D technology is the growing trend, and still remains the only possible way for prediction
planning of surgical correction of facial asymmetry. As 3D surgical navigation is gaining acceptance and as patients become more aware of its availability, a higher usage demand for 3D technology is expected in the coming years.
Segmental Osteotomy Segmental osteotomy is more commonly practiced in Hong Kong. This is due to the high prevalence of dentoalveolar hyperplasia. With regards to the maxilla, these patients often present with a hypoplastic maxilla but a hyperplastic maxillary dentoalveolus, leading to a protruding upper lip and reduced nasolabial angle but depressed paranasal area bilaterally. This poses a challenge in treatment if 1-piece Le Fort I osteotomy was to be used. In such cases, a 2-piece or 4-piece Le Fort I procedure is considered more appropriate where the anterior segment can be rotated independently of the others and the deformity be corrected in multiple planes.37 Likewise, mandibular segmental osteotomy such as lower anterior subapical (Hofer) osteotomy was practiced more commonly in Hong Kong to correct mandibular dentoalveolar hyperplasia. Similarly, segmental osteotomy was commonly employed in the correction of anterior open bite, which again has a higher incidence in Hong Kong.
Sagittal Split versus Vertical Subsigmoid Osteotomy In Hong Kong, it is a common practice to perform vertical subsigmoid osteotomy to setback the mandible and to perform sagittal split osteotomy for advancement. Since the majority of patients seeking treatment in Hong Kong present with a class III deformity, it is not a surprise to see the high number of cases requiring mandibular setback, hence the use of vertical subsigmoid osteotomy. In Glasgow, sagittal split osteotomy is the preferred procedure, in both mandibular advancement and setback. This is to avoid the use of intermaxillary fixation, which is normally required after vertical subsigmoid osteotomies. Intermaxillary fixation generally has poor patient acceptance, and can to lead potential complications such as poor oral hygiene, malnutrition, and aspiration of vomit, particularly in the early recovery period. Despite these disadvantages, studies have shown that vertical subsigmoid osteotomy can provide better immediate skeletal stability in cases of mandibular setback, owing to the lower condylar torque and the dissipation of forces of muscle pull from the stretching of the pterygomasseteric sling.38 In cases of mandibular setback with sagittal split, continuous remodeling at the osteotomy site and condylar resorption may lead to late relapse due to reduction in condylar height and results in anterior open bite.39 To overcome the disadvantages of intermaxillary fixation following vertical subsigmoid osteotomies, Hong Kong has pioneered the technique of rigid fixation for vertical subsigmoid osteotomy, via a transbuccal trocar or right angle drill and screwdriver in combination with an intraoral endoscope.40 With these technological advances, intermaxillary fixation, the main disadvantage of vertical subsigmoid osteotomy, may no longer be required, allowing vertical subsigmoid to be more effective in the treatment of mandibular prognathism over sagittal split in terms of short-term and long-term stability and the reduced risk of condylar resorption.
Distraction Osteogenesis Distraction osteogenesis has gained popularity in recent years due to the active research by Hong Kong in this field, with a much higher number of cases performed in Hong Kong than Glasgow. Clinical studies in Hong Kong have shown better stability in mandibular advancements using distraction in patients with high mandibular plane angles, and due to the gradual distention of both hard and soft tissue, the risk of neural complications due to the stretching of nerves are much lower.41 In cleft patients, it has been shown that maxillary distraction was more stable
than orthognathic surgery with Le Fort I osteotomy in the long term with 5-year follow up.42 Nevertheless, clinical trials of distraction osteogenesis in non-cleft patients are still limited. Despite this, the prolonged placement of distractors may be a source of chronic infection and anxiety during the distraction period.43 A second operation is required for the removal of distractors. The increasing cost of the distractors may be a prohibiting factor to many patients in popularizing the usage of distraction osteogenesis unless the hospital system is able to cover the cost of these devices. Yet, the use of distraction osteogenesis is expected to gain popularity, particularly in treatment of patients with congenital deformities and in patients with obstructive sleep apnoea as a result of excessively hypoplastic jaws.
Conclusion There exist large differences in the profile of dentofacial deformities in patients presenting for treatment in Hong Kong and Glasgow. Class III facial pattern was the most common category of dentofacial deformity presented for treatment in both centres. Bimaxillary protrusion and facial asymmetry had a higher prevalence in Hong Kong, whilst bimaxillary retrusion and zygomatic hypoplasia were diagnosed more often in Glasgow. For both centres, a multidisciplinary team was involved in the treatment of patients, with oral and maxillofacial surgeons and orthodontists leading the team. In Glasgow, clinical psychologists also play integral roles in the team, having extensive responsibilities such as preoperative psychological counseling. In Hong Kong, due to the higher patient throughput, psychological screening questionnaires were used and referrals to clinical psychologists were only made when results from the questionnaires indicated. Preoperatively, comprehensive investigations including 2D and 3D photography, dental models, radiography, and cephalometry, were undertaken in both centres for the preparation of the patients for surgery. The use of 3D surgical planning, including 3D photography and CBCT is part of the treatment protocol in Glasgow. Conversely, the use of 3D surgical planning is reserved for complex cases in Hong Kong. Concerning surgical techniques, Hong Kong, with a higher complexity of deformities, commonly performed osteotomies on both jaws and practiced segmental osteotomies, such as Hofer osteotomy of the mandible and multi-piece Le Fort I osteotomy of the maxilla, in order to achieve a normal occlusion and balanced facial proportion. On the contrary, Glasgow seldom performed segmental or subapical osteotomies and many patients had surgery only in one jaw. For the treatment of class III patients with mandibular hyperplasia, Hong Kong preferred to use vertical subsigmoid osteotomy whereas Glasgow used sagittal split osteotomy. Aside from traditional orthognathic surgery, distraction osteogenesis is also gaining popularity in Hong Kong and is being extensively researched and employed in patients where extensive jaw advancements are required. Word count: 4992 (excluding title and headings, tables and figures, and references)
References 1. Proffit WR, Sarver DM. Contemporary Treatment of Dentofacial Deformity. Mosby, 2003. 2. McGrath C, Zhang M, Hagg U. The impact of malocclusion and its treatment on quality of life: A literature
review. International Journal of Paediatric Dentistry. 2006;16:381-87. 3. Teck SRS, Smith JD, Chan ASY. (2000). Comparison of the aesthetic facial proportions of Southern Chinese
and White women. Archives of Facial Plastic Surgery. 2000;2:113-20. 4. Chow B, Lau A. The planning of orthognathic surgery – The digital era. The Hong Kong Medical Diary.
2009;14:11-14. 5. Moos KF, Ayoub AF. The surgical correction of dentofacial deformities: Past, present and future. Egyptian
Journal of Oral and Maxillofacial Surgery. 2010;1:2-6. 6. Gibson I, Cheung LK, Chow SP, Cheung WL, Beh SL, Savalani M, Lee SH. The use of rapid prototyping to
assist medical applications. Rapid Prototyping Journal 2006;12:53-8. 7. Steinhauser EW. Historical development of orthognathic surgery. Journal of Cranio-Maxillofacial Surgery.
1996;24:195-204. 8. McCarthy JG, Stelnicki EJ, Mehrara BJ, Longaker M. Distraction osteogenesis of the craniofacial skeleton.
Plastic and Reconstructive Surgery. 2001;107:1812-27. 9. Boeck EM, Lunardi N, Pinto A. Occurrence of skeletal malocclusions in Brazilian patients with dentofacial
deformities. Brazilian Dental Journal. 2001;22:340-5. 10. Ong M. Spectrum of dentofacial deformities: A retrospective survey. Annals Academy of Medicine Singapore.
2004;33:239-42. 11. Scariot R, da Costa DJ, Rebellato NLB. Epidemiological analysis of orthognathic surgery in a hospital in
Curitiba, Brazil: Review of 195 cases. Revista Espanola de Cirugia Oral y Maxillofacial. 2010;32:147-151. 12. Chew MT. Spectrum and management of dentofacial deformities in a multiethnic Asian population. Angle
Orthodontist. 2006;76:806-9. 13. Martos Diaz P, Garcia RG, Gias LN. Time used for orthodontic surgical treatment of dentofacial deformities
in white patients. Journal of Oral and Maxillofacial Surgery. 2010;68:88-92. 14. Zia AU, Qazi HS, Khan WU. The pattern of skeletal representation at Islamabad Dental Hospital: An
estimate of their minimum reporting frequency to aid in planning areas of future research. Pakistan Orthodontic Journal. 2011;3:11-5.
15. Samman N, Tong ACK, Cheung LK. Analysis of 300 dentofacial deformities in Hong Kong. International
Journal of Adult Orthodontic Orthognathic Surgery. 1992;7:181-5. 16. Baily LJ, Haltiwanger LH, Blakery GH, Proffit WR. Who seeks surgical-orthodontic treatment: A current
review. International Journal of Adult Orthodontic Orthognathic Surgery. 2001;16:280-92. 17. Al-Deaiji A. Characteristics of dentofacial deformities in a Saudi population. Saudi Dental Journal.
2001;13:101-5. 18. Green CA, Pope CR. Gender, psychosocial factors and the use of medical services: A longitudinal analysis.
Social Sciences and Medicine. 1999;48:1363-72. 19. Tung AW, Kiyak HA. Psychological influences on the timing of orthodontic treatment. American Journal of
Orthodontics and Dentofacial Orthopedics. 1998;113:29-39.
20. Mayo KH, Vig KD, Vig PS, Kowalski CJ. Attitude variables of dentofacial deformity patients: Demographic characteristics and associations. Journal of Oral and Maxillofacial Surgery. 1991;49:594-602.
21. Shalhoub SY. Scope of oral and maxillofacial surgery: The psychosocial dimensions of orthognathic surgery.
Australian Dental Journal. 1994;39:181-3. 22. Flanary CM, Barnwell GM Jr, Alexander JM. Patient perceptions of orthognathic surgery. American Journal of
Orthodontics. 1985;88:137-45. 23. Rivera SM, Hatch JP, Dolce C, Bays RA, Va Sickels JE, Rugh JD. Patients’ own reasons and patient-
perceived recommendations for orthognathic surgery. American Journal of Orthodontics and Dentofacial Orthopedics. 2000;118:134-40.
24. Vallino LD, Tompson B. Perceptual characteristics of consonant errors associated with malocclusion. Journal
of Oral and Maxillofacial Surgery. 1993;51:850-6. 25. Chu YM, Chen RPH, Morris DE, Ko WEC, Chen YR. Surgical approach to the patient with bimaxillary
protrusion. Clinics in Plastic Surgery. 2007;34:535-46. 26. Cunningham SJ, Gilthorpe MS, Hunt NP. Are pre-treatment psychological characteristics influenced by pre-
surgical orthodontics? European Journal of Orthodontics. 2001;23:751-8. 27. Cunningham SJ, Gilthorpe MS, Hunt NP. Are orthognathic patients different? European Journal of
Orthodontics. 2006;22:195-202. 28. Vulink NCC, Rosenberg A, Plooij JM, Koole R, Berge SJ, Denys D. Body dysmorphic disorder screening in
maxillofacial outpatients presenting for orthognathic surgery. International Journal of Oral and Maxillofacial Surgery. 2008;37:985-91.
29. Cunningham SJ, Feinmann C. Psychological assessment of patients requesting orthognathic surgery and the
relevance of body dysmorphic disorder. Journal of Orthodontics. 1998;25:293-8. 30. Yokoo S, Komori T, Watatani S. Indications and procedures for segmental dentoalveolar osteotomy: A review
of 13 patients. International Journal of Adult Orthodontics and Orthognathic Surgery. 2002;17:254-63. 31. Chen YR, Yeow VKL. Multiple-segment osteotomy in maxillofacial surgery. Plastic and Reconstructive Surgery.
1999;104:381-88. 32. Santher G, Kracher H, Ruda C. Indications and limitations of three-dimensional models in cranio-
maxillofacial surgery. Journal of Cranio-Maxillofacial Surgery. 1998;26:11-6. 33. Roberts JA, Drage NA, Davies J. Effective dose from cone beam CT examinations in dentistry. The British
Journal of Radiology. 2009;82:35-40. 34. Shafi MI, Ayoub AF, Ju X, Khambay BS. The accuracy of three-dimensional prediction planning for the
surgical correction of facial deformities using Maxilim. International Journal of Oral and Maxillofacial Surgery. 2013 (in press).
35. Naudi KB, Benramadan R, Brocklebank L, Ayoub AF, Ju X, Khambay BS. The virtual human face –
superimposing the simultaneously captured 3D photorealistic skin surface of the face on the untextured skin image of the CBCT scan. International Journal of Oral and Maxillofacial Surgery. 2013 (in press).
36. Jayaratne YSN, Zwahlen RA, Lo J, Tam SC, Cheung LK. Computer-aided maxillofacial surgery: An update.
Surgical Innovation. 2010;17:217-25. 37. Kahnberg KE, Hagberg B. The approach to dentofacial skeletal deformities using a multisegmentation
technique. Clinics in Plastic Surgery. 2007;34:477-84.
38. Ayoub AF, Millett DT, Hasan S. Evaluation of skeletal stability following surgical correction of mandibular prognathism. British Journal of Oral and Maxillofacial Surgery. 2000;38:305-11.
39. Eggensperger N, Raditsch T, Taghizadeh F, Iizuka T. Mandibular setback by sagittal split ramus osteotomy: A
12-year follow-up. Acta Odontologica Scandinavica. 2005;63:183-8. 40. Cheung LK, Lo J. Endoscope-assisted rigid fixation for intraoral vertical subsigmoid osteotomy: A preliminary
clinical study. Journal of Oral and Maxillofacial Surgery. 2010;68:8-14. 41. Ow A, Cheung LK. Skeletal stability and complications of bilateral sagittal split osteotomies and mandibular
distraction osteogenesis: An evidence-based review. Journal of Oral and Maxillofacial Surgery. 2009;67:2344-53. 42. Chua HDP, Ho SMY, Cheung LK. The comparison of psychological adjustment of patients with cleft lip and
palate after maxillary distraction osteogenesis and conventional orthognathic surgery. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2012;114:S5-S10.
43. Cenzi R, Farina A, Zuccarino L, Carinci F. Clinical outcome of 285 Mepor grafts used for craniofacial
reconstruction. Journal of Craniofacial Surgery. 2005;16:526-30.