Embed Size (px)
Citation preview
Journal of Surgical Oncology 37: 200-103 (1988)
Primary Breast Cancer in Patients With Previous Endometrial or Ovarian Cancer
RAYMOND C. DOBERNECK, MD, PhD, AND JOSEPH E. GARCIA, MD
From the University of New Mexico School of Medicine, Albuquerque, New Mexico
The incidence of primary breast cancer is known to be increased in patients with previous endometrial or ovarian cancer, but the behavior of the breast cancer and the ultimate outlook for such patients is unknown. To provide data concerning these two questions, a group of 123 patients treated for breast cancer alone (Group I) served as a control for comparison with ten patients who had endometrial cancer (Group 11) and six patients who had ovarian cancer (Group 111) prior to diagnosis of breast cancer. The interval between the diagnosis of endometrial cancer and breast cancer averaged 4.6 yr, and between ovarian cancer and breast cancer, 5.4 yr. Age at diagnosis of breast cancer in Groups I, 11, and 111 was 56, 66 (P = 0.05) and 56 yr, respectively. The incidence of patients with stage I, 11, and 111 breast cancer was similar in Groups I, 11, and 111 as was tumor size and number of metastatic nodes in each stage in each of the three groups. Average duration of follow-up after diagnosis of breast cancer was 3, 3.1, and 2.8 yr in Groups I, 11, and 111, respectively, with 70%, 60%, and 33 % of patients living and free of either breast cancer, endometrial cancer, or ovarian cancer. Two of four deaths in Group I1 were due to endometrial cancer, and all four deaths in Group I11 were due to ovarian cancer. The remaining two deaths or recurrences in Group I1 were due to breast cancer. We conclude.that 1) the behavior of breast cancer is similar in patients with or without previous endometrial or ovarian cancer; 2) breast cancer develops at an older age in patients with previous endometrial cancer than in patients with or without previous ovarian cancer and 3) death or recurrent cancer in patients with breast cancer and previous ovarian cancer is due to ovarian cancer, whereas, death or recurrent cancer in patients with breast cancer and previous endometrial cancer is due equally to breast cancer and endometrial cancer.
KEY WORDS: breast, endometrial ovarian cancer, multiple cancers
INTRODUCTION
The description of multiple primary malignant tumors in a single patient by Billroth is among the earliest on the subject Since then scribe the associations of certain types of malignancies, among them breast with endometrial and ovarian cancer [2-51. This latter association is reported to occur 1.5 to 2 times as often as anticipated. Unfortunately, many reports do not make clear which is the initial malignancy Accepted for pub'jcation December 29, 1986*
Address reprint requests to Dr. Raymond C. Doberneck, University but most reprts describe second primary of New Mexico School of Medicine, Department of Surgery, 2211 in patients with initial breast cancer. Moreover whether Lomas, N.E., Albuquerque, NM 87131.
or not a common basis exists for the association of breast with endometrial and ovarian cancer is unknown.
A medline search reveals little concerning the outlook additional reports de- for patients with initial endometrial or ovarian cancer
who develop a second primary breast cancer. An occa- sional report states that the outlook for patients with multiple primary malignancies is governed by the neo-
0 1988 Alan R. Liss, Inc.
Primary Breast Cancer 101
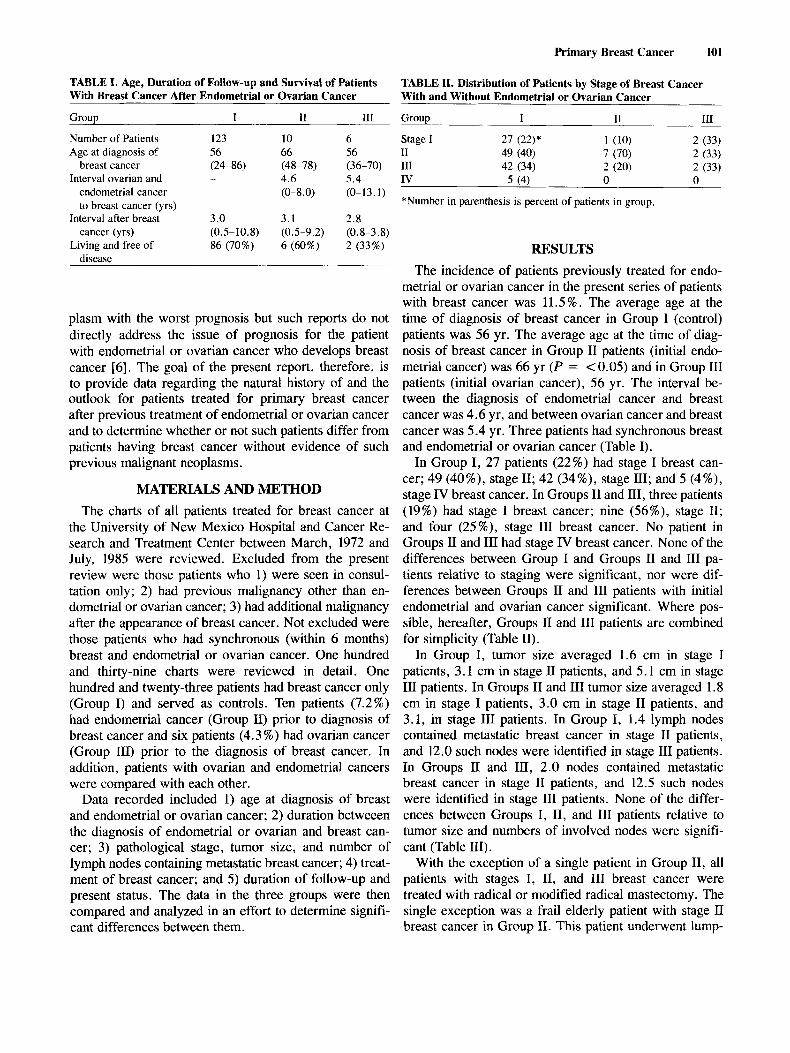
TABLE I. Age, Duration of Follow-up and Survival of Patients With Breast Cancer After Endometrial or Ovarian Cancer
TABLE XI. Distribution of Patients by Stage of Breast Cancer With and Without Endometrial or Ovarian Cancer
Group I I1 I11
Number of Patients Age at diagnosis of
breast cancer Interval ovarian and
endometrial cancer to breast cancer (yrs)
cancer (yrs)
disease
Interval after breast
Living and free of
123 10 56 66 (24-86) (48-78) - 4.6
(0-8.0)
3 .O 3.1
86 (70%) 6 (60%) (0.5-10.8) (0.5-9.2)
6 56 (36-70) 5.4 (0-13.1)
2.8 (0.8-3.8) 2 (33%)
plasm with the worst prognosis but such reports do not directly address the issue of prognosis for the patient with endometrial or ovarian cancer who develops breast cancer 161. The goal of the present report, therefore, is to provide data regarding the natural history of and the outlook for patients treated for primary breast cancer after previous treatment of endometrial or ovarian cancer and to determine whether or not such patients differ from patients having breast cancer without evidence of such previous malignant neoplasms.
MATERIALS AND METHOD The charts of all patients treated for breast cancer at
the University of New Mexico Hospital and Cancer Re- search and Treatment Center between March, 1972 and July, 1985 were reviewed. Excluded from the present review were those patients who 1) were seen in consul- tation only; 2) had previous malignancy other than en- dometrial or ovarian cancer; 3) had additional malignancy after the appearance of breast cancer. Not excluded were those patients who had synchronous (within 6 months) breast and endometrial or ovarian cancer. One hundred and thirty-nine charts were reviewed in detail. One hundred and twenty-three patients had breast cancer only (Group I) and served as controls. Ten patients (7.2%) had endometrial cancer (Group 11) prior to diagnosis of breast cancer and six patients (4.3 %) had ovarian cancer (Group 111) prior to the diagnosis of breast cancer. In addition, patients with ovarian and endometrial cancers were compared with each other.
Data recorded included 1) age at diagnosis of breast and endometrial or ovarian cancer; 2) duration betweeen the diagnosis of endometrial or ovarian and breast can- cer; 3) pathological stage, tumor size, and number of lymph nodes containing metastatic breast cancer; 4) treat- ment of breast cancer; and 5 ) duration of follow-up and present status. The data in the three groups were then compared and analyzed in an effort to determine signifi- cant differences between them.
Grouu I I1 111
*Number in parenthesis is percent of patients in group.
RESULTS The incidence of patients previously treated for endo-
metrial or ovarian cancer in the present series of patients with breast cancer was 11.5 % . The average age at the time of diagnosis of breast cancer in Group I (control) patients was 56 yr. The average age at the time of diag- nosis of breast cancer in Group I1 patients (initial endo- metrial cancer) was 66 yr (2' = < 0.05) and in Group I11 patients (initial ovarian cancer), 56 yr. The interval be- tween the diagnosis of endometrial cancer and breast cancer was 4.6 yr, and between ovarian cancer and breast cancer was 5.4 yr. Three patients had synchronous breast and endometrial or ovarian cancer (Table I).
In Group I, 27 patients (22%) had stage I breast can- cer; 49 (40%), stage 11; 42 (34%), stage 111; and 5 (4%), stage IV breast cancer. In Groups I1 and 111, three patients (19%) had stage I breast cancer; nine (56%), stage 11; and four (25%), stage I11 breast cancer. No patient in Groups I1 and I11 had stage IV breast cancer. None of the differences between Group I and Groups I1 and I11 pa- tients relative to staging were significant, nor were dif- ferences between Groups I1 and I11 patients with initial endometrial and ovarian cancer significant. Where pos- sible, hereafter, Groups I1 and I11 patients are combined for simplicity (Table 11).
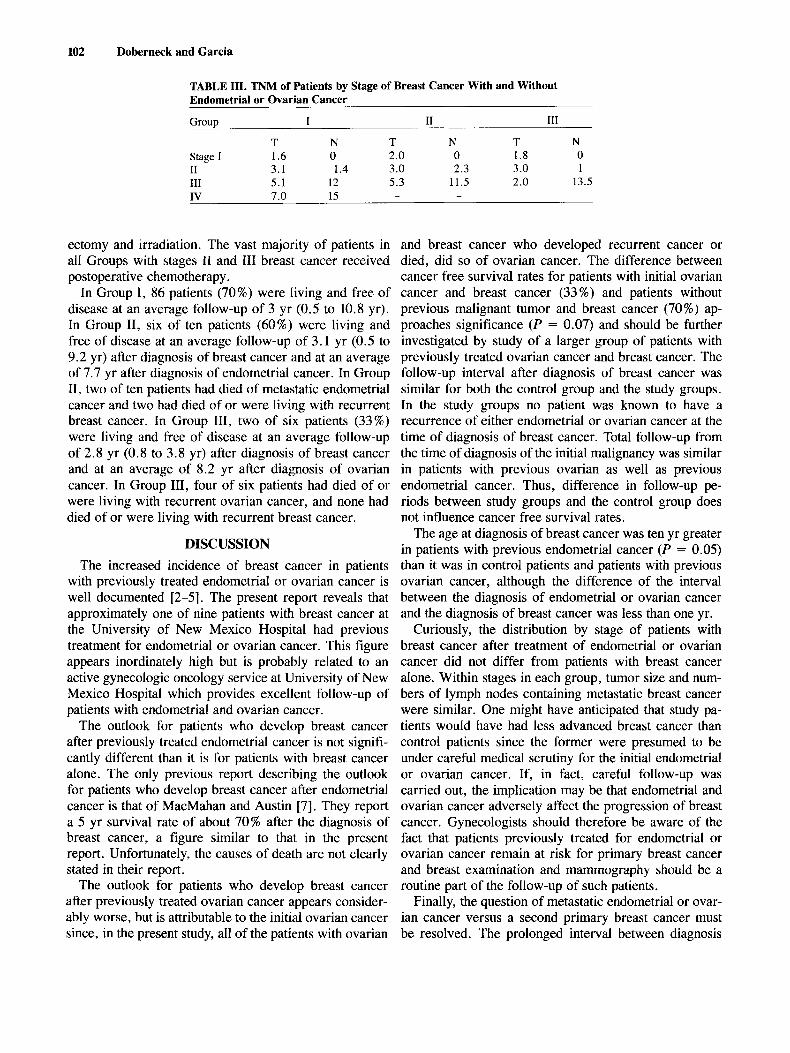
In Group I, tumor size averaged 1.6 cm in stage I patients, 3.1 cm in stage I1 patients, and 5.1 cm in stage III patients. In Groups I1 and 111 tumor size averaged 1.8 cm in stage I patients, 3.0 cm in stage I1 patients, and 3.1, in stage I11 patients. In Group I, 1.4 lymph nodes contained metastatic breast cancer in stage I1 patients, and 12.0 such nodes were identified in stage I11 patients. In Groups I1 and 111, 2.0 nodes contained metastatic breast cancer in stage I1 patients, and 12.5 such nodes were identified in stage I11 patients. None of the differ- ences between Groups I, 11, and 111 patients relative to tumor size and numbers of involved nodes were signifi- cant (Table 111).
With the exception of a single patient in Group 11, all patients with stages I, 11, and 111 breast cancer were treated with radical or modified radical mastectomy. The single exception was a frail elderly patient with stage I1 breast cancer in Group 11. This patient underwent lump-
102 Doberneck and Garcia
TABLE 111. TNM of Patients by Stage of Breast Cancer With and Without Endometrial or Ovarian Cancer
Group I I1 111
Stage I 1.6 0 2.0 0 1.8 0 T N T N T N
I1 3.1 1.4 3.0 2.3 3 .O 1 111 5.1 12 5.3 11.5 2.0 13.5 IV 7.0 15 - -
ectomy and irradiation. The vast majority of patients in and breast cancer who developed recurrent cancer or all Groups with stages I1 and I11 breast cancer received died, did so of ovarian cancer. The difference between postoperative chemotherapy. cancer free survival rates for patients with initial ovarian
In Group I, 86 patients (70%) were living and free of cancer and breast cancer (33%) and patients without disease at an average follow-up of 3 yr (0.5 to 10.8 yr). previous malignant tumor and breast cancer (70%) ap- In Group 11, six of ten patients (60%) were living and proaches significance ( P = 0.07) and should be further free of disease at an average follow-up of 3.1 yr (0.5 to investigated by study of a larger group of patients with 9.2 yr) after diagnosis of breast cancer and at an average previously treated ovarian cancer and breast cancer. The of 7.7 yr after diagnosis of endometrial cancer. In Group follow-up interval after diagnosis of breast cancer was 11, two of ten patients had died of metastatic endometrial similar for both the control group and the study groups. cancer and two had died of or were living with recurrent In the study groups no patient was known to have a breast cancer. In Group 111, two of six patients (33 %) recurrence of either endometrial or ovarian cancer at the were living and free of disease at an average follow-up time of diagnosis of breast cancer. Total follow-up from of 2.8 yr (0.8 to 3.8 yr) after diagnosis of breast cancer the time of diagnosis of the initial malignancy was similar and at an average of 8.2 yr after diagnosis of ovarian in patients with previous ovarian as well as previous cancer. In Group 111, four of six patients had died of or endometrial cancer. Thus, difference in follow-up pe- were living with recurrent ovarian cancer, and none had riods between study groups and the control group does died of or were living with recurrent breast cancer. not influence cancer free survival rates.
The age at diagnosis of breast cancer was ten yr greater DISCUSSION in patients with previous endometrial cancer (P = 0.05)
The increased incidence of breast cancer in patients than it was in control patients and patients with previous with previously treated endometrial or ovarian cancer is ovarian cancer, although the difference of the interval well documented [2-51. The present report reveals that between the diagnosis of endometrial or ovarian cancer approximately one of nine patients with breast cancer at and the diagnosis of breast cancer was less than one yr. the University of New Mexico Hospital had previous Curiously, the distribution by stage of patients with treatment for endometrial or ovarian cancer. This figure breast cancer after treatment of endometrial or ovarian appears inordinately high but is probably related to an cancer did not differ from patients with breast cancer active gynecologic oncology service at University of New alone. Within stages in each group, tumor size and num- Mexico Hospital which provides excellent follow-up of bers of lymph nodes containing metastatic breast cancer patients with endometrial and ovarian cancer. were similar. One might have anticipated that study pa-
The outlook for patients who develop breast cancer tients would have had less advanced breast cancer than after previously treated endometrial cancer is not signifi- control patients since the former were presumed to be cantly different than it is for patients with breast cancer under careful medical scrutiny for the initial endometrial alone. The only previous report describing the outlook or ovarian cancer. If, in fact, careful follow-up was for patients who develop breast cancer after endometrial carried out, the implication may be that endometrial and cancer is that of MacMahan and Austin [7]. They report ovarian cancer adversely affect the progression of breast a 5 yr survival rate of about 70% after the diagnosis of cancer. Gynecologists should therefore be aware of the breast cancer, a figure similar to that in the present fact that patients previously treated for endometrial or report. Unfortunately, the causes of death are not clearly ovarian cancer remain at risk for primary breast cancer stated in their report. and breast examination and mammography should be a
The outlook for patients who develop breast cancer routine part of the follow-up of such patients. after previously treated ovarian cancer appears consider- Finally, the question of metastatic endometrial or ovar- ably worse, but is attributable to the initial ovarian cancer ian cancer versus a second primary breast cancer must since, in the present study, all of the patients with ovarian be resolved. The prolonged interval between diagnosis

of endometrial or ovarian cancer and the appearance of breast cancer argues in favor of a new primary rather than metastatic cancer to the breast. Unfortunately, this argument is weakened by the synchronous appearance of breast and ovarian cancer in two patients and breast and endometrial cancer in one patient in the present study. To counter the latter argument is the fact that the pathologists involved in the present study were aware of the existence of the initial neoplasm and yet were unequivocal in their diagnosis of primary breast cancer on the basis of biopsy of the breast. Moreover, all patients with ovarian cancer in the present report had an initial unilateral ovarian neoplasm whereas the majority of breast cancers metas- tasizing to ovary do so bilaterally [8].
CONCLUSION The incidence of breast cancer is increased in patients
with previous endometrial or ovarian cancer, but the influence of the latter on the former is unknown. One hundred twenty-three patients with only breast cancer were compared with 16 patients who developed breast cancer after initial endometrial (ten patients) or ovarian cancer (six patients). Distribution by stage of breast can- cer, tumor size, and number of lymph nodes involved was similar in all groups. Patients who developed breast cancer after initial endometrial cancer were ten yr older than patients with breast cancer alone and patients who developed breast cancer after initial ovarian cancer. Sev- enty percent of patients with breast cancer alone were
Primary Breast Cancer 103
living and free of disease at an average of three yr after diagnosis of breast cancer while 60% of patients with breast cancer after endometrial cancer and 33% of pa- tients with breast cancer after ovarian cancer were in such condition at an average of three yr after diagnosis of breast cancer. We conclude that the outlook for pa- tients who develop breast cancer after the initial devlop- ment of ovarian cancer is probably adversely affected by the ovarian cancer. The behavior of breast cancer in patients with previous endometrial or ovarian cancer ap- pears similar to that of breast cancer in patients having breast cancer as their only malignancy.
REFERENCES 1.
2.
3.
4.
5.
6.
7.
8.
Billroth T: Die allgemeine chirgishe. Pathologie und Therapie. 14 Auflage. Berlin, Reimer, p 908, 1899. Bailar JC: The incidence of independent tumors among uterine cancer patients. Cancer 16:842-853, 1963. Schottenfeld D, Berg J: Incidence of multiple primary cancers. IV. Cancers of the female breast and genital organs. J Nat Cancer
Reimer RR, Hoover R, Fraumeni JF, Young RC: Second primary neoplasms following ovarian cancer. J Nat Cancer Inst 61:1195- 1197, 1978. Ray P, Sharifi R, Ortolano V, Grunan P: Involvement of the genitourinary system in multiple primary malignant neoplasms: A review. J Clin Oncol 1574-581, 1983. Yohoe R, Ishida T, Iino U, Kawai T, Izuo M: Clinicopathological study of breast cancers associated with other primary cancers. Gan No Rinsho 30: 1883-1891, 1984. MacMahan B, Austin JH: Association of carcinomas of the breast and corpus uteri. Cancer 23:275-280, 1969. Young RH, Carey RW, Robboy SJ: Breast cancer masquerading as primary ovarian neoplasm. Cancer 48:210-212, 1981.
Inst 46: 161-170, 1971.