-
8/7/2019 Presentation TCT Washington 2
1/28
PCI and hypothermia for PCI and hypothermia for STEMI in a
patient foundSTEMI in a patient found
and resuscitated in aand resuscitated in ahospital elevator
hospital elevator
Kristina Maric Besic, MDKristina Maric Besic, MD
Department of Cardiovascular Department of Cardiovascular
MedicineMedicine
School of Medicine & University Hospital CentreSchool of
Medicine & University Hospital Centre
ZagrebZagreb
Zagreb, CroatiaZagreb, Croatia
-
8/7/2019 Presentation TCT Washington 2
2/28
Disclosure Statement of Financial InterestDisclosure Statement
of Financial Interest
I,I, Kristina Maric BesicKristina Maric Besic DO NOT have aDO
NOT have a
financial interest/arrangement or affiliationfinancial
interest/arrangement or affiliationwith one or more organizations
that couldwith one or more organizations that couldbe perceived as
a real or apparent conflictbe perceived as a real or apparent
conflictof interest in the context of the subject of of interest in
the context of the subject of
this presentation.this presentation.
-
8/7/2019 Presentation TCT Washington 2
3/28
CASE REPORT:CASE REPORT:
March 2010March 2010 - - male, 45 years, no history or male, 45
years, no history or known risk factors for CVDknown risk factors
for CVD
UUnwitnessed cardiac arrest in a hospitalnwitnessed cardiac
arrest in a hospitalelevator (found at aprox.elevator (found at
aprox. 7 7:20 p.m):20 p.m)CPR in ER: adrenalin 3 mg, DCx4 for VFCPR
in ER: adrenalin 3 mg, DCx4 for VFECG:sinus rhythm, anterolateral
STEMIECG:sinus rhythm, anterolateral STEMI
AAdmitted to CCU (arounddmitted to CCU (around 8 8:00 p.m) RR:00
p.m) RR90/60 mmHG, without spontaneus90/60 mmHG, without
spontaneusbreathing, comabreathing, coma GCS 3GCS 3
-
8/7/2019 Presentation TCT Washington 2
4/28
UUrgent coronary angiography and PPCIrgent coronary angiography
and PPCIwithout prior neurological examinationwithout prior
neurological examinationHHypothermia after PCIypothermia after
PCI
NG tubeNG tube retention 500 mlretention 500 ml- - did not
recievedid not recieveaspirin or clopidogrel befor PCIaspirin or
clopidogrel befor PCIUUnfractioned heparin during PCInfractioned
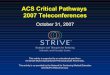
heparin during PCICoronary angiography findingCoronary angiography
finding- - occlusionocclusionof prox. LAD, significant stenosis of
LCXof prox. LAD, significant stenosis of LCXand RCAand RCA
-
8/7/2019 Presentation TCT Washington 2
5/28
-
8/7/2019 Presentation TCT Washington 2
6/28
-
8/7/2019 Presentation TCT Washington 2
7/28
-
8/7/2019 Presentation TCT Washington 2
8/28
-
8/7/2019 Presentation TCT Washington 2
9/28
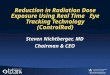
PPerforation of coronary arteryerforation of coronary artery -
-call the surgeon?call the surgeon?
-
8/7/2019 Presentation TCT Washington 2
10/28
-
8/7/2019 Presentation TCT Washington 2
11/28
-
8/7/2019 Presentation TCT Washington 2
12/28
-
8/7/2019 Presentation TCT Washington 2
13/28
-
8/7/2019 Presentation TCT Washington 2
14/28
-
8/7/2019 Presentation TCT Washington 2
15/28
-
8/7/2019 Presentation TCT Washington 2
16/28
-
8/7/2019 Presentation TCT Washington 2
17/28
PCI PROCEDUREPCI PROCEDURE
StartedStarted 8 8:55 p.m, ended 10:52 p.m.:55 p.m, ended 10:52
p.m.
RResuscitatedesuscitated adrenalin, atropinadrenalin,
atropinLADLAD 5 stents5 stents - - TIMI 3TIMI 3
RCARCA 2 stents2 stents TIMI 3TIMI 3
-
8/7/2019 Presentation TCT Washington 2
18/28
ANTITHROMBOTIC THERAPYANTITHROMBOTIC THERAPY
15 000 IU unfractioned heparin during PCI15 000 IU unfractioned
heparin during PCI
Continuous iv unfractioned heparin after Continuous iv
unfractioned heparin after PCIPCI-- was not given because of was
not given because of prolongedprolongedAPTTAPTT
-
8/7/2019 Presentation TCT Washington 2
19/28
ECHOECHO-- no pericardial effusionno pericardial effusion
NNeurological examinationeurological examination pupils no
lightpupils no lightresponse, corneal reflex and MTR
absentresponse, corneal reflex and MTR absent
HHypothermia (induced at 1:15 a.m)ypothermia (induced at 1:15
a.m)
MMidazolam, rocuronium (sedation andidazolam, rocuronium
(sedation andneuromuscular blockade)neuromuscular blockade)
CCooling induction with cold saline 4ooling induction with cold
saline 4 CC(30ml/kg during 30(30ml/kg during 30- -60 min) and ice60
min) and icepackages (neck, armpits, groins)packages (neck,
armpits, groins) targettargetbody temperature 32body temperature
32- -3434C during 2C during 2- -6 h6 h
-
8/7/2019 Presentation TCT Washington 2
20/28
AAt 5:30 a.m RRt 5:30 a.m RR 90/60 mmHg 90/60 mmHg - -
dopaminedopamine
AAt 7:30 a.m RR 70/50 mmHgt 7:30 a.m RR 70/50 mmHg - -
dobutaminedobutamineand noradrenalineand noradrenaline
Hgb (132 Hgb (132- -126126--120120--97g/L), normal
platlet97g/L), normal platlet
count, APTT >120, >150 s (24.0count, APTT >120, >150
s (24.0- -33.0)33.0)X rayX ray-- left pleural effusionleft pleural
effusion
AAtt 22:20 p.m VT, VF,:20 p.m VT, VF, - - CPR, urgentCPR,
urgent
evacuation of pleural effusionevacuation of pleural effusion
1500 ml of 1500 ml of bloodblood- -
autotransfusionautotransfusion
DDeath at 3:45 p.meath at 3:45 p.m hemorrhagic shockhemorrhagic
shock
-
8/7/2019 Presentation TCT Washington 2
21/28
2005 AHA Guidelines for Cardiopulmonary2005 AHA Guidelines for
Cardiopulmonary
Resuscitation and EmergencyResuscitation and
EmergencyCardiovascular Care:Cardiovascular Care:
UUnconscious patients with ROSC after outnconscious patients
with ROSC after out- -of of--hospital cardiac arrest should be
cooledhospital cardiac arrest should be cooledto 32to 32C to 34C to
34 C for 12C for 12- -24 hours when the24 hours when theinital
rhytm was VF (Class IIa)inital rhytm was VF (Class IIa)
MMay be beneficial for patients with nonay be beneficial for
patients with non- -VFVFarrest out of hospital or for inarrest out
of hospital or for in- -hospitalhospitalarrest (Class IIb)arrest
(Class IIb)
-
8/7/2019 Presentation TCT Washington 2
22/28
HYPOTHERMIA INDICATIONSHYPOTHERMIA INDICATIONS
CCardiorespiratory arrest (VT,VF, PEA,ardiorespiratory arrest
(VT,VF, PEA,asystolia)asystolia)
DDuration of cardiorespiratory arrest 5 uration of
cardiorespiratory arrest 5- -15 15
min (from the beginning until CPR)min (from the beginning until
CPR)DDuration to spontaneous circulationuration to spontaneous
circulation 60 60 minmin
CComa, GCS
-
8/7/2019 Presentation TCT Washington 2
23/28
HYPOTERMIA CONTRAINDICATIONSHYPOTERMIA CONTRAINDICATIONS
HHaemodinamic instabilityaemodinamic instability
RRecurrent or refractory VF or VTecurrent or refractory VF or
VT
HHaemorrhageaemorrhage
RRefractory hypoxiaefractory hypoxia
OOther:ther: unwitnessed arrest,unwitnessed arrest, coma of
other coma of other etiology, head trauma, operation before
14etiology, head trauma, operation before 14days, terminal illnes,
pregnancy, sepsis,days, terminal illnes, pregnancy, sepsis,burns,
sickle cell anemiaburns, sickle cell anemia
-
8/7/2019 Presentation TCT Washington 2
24/28
HYPOTERMIA RELATIVEHYPOTERMIA RELATIVE
CONTRAINDICATIONSCONTRAINDICATIONS
CCoagulopathy: INR > 2, trc < 50 000, APTToagulopathy: INR
> 2, trc < 50 000, APTT
> 65, cryoglobulinaemia, Raynaud sy> 65,
cryoglobulinaemia, Raynaud sy
H ypothermia is not contraindicated in PCI H ypothermia is not
contraindicated in PCI and thrombolysis for AMI and thrombolysis
for AMI
-
8/7/2019 Presentation TCT Washington 2
25/28
DILEMMASDILEMMAS
ShouldShould all or selected cardiac arrestall or selected
cardiac arrestpatients undergo PPCIpatients undergo PPCI ? ? --
unwitnessedunwitnessedcardiac arrest (poor predictor of
survival)cardiac arrest (poor predictor of survival)
PCI before or after neurologicalPCI before or after
neurologicalexamination?examination? - - waist of time?waist of
time?Hypothermia before or after PCI?Hypothermia before or after
PCI?
AAntiplatlet and antithrombotic therapy, GPntiplatlet and
antithrombotic therapy, GP
IIb/IIIa in prolonged CPR and hypothermia?IIb/IIIa in prolonged
CPR and hypothermia?
-
8/7/2019 Presentation TCT Washington 2
26/28
THINK ABOUTTHINK ABOUT
CComplications after prolonged CPR are notomplications after
prolonged CPR are notrare (sternal or rib fractures,rare (sternal
or rib fractures,hematothorax, pneumothorax.....)hematothorax,
pneumothorax.....)
HHypothermia and bleeding complicationsypothermia and bleeding
complications(coagulopathy(coagulopathy- - platlet count,
platletplatlet count, platletfunction, kinetics of clotting enzymes
andfunction, kinetics of clotting enzymes andplasminogen activator
inhibitors...)plasminogen activator inhibitors...)
Other hypothermia complicationsOther hypothermia complications-
-arrhythmias, sepsis, hyperglycemia...arrhythmias, sepsis,
hyperglycemia...
-
8/7/2019 Presentation TCT Washington 2
27/28
TREATMENT OPTIONSTREATMENT OPTIONS
ECMO (ExtraCorporeal MembraneECMO (ExtraCorporeal
MembraneOxygenation) in cardiac arrestOxygenation) in cardiac
arrest
PProtocolrotocol CPR, ECMO, IABP, PPCI,CPR, ECMO, IABP,
PPCI,hypothermiahypothermiaNew studiesNew studies- -CHEER
(refractory out of CHEER (refractory out of hospital cardiac arrest
treated withhospital cardiac arrest treated withmehanical CPR,
Hypothermia, ECMO andmehanical CPR, Hypothermia, ECMO andEarlyEarly
RReperfusion)eperfusion)
New guidelines 2010New guidelines 2010
-
8/7/2019 Presentation TCT Washington 2
28/28
Thank you for your attention