Embed Size (px)
Citation preview
Pediatric Pulmonology 41:694–698 (2006)
Case Report
Primary Pulmonary Hodgkin’s Disease andTuberculosis in an 11-Year-Old Boy:
Case Report and Review of the Literature
Daniela Codrich, MD,1* Margherita Monai, MD,1 Gloria Pelizzo, MD,1 Rossana Bussani, MD,2
Marco Rabusin, MD,3 Pierpaolo Guastalla, MD,4 Egidio Barbi, MD,5 and Jurgen Schleef, MD1
Summary. Tuberculosis (TB) has been described in association with different malignancies
including Hodgkin’s disease. However, the association with primary pulmonary Hodgkin’s disease
(PPHD) is hardly reported in literature and in teenage is quite exceptional. We report a case of an
11 years old boy in whom the diagnosis of tuberculosis preceded and delayed the diagnosis of
PPHL. Pediatr Pulmonol. 2006; 41:694–698. � 2006 Wiley-Liss, Inc.
Key words: tuberculosis; primary pulmonary Hodgkin’s lymphoma.
INTRODUCTION
Secondary lung involvement in Hodgkin’s disease (HD)is reported to occur in 15–40% of cases.1 Primarypulmonary Hodgkin’s disease (PPHD) is extremelyrare. PPHD is defined by the following parameters:(1) histologic documentation of Hodgkin’s disease; (2)restriction to the lung parenchyma, with or without mini-mal hilar-node involvement; and (3) no extrapulmonarydisease (CT scans of the thorax and abdomen, and bonemarrow aspirates).1,2
The largest series of PPHD contained 61 patients;1 todate, fewer than 100 cases have been reported in theEnglish-language literature.3
Tuberculosis (TB) can be associated with any malig-nancy which causes immunosuppression, and was repor-ted in cases of HD. According to our knowledge, anassociation with PPHD was reported in the literature onlyby Weber in one case, in 1930.4
We report on a case in which diagnostic dilemmas arosebecause of this very rare association of TB and PPHD.
CASE REPORT
An 11-year-old boy, with a long-standing history ofallergic asthma, presented at our pediatric departmentwith a 2-month persisting dry cough, unresponsive toantihistaminic and bronchodilator therapy. A 6-kg weightloss was noted in the past year, and abfebrile temperatureswere reported in the last 2 weeks.
The physical examination showed an 11-year-old boyin poor general condition, abfebrile (37.68C), and with arespiratory rate of 30/min. Breath sounds were dimin-ished, and the percussion note was dull in the middleand lower left thorax. No palpable lymph nodes weredetected. The liver and spleen were not enlarged. Indicesof inflammation were elevated: white blood cells (WBC),20.110/mm3; erithrocyte sedimentation rate (ESR),53mm/hr;Creactiveprotein (CRP),5.30mg/dl; andLactatedehydrogenase (LDH), 722 IU/ml. A chest x-ray showed
1Department of Surgery, IRCCS Burlo Garofolo, Trieste, Italy.
2Institute of Pathology, University of Trieste, Trieste, Italy.
3Department of Pediatric Oncology, IRCCS Burlo Garofolo, Trieste, Italy.
4Department of Pediatric Radiology, IRCCS Burlo Garofolo, Trieste, Italy.
5Clinic of Pediatrics, University of Trieste, Trieste, Italy.
*Correspondence to: Daniela Codrich, M.D., Department of Pediatric
Surgery, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) Burlo
Garofolo, Children’s Hospital, Via dell’Istria 65/1, 34100 Trieste, Italy.
E-mail: [email protected]
Received 2 September 2005; Revised 30 October 2005; Accepted 31
October 2005.
DOI 10.1002/ppul.20422
Published online 15 May 2006 in Wiley InterScience
(www.interscience.wiley.com).
� 2006 Wiley-Liss, Inc.
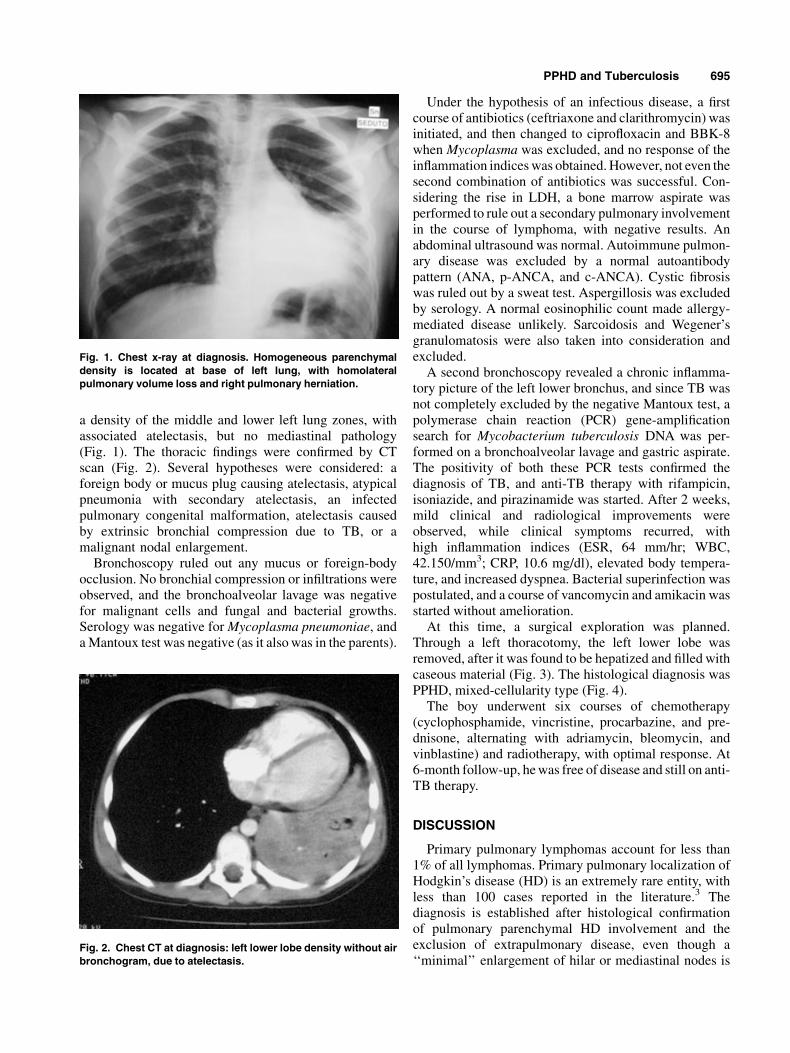
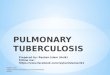
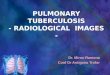
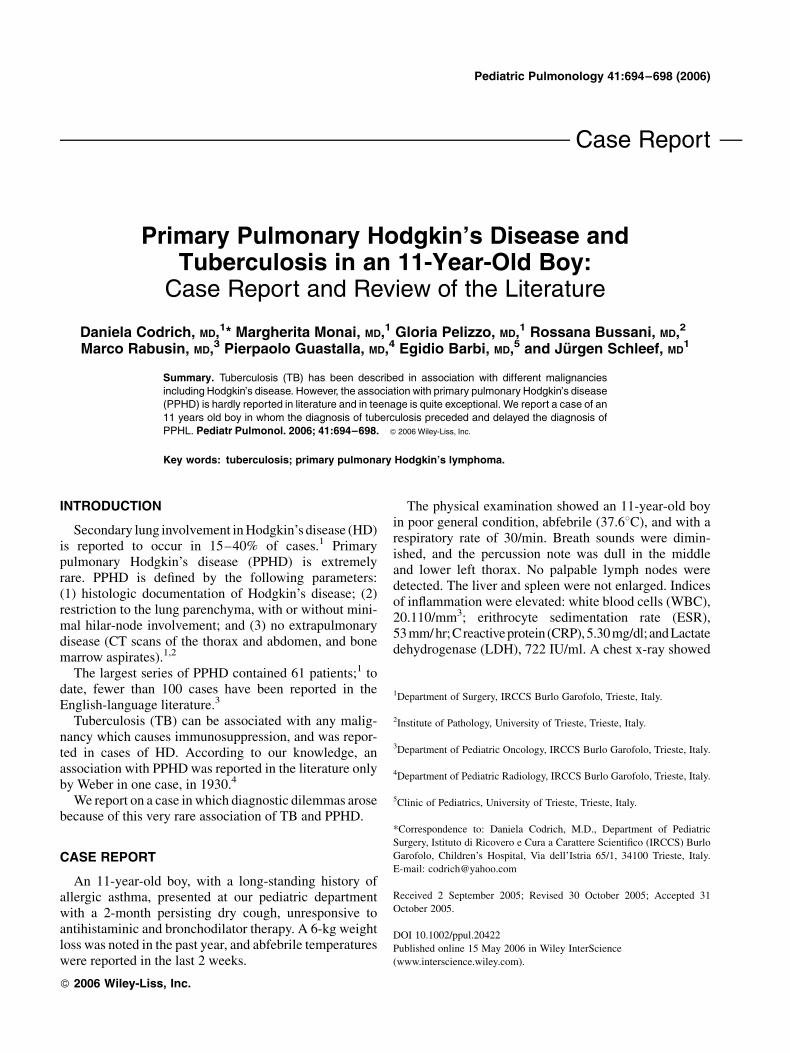
a density of the middle and lower left lung zones, withassociated atelectasis, but no mediastinal pathology(Fig. 1). The thoracic findings were confirmed by CTscan (Fig. 2). Several hypotheses were considered: aforeign body or mucus plug causing atelectasis, atypicalpneumonia with secondary atelectasis, an infectedpulmonary congenital malformation, atelectasis causedby extrinsic bronchial compression due to TB, or amalignant nodal enlargement.
Bronchoscopy ruled out any mucus or foreign-bodyocclusion. No bronchial compression or infiltrations wereobserved, and the bronchoalveolar lavage was negativefor malignant cells and fungal and bacterial growths.Serology was negative for Mycoplasma pneumoniae, anda Mantoux test was negative (as it also was in the parents).
Under the hypothesis of an infectious disease, a firstcourse of antibiotics (ceftriaxone and clarithromycin) wasinitiated, and then changed to ciprofloxacin and BBK-8when Mycoplasma was excluded, and no response of theinflammation indices was obtained. However, not even thesecond combination of antibiotics was successful. Con-sidering the rise in LDH, a bone marrow aspirate wasperformed to rule out a secondary pulmonary involvementin the course of lymphoma, with negative results. Anabdominal ultrasound was normal. Autoimmune pulmon-ary disease was excluded by a normal autoantibodypattern (ANA, p-ANCA, and c-ANCA). Cystic fibrosiswas ruled out by a sweat test. Aspergillosis was excludedby serology. A normal eosinophilic count made allergy-mediated disease unlikely. Sarcoidosis and Wegener’sgranulomatosis were also taken into consideration andexcluded.
A second bronchoscopy revealed a chronic inflamma-tory picture of the left lower bronchus, and since TB wasnot completely excluded by the negative Mantoux test, apolymerase chain reaction (PCR) gene-amplificationsearch for Mycobacterium tuberculosis DNA was per-formed on a bronchoalveolar lavage and gastric aspirate.The positivity of both these PCR tests confirmed thediagnosis of TB, and anti-TB therapy with rifampicin,isoniazide, and pirazinamide was started. After 2 weeks,mild clinical and radiological improvements wereobserved, while clinical symptoms recurred, withhigh inflammation indices (ESR, 64 mm/hr; WBC,42.150/mm3; CRP, 10.6 mg/dl), elevated body tempera-ture, and increased dyspnea. Bacterial superinfection waspostulated, and a course of vancomycin and amikacin wasstarted without amelioration.
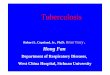
At this time, a surgical exploration was planned.Through a left thoracotomy, the left lower lobe wasremoved, after it was found to be hepatized and filled withcaseous material (Fig. 3). The histological diagnosis wasPPHD, mixed-cellularity type (Fig. 4).
The boy underwent six courses of chemotherapy(cyclophosphamide, vincristine, procarbazine, and pre-dnisone, alternating with adriamycin, bleomycin, andvinblastine) and radiotherapy, with optimal response. At6-month follow-up, he was free of disease and still on anti-TB therapy.
DISCUSSION
Primary pulmonary lymphomas account for less than1% of all lymphomas. Primary pulmonary localization ofHodgkin’s disease (HD) is an extremely rare entity, withless than 100 cases reported in the literature.3 Thediagnosis is established after histological confirmationof pulmonary parenchymal HD involvement and theexclusion of extrapulmonary disease, even though a‘‘minimal’’ enlargement of hilar or mediastinal nodes is
Fig. 1. Chest x-ray at diagnosis. Homogeneous parenchymal
density is located at base of left lung, with homolateral
pulmonary volume loss and right pulmonary herniation.
Fig. 2. Chest CT at diagnosis: left lower lobe density without air
bronchogram, due to atelectasis.
PPHD and Tuberculosis 695

accepted.1–3,5,6 To date, the largest published reportcontained 61 cases of proven PPHD,1 and since then,few cases have been added. However, the present caseshows two other peculiarities in addition to the alreadyrare diagnosis: one is the association with TB, and theother is the age (11 years) of our patient. The only case ofassociated PPHD and TB was reported in 1930 by Weberin a 27-year-old man.4
The association between TB and nonprimary pulmon-ary HD was previously described.7,8 Immune suppressionis a well-known condition in HD, where cellular immunedeficiency can lead to secondary infection. Karakas et al.7
reported TB associated with HD in 14 of 70 children(20%). Of these 14 patients, the diagnosis of TB precededthat of HD in 3, in 2 there was a concomitant diagnosis, and7 developed TB during HD treatment. However, none ofthese patients were reported to have PPHD.
Our delay in the diagnosis of TB was due to boththe negative result of the Mantoux test and the first
negative growth of alcohol-acid-resistant bacilli onsputum. The first issue can be explained by the impairedcellular response occurring during HD, while the secondcan be explained by the low bacteriological yield of BAL(around 30%).9 Moreover, the patient had been treatedwith two antibiotics (ciprofloxacin and amikacin) that areboth active against TB. PCR on sputum and/or on gastriclavage has a sensitivity of 97.8% and 63.4%, respec-tively,10 and it was the procedure which gave us thediagnosis of TB.
PPHD seems to be more frequent in females and to have abimodal age distribution,1 with peaks in the third and sixthdecades: the youngest patient reported so far is a 15-year-old boy.3 Presenting symptoms of TB and HD can be quitesimilar and misleading. As described by Radin,1 patientswith PPHD usually present for evaluation of respiratorysymptoms such as persistent dry cough, mild chestdiscomfort, and less commonly, hemoptysis and wheezing.Systemic TB-like symptoms (i.e., weight loss, fever, and
Fig. 3. Left lower lobe after resection, macroscopic aspect: lung parenchyma exhibited total loss
of architecture, with occasional foci of necrosis and presence of caseous material.
696 Codrich et al.
night sweats) were reported in only 22 of 61 patients.1 Ourpatient showed dry cough, and weight loss, and fever. As inour case, the median duration of symptoms before clinicalpresentation was between 2–4 months.
Parenchymal pulmonary involvement can be eithermultinodular or massive, with or without cavitations.Pneumonic infiltration was also described, but is moreuncommon (13 of 61 patients in the series of Radin).1
Bilateral involvement was reported in 2 patients.1
A common problem in cases of PPHD is the delayeddiagnosis and the inconclusive responses of both radi-ological examinations and bronchoscopy.1–3,5,6 In thelargest series, only one bronchoscopy out of 39 wasdiagnostic.1 Usually no malignant cell can be collectedfrom the bronchial lavage, and only a few nonspecificinflammatory signs can be detected. In cases of peribron-chial lymphoma, signs of external bronchial compressioncan be detected. In all instances, the diagnosis was notsuspected before histological evaluation of a surgicallycollected specimen.
Common treatment in the literature consists of acombination of surgery, chemotherapy, and radiotherapy.Protocols usually include a combination of drugs. Thecombination we used was described by others,2 and it isthe chemo-radiotherapy protocol we use in patients withstage 3 or stage 4 disease. The small number of reportedcases and the scarcity of follow-up information do notallow a correct estimation of survival, although bilateral
disease and the involvement of more than one lobe wereassociated with a poorer prognosis1.
CONCLUSIONS
PPHD is a rare entity which can associate with otherpulmonary diseases. The diagnosis can be very challen-ging. Our experience and the published literature confirmthat in any suspicious case, a pulmonary biopsy obtainedat thoracotomy is essential for diagnosis. Nevertheless, anearly thoracoscopic approach in difficult and unclear casesmight be justified to obtain lung and lymph node tissue.The resection of the involved tissue might be indicated, toimprove the prognosis of this rare oncological entity.
REFERENCES
1. Radin AI. Primary pulmonary Hodgkin’s disease. Cancer
1990;65:550–563.
2. Pinson P, Joos G, Praet M, Pauwels R. Primary pulmonary
Hodgkin’s disease. Respiration 1992;59:314–316.
3. Boshnakova T, Michailova V, Koss M, Georgiev C, Todorov T,
Sarbinova M. Primary pulmonary Hodgkin’s disease—report of
two cases. Respir Med 2000;94:830–831.
4. Weber H. Lungenlymphogranulome. Beitr Z Pathol Anat Verh Z
Allg Pathol 1930;84:1–32.
5. Pik A, Cohen N, Weissgarten J, Kaufman S, Modai D. Primary
pulmonary Hodgkin’s disease with air bronchogram. Respiration
1986;50:226–229.
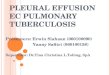
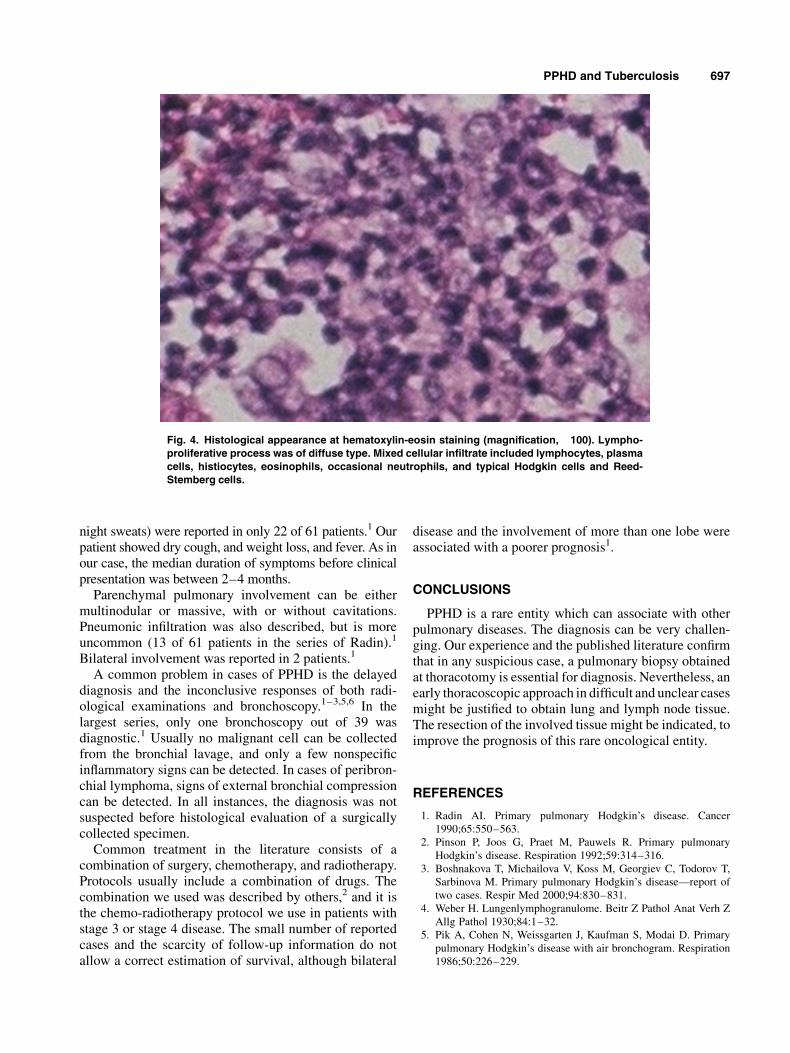
Fig. 4. Histological appearance at hematoxylin-eosin staining (magnification, �100). Lympho-
proliferative process was of diffuse type. Mixed cellular infiltrate included lymphocytes, plasma
cells, histiocytes, eosinophils, occasional neutrophils, and typical Hodgkin cells and Reed-
Stemberg cells.
PPHD and Tuberculosis 697

6. van der Schee AC, Dinkla BA, van Knapen A. Primary pulmonary
manifestation of Hodgkin’s disease. Respiration 1990;57:127–
128.
7. Karakas Z, Agaoglu L, Taravari B, Saribeyoglu E, Somer NG,
Unuvar A, et al. Pulmonary tuberculosis in children with
Hodgkin’s lymphoma. Hematol J 2003;4:78–81.
8. Costa LJ, Gallafrio CT, Franca FO, del Giglio A. Simultaneous
occurrence of Hodgkin’s disease and tuberculosis: report of three
cases. South Med J 2004;97:696–698.
9. Somu N, Swaminathan S, Paramasivan CN, Vijayasekaran D,
Chandrabhooshanam A, Vijayan VK, et al. Value of bronchoal-
veolar lavage and gastric lavage in the diagnosis of pulmonary
tuberculosis in children. Tuberc Lung Dis 1995;76:295–299.
10. Mitarai S, Oishi K, Fukasawa M, Yamashita H, Nagatake T,
Matsumoto K. Clinical evaluation of polymerase chain reaction
DNA amplification method for the diagnosis of pulmonary
tuberculosis in patients with negative acid-fast bacilli smear.
Tohoku J Exp Med 1995;177:13–23.
698 Codrich et al.