Embed Size (px)
Citation preview

Jnt. J. Oral Surg. 1981: 10: 81-86
(Key words: osteotomy, sagil/al split; surgery, orthogna/hie; mandible, prognuthic; prognathism)
Problems encounteredin the sagittal split operation
WILLIAM SIMPSON
Department of Oral Surgery, University Hospital of South Manchester,Manchester, England
ABSTRACT - The sagittal split mandibular osteotomy is a technicallydifficult operation. This article discusses some of the problems encountered in a series of over 100 cases and describes the instrumentation developed over the years to help overcome the technical difficulties.
(Received for publication 25 August, accepted 15 September 1980;
A great deal has been written about thesagittal split mandibular osteotomy over thelast 20 years, particularly with regard to thelong term results achieved by this operationfor treatment of both the prognathic andretrognathic mandible. It is now generallyaccepted as a standard procedure in theoral surgeon's repertoire, but it is agreedthat technically it is a difficult operation.
It is proposed to discuss the technicalproblems encountered with this operationover the last 10 years and to show some ofthe instrumentation developed to overcomethese technical difficulties, in over 100sagittal split operations for both the prognathic and retrognathic mandible. Thethree main areas to be discussed are asfollows:
1. Access and illumination.2. The bone cuts ancI bone split.3. The position of the mandibular frag
ments following the split.
Access to the ascending ramus is difficultand certainly where there is any trismuspresent it is preferable to use some othertechnique. However, in a patient with reasonable mandibular movement in which theoperation is to be used, it is preferable toget the maximum access possible bp stripping masseter completely from the buccalaspect of the ascending ramus and most ofthe insertion of temporalis from the coronoid process.
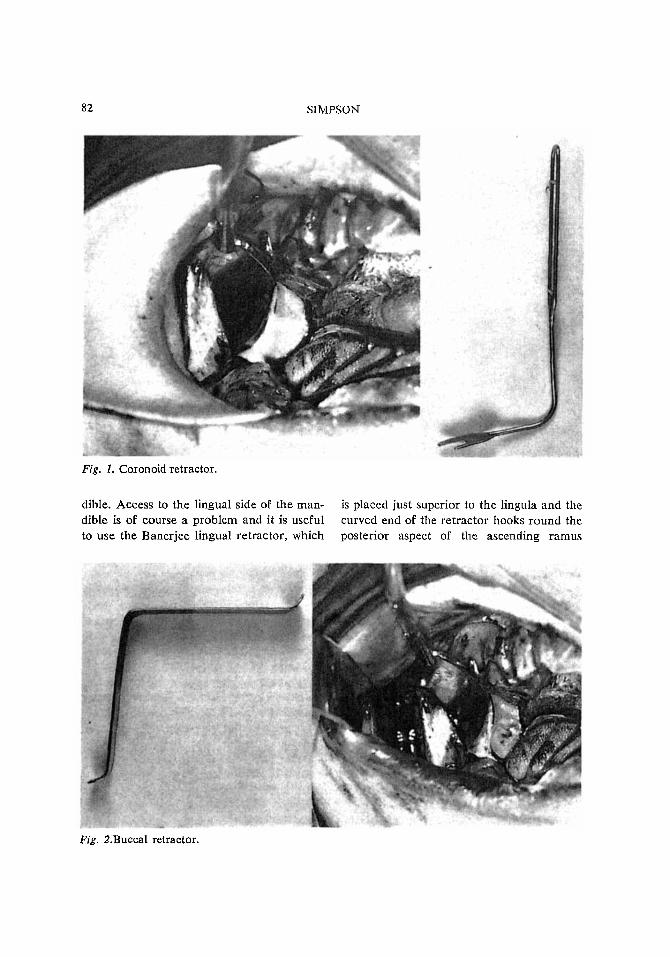
With extreme stripping of the temporalisit is difficult to retract the sof,t tissue fromthe superior aspect of the operative fieldand the coronoid retractor (Fig. 1) hasbeen found useful to retract these tissuesinclUding the buccal pad of fat. Fig. 2shows a buccal retractor which is extremelyuseful both to expose the buccal aspect ofthe mandible and to protect the soft tissueswhen the buccal cut is being made eitherat the angle or the lower border of man-
0300-9785/81/020081-06$02.50/0 @ 1981 Munksgaard, Copenhagen
82 SIMPSON
Fig. 1. Coronoid retractor.
dible. Access to the lingual side of the mandible is of course a problem and it is usefulto use the Banerjee lingual retractor, which
is placed just superior to the lingula and thecurved end of the retractor hooks round theposterior aspect of the ascending ramus
Fig. 2.Buccal retractor.

PROBLEMS IN SAGITIAL SPLIT 83
Fig. 3. Lingual retractor.
(Fig. 3). The operator again has some protection of the soft tissues when the lingualcut is being made. This retractor is ofcourse somewhat similar to other lingualretractors but offers the operator greaterprotection.
Lighting is also a major problem, particularly on the lingual side of the mandibleand to overcome this problem a fibre lightattachment to the Banerjee lingual retractor was devised which gives much improved
Fig. 4. Fibre light attachments.
illumination on the lingual side of themandible. The fibre light stem can be inserted either before or after the lingualretractor has been placed in position. A setof instruments with fibre light attachmentshas been available on a commercial basisfor some time (Fig. 4) (SIMPSON & STAN
LEy6).
Having achieved adequate retraction andillumination the standard bone cuts aremade with a Hall air drill, using a Meissinger surgical bur for the lingual cut.While it is preferable to take the lingualcut back to the posterior border of themandible, there are a number of caseswhere this is difficult because of the severepost lingular depression. The concavity canbe so great and the ascending ramus sothin in this region that the lingual cut mayhave to stop at the lingula as suggested byDAL PoNTi! and HUNSUCK4. An assessmentof the width of the ascending ramus shouldbe made pre-operatively and usually a submenta vertical view of the ascending ramiis sufficient although a tomographic examination of the ascending rami has beensuggested by some authorities. However, areview of a number of cases where it wasonly possible to finish the lingual cut at thelingula, showed that the split in the majority of these cases dips down below the post
Fig. 5. Bone splits following short lingual cuts.
84 SIMPSON
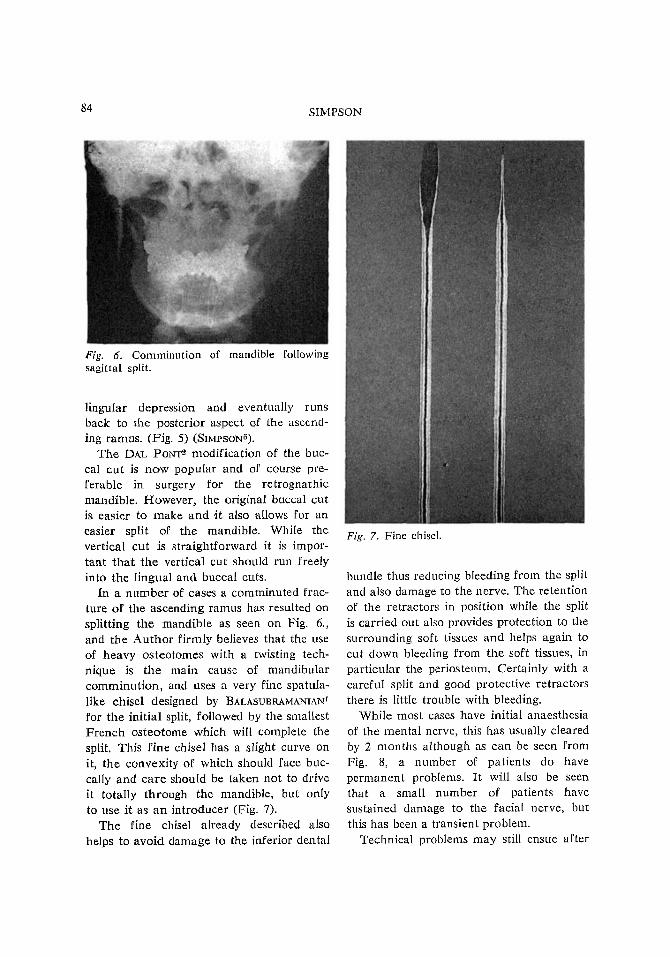
Fig. 6. Comminution of mandible followingsagittal split.
Iingular depression and eventually runsback to the posterior aspect of the ascending ramus. (Fig. 5) (SnvlpsoN5).
The DAL PONT2 modification of the buccal cut is now popular and of course preferable in surgery for the retrognathicmandible. However, the original buccal cutis easier to make and <it also allows for aneasier split of the mandible. While thevertical cut is straightforward it is important that the vertical cut should run freelyinto the lingual and buccal cuts.
In a number of cases a comminuted fracture of the ascending ramus has resulted onsplitting the mandible as seen on Fig. 6.,and the Author firmly believes that the useof heavy osteotomes with a twisting technique is the main cause of mandibularcomminution, and uses a very fine spatulalike chisel designed by BALASUBRAMANIANl
for the initial split, followed by the smallestFrench osteotome which will complete thesplit. This fine chisel has a slight curve onit, the convexity of which should face buccally and care should be taken not to driveit totally through the mandible, but onlyto use it as an introducer (Fig. 7).
The fine chisel already described alsohelps to avoid damage to the inferior dental
Fig. 7. Fine chisel.
bundle thus reducing bleeding from the splitand also damage to the nerve. The retentionof the retractors in position while the splitis carried out also provides protection to thesurrounding soft tissues and helps again tocut down bleeding from the soft tissues, inparticular the periosteum. Certainly with acareful split and good protective retractorsthere is little trouble with bleeding.
While most cases have initial anaesthesiaof the mental nerve, this has usually clearedby 2 months although as can be seen fromFig. 8, a number of patients do havepermanent problems. It will also be seenthat a small number of patients havesustained damage to the facial nerve, butthis has been a transient problem.
Technical problems may still ensue after
PROBLEMS IN SAGITTAL SPLIT 85
Fig. 8. Neurological involvement followingsagittal split osteotomy.
.;
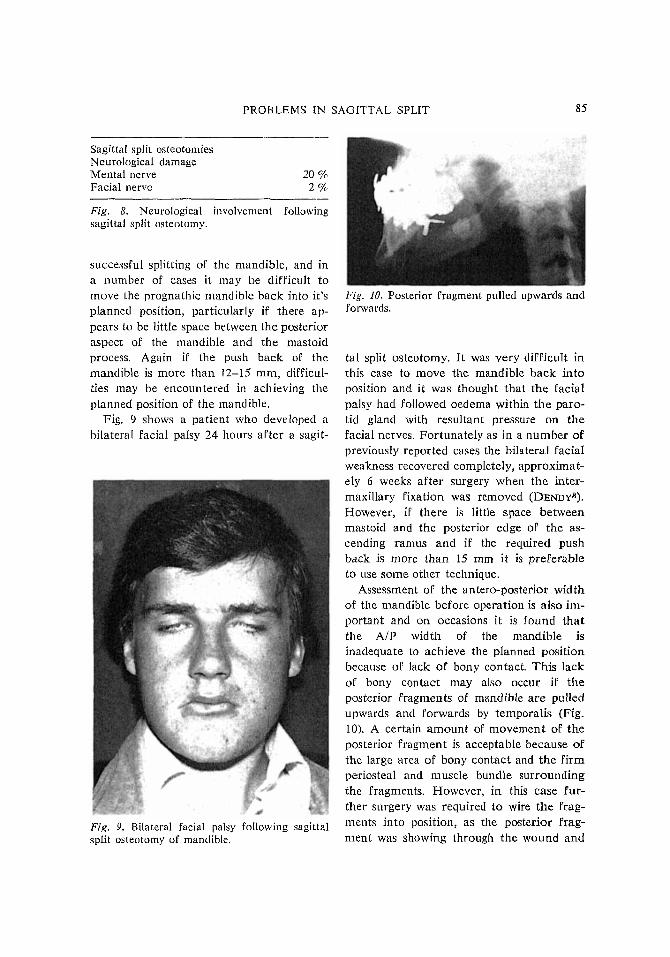
Fig. 9. Bilateral facial palsy following sagittalsplit osteotomy of mandible.
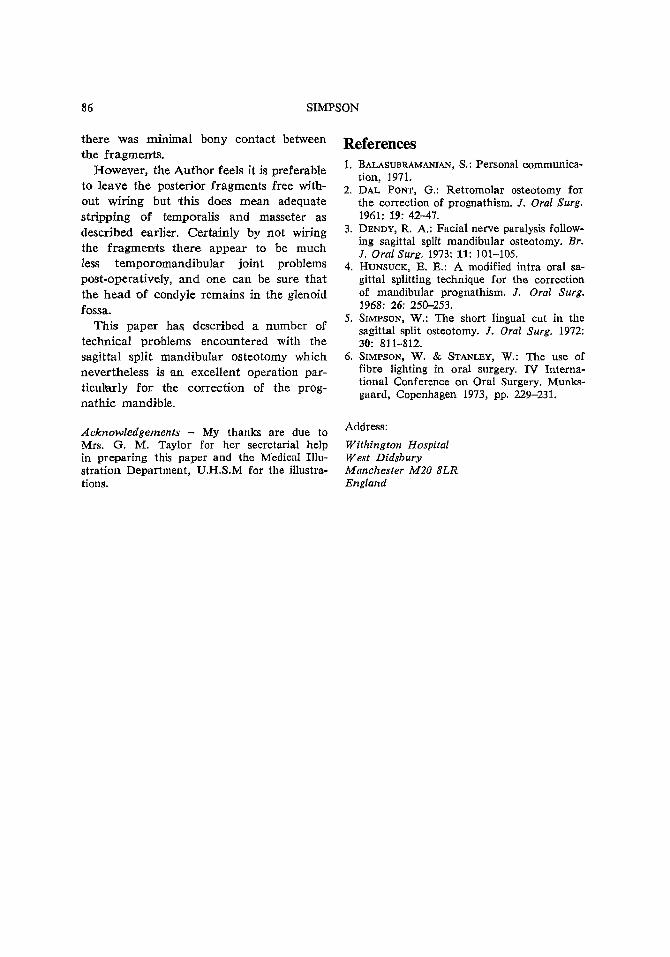
Fig. 10. Posterior fragment pulled upwards andforwards.
tal split osteotomy. It was very difficult inthis case to move the mandible back intoposition and it was thought that the facialpalsy had followed oedema within the parotid gland with resultant pressure on thefacial nerves. Fortunately as in a number ofpreviously reported cases the bilateral facialweakness recovered completely, approximately 6 weeks after surgery when the intermaxillary fixation was removed (DENDy3).
However, if there is little space betweenmastoid and the posterior edge of the ascending ramus and if the required pushback is more than 15 mm it is preferableto use some other technique.
Assessment of the antera-posterior widthof the mandible before operation is also important and on occasions it is found thatthe AlP width of the mandible isinadequate to achieve the planned positionbecause of lack of bony contact. This lackof bony contact may also occur if theposterior fragments of mandible are pulledupwards and forwards by temporalis (Fig.10). A certain amount of movement of theposterior fragment is acceptable because ofthe large area of bony contact and the firmperiosteal and muscle bundle surroundingthe fragments. However, in this case further surgery was required to wire the fragments into position, as the posterior fragment was showing through the wound and
20'){2%
Sagittal split osteotomiesNeurological damageMental nerveFacial nervc
successful splitting of the mandible, and ina number of cases it may be difficult tomove the prognathic mandible back into it'splanned position, particularly if there appears to be little space between the posterioraspect of the mandible and the mastoidprocess. Again if the push back of themandible is more than 12-15 mm, difficulties may be encountered in achieving theplanned position of the mandible.
Fig. 9 shows a patient who developed abilateral facial palsy 24 hours after a sagit-
86 SIMPSON
there Was minimal bony contact betweenthe fragments.
However, the Author feels it is preferableto leave the posterior fragments free without wiring but this does mean adequatestripping of temporalis and masseter asdescribed earlier. Certainly by not wiringthe fragments there appear to be muchless temporomandibular joint problemspost-operatively, and one can be sure thatthe head of condyle remains in the glenoidfossa.
This paper hall described a number oftechnical problems encountered with thesagittal split mandibular osteotomy whichnevertheless is an excellent operation particul'arly for the correction of the prognathic mandible.
Acknowledgements - My thanks are due toMrs. G. M. Taylor for her secretarial helpin preparing this paper and the Medical Illustration Department, U.H.8.M for the illustrations.
References1. BALASUBRAMANIAN, S.: Personal communica
tion, 1971.2. DAL PONT, G.: Retromolar osteotomy for
the correction of prognathism. J. Oral Surg.1961: 19: 42-47.
3. DENDY, R. A.: Facial nerve paralysis following sagittal split mandibular osteotomy. Br.J. Oral Surg. 1973: 11: 101-105.
4. HUNSUCK, E. E.: A modified intra oral sagittal splitting technique for the correctionof mandibular prognathism. J. Oral Surg.1968: 26: 250-253.
5. SIMPSON, W.: The short lingual cut in thesagittal split osteotomy. J. Oral Surg. 1972:30: 811-812.
6. SIMPSON, W. & STANLEY, W.: The use offibre lighting in oral surgery. IV International Conference on Oral Surgery. Munksgaard, Copenhagen 1973, pp. 229-231.
Address:
Withington HospitalWest DidsburyManchester M20 8LREngland





























