Embed Size (px)
DESCRIPTION
Bangladesh Overview: Progress of Newborn Health Activities and Vision for the FuturePresentation by Dr. Mohammod Shaidullah
Citation preview

Bangladesh Overview: Progress of Newborn Health Activities
and Vision for the Future
Professor Dr. Mohammod Shahidullah
Helping Babies Survive Asia Regional Workshop
Dhaka, April 8, 2015

Structure
• Context • Policy response • Program response • Key challenges • Way forward

Context

133
116
94 88
65
53
41 48
87 82
66 65
52 43
33 31
52 48 42 41 37
32 24 22
0
20
40
60
80
100
120
140
1993 1997 2001 2004 2007 2011 2013 2015
U-5 MR
IMR
NMR
MDG Target
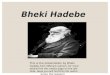
Bangladesh has achieved MDG 4 !
UN-IAGCME 2013
Source: BDHS, UN-IAGCME- UN Inter-agency group for Child Mortality Estimation, 2013
Bangladesh is 1 of 23 countries on track to achieve MDG4
& has the 4th most rapid rate of decline in child
mortality

Proportion of neonatal deaths among U5: Increasing trend
39% 41% 45% 47%
57% 60%
0%
10%
20%
30%
40%
50%
60%
70%
1989-93 1992-94 1995-99 1999-03 2002-06 BDHS 2011

National burden of mortality
• Neonatal mortality rate 24.4 per 1,000 live births (2012) [2] 75,903 neonatal deaths (2012) [2]
• Stillbirth rate 36.0 per 1,000 total births (2009) [1] 117,442
stillbirth (2009) [4]
• Maternal mortality ratio- 194 per 100,000 live births (2010) [3] 7,300 maternal deaths (2010) [3] -
[1] WHO (2013): Global Health Observatory Data Repository ( still birth rate originally published in Consens et al, Lancet 2011); [2] UNICEF/WHO/The World Bank/UN Pop Div. Levels and Trends in Child Mortality. Report 2013.
[3] Bangladesh Maternal Mortality Survey 2010
[4] Estimated

Mortality rate by age group: Bangladesh, region and globe
19.3
5.4
9 7.6
22.5
6.4
14.2
10.5
14
4.4
13.2 13.1
0
5
10
15
20
25
Early NMR Late NMR Post neonatal IMR Post infant Under5 Mortality
Bangladesh Region Global
IGME Estimate- 2013

Causes of newborn mortality (Bangladesh)
• The Three Major Causes Contributes 88% of all newborn deaths
1. Complications of preterm birth
2. Intra-partum related (Birth Asphyxia)
3. Severe Infection 1. Data source: Bangladesh-specific
mortality estimâtes (Liu et al. 2012).

The first day of life : The most dangerous day
• Worldwide, the day a child is born is by far the most dangerous day in a child’s life because mortality is very high in the first 24 hours after birth.
• In Bangladesh 21% of all deaths in children younger than 5 years happened in first day of their life and the estimated first day death in 2012 was 28,100. **
Day 0 37%
Day 1 13%
Day 2-7
31%
Day 8-28
19%
Surviving the First Day. State of the World’s Mothers 2013, Save the Children BDHS 2011 data

Prematurity /LBW 11%
Pneumonia 13%
Prematurity /LBW 11% Undefined
20%
BDHS 2011
Neonatal Deaths
Neonatal Infections and Pneumonia (38,000 deaths)
Reducing neonatal mortality is key to future progress

0-28 d
Pneumonia 13%
Prematurity /LBW 11%
Undefined 20%
Neonatal Deaths
Preterm birth (12,000 deaths + 20,000 deaths as underlying cause)
Neonatal Infections and Pneumonia (38,000 deaths)
Reducing neonatal mortality is key to future progress
BDHS 2011

Neonatal Deaths
Pneumonia 13%
Prematurity /LBW 11% Undefined
20% Preterm birth (12,000 deaths + 20,000 deaths as underlying cause)
Birth Asphyxia (21,500 deaths):
Neonatal Infections and Pneumonia (38,000 deaths)
Reducing neonatal mortality is key to future progress
Neonatal sepsis, birth asphyxia and prematurity/LBW accounts for 63% of all newborn deaths; significant portion of these deaths could be averted through Immediate Newborn Care and Ante Natal Care
BDHS 2011

Policy response

Milestone research initiatives in Bangladesh
• Projahnmo trial – 34% reduction in neonatal mortality through a package of community based interventions. A home care strategy to promote an integrated package of preventive and curative newborn care is effective in reducing neonatal mortality in communities with a weak health systems, low health care use, and high neonatal mortality. (Lancet, 2008)
• Chlorhexidine trial – Significant neonatal mortality reduction with single application of CHX, and severe cord infection reduction with multiple application of CHX was observed. Chlorhexidine cleansing of a neonate’s umbilical cord can save lives, but further studies are needed to establish the best frequency with which to delivery the intervention. (Lancet, 2012)
• SATT trial – Results suggest that the two alternative antibiotic regimens (i. gentamicin single dose and oral amoxicillin twice daily for 7 days and, ii. procain bezylpenicillin and gentamicin single dose for 2 days followed by oral amoxicillin twice daily for 5 days) for outpatient treatment of clinical signs of severe infection in young infants whose parents refused hospital admission are as efficacious as thee standard regimen (procain bezylpenicillin and gentamicin single dose for 7 days). This finding could increase treatment options in resource-poor settings when referral care is not available or acceptable. (Lancet 2015)

Policy and strategic initiatives for newborn health during 2009-2014
National Neonatal Health Strategy and Guidelines developed in 2009
Scale-Up Plan incorporated in the MNCH-OP in 2013
SOP developed for Facility Newborn Care in 2011
National Scale-up of HBB initiative 2012-13
National Technical Committee formed in 2013
Training modules developed in 2012
Capacity building of service providers on newborn care 2012
National IEC materials developed and distributed on newborn care 2012
Community based newborn care scaled-up in >20 districts 2012
SCANU scaled-up in 34 districts by 2015
HIMS on newborn health developed and integrated in DHIS 2 (2013)
BNA conducted and draft BENAP developed in 2014-15

Bangladesh Declaration for Ending Preventable Child Deaths by 2035

Maternal Health interventions
1. Skilled birth attendance (CSBAs and Midwives)
2. Functional and 24/7 BEmONC and CEmONC at strategically located facilities
Newborn health specific
interventions
3. Essential newborn care with newborn resuscitation & application of Chlorhexidine
4. Antenatal steroids for premature labor and Kangaroo mother care (KMC) for premature/low birth weight babies
5. Neonatal sepsis management at PHC level
6. Specialized newborn care at district & sub-district level
Child Health specific interventions
7. Effective referral linkage to ensure continuum of care – from community clinics to district /tertiary hospitals
8. IMCI at all levels
9. Multi-sectoral approach to promote exclusive BF and IYCF
10. Community based child drowning prevention activities
11. New vaccines: pneumococcal and rotavirus
Bangladesh Declaration for Ending Preventable Child Deaths by 2035: Interventions

Benchmarks for progress tracking of key interventions
0
0
0
28%
40%
50%
20%
50%
80%
90%
50%
80%
0% 20% 40% 60% 80% 100%
Antenatal corticosteroid
CHX umbilical cord cleansing
KMC for pre-term baby
Neonatal sepsis treatment
32% 50%
80% Skilled attendant at birth
Current Target 2016 Target 2020
Mat
erna
l H
ealth
In
terv
entio
ns
New
born
Hea
lth
Inte
rven
tions
New Interventions

ENAP Initiatives
National Guideline
Development under NTWC
and NCC
Global Initiative for
Child Survival Call for Action &
APR
National Policy
Dialogue initiated in
2012
Bangladesh Every
Newborn Action Plan
2014
Consensus build on priority
intervention 2012
Political Commitments
and Target Fixation
2013
4 Guideline Developed
2014
Partnership: MOH&FW, DPs, NGOs, Academicians and Researchers
COIA UNCoLSC EMEN
GAPPD
EPMM APR
Linking with global initiatives towards a national action plan

Program response

Development of national guideline for 4 new newborn interventions
Four Technical sub-groups formed by NTWC on NBH for development of Guideline and Protocols (CHX, ACS, KMC and NB Sepsis) in light of HBS. We are heading towards development, pilot testing finalization of a comprehensive newborn care package for national use. A comprehensive national newborn campaign is being planned.

Strengthening Health Systems: Quality Improvement: implemented in 97 hospitals with 5S-CQI-TQM approach
QA National Steering Committee (MoHFW)
National Quality Improvement Committee (HEU, MoHFW)
National Technical Committee for QA (DGHS)
District QI Committee
Divisional QI Committee
Quality Improvement Team (Facility level)
QI Secretariat (HEU, MoHFW)
Type of Hospitals/Facilities # of facilities
Medical College Hospitals 3 District Hospitals 14 MCWC 3 Upazila Health Complexes 77 Total 97

Policy advocacy through demonstrating innovations for Improved Quality of Newborn Care in SCANU
23
Quality Improvement of services adopting TQM
approach
Competency based training and use of audio-
visual tools for skill development
Paper-based record keeping and reporting to individual case-tracking through web-based MIS

Existing SCANU (17) Planned SCANU (34)
2011-13 2014-15 2015-16 2017-18 Total District
Hospital MCH District
Hospital MCH District
Hospital MCH District
Hospital MCH
SDF (GOB) 10 10
UNICEF 12 4 7 2 4 3 32 JICA 1 01 USAID 3 03 GOB/DPs 5 12 1 18
12 4 18 2 12 3 12 1 64
Strengthening Health Systems: Scaling-up SCANU for full supportive care of sick newborn
30.6 22.2 20.7
0
20
40
CFR
Case Fatality Rate in the SCANU of Tangail District Hospital
2012 2013 2014

Strengthening Health Systems: HMIS: Integrated web-based MIS for all MNCH program Individual case tracking of every newborn through DHIS 2

Strengthening Health Systems: Maternal and perinatal death review for program actions

Scaling-up

National Scaling Up of Helping Babies Breathe Initiatives in Bangladesh
Partnership development and ensure resource
Pilot study, National consensus for scale-up, Policy adoption with High political
commitment
Ensure Logistics
Supervision Monitoring & Evaluation
Incorporation in training curriculums
Training Planning and review Refreshers training
Development of National Scale-up plan, Incorporate into Sector Program and Operation
Plans
National scaling-up of HBB

National preparedness for CHX scale-up
Evidence Generation Dissemination and Advocacy Consensus Building
Policy endorsement Development of national Guideline that includes productione, application, distribution and communication guideline Incorporation in OP with budget allocation
Pilot study Ensure Availability of CHX Partners engagement Development of BCC material and training materials

National Core Committee (NCC) for
newborn health
MOH&FW Systems strengthening
Intensive/pilot im
plementation
Capacity building
Technical assistance
The way we work in partnership
Newborn Technical Working Committee
(NTWC)
Technical Support Groups (TSG)
Technical Support Groups (TSG)
DGHS, DGFP, DPs, NGOs, Professional Agencies, Academia, Research Organizations
As needed As needed
Develop Leadership and policy advocacy
Innovations and research for evidence generation
Attain effective coverage of high impact interventions
Provision of Adequate skilled HR, commodities and technology

• UNICEF, SNL, MaMoni, JICA provides support towards intensive implementation in several districts
• UNICEF, WHO, JICA, GIZ, icddr,b, Mamoni support MoHFW for system strengthening of QI initiatives for MNH
• icddr,b supports evaluation and implementation research and documentation
• NHSDP, UPHCP, BRAC and other NGOs provide newborn care with nationwide coverage through clinic and community networks
• SIAPS provide support to strengthen supply chain management of essential commodities
• SMC and BRAC produces clean delivery kit (planning to include CHX) • Pharmaceuticals has started commercial production of 7.1% CHX
Support from the partners to the MOH&FW

Challenges

17 16 16 22 21 20
26 32
27
50 50 50
0
10
20
30
40
50
60
70
80
90
100
ANC 4 by MTP Delivery by MTP PNC by MTP <2days
BDHS2004 BDHS2007 BDHS2011 Target 2016
Low coverage of skilled care
All Services are increasing gradually , slowest progress in ANC 4

• Demand side: • High home delivery • Low essential newborn care practices • Low utilization
• Supply side: • Low home based service delivery • Primary facilities are not well prepared yet
• Health system: • Inadequate skilled HR for maternal and newborn care • Weaker supervision and monitoring • Newborn indicators are yet to be incorporated at the process level
• Inequity: • Geographic inequity in mortality • Very low effective coverage of interventions • Poor still remains underserved
Challenges

Way forward

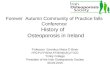
Global mortality targets for 2035 Unless we greatly accelerate newborn survival efforts, goal to end preventable child deaths
by 2035 unreachable
0
10
20
30
40
50
60
70
80
90
100
1990 1995 2000 2005 2010 2015 2020 2025 2030 2035
Mor
talit
y ra
te (p
er 1
,000
live
birt
hs)
2000-2012 AAR = 2.7%
Proposed NMR target 2035: National NMR of 10 (ENAP)
2000-2012 AAR = 3.8% Global U5MR
Global NMR
2035 target: National U5MR of 20
Business as usual: U5MR
AAR = 4.3%
Business as usual: NMR
Scenario 2035 global NMR 2035 neonatal deaths
If current trends are unchanged 13 1.8 million
Every country to NMR of 10 per 1000 7 0.9 million

52 48
42 41 37
32
24
19 15
12
0
5
10
15
20
25
30
35
40
45
50
55
60
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030
Actual NMR and Projections for Bangladesh: 2010 to 2030
Actual NMR (BDHS) Projected NMR

Priority actions • Launch massive, comprehensive campaign to promote newborn
behavior and practices, care seeking and utilization of services
• Focus on quality improvement and ensure adherence to SOPs. Improvement in effective coverage of services
• Strengthen measurement and monitoring of adequacy of inputs, processes and outputs
• Prepare facilities with skilled HR and supplies. Primary level for preventive, screening and follow-up care and, Secondary and tertiary level for full supportive care for sick newborn
• Reduce equity gap to reach the unreached and most vulnerable, marginalized population with differential programming

Thank You