Embed Size (px)
Citation preview

Prehospital Cardiopulmonary Resuscitation of the Critically
Injured Patient
Michael K. Copass, MD, Seattle, Washington
Michael R. Oreskovich, MD, Seattle, Washington
Mark R. Bladergroen, MD, Seattle, Washington
C. James Carrico, MD, Seattle, Washington
As the concept that care of the injured should be re- gionalized to specific trauma centers has become more accepted, attention has shifted to that segment of care provided in the prehospital setting. Unfor- tunately, considerable controversy has developed regarding appropriate management of the victim before arrival at the trauma center. The pendulum has shifted away from a concept of “field stabiliza- tion” toward “scoop and run.” Although the impor- tance of rapid transport can not be overemphasized, the data that support this concept to the exclusion of attempts at establishing an airway or intravenous lines is circumstantial at best. More importantly, what effect a particular paramedic system has on the mortality rate for various injuries is only now being reported in various publications. The purpose of the present study was to review the experience of the paramedic system where interventions were reserved for trauma victims in cardiopulmonary arrest.
Material and Methods
In 1969, the City of Seattle Fire Department established the Medic One program. Before that time, emergency care in the City of Seattle was provided by first-aid trained ambulance attendants and Seattle firemen who did not have advanced life support training. Now, Seattle Fire Department paramedics have 2,000 hours of classroom and laboratory training, 40 percent of which is devoted to the principles of management of the multiply injured patient. They are experienced in the mechanical and physiologic care of trauma victims, including endotracheal intubation, intravenous cannulation, pleural decompression, fracture
From the University of Washington School of Medicine, Department of Surgery, Harborview Medical Center, Seattle, Washington.
Requests for reprints should be addressed to Michael R. Oreskovich. MD, Harborview Medical Center, 325 9th Avenue, Seattle, Washington 98104.
Presented at the 55th Annual Meeting of the Pacific Coast Surgical As- sociation, Newport Beach, California, February 19-22, 1984.
and spine stabilization, and cardiopulmonary resuscitation. All paramedic activities are supervised by a single physi- cian. The paramedic unit in the field is in direct radio contact with the trauma center. In addition, stringent physician review is conducted within 24 hours of all para- medic activity. Cardiopulmonary resuscitation is instituted for those trauma victims who are pulseless or do not have an auscultable blood pressure. However, it is carried out in conjunction with an attempt to place an endotracheal tube and two 14 gauge cannulas for intravenous adminis- tration of fluids.
Over a 3 year period, all patients who were trauma vic- tims and required cardiopulmonary resuscitation were identified. The mechanism of injury and body regions in- volved were recorded. The injury severity score was com- puted using the basic technique of Baker and the modifi- cations of Champion and Sacco. In all circumstances, the intravenous fluid that was administered was lactated Ringer’s solution. All patients who required intravenous lines for resuscitation had a blood sample drawn for typing and cross matching. The vital signs on arrival of the para- medic unit and on disposition of the patient at the emer- gency room were recorded so that change in vital signs could be plotted against the interval of time. The indication for and duration of cardiopulmonary resuscitation were carefully detailed as was the total transport time. Imme- diately on arrival in the emergency room, arterial blood gases were drawn. Finally, the operative procedures were performed, and the outcome in the patients and their re- turn to prehospital function were analyzed.
Results
Over a 3 year period, the same paramedic system transported 5,761 injured patients to the same trauma center. This excluded any transports by ro- tary wing or fixed wing aircraft and excluded trans- ports other than those by prehospital personnel with the same level of training. One hundred thirty-one of these patients required cardiopulmonary resus- citation (Table I). The analysis compared surviving
20 The American Journal ol Surgwy

Cardiopulmonary Resuscitation for Trauma
TABLE I ldentlfying Characteristics
Surviving Nonsurviving Patients Patients D Value
Patients (n) Mean age Sex
(male to female) Mechanism
Blunt injury Penetrating injury
Multiple injuries ISS
ISS = injury severity score; NS = not significant.
30 101 28 34 NS
2:l 2:l
12 (40%) 95 (95%) <O.Ol 18 (60%) 6 (6%) <O.Ol 20 (67%) 70 (70%) NS 32 28 NS
patients with nonsurviving patients. Both groups were equally young with an age range of 2 to 79 years. The difference in mean values between the survivors and nonsurvivors was not statistically significant. The sex ratio of male to female patients was equal in the two groups. Of significant difference was the fact that 60 percent of the surviving patients had sus- tained penetrating injuries whereas 95 percent of the nonsurviving patients had blunt injuries. When grouped according to multiplicity of injuries for various body regions, the incidences were almost identical. This helps explain the fact that the injury severity scores were very similar in both groups. As far as the identifying characteristics were concerned, the major difference in the two groups was the mechanism by which they were injured.
The analysis was extended to those factors that involved prehoepital care to see if the survivors could be separated from the nonsurvivors (Table II). Since it appears that once a trauma patient has arrested, the injury severity score does not predict survival, the various mechanisms of intervention were analyzed.
Twenty-nine out of 30 surviving patients had successful placement of an endotracheal tube. This was true of only two thirds of the nonsurviving pa- tients. Esophagel obturator airways were not used during this interval of time. At least two intravenous lines were placed in the antecubital fossa in all of the
TABLE II Prehospital Care
surviving patients. This was true of only 70 percent of the nonsurviving patients. Lactated Ringer’s so- lution was the choice in all circumstances. No patient received colloid or blood products in a prehospital setting. Although the surviving patients received 2,200 ml of lactated Ringer’s solution and the non- surviving patients received 2,800 ml, this difference was not statistically significant. Transport time was interpreted as the moment from arrival of the para- medic unit to arrival of the patient in the emergency room. The times were virtually identical in the two groups. Cardiopulmonary resuscitation lasted a mean duration of 12 minutes in the surviving patients but nearly 28 minutes in the nonsurviving patients. The duration of cardiopulmonary resuscitation exceeded the transport time in the nonsurviving patients be- cause in many circumstances emergency medical technician personnel or citizen bystanders had ini- tiated cardiopulmonary resuscitation before the ar- rival of the paramedic unit. The pH in Table II re- flected the first set of arterial blood gas values ob- tained in the emergency room. Under most circum- stances, these were obtained within 5 minutes of the patient’s arrival. Although the pH was 7.30 in the surviving patients versus 7.15 in the nonsurviving patients, the degrees of metabolic acidosis were not significantly different.
In an effort to measure improvement of perfusion
Surviving Nonsurviving Patients Patients
Patients (n) 30 101 ET tube 29 (97%) 66 (65%) IV lines (2) 30 (100%) 70 (70%) IV fluid (ml) 2,200 2,800 Transport 22 20
time (min) Duration of CPR 12 28
PH 7.30 7.15
CPR = cardiopulmonary resuscitation; ET = endotracheal; IV = intravenous; NS = not significant.
p Value
<O.Ol <O.Ol
NS NS
<O.Ol NS
V&me 148, July 1984 21

Copass et al
130 120
110 100
Syttollc go Blood 80
Press&Ire ,O (mean and 80
rww) 50 40 30 20 10
0 1
T
! p=Qo1
I
Field Emergency Room
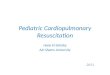
Figure 1. Relaffonshfp befween swvivlng patient’s sysfogc Mood pressures (mm Hg) upon arrival of fhe paramedic unit and upon arrival in the emergency room as measured in the field and upon arrival at the trauma cenfer.
in the surviving patients, the initial systolic blood pressure on arrival of the paramedic unit was plotted as the means and the ranges in the field and in the emergency room (Figure 1). The improvement in the mean blood pressure from 20 mm Hg to 90 mm Hg was a very significant observation.
Thirteen of the 30 surviving patients had cardiac injury (Table III). Eleven of the 30 had stab wounds or gunshot wounds to the heart and 2 had blunt car- diac rupture. Four additional patients had injury to the thoracic aorta, including two patients with blunt thoracic aortic rupture. There were also penetrating injuries to the trachea or lung in six additional pa- tients. Twenty-three of 30 patients had injury to the chest which, in most circumstances, was a penetrat- ing injury. Although emergency thoracotomy was necessary in most of these patients, it was performed in the operating room in most circumstances.
Of the 30 surviving patients, 1 died in the intensive care unit on the fourth postoperative day. Twenty- nine patients were discharged. One patient who had initially sustained a self-inflicted gunshot wound to the chest was successful in her second suicide at- tempt 2 years later. Three patients had significant neurologic injury. This included one patient who was both hemiplegic and blind, one who remains in a nursing home because of anoxic encephalopathy, and one who is a functional paraplegic. Twenty-five pa- tients returned to their prehospitalization significant gainful activities. However, within the follow-up period that ranged from 1 to 4 years, two required additional operations. One stab wound to the heart developed a hemodynamically significant ventricu- loseptal defect and the patient had to undergo open heart surgery, and another patient underwent an exploratory laparotomy for lysis of adhesions 3 years after initial operation for a small bowel obstruc- tion.
TABLE III Survivors: Major Organ Injury
Site of Injury
Heart Thoracic aorta Trachea Lung Liver Pancreas Spleen Hepatic vein Inferior vena cava
Total
Patients
0.0
13 4 3 3 2 2 1 1 1
30
Comments
At the 42nd Annual Session of the American As- sociation for the Surgery of Trauma, a special panel was assembled to address the issue of “Prehospital Trauma Care-Stabilize or Scoop and Run?” [I]. The request for the panel arose from a legitimate concern on the part of some of the members of the American Association for the Surgery of Trauma that major errors had occurred in the extension of ad- vanced life support services to trauma patients.
While participating in the panel and reviewing the experience from San Francisco General Hospital, Lewis stated that in an urban environment, when the time to the nearest hospital is 5 to 10 minutes, it is extremely doubtful that paramedic services will be beneficial. He also reviewed the experience from the South Carolina emergency medical service system that the average time for starting intravenous lines is 10 to 12 minutes after injury occurs, and where that time exceeds the transport time to the hospital, the paramedic system is clearly deleterious instead of beneficial to the patient.
A few recent studies appear to support that opin- ion. Gervin and Fischer [2] reviewed the importance of prompt transport in salvage of patients with pen- etrating heart wounds. Their retrospective study compared patients promptly transported with min- imal therapy after penetrating cardiac injuries with patients in whom prolonged attempts at stabilization had been made in the field. Fifty-six percent of their patients were alive at the time of ambulance arrival with a systolic blood pressure of greater than 90 mm Hg. All patients were injured within 10 minutes of transport time from their institution. Among the group in which they judged the injury to be salvaga- ble, the statement was made that a salvage rate of 80 percent was achieved if transport delays were mini- mized. However, there were only six patients in the scoop and run group and seven patients in the sta- bilization in the field group. In addition to the sample size being small in the respective groups such that statistical significance could not be analyzed, no record was made of whether or not attempts at en-
22 The American Journal of Surgery

Cardiopulmonary Resuscitation for Trauma
dotracheal intubation, placement of intravenous lines, or closed chest massage had an impact on the stabilization in the field group. The researchers identified a specific type of injury in which rapid transport to the hospital seemed most appropriate. Additional extrapolations about various therapeutic interventions are difficult to make.
Shimazu and Shatney [3] presented their experi- ence with 267 patients who had sustained cardio- pulmonary arrest after trauma. The long-term sur- vival rate was 2.6 percent, and only 1.5 percent of the patients became functional. The majority of the pa- tients (91 percent) were brought by helicopter di- rectly to the Maryland Institute of Emergency Medical Services from the scene of the accident. However, the average interval between the time of the accident and the arrival of the patient at the trauma center was 1 hour. In addition, the prehos- pita1 care was provided by emergency technicians, but data regarding the establishment of an airway and placement of intravenous lines was not reported. Statements relative to the appropriateness of pre- hospital care could not be made from this study. Rather it emphasized what can be anticipated when trauma patients present “dead on arrival” to the trauma center.
Jacobs and co-workers [4] from the Boston City Hospital analyzed the benefits of prehospital ad- vanced life support in trauma patients. Their study concluded that the trauma score on arrival at the hospital increased significantly more for patients who received advanced life support care than for patients transported by basic life support ambulances. Ad- vanced life support resuscitation had the most in- fluence on patients with trauma scores of 4 to 13 and did not delay transport time. In addition, a positive change in the prehospital trauma score was signifi- cantly related to an increased chance of long-term survival for any given severity of injury. Unfortu- nately, the average trauma score for the total group of patients was 13 which represents only a moderate degree of severity of injury. Of note is the fact that in patients with a trauma score of 1 to 3, the mortality rate was 96 percent. This is clearly the group of pa- tients in whom endotracheal intubation, intravenous lines, and rapid transport should have had the biggest impact. Because of the high mortality in this group, such an analysis was not possible, and the study was not suitable for any conclusion to be drawn.
Recently Smith and co-workers [5] from the Uni- versity of California at Davis, presented their data at the 43rd Annual Meeting of the American Asso- ciation for the Surgery of Trauma. They reviewed 52 consecutive trauma cases in which the patient had a blood presure of less than 100 mm Hg in the field or on arrival at the hospital. The researchers analyzed the time taken for establishment of intravenous lines versus the time taken for hospital transport. From their analysis they concluded that seriously injured,
hypovolemic patients should not have resuscitative efforts at the scene but should be subject to an au- tomatic “load and go” protocol. They stated that it was not proved that starting intravenous lines at the scene increased survival and that patients should be intubated by way of the endotracheal route, external bleeding should be controlled by pressure, and transport should begin at once. Unfortunately, in this group of patients, the usual device for establishment of an airway was the esophageal obturator. The role of endotracheal intubation in the resuscitation was not addressed.
Of note is the fact that in all three patient groups the time to establish an intravenous line exceeded the time to transport the patient to the hospital. It would appear that in emergency medical service systems where this duration is necessary to establish a route for administration of intravenous fluids that trans- port to a trauma center instead would appear to be a logical conclusion.
The purpose of the present study was to attempt to bring clarity to the issues that were faced by the panel in 1983. Our goal was to analyze the results of prehospital intervention in a group of patients who were in cardiac arrest on arrival of the paramedic unit. In 131 patients, endotracheal intubation, in- travenous lines, and cardiopulmonary resuscitation were instituted in conjunction with rapid transport to the trauma center. We chose this critically injured group of patients, recognizing that a successful in- tervention could be life saving and that the outcome without intervention was predictable. The fact that the injury severity score did not predict survival among this group of patients was not surprising. Once a patient has sustained cardiac arrest, be it due to a gunshot wound to a major blood vessel or to a mul- tiplicity of blunt injuries, the event should be con- sidered a terminal one, and it is appropriate that the injury severity score not apply. However, the sur- viving patients were clearly separated by having a tenfold higher incidence of penetrating injury. This serves to emphasize the fact that the prehospital care system is a prelude to appropriate surgical follow- through. In one instance, by being able to report that a patient had sustained a penetrating injury to the thorax, the operating team at the trauma center was able to be prepared to follow through with appro- priate hemostatic measures on the patient’s arrival. This observation supports the role of rapid transport reported in the previous studies. The observation of the difference in penetrating trauma between the surviving and nonsurviving patients was not repro- ducible in the study from Kino Community Hospital by Gervin and Fischer [2] but was quite consistent with previous reports in the literature.
To date, most investigators have emphasized the need for establishment of an airway. The group from Sacramento has shown that the esophageal obturator airway is not an adequate substitute [6,7]. Estab-
Volume 148,July 1994 23

Copass et al
lishment of such an airway has not been a therapeutic intervention taught during the Medic One program. All surviving patients except one had successful placement of an endotracheal tube, and a third of the nonsurviving patients had attempts at endotracheal intubation that were unsuccessful. This difference in therapeutic intervention was statistically signifi- cant. Because 23 of these 30 surviving patients had injuries that involved the thorax, the role that the endotracheal tube may have played in their survival was probably further enhanced.
It was possible to place two 14 gauge intravenous lines in the antecubital fossa in all of the surviving patients. In 30 percent of the nonsurviving patients, these attempts were unsuccessful. Unfortunately, the time for placement of the intravenous lines was not recorded, but from a retrospective review of the records an appropriate extrapolation would be that it was much less than the 10 to 15 minutes that had been reported by the emergency medical service group from South Carolina. Within an average of 22 minutes, surviving patients had placement of an endotracheal tube, two intravenous lines, were po- sitioned on a backboard, and they arrived at the trauma center.
The range of administration of intravenous fluids in the surviving patients was 900 to 3,700 ml. This serves to answer the concerns expressed by Border et al [I], that in the urban setting, the transport time is short enough that adequate fluid cannot be ad- ministered to counteract the effect of severe hem- orrhage. Even recognizing that as little as a third of the lactated Ringer’s solution may remain in the in- travascular circulation the patients were receiving restoration of as much as 20 percent of their blood volume by this crystalloid solution.
The difference in transport times between the two groups was virtually nonexistent. Transport time was interpreted as the time from arrival of the paramedic staffed unit at the scene to arrival of the patient at the trauma center. It incorporated time for all ther- apeutic interventions. Of note is the fact that within the average radius of transportation of these patients, the transport time could not have been less than 12 to 15 minutes. At best, the three aforementioned therapeutic interventions added 6 to 7 minutes to the transport time. All of the surviving patients required cardiopulmonary resuscitation. All but one were in arrest on arrival of the medic unit. The fact that the duration of cardiopulmonary resuscitation in the nonsurviving patients exceeded that of the transport time is representative of the fact that the first re- sponding unit was usually doing cardiopulmonary resuscitation before arrival of the paramedic unit. Arterial blood gas measurements were taken from all victims within 5 minutes of arrival in the emergency room. Although virtually all patients had some de- gree of acidosis, the acidosis was usually metabolic in origin and not respiratory. This was probably re-
lated to the degree of blood loss that they had as opposed to inadequate ventilation by the endotra- cheal route. Two thirds of the surviving patients had a major organ injury that was intrathoracic. In most of these patients it was a penetrating injury. The success among the surviving patients is probably attributable to the fact that they had lesions that were surgically salvagable. This included 11 stab wounds to the heart and 2 blunt cardiac ruptures which were rapidly diagnosed and treated. In addi- tion, there were four injuries of the thoracic aorta which were surgically corrected and three penetra- tions of the trachea which were repaired. The fact that this is the group that is most likely to benefit from rapid transport and emergency thoracotomy has been reported a number of times in the literature 101.
The purpose of the presentation of these data was to express a concern that the pendulum may have swung too far away from any form of prehospital in- tervention toward complete scoop and run to the detriment of a group of patients that may clearly benefit from certain prehospital interventions. Clearly, the patient who is a matter of a few minutes away from the trauma center and who has pene- trating injury to the chest, might best be served by a scoop and run system. However, there are entirely other categories of patients that require certain in- terventions. For example, the patient with an isolated head injury who is apneic may not need placement of intravenous lines but successful establishment of an endotracheal tube may be life saving. The patient who is more than 15 minutes from a trauma center may benefit not only from the endotracheal tube but also from instillation of crystalloid solution if the cannula can be rapidly placed. The patient with an unstable pelvic fracture may benefit from application of MAST@ trousers.
Hopefully, what this review of a 3 year experience with trauma patients transported by the same emergency medical service system serves is to point out the need for a uniform system with stringent medical control and the ability to individualize the prehospital plan to the particular patient. The Seattle system supports scoop and run when the patient is close to the trauma center and has pene- trating thoracic trauma. The number and degree of interventions escalate where the transport time in- creases and the injuries are more likely to be mul- tiple.
Summary
Prehospital cardiopulmonary resuscitation com- bined with endotracheal intubation, vigorous fluid resuscitation, and rapid transport can be effective in resuscitating trauma patients in cardiopulmonary arrest. Survival does not correlate with the injury severity score or transport time once the patient has arrested but does correlate with the mechanism of
24 The American Journal of Surgery

Cardiopulmonary Resuscitation for Trauma
injury, endotracheal intubation, and placement of intravenous lines.
References
1. Border JR, Lewis FR, Aprahamian C, Halier JA, Jacobs LM, LU- tematl A. Panel: prehospital trauma care-stabilize or scoop and run. J Trauma 1983;23:708-11.
2. Gervin AS, Fischer RP. The importance of prompt transport in salvage of patients with penetrating heart wounds. J Trauma 1982;22:443-8.
3. Shimazu S, Shatney Cl-i. Outcomes of trauma patients with no vital signs on hospital admission. J Trauma 1983;213-8.
4. Jacobs LM, Sinclair A, Beiser A, D’Agostino RB. Prehospital advanced life support: benefits in trauma. J Trauma 1984; 24~8-13.
5. Smith JP, Bodai BI, Hill AS, Frey CF. Prehospitai stabilization of critically injured patients: a failed concept. (abstr) J Trauma 1983;23:666.
6. Smith JP, Bodai Bi, Seifkin A, Paider S, Thomas V. The esoph- ageal obturator airway: a review. JAMA 1983;250:1081-4.
7. Smith JP, Bodai Bi, Aubourg R, Ward RE. A field evaluation of the esophageal obturator airway. J Trauma 1983;23:317- 21.
8. Baker CC, Thomas AN, Trunkey DD. The role of emergency room thoracotomy in trauma. J Trauma 1980;20:848-55.
9. Harnar TJ, Oreskovich MR, Copass MK, Heimbach DM, Herman CH, Carrico CJ. Role of emergency thoracotomy in the re- suscitation of moribund trauma victims: 100 consecutive cases. Am J Surg 1981;142:92-9.
Discussion
Charles F. Frey (Sacramento, CA): We recently pre- sented a paper entitled “Pre-hospital Stabilization of the Critically Injured Patient, A Failed Concept,” before the American Association for the Surgery of Trauma. We made the point that when the time to transport the patient to the hospital is less than the time it takes to start an intravenous line, somewhere from 8 to 12 minutes, a load and go phi- losophy should be pursued because the amount of fluid that can be given to a patient who is bleeding rapidly is often less than that which is lost. An average volume of 2,000 ml of fluid was given in this study, only a third of which stayed in the intravascular space, which is not suf- ficient to replace the fluid loss in these patients if they arrested from hypovolemia. An arrest from hypovolemia means the fluid lost must exceed more than half the pa- tient’s blood volume to leave the patient without vital signs. Perhaps the work with hypertonic saline solution which Dr. Holcroft at our institution is pursuing might permit a much greater volume repletion effect with a smaller volume of fluid and may be of some future benefit in the resuscitation of the hypovolemic patient.
We also believe it is important to establish an airway before transport, a point which the authors have very well documented. For longer transport times of more than 8 to 12 minutes, an intravenous line should be established, al- though we would prefer that this be performed en route rather than delaying at the scene of the injury. In the fu- ture, placement of intravenous lines en route in the vehicle will become technically more feasible. Vans constructed in Europe now are much smoother riding and permit the institution of procedures en route, whereas it is more dif- ficult in the type of vans that we now have. Dr. Carrico, were the survivors and nonsurvivors comparable groups aside from whether an airway was established? The non- survivors apparently were often receiving cardiopulmonary
resuscitation by bystanders before the arrival of the paramedics and presumably were in shock for a longer period of time than survivors were before endotracheal intubation and fluid administration. How many of the survivors who suffered an arrest suffered more from res- piratory insufficiency than hypovolemia? The dramatic effect of endotracheal intubation in your survivors leads me to believe you were treating respiratory rather than hypovolemic arrest.
I find the authors’ philosophy of individualizing the prehospital management of the injured patient based on the time interval from arrival at the site of injury to arrival at the trauma center a theme worth pursuing.
Donald D. Trunkey (San Francisco, CA): I rise to em- phasize one point that was brought out in the manuscript. One of the best features of the Seattle system is medical control. I want to emphasize this because the surgeons and the physicians in Seattle still control their paramedic system. This is quite different from what occurs in most communities.
The question that I have relates to cost. The authors have shown that, with medical arrest, the paramedic probably is best off doing blind defibrillation. Electrome- chanical dissociation and asystole have such miserable outcomes that it really makes no difference if the para- medic can read the electrocardiogram. Blind defibrillation is perfectly acceptable. The other’paramedic intervention that the medical arrest requires is an intravenous line to administer the medications to control the dysrhythmia if it continues to be a problem. This leads up to my question. Dr. Carrico, is it worthwhile to train paramedics for 2,000 hours? Is it worthwhile to have that extra expense to train for that long? Would it not be better to just train these people in endotracheal intubation, intravenous skills, protection of the spine, and splint techniques en route to the hospital? It certainly wouldn’t require 2,000 hours. What is the ideal amount of time these people should be trained in, and what are the cost trade-offs?
Richard M. Peters (San Diego, CA): I would like to suggest that there is physiologic evidence that supports the importance of intubation and ventilation of these patients. A patient who has hypovolemic shock or a low cardiac output is more likely to have respiratory arrest as the fatal occurrence rather than cardiac arrest. This has been doc- umented by Dr. Macklin’s group in Montreal who showed that, in effect, these patients have inadequate blood supply to their respiratory muscles with their hypovolemia. Therefore, they fatigue their respiratory muscles and have a central respiratory arrest before they have a cardiac ar- rest. I think this is a very important additional reason for the point that putting an endotracheal tube in and venti- lating these patients is more likely to stop arrest than anything else. When a patient has a low cardiac output, he will arrest his respiration because he has inadequate blood supply to the respiratory muscles.
C. James Carrico (closing): Dr. Copass is a major force in the Seattle system. It is a type of paramilitary system with a boss. It is clear that physician control is one of the most crucial parts of any system such as this. For the population of Seattle, there are small numbers of para- medic units. They are supported by emergency medical technicians on fire engines and by medical aid units which
Volume 149, July 1994 25

Copass et al
provide emergency medical technician delivery virtually always within 3 minutes. This has numerous benefits, most of all economic. One pays a tenth as many paramedics. Another benefit is training; it becomes cost-effective to provide the trainee with extensive training for all the things you ask them to do, such as dealing with cardiac arrest, trauma, poisoning, and so on. A crucial point is that, with our system, the paramedics are able to maintain their ex- perience at a very high level because the group of selected people are continually doing, being critiqued, and keeping their experience high.
Our goal was to evaluate people who had arrest at the scene. To achieve that, the run reports were checked on which the paramedics had indicated “cardiopulmonary resuscitation started immediately.” The requirements for cardiopulmonary resuscitation are that the patient be pulseless or have no auscultable blood pressure. Of the 30 surviving patients, 25 had no auscultable blood pressure, no pulse, and therefore, no palpable blood pressure. There were four patients who had no audible blood pressure but had a palpable blood pressure at 40 mm Hg, 20 mm Hg, 20 mm Hg, and 10 mm Hg. The remaining patient had a blood pressure of 70 mm Hg on arrival and arrested immediately after arrival of the paramedics. Of the 30 surviving patients, there was 1 who was not already in arrest by our definition when the paramedics got there.
The cardiopulmonary resuscitation time was much shorter in the surviving patients because a significant number of these people were successfully resuscitated en route and were out of arrest when they arrived at the hos- pital. Regarding the nonsurviving patients in this group, we all now try to find if we can identify people who the system hurt, who were alive when the paramedics got there and subsequently arrested, perhaps because the para- medics delayed too long. Since the 1980 data have not been entered into a computer, finding these data is not easy. At
this point, there are less than five patients in the nonsur- vivor group who had any blood pressure on arrival, so the number who arrested after the paramedics arrived was very small.
Approximately 95 percent of the nonsurviving patients had blunt injury. The primary cause of death in that group of patients was massive head injury. There were two people who had massive hepatic vein disruption from the vena cava, and for them, more rapid transportation to the hos- pital might have made a difference. We found no nonsur- vivor with a single repairable organ injury. One major point regarding possible delays is that the difference in transport time between the surviving and nonsurviving patients was 2 minutes, with the nonsurviving patients having shorter transport time. The other is that the average travel time from the scene to the hospital was 14 minutes. Thus, there was a maximum of 6 minutes of stabilization time for the nonsurviving patients. According to Dr. Copass’s surveys, it takes 4 minutes to start an intravenous line.
I agree that endotracheal tube control of the airway is of prime importance and I agree with Dr. Peters that ade- quate airway control and ventilation are most important. We really don’t know whether intravenous fluids did much good, but remember, putting in an intravenous line allows the paramedics to send blood to the blood bank. Thus, we get type-specific blood sometimes as rapidly as the patient arrives at the hospital. We do see improvement in perfusion due to restoration of circulating volume. Also restoring ventilation may assist in this regard. I would quibble with Dr. Frey’s statement that when one gives 2 liters of Ringer’s solution to someone in shock, only a third of it stays in the intravascular circulation. That is true under normal cir- cumstances; however, the lower the hydrostatic pressure, the longer that fluid stays in the intravascular circulation. Thus, we may be doing more than we give ourselves credit for.
26 The American Journal of Suqery