Embed Size (px)
Citation preview
PROBLEMS IN PRESCRIBING READING AIDS FOR PARTIALLY-SIGHTED CHILDREN
LOUISE L. SLOAN AND ADELAIDE HABEL
Baltimore, Maryland
Selection of a reading aid for the partially-sighted child presents a more complex problem than does prescribing for the adult with equally impaired vision because of two important differences in these groups. The first concerns the size of visual detail to be discriminated. Most adults wish to read ordinary newspapers, magazines, and books. The print in school books and in other teaching material used by all children in the lower grades is larger than that in books for adults. Special textbooks in still larger print, in some or in all subjects, are often provided for the partially-sighted. These are occasionally used in the upper as well as in the lower school grades. A second difference in the needs of partially-sighted children and adults is related to the ability of the young child to sustain accommodation for close viewing. The power of the strong convex lens, which permits the adult to read standard print at the distance required by his level of visual impairment, is determined almost entirely by this more or less fixed reading distance because the dioptric power which he can contribute by accommodation is usually a negligible factor. In the young child, on the other hand, a high amplitude of accommodation may reduce or eliminate altogether the need for a strong reading addition or other optical device.
It is well established that the amplitude of accommodation decreases steadily with increasing age. For the eye with normal vision it is generally assumed that one-half to two-
From the Wilmer Institute, Johns Hopkins Hospital, Baltimore, Maryland. This investigation was supported in part by Public Health Service Grant S ROI EY00005 from the National Institute of Neurological Diseases and Blindness, and by a grant from Seeing Eye, Inc., Morristown, New Jersey.
Reprint requests to Louise L. Sloan, Department of Ophthalmology, Wilmer Institute, Johns Hopkins University, School of Medicine, Baltimore, Maryland 21205.
thirds of the individual's maximal amplitude can be sustained without eye fatigue. Some young, partially-sighted children can read monocularly at distance requiring as much as eight diopters of accommodation. It is, however, not safe to make assumptions based on age norms as to the accommodation that can be maintained with comfort by any particular partially-sighted child. This is probably because the stimulus to accommodation, resulting from an out-of-focus retinal image, may not operate efficiently when vision is impaired by ocular disease or anomaly. For this reason the power of the reading addition needed for sustained reading without fatigue may be significantly greater than would be predicted from the child's age.
This study describes the application of systematic test procedures for examination of the partially-sighted school child. These test procedures attempt to determine empirically the power of the reading spectacles or other optical aid needed to provide comfortable reading vision for an adequate period of time.
PROCEDURE
The first step in the examination consists of a precise measure of ability to read continuous text. This test is given at a standard distance of 40 cm (16 inches) with a series of cards graded in M units from IM, the smallest, to 10M, which is 10 times as large. Print in IM size corresponds approximately to the size of normal reading material in newspapers, magazines, and books, including textbooks used in the upper grades of school.* The overall size of the lower case letters of IM print subtends a visual angle of five minutes at a distance of one meter—i.e.,
* Some of the print in standard dictionaries and some of the material in arithmetic texts is slightly smaller than IM print.
1023
1024 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
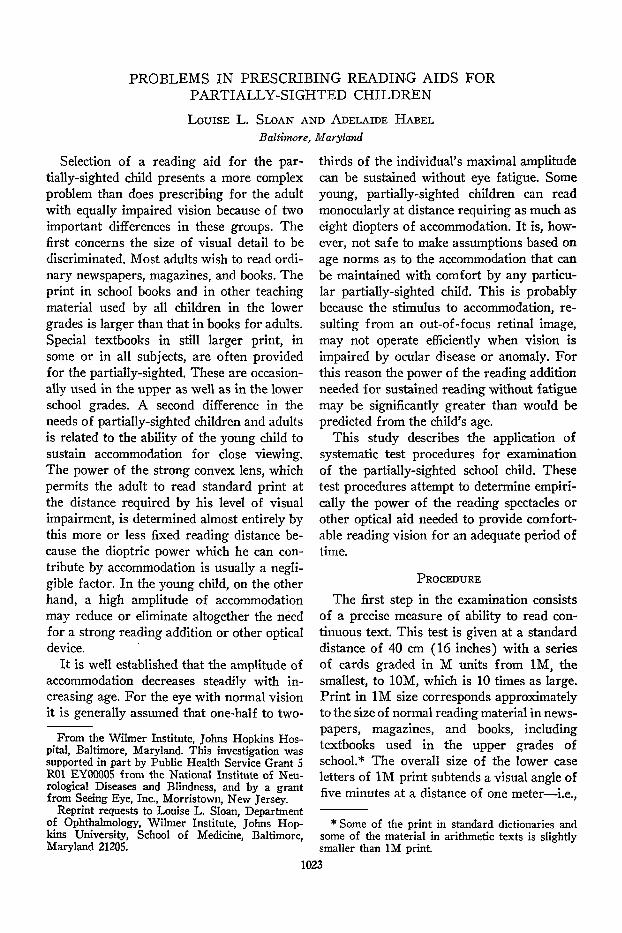
the same angular size as the 20/20 capital letters of an acuity chart viewed from 20 feet. At 40 cm its Snellen notation is 40/100 (or 20/50 equivalent) because the testing distance is 40 cm and the distance at which the letters subtend a five-minute visual angle is 100 cm. Since 2M print is twice as large, it has a Snellen notation of 40/200. Figure 1 shows the test cards composed of third-grade reading material. Similar cards, providing longer samples of text in each size, may be used for older children. They have been de
scribed and illustrated in a previous publication1 which also explains in detail the M unit and its use in rating degrees of visual impairment.
We have shown in this study that ability to read continuous text cannot be predicted accurately from measurements of acuity made with isolated capital letters. Direct measures of the size of print required for easy reading provide a far more valid and useful measure of visual impairment. For these reading tests at 40 cm, the patient
Fig. 1 (Sloan and Habel). Reading material in graded sizes composed of words at a third-grade level. The smallest size read with ease at 40 cm (16 inches) determines the distance required to read print of any other desired size.

VOL. 75, NO. 6 READING AIDS 102S
wears whatever glasses he requires to obtain maximal clarity of the print. Children, unless aphakic, can usually be tested with their best distance correction because they are able to accommodate the required 2.50 diopters. However, because of the somewhat unpredictable nature of the accommodative response in patients with subnormal vision, our standard procedure includes check tests with additional convex spheres to see if any addition to the distance correction will improve acuity at 40 cm. The aphakic child will, of course, require the full 2.50 diopter addition for the 40 cm distance.
It is possible to predict from tests made at 40 cm with these reading cards the closer viewing distance needed to read any particular size of smaller print. As an example, consider the cases of three children with different degrees of visual impairment who read with ease 2M, 4M, and 10M print, respectively, at the standard distance of 40 cm. To obtain equivalent magnifications of the retinal image of IM print, it must be held at 20, 10, and 4 cm, respectively. If the same three children use only large-print books (print that is equivalent to about 2M in size), the required viewing distances can be doubled and are respectively 40, 20, and 8 cm. The test cards therefore provide the information necessary to calculate the viewing distance required for any given reading material if its approximate size in M units is known.
In the case of children with varying amounts of accommodative power, there still remains the more complex problem of determining what strength of optical aid is needed, if any, to permit sustained comfortable reading with the better eye at the close distance indicated by the results of the reading test at 40 cm. The special situations in which a binocular correction should be tried are considered later in this paper.
To obtain an estimate of the maximal dioptric power which will be accepted, usually in the form of a spectacle correction, to read at the required distance, we use a combination of two different tests. Both of them are
merely methods of choosing the best reading addition for print viewed at a predetermined near location. An important feature of the test procedure is that the child himself should hold the reading material. It has been our experience that more accommodation is stimulated by the normal situation in which there are kinesthetic cues as to the distance of the reading page. This observation is further evidence that in the partially-sighted individual out-of-focus blurring of the retinal image may be a much less effective stimulus to accommodation that it is in the normal eye.
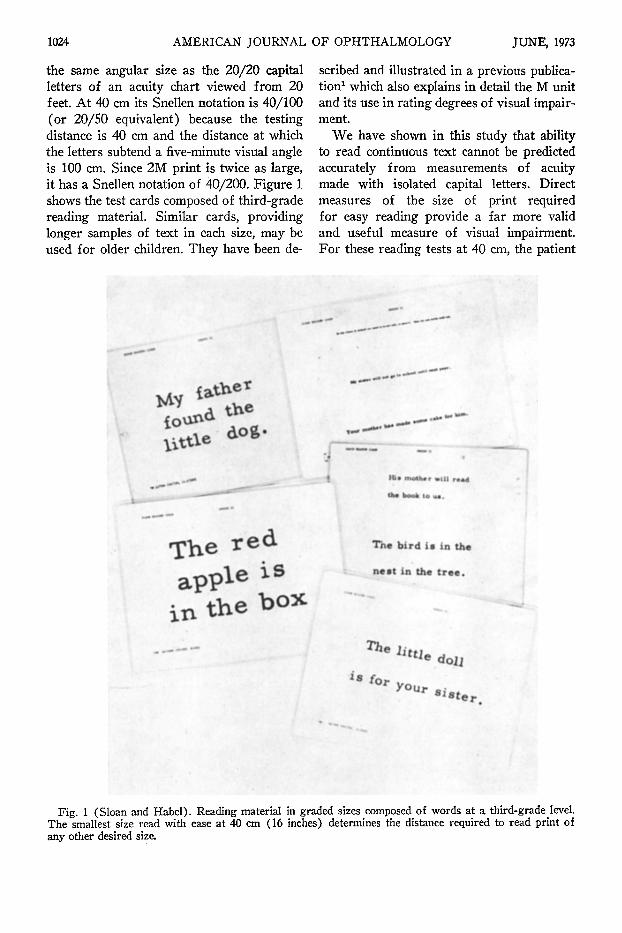
Figure 2 shows the simple equipment we use to present reading material of the desired size and at the desired fixed distance under conditions such that the user gets the proper kinesthetic cues as to its distance. The spherical power before the eye is varied to find the greatest and the least amount that will be accepted without noticeable blurring of the print. We find it best to start with the maximal power in the trial frame, corresponding to zero accommodation, and decrease this by steps of one diopter. The lens tree (Fig. 2) has a series of 4 minus spheres varying in steps of one diopter and provides a convenient and rapid means of reducing the power of the reading addition. The maximal dioptric power indicated by this test is then checked by letting the child read with this correction while holding a book in print of the desired size. If he holds the book significantly closer than the predetermined required distance, a reduction in power of the reading addition may be advisable. These brief tests in the Low Vision Clinic do not, however, insure that the child will not experience eye fatigue when he uses the selected reading addition for long periods of time. When feasible, it is helpful to prescribe inexpensive Selsi jeweller's loupes2 in at least two different suitably chosen powers for home trial so that the patient can select the one which allows him to read comfortably and efficiently for an adequate period of time. Since the weakest Selsi loupe has a
1026 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
Fig. 2 (Sloan and Habel). Equipment for measuring the dioptric power of the reading addition needed to read at the specific distance required by the degree of visual impairment. Kinesthetic cues help to stabilize accommodation for this distance. The lens tree, L, shown in the photograph, provides a convenient means of making rapid changes in spherical power, in order to determine the most satisfactory reading addition.
power of eight diopters, other methods of providing temporary reading glasses of lesser power are sometimes necessary. The Halberg clip to hold trial-case lenses, Magna-add bifocal clip-ons, and Fresnel press-on lenses are some of the possible ways of providing temporary reading aids for home trial.
As a rule children adapt well to reading aids in spectacle form. Maintenance of the proper distance from book to lens is less a problem than for the older patient because of the child's better motor control and because he can change his accommodation to focus for unavoidable changes in object-to-lens distance. When a reading addition of more than about 20 diopters is required, however, children as well as adults may prefer a fo-cusable stand magnifier which maintains the reading page at the desired distance and permits the use of an attached illuminating device.3 Fixed-focus stand magnifiers in lower powers, which require 2.5 diopters of accommodation, are convenient for preliminary
home trial by those who have been reading without any optical aid. If such a device is found to reduce eye fatigue, it suggests the need for a spectacle reading addition to decrease the demand on accommodation. Data reported elsewhere2 provide the information necessary to choose spectacle reading aids equivalent in power to the various stand magnifiers.
TYPICAL RESULTS
MONOCULAR READING AIDS
The subjects tested were children attending regular school (including "sight saving" classes) who had already learned to read continuous text at a third-grade level or better. They were referred to our Low Vision Clinic by their ophthalmologists for recommendation as to whether or not some form of optical reading aid was needed. Whenever possible, after the first examination, re-evaluations were made at intervals of a year or more to test for changes in the required reading aid resulting from (1) decreased
VOL. 75, NO. 6 READING AIDS 1027
ability to sustain accommodation, (2) decrease in the size of print in the books read at school or at home, (3) a significant increase or decrease in the degree of visual impairment because of progression of the eye disease or because of surgical or medical therapy.
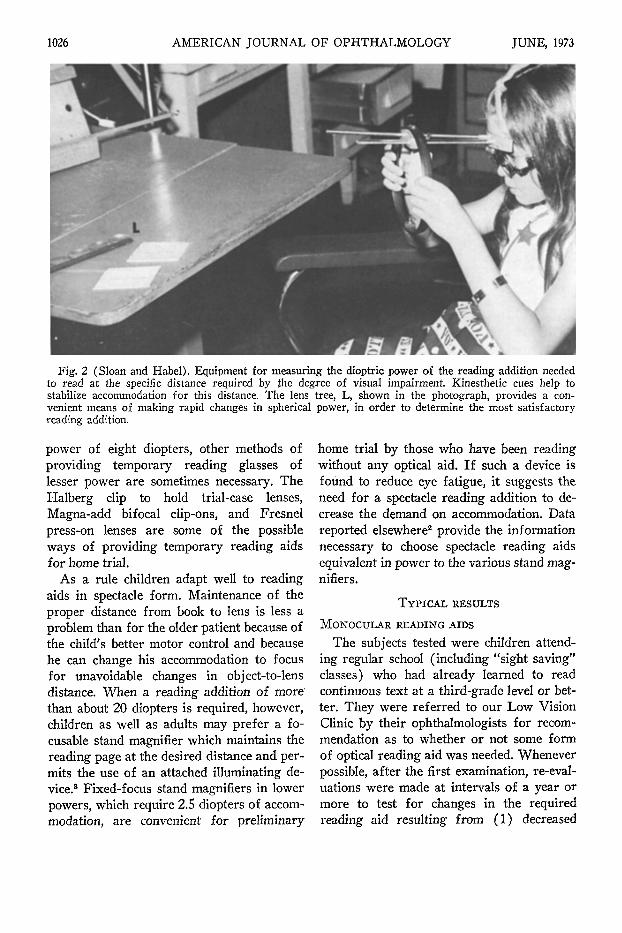
Table 1 summarizes data for 11 children followed for two to seven years to illustrate the several factors which may result in
changes in the required power of the reading aid. From the data of columns 4 and 5 it is possible to calculate the approximate distance at which this print must be held to be read with ease. These estimates are listed in column 6. Column 7 gives the dioptric power of the prescribed reading addition, column 8 the additional power which must be supplied by accommodation to read at the distance listed in column 6.
TABLE 1 PATIENTS GIVEN MONOCULAR READING AIDS
Case No. and Diagnosis
Age (in years)
Corrected Acuity
M Rating
(at 40 cm)
Required Print Size (M units)
Computed Reading Distance (in cm)
Accommodation Required
(in diopters)
1. Congenital glaucoma
2. Retrolental fibroplasia
3. Toxoplasmosis
4. Retrolental fibroplasia
5. Retrolental fibroplasia
6. Optic atrophy
7. Retrolental fibroplasia
8. Retrolental fibroplasia
9. Post-traumatic optic atrophy
10. Cataracts
11. Albinism and nystagmus
IS 17.S 18.5 19.S
IS 17 21 22
10 là
8 9
10 12 15
12 14
12 12 14
8 11 IS
7 13
8 11 13 14 14.5
15 16 17
10 15
16/200 20/200*
15/100*
8/100*
20/200*
16/200 20/200
10/200 10/200 14/200
8/200 9/200 6/200
15/200 20/200
5/200 6/200 8/200 8/200 7/200
20/70 15/100 20/60
13/200 13/100
4 M *
4 M *
5 M *
2 M *
4 M *
7 M *
10M*
S M 10M
14M 14M 14M 14M 20M (uses focusable stand magnifier)
3 M ■ 4M 2.5M (using mydriatic)
5 M 4 M
I M *
I M *
I M *
0.6M*(for small detail in arithmetic book)
1.5M I M
l .SM I M I M
I M I M
0.9M(for dictionary)
l .SM I M
2 M 2 M
1.5 1 1.25M
I M *
I M *
10*
10*
8*
12*
15 10
8 . 6 5 . 7 S.7
4 4
3 . 6
12 4
5 .7 S .7 4 . 3 4 . 3 2 . 5
13 10 16
8 10
5.50 5.50
8 8
5 S 7 7
9 12
3 4 6 8 8
4 10
0 7
19
19 23 28
0(RE) 24.5
11 13 20 22 44
4.25 9 5 .5
16 11
4.SO 4.SO
2 2
S S 3 3
3.S 0.5
5 . 3 4 . 3 2 . 3 0 . 3 0 . 3
2 . 7 0
11 11.S 0
6 2 0
8 . 3 0 . 5
6 . 5 4.S 3 . 0 1.0
0
3.75 1.0 0.7S
0 0
* Unchanged.
Reading Addition
(prescribed diopters)
1028 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
In Cases 1-4 there was no change in the M rating or in the size of print to be read during the period that these patients were followed. In Case 4, because of the small detail in his arithmetic book, the required reading distance was computed from an estimated print size of 0.6M instead of the IM usually taken as representative of normal print. In later examinations, all four patients showed an increase in the dioptric power of the spectacle preferred for comfortable reading and consequently a decrease in the required diopters of accommodation. In Cases 5 to 9 decrease in size of print to be read is a second factor responsible for the increase in the power of the reading addition. In three cases this was a change from large print to normal IM print. In Case 7 the need to see somewhat smaller print in the dictionary was in part responsible for an increase in the power of the reading addition at the age of 15 years. In Cases 8 and 9 a third factor contributing to the increase in the reading addition with increasing age was a progressive impairment of vision, demonstrated by an increase in size of print required for easy reading at 40 cm. In Case 10, at the time of the second examination, this child with congenital cataracts showed a slightly greater impairment of reading vision. One year later a significant improvement was noted, resulting from the routine use of a mydriatic. This permitted a decrease in the power of the preferred reading addition from 9 to 5.5 diopters. In Case 11 the improvement in reading ability from 5M to 4M is probably explained by the reduction in nystagmus. It permitted a decrease in the preferred reading addition from 16 to 11 diopters.
These case histories illustrate the several factors which must be considered in prescribing for the partially-sighted child and emphasize the need for re-evaluation as soon as there is any evidence that the reading aid in use is no longer adequate to meet the child's needs. It may be seen from Table 1 that in successive examinations at intervals of one year or more all 11 children showed a
decrease in the amount of accommodation they preferred to maintain when reading at the required distance. At the time of the last examination, when their ages ranged from 13 to 17 years, nine of the 11 accepted a reading addition which permitted them to use less than one diopter of accommodation. There is, however, no reason to suppose that these children have any true physiologic impairment of accommodation. Their preference for high reading additions is, we believe, because the visual cues which provide precise control of the accommodative response in normal vision may function less efficiently when acuity is reduced by factors other than optical blurring. It should be remembered also that the children in this study represent a selected group, referred because they were experiencing eye fatigue or other visual difficulties. The reading aids prescribed were selected after home trial whenever possible and were close to the maximum power which was accepted for sustained comfortable reading at the distance required by the degree of visual impairment.
It may be argued that the minimal acceptable addition should be prescribed in order to make the child strengthen his own power of accommodation. If, however, some degree of supplementary assistance to accommodation in the form of reading glasses or bifocals is necessary, there are valid arguments for prescribing as much power as the patient will accept. This minimizes the likelihood of eye fatigue and prolongs the time before an increase in power will be needed. It must be emphasized, however that these considerations apply only to corrections for monocular reading with the better eye. The situation may be quite different in binocular corrections for a close reading distance where) the excessive demands on convergence are more likely to be a cause of eye fatigue than excessive accommodation.
READING AIDS FOR APHAKIC CHILDREN
In the case of the aphakic child, selection of the most satisfactory power for the read-
VOL. 75, NO. 6 READING AIDS 1029
ing addition is simplified by the fact that accommodation is not a factor. It can be predicted precisely when the required reading distance has been computed from the size of print in M units read at 40 cm and the size to be read.
Consideration must also be given to the possible need for a weaker addition, of 2.50 diopters for example, for other viewing tasks at an intermediate distance. Because of the larger detail and less critical nature of such tasks, the distance correction is often adequate. When it is not, a possible solution is to prescribe a stand magnifier of the type designed for use with a 2.5D near addition for reading. The available devices have a wide range of powers equivalent to spectacle reading additions ranging from 4.50 to 17.50 diopters and are therefore suitable for patients with visual impairments from 2M to 7M who wish to read IM print. Typical stand readers of this type are the well-known Coil Plasta Cataract and Hi-Power Plasta Stand Magnifiers. Complete specifications and sources of supply for a number of these fixed-focus stand readers have been published elsewhere.2
BINOCULAR READING AIDS
In a small number of partially-sighted patients a binocular reading addition may be preferable to correction of only one eye. There are three classes of patients for whom we found it advisable to try a binocular reading correction : ( 1 ) The first group are those able to obtain binocular single vision and some degree of depth perception without excessive demands on either accommodation or convergence. (2) The second group includes patients with congenital nystagmus, often in association with albinism. Binocular reading glasses were prescribed if nystagmus was decreased and reading was therefore improved when both eyes were corrected. This occurred even though tests for binocular vision usually revealed either a tropia or a central suppression of one eye. The decrease in nystagmus in binocular vision was some
times obvious to inspection by watching the better eye as the other was intermittently occluded. It was usually possible to show that reading ability, as indicated by the M rating measured at 40 cm, was better with binocular vision than with the better eye alone. (3) A third group used alternate fixation when reading with both eyes. They were given binocular corrections when there was evidence that they read more comfortably or more rapidly or could read smaller print with a binocular than with a monocular correction. As we shall show later, partial non-overlapping of ceco-central scotomas was shown in several cases to be responsible for the advantage of alternate use of the two eyes.
Tests for binocular vision-—Several procedures were used to see whether a given reading addition provided single binocular vision. A simple bar reading test may, for example, detect either a tropia or a suppression of the image of one eye. The Titmus Polaroid test of depth perception in near vision can also provide helpful information. Its circle and animal targets were viewed by the patient at the close distance he required to read ordinary print. The parallactic angles are therefore greater than those listed on the score card for a standard testing distance of 16 inches. Consistent evidence of at least gross depth perception, as indicated by correct answers to at least two of the circle or animal targets, can be taken as evidence of true binocular vision without either suppression or tropia. Failure to perceive depth on this test does not, however, eliminate the possibility of binocular single vision since some normally sighted individuals have difficulty in perceiving the simulated depth provided by the disparate images of stereoscopic test targets.4 If the Titmus depth test is failed, additional information as to the status of binocular vision at the reading distance can be obtained from a vectograph slide (Catalogue No. 11243, American Optical Co., intended for use at distance in their Project-O-Chart). This slide can be viewed directly against a white background at the
1030 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
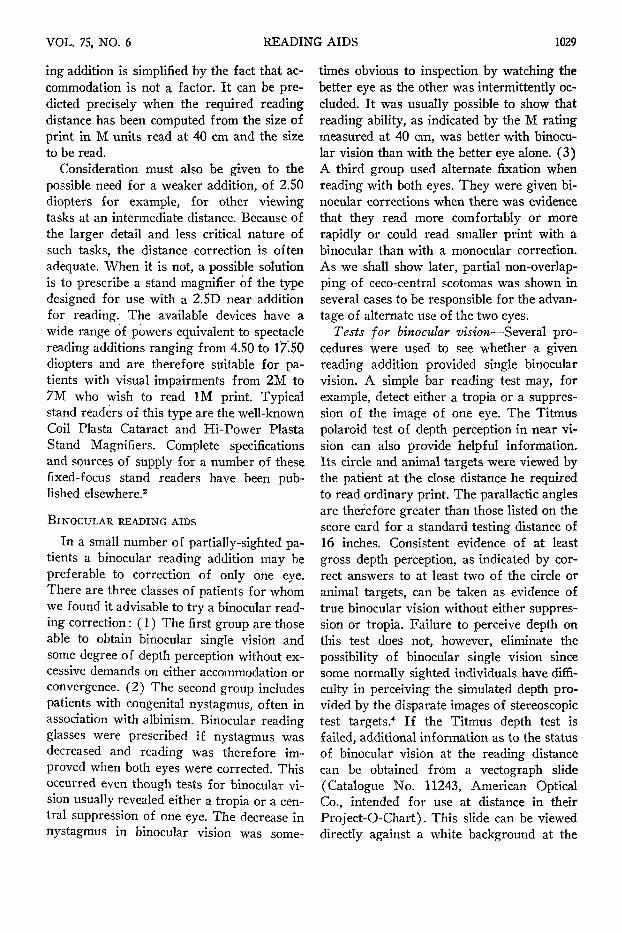
reading distance normally used by the partially-sighted patient. Figure 3 shows the test material seen through polaroid spectacles by each eye alone, and that seen by both eyes when there is normal binocular vision. The radiating line target, marked A in the figure, indicates gross suppression if either the left or the right fan is not seen. Gross suppression is also detected by test B if the letters on one side of the vertical line are not seen. A more delicate test for foveal suppression is provided by the letter test marked C in the figure. Tropias are indicated on Test E by a separation of the right and left eye targets so that they do not form a cross. Test D is similar except that the absence of the fusion stimulus provided by the circle makes it a test for phoria rather than for tropia. In Test F, one of the circles in each row appears closer than the others if there is stereoscopic depth perception.
READING AIDS TO PROVIDE BINOCULAR SINGLE VISION
Selection of the dioptric power of a binocular reading addition and determination of the inward decentration required to provide base-in prism of suitable strength is not a simple procedure and may require extensive experimentation to arrive at a satisfactory prescription. In a binocular spectacle correction, it is desirable to keep the spherical power of the reading addition as low as possible so that the accommodation exerted by the patient will assist him in converging for the close reading distance required by his impaired vision. Inward decentration of the optical centers of the bifocal segments can provide some base-in prism and so reduce the demand on convergence. Fonda5 uses a simple rule which requires a decentration of each reading segment of 1 mm per diopter.
Application of this formula provides a convenient starting point, but compensates for only a part of the convergence required for reading at a close distance6 and takes no account of individual differences in lateral phoria and in amplitude of fusion.
Experimental tests of the effect of various decentrations of the bifocal segments are not easy to duplicate with lenses in a trial frame. If the patient has adequate spectacles for distance, Halberg clips holding spheres from the trial case provide a means of varying the distance between the ocular centers of the reading additions. We have also used decen-tered Fresnel lenses mounted in trial case rings to test the effect of various amounts of dencentration on the patient's ability to achieve binocular vision. These Fresnel paste-on lenses can also be prescribed as temporary reading additions for home trial. We have, however, seldom found them acceptable as a permanent correction because of the loss of contrast resulting from scattered light.
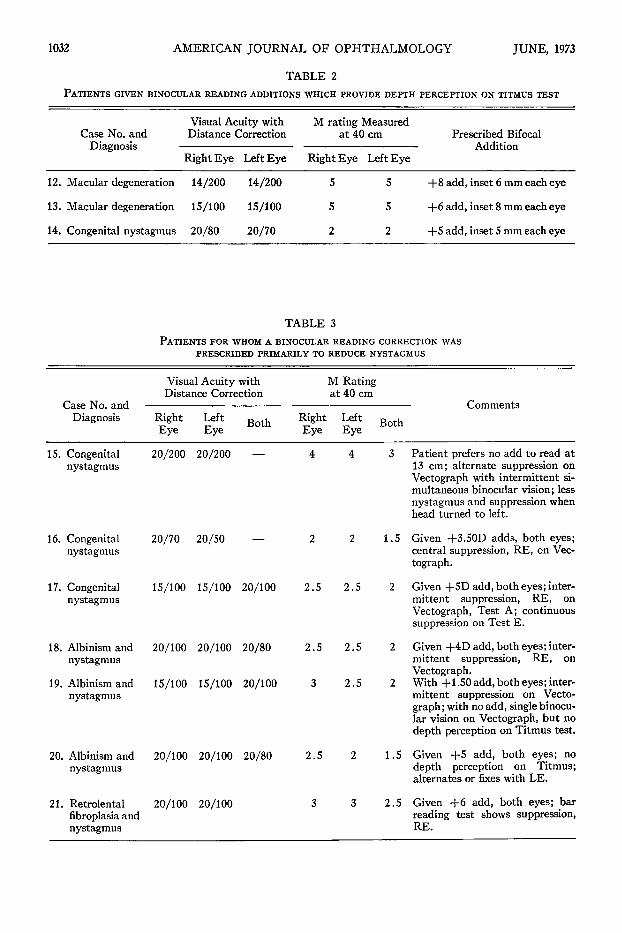
Table 2 gives illustrative data for three patients who, with the bifocals prescribed, were able to get depth perception on the Tit-mus Test.
BINOCULAR READING AIDS PRESCRIBED PRIMARILY TO REDUCE NYSTAGMUS
Table 3 summarizes the findings for seven patients with congenital nystagmus. In three, it was associated with albinism and in one with retrolental fibroplasia. In every case the reading vision, tested at 40 cm with M cards, was slightly better when measured binocu-larly than with either eye alone. The binocular reading aids prescribed did not, however, provide sustained binocular vision and depth perception in this group of patients. In Case 15, this child preferred no reading addition
it/1) f
Fig. 3 (Sloan and Habel). Vectograph slide (American Optical Co.) used to test for suppression or tropia at the near reading distance required by the level of visual impairment. The test material presented to the left and right eyes respectively, when viewed through polaroid glasses, is shown at the left and right. The middle chart shows the combined images as seen in normal binocular vision.
1032 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
TABLE 2 PATIENTS GIVEN BINOCULAR READING ADDITIONS WHICH PROVIDE DEPTH PERCEPTION ON TITMUS TEST
12.
13.
14.
Case No. and Diagnosis
Macular degeneration
Macular degeneration
Congenital nystagmus
Visual Acuity with Distance Correction
Right Eye
14/200
15/100
20/80
Left Eye
14/200
15/100
20/70
M rating Measured at 40 cm
Right Eye
5
5
2
Left Eye
5
5
2
Prescribed Bifocal Addition
+8 add, inset 6 mm each eye
+ 6 add, inset 8 mm each eye
+5 add, inset 5 mm each eye
TABLE 3 PATIENTS FOR WHOM A BINOCULAR READING CORRECTION WAS
PRESCRIBED PRIMARILY TO REDUCE NYSTAGMUS
Visual Acuity with Distance Correction
M Rating at 40 cm
Case No. and Diagnosis Right Left
Eye Eye Both Right Left B o t h Eye Eye
Comments
15. Congenital nystagmus
20/200 20/200
16. Congenital 20/70 20/50 nystagmus
17. Congenital 15/100 15/100 20/100 nystagmus
18. Albinism and 20/100 20/100 20/80 nystagmus
19. Albinism and 15/100 15/100 20/100 nystagmus
20. Albinism and 20/100 20/100 20/80 nystagmus
21. Retrolental 20/100 20/100 fibroplasia and nystagmus
2.5 2.5
2.5 2.5
3 2.5
2.5 2
3 Patient prefers no add to read at 13 cm; alternate suppression on Vectograph with intermittent simultaneous binocular vision; less nystagmus and suppression when head turned to left.
1.5 Given +3.50D adds, both eyes; central suppression, RE, on Vectograph.
2 Given +5D add, both eyes; intermittent suppression, RE, on Vectograph, Test A; continuous suppression on Test E.
2 Given +4D add, both eyes; intermittent suppression, RE, on Vectograph.
2 With +1.50 add, both eyes; intermittent suppression on Vectograph; with no add, single binocular vision on Vectograph, but no depth perception on Titmus test.
1.5 Given +5 add, both eyes; no depth perception on Titmus; alternates or fixes with LE.
2.5 Given +6 add, both eyes; bar reading test shows suppression, RE.
4 4
2 2
3 3
VOL. 75, NO. 6 READING AIDS 1033
and could read small print at a distance of 13 cm. There was alternate suppression in the primary position. There was less nystagmus and suppression when she turned her head to the left. In Case 19, this child was able to read at 20 cm without any reading addition and showed single binocular vision but no depth perception on the Titmus test. The other five patients showed intermittent or continuous suppression of one eye. All seven, however, preferred a binocular reading addition to a correction for one eye only. This is probably accounted for by a reduction in nystagmus when both eyes were corrected for near vision.
BINOCULAR READING AIDS FOR PATIENTS WHO USE ALTERNATE FIXATION.
Three children who preferred a binocular to a monocular reading correction used alternate fixation. They read the left half of the page with the right eye and shifted to the left
eye to read the right half. We have examined more extensively three adults with a similar preference for alternate fixation. Studies of the central visual fields of two of these adults helped to explain the advantages of alternate fixation.
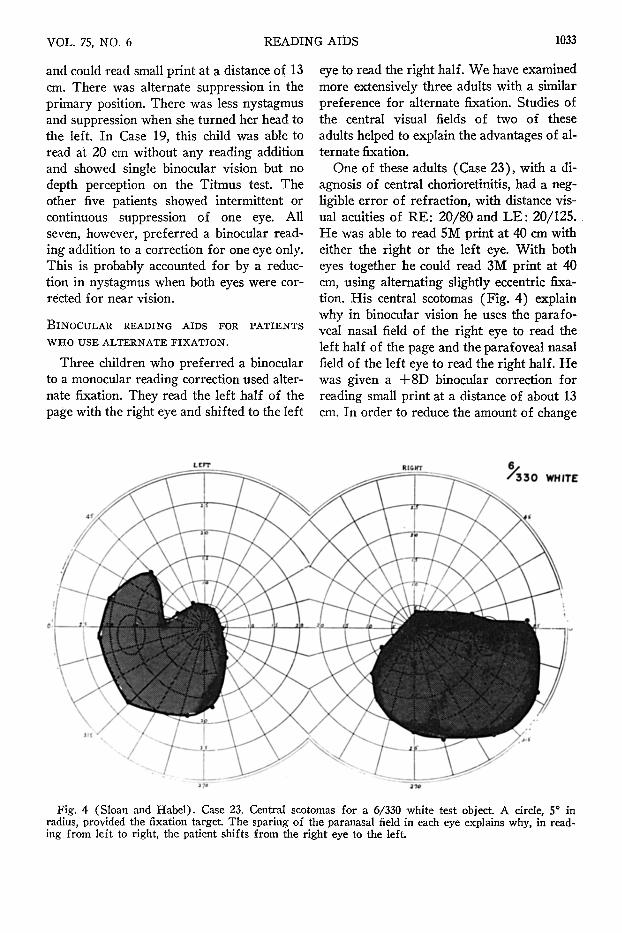
One of these adults (Case 23), with a diagnosis of central chorioretinitis, had a negligible error of refraction, with distance visual acuities of RE: 20/80 and L E : 20/125. He was able to read 5M print at 40 cm with either the right or the left eye. With both eyes together he could read 3M print at 40 cm, using alternating slightly eccentric fixation. His central scotomas (Fig. 4) explain why in binocular vision he uses the parafo-veal nasal field of the right eye to read the left half of the page and the parafoveal nasal field of the left eye to read the right half. He was given a + 8 D binocular correction for reading small print at a distance of about 13 cm. In order to reduce the amount of change
Fig. 4 (Sloan and Habel). Case 23. Central scotomas for a 6/330 white test object. A circle, 5° in radius, provided the fixation target. The sparing of the paranasal field in each eye explains why, in reading from left to right, the patient shifts from the right eye to the left.
1034 AMERICAN JOURNAL OF OPHTHALMOLOGY JUNE, 1973
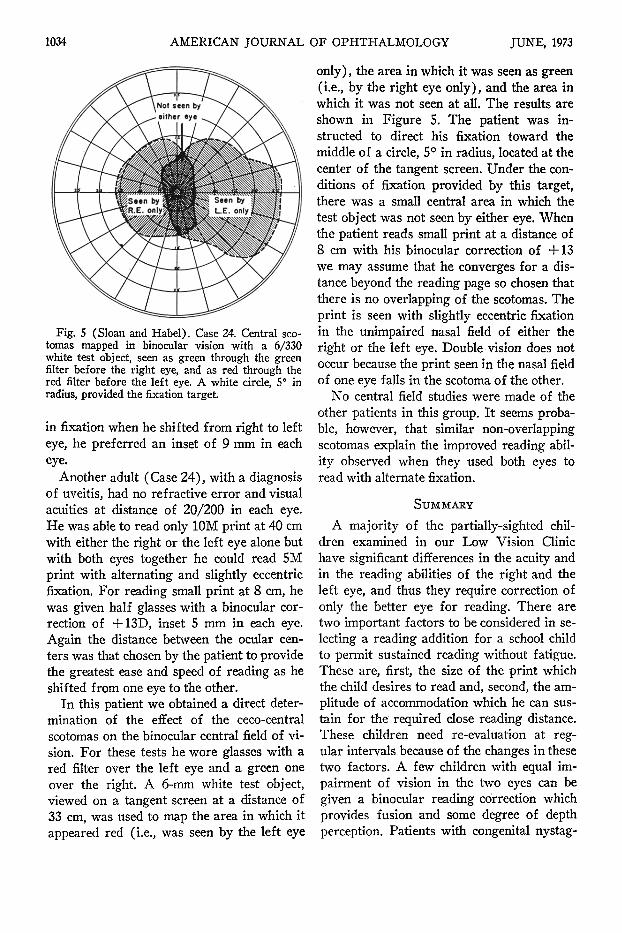
Fig. 5 (Sloan and Habel). Case 24. Central sco-tomas mapped in binocular vision with a 6/330 white test object, seen as green through the green filter before the right eye, and as red through the red filter before the left eye. A white circle, 5° in radius, provided the fixation target.
in fixation when he shifted from right to left eye, he preferred an inset of 9 mm in each eye.
Another adult (Case 24), with a diagnosis of uveitis, had no refractive error and visual acuities at distance of 20/200 in each eye. He was able to read only 10M print at 40 cm with either the right or the left eye alone but with both eyes together he could read 5M print with alternating and slightly eccentric fixation. For reading small print at 8 cm, he was given half glasses with a binocular correction of +13D, inset 5 mm in each eye. Again the distance between the ocular centers was that chosen by the patient to provide the greatest ease and speed of reading as he shifted from one eye to the other.
In this patient we obtained a direct determination of the effect of the ceco-central scotomas on the binocular central field of vision. For these tests he wore glasses with a red filter over the left eye and a green one over the right. A 6-mm white test object, viewed on a tangent screen at a distance of 33 cm, was used to map the area in which it appeared red (i.e., was seen by the left eye
only), the area in which it was seen as green (i.e., by the right eye only), and the area in which it was not seen at all. The results are shown in Figure 5. The patient was instructed to direct his fixation toward the middle of a circle, 5° in radius, located at the center of the tangent screen. Under the conditions of fixation provided by this target, there was a small central area in which the test object was not seen by either eye. When the patient reads small print at a distance of 8 cm with his binocular correction of +13 we may assume that he converges for a distance beyond the reading page so chosen that there is no overlapping of the scotomas. The print is seen with slightly eccentric fixation in the unimpaired nasal field of either the right or the left eye. Double vision does not occur because the print seen in the nasal field of one eye falls in the scotoma of the other.
No central field studies were made of the other patients in this group. It seems probable, however, that similar non-overlapping scotomas explain the improved reading ability observed when they used both eyes to read with alternate fixation.
SUMMARY
A majority of the partially-sighted children examined in our Low Vision Clinic have significant differences in the acuity and in the reading abilities of the right and the left eye, and thus they require correction of only the better eye for reading. There are two important factors to be considered in selecting a reading addition for a school child to permit sustained reading without fatigue. These are, first, the size of the print which the child desires to read and, second, the amplitude of accommodation which he can sustain for the required close reading distance. These children need re-evaluation at regular intervals because of the changes in these two factors. A few children with equal impairment of vision in the two eyes can be given a binocular reading correction which provides fusion and some degree of depth perception. Patients with congenital nystag-
VOL. 75, NO. 6 READING AIDS 103S
mus also benefit from a binocular reading correction even though there is central suppression of one eye. There is usually a significant reduction in the nystagmus and improvement in reading vision when the same near reading addition is given to both eyes. A third small group who prefer a binocular correction use alternate fixation in reading, because their central scotomas are partially non-overlapping.
REFERENCES
1. Sloan, L. L., and Brown, D. J. : Reading cards for the selection of optical aids for the partially
sighted. Am. J. Ophth. 55:1187, 1963. 2. Sloan, L. L : Recommended Aids for the Par
tially Sighted, 2nd ed. New York, National Society for the Prevention of Blindness, 1971 (Cat. No. P40S).
3. : New f ocusable stand magnifiers. Am. J. Ophth. 58:604, 1964.
4. Sloan, L. L., and Altaian, A. : Factors involved in several tests of binocular depth perception. Arch. Ophth. 52:524, 1954.
5. Fonda, G. : Management of the Patient with Subnormal Vision, 2nd ed. St. Louis, C. V. Mosby, 1970.
6. Sloan, L. L.: Recommended Aids for the Partially Sighted, 2nd ed. New York, National Society for Prevention of Blindness, 1971 (Cat. No. P405), p. 60.
OPHTHALMIC MINIATURE
Piggy shook his head and came to the pile. "My ! you've made a big heap, haven't you ?" Jack pointed suddenly. "His specs—use them as burning glasses !" Piggy was surrounded be
fore he could back away. "Here! Let me go!" His voice rose to a shriek of terror as Jack
snatched the glasses off his face. "Mind out ! Give 'em back ! I can hardly see !"
Ralph elbowed him to one side and knelt by the pile . . . Ralph moved the lenses back and forth, this way and that, till a glossy white image of the declining sun lay on a piece of rotten wood . . . a tiny flame appeared.
"My specs !" howled Piggy. "Give me my specs !" Ralph stood away from the pile and put the glasses into Piggy's groping hands. His voice subsided to a mutter.
"Jus' blurs, that's all. Hardly see my hand. . . ." William Golding Lord of the Flies
Faber, 1954





























