Embed Size (px)
Citation preview
Predictors and Patterns of Recurrence afterResection of Hepatocellular CarcinomaCharles Cha, MD, Yuman Fong, MD, FACS, William R Jarnagin, MD, FACS, Leslie H Blumgart, MD, FACS,Ronald P DeMatteo, MD, FACS
BACKGROUND: The majority of patients with hepatocellular carcinoma (HCC) who undergo complete tumorresection subsequently develop tumor recurrence. The objectives of this study were to deter-mine the risk factors for recurrence of HCC after hepatectomy and to examine the outcomesonce tumor recurrence occurs.
STUDY DESIGN: From February 1990 to May 2001 a total of 164 patients underwent liver resection for HCC atour institution and were prospectively followed. Time to recurrence and survival after recur-rence were determined by Kaplan-Meier analysis. Patient, tumor, and treatment characteristicswere tested for their prognostic significance by univariate and multivariate analysis using thelogrank test and the Cox proportional hazards model, respectively.
RESULTS: The median patient age was 64 years (range 21 to 87 years) and 106 patients (65%) were male.After a median followup of 26 months, 90 patients (55%) have developed recurrent cancer.Among them, 75 patients (83%) had tumor detectable in the liver, which was the only site ofdisease in 67 (74%). In all, 15 patients (20%) had extrahepatic disease (7 lung, 4 peritoneum,2 pancreas, 1 bone, and 1 brain). The median time to recurrence was 24 months (range 1 to 274months). Predictors of recurrence on univariate analysis were tumor size greater than 5 cm,more than one tumor, cirrhosis, vascular invasion (microscopic or macroscopic), and tumorsatellites. On multivariate analysis only tumor size greater than 5 cm (p � 0.04) and vascularinvasion (p � 0.01) predicted recurrence. The median survival after recurrence was 11 months(range 0 to 60 months). Of the 90 patients who developed tumor recurrence 49 (67%) were ableto undergo additional ablative or surgical therapy (33 embolization, 9 ethanol injection, and 14re-resection). On multivariate analysis vascular invasion in the original tumor predicted poorsurvival after recurrence (p � 0.009).
CONCLUSIONS: The liver is the predominant site of first recurrence after resection of hepatocellular carcinoma,and once recurrence occurs survival is limited. The current study underscores the need foreffective adjuvant therapy for patients with HCC treated with partial hepatectomy. ( J Am CollSurg 2003;197:753–758. © 2003 by the American College of Surgeons)
Hepatocellular carcinoma (HCC) is one of the most com-mon types of cancer in the world, with an annual incidenceof approximately 1 million cases.1 Although HCC is muchless common in the United States compared with the rest ofthe world, its incidence has risen over the past decade and isnow reportedly as much as 75%.2,3 The reason for the in-crease is unclear but it may reflect a higher prevalence ofhepatitis in the Western world as well as improved detec-tion of the disease. The natural history of hepatocellular
cancer both in the West and in endemic areas is unfavor-able. The median survival in unresectable patients is lessthan 4 months.4,5 For the 13% to 35% of patients whoundergo resection,6,7 survival is approximately 25% to 40%at 5 years.8-18 The relative role of resection, ablation, andtransplantation for patients with HCC is currently a matterof considerable debate.19 The current study defines the pat-terns of recurrence after potentially curative resection ofHCC as well as postrecurrence survival. The results areuseful for the rational design of adjuvant therapy and theidentification of a patient subset at high risk for tumorrecurrence.
METHODSA total of 549 patients with the diagnosis of HCC wereevaluated by members of the Hepatobiliary Service at
No competing interests declared.
Received June 18, 2003; Accepted July 21, 2003.From the Hepatobiliary Service, Memorial Sloan-Kettering Cancer Center,New York, NY.Correspondence address: Ronald P DeMatteo, MD, Hepatobiliary Service,Memorial Sloan-Kettering Cancer Center, 1275 York Ave, New York, NY10021.
753© 2003 by the American College of Surgeons ISSN 1072-7515/03/$21.00Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2003.07.003
Memorial Sloan-Kettering Cancer Center between1990 and 2001 and were entered into a prospective da-tabase. There were 164 patients who underwent partialhepatectomy with complete gross resection of disease.Intraoperative ultrasonography was used routinely toevaluate the liver remnant for additional tumors. An-other 39 patients (19%) who were found to be unable toundergo resection at the time of abdominal explorationwere excluded from the present analysis. Postoperativelythe patients were prospectively followed with serial CTscans and determination of serologic �-fetoproteinlevels.
Resected liver specimens were fixed in 10% formalin,embedded in paraffin, and sectioned. Tumors were ex-amined for evidence of vascular invasion, satellitosis,neural invasion, and differentiation. Noncancerous liverparenchyma was inspected for evidence of cirrhosis. Vas-cular invasion included microscopic or gross invasion ofvessels. Survival rates were calculated by the Kaplan-Meier method, and comparisons were performed using
the log-rank test. Multivariate analysis was performedusing the Cox proportional hazards model (SPSS soft-ware version 10; SPSS Inc.). A p value of less than 0.05was considered to be statistically significant.
RESULTSPatient and tumor characteristicsThe clinicopathologic factors of the entire patient pop-ulation (n � 164) with resected HCC are shown in Ta-ble 1. There were 106 men (65%) and 58 women(35%). The median age at diagnosis was 64 years (range21 to 87 years). The racial distribution was 102 Cauca-sian patients (63%), 45 Asian (27%), 6 African-American (4%), 4 Hispanic (2%), and 7 not recorded(4%). There were 66 patients (40%) who had evidenceof cirrhosis at the time of resection. Among them 56patients (84%) were Child class A and the remaining 10(15%) were Child class B. Cirrhosis was associated withhepatitis B or C in 47 patients (71%) and with alcohol in10 patients (15%). The median number of tumors was 1(range 1 to 12 lesions) with multiple lesions occurring in59 patients (36%). The median tumor size of the dom-inant lesion was 10 cm (range 1 to 35 cm). Both lobes ofthe liver were involved in 61 patients (37%).
TreatmentThe types of liver resections are shown in Table 2. Themajority (85%) of patients required a hemihepatectomy,extended resection, or multiple segmental resections. Allgross cancer was removed with curative intent. Thepathologic margins of resection were free of microscopictumor in 151 patients (92%), although 37 patients(23%) had close (less than 0.5 cm) margins. Vascularinvasion was found in 80 patients (49%), 12 (7%) ofwhom had gross involvement of either the portal or he-patic veins. Perioperative mortality was 4% (7 of 164patients) with an overall complication rate of 20% (31 of164).
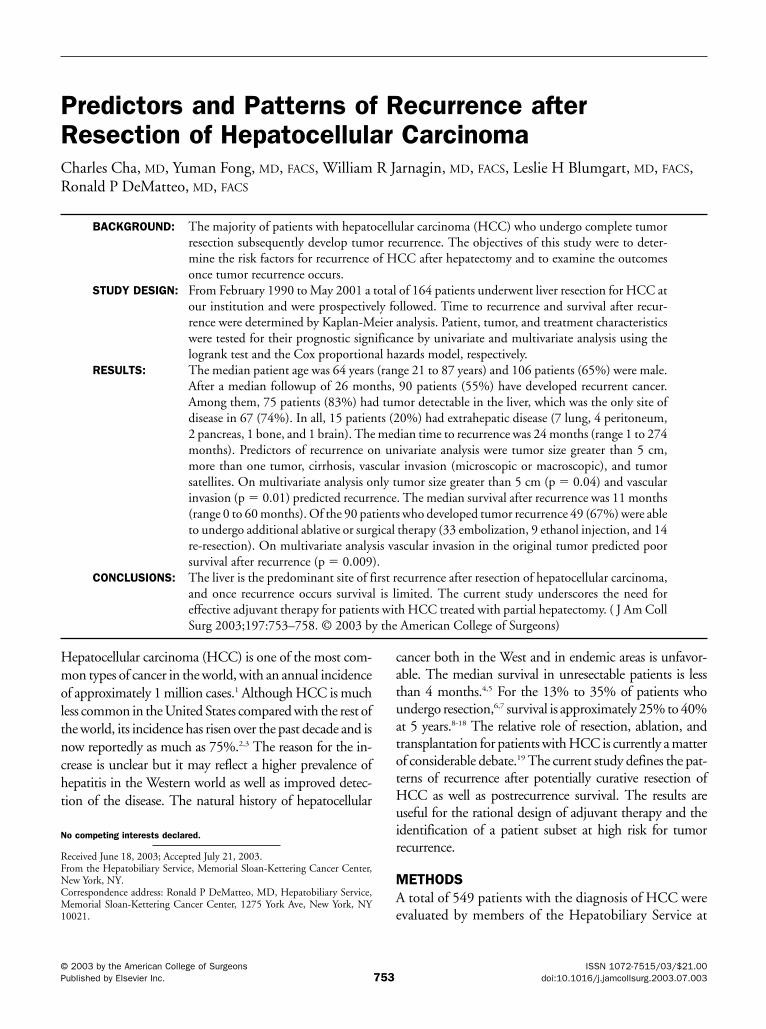
Recurrence and survivalAt a median followup of 26 months for survivors, recur-rence had developed in 90 patients (55%) (Fig. 1).Among them, 67 patients (74%) had recurrent diseaseisolated to the liver. Additional therapy was performedin 49 patients. There were 14 patients who underwentrepeat hepatectomy and 35 patients who underwent ar-terial embolization, radiofrequency ablation, or ethanol
Table 1. Summary of Patient and Tumor Characteristics(n � 164)Characteristic n %
Male 106 65Cirrhosis 66 40
Child class A 56 84Hepatits B/C 47 28EtOH 10 6
Multiple lesions 59 36Bilobar involvement 61 37Resection margin
Positive 13 8�0.5 cm 37 23
Vascular invasion 80 49Satellitosis 41 25Neural invasion 4 2Differentiation
Poor 33 20Moderate 73 44Well 38 23
Table 2. Hepatic Resections (n � 164)Resection n %
Wedge resection 6 4Segmentectomy 18 11Multiple segmentectomy 38 23Hemihepatectomy 40 24Extended hepatectomy 62 38
754 Cha et al Resection of Hepatocellular Carcinoma J Am Coll Surg
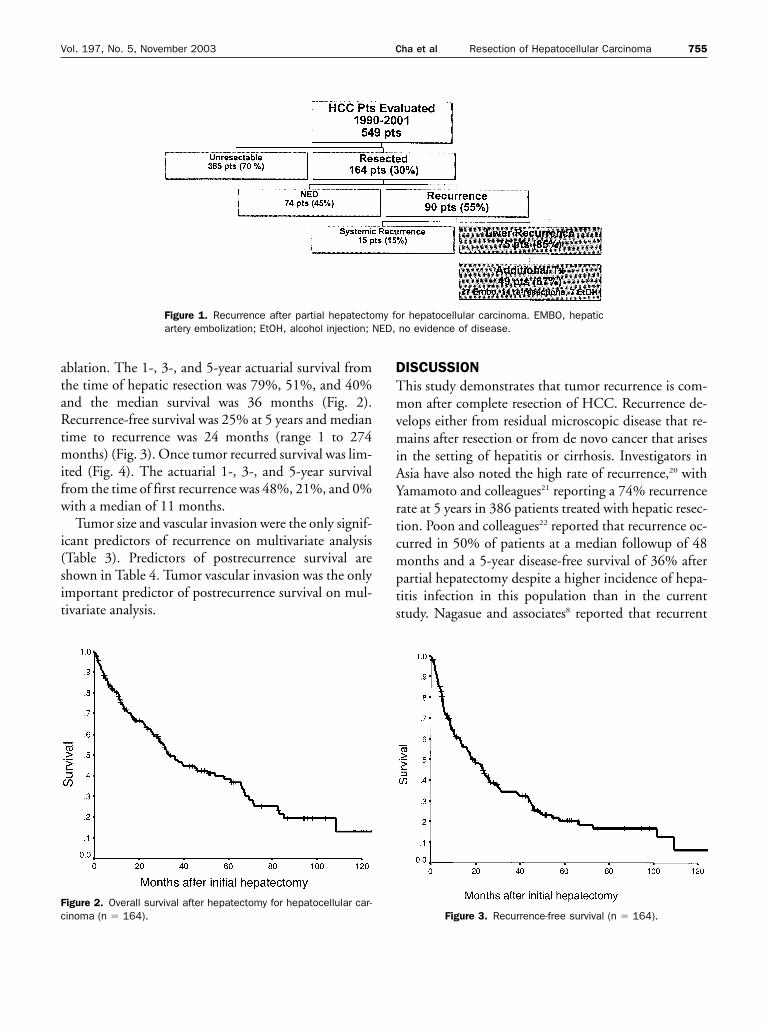
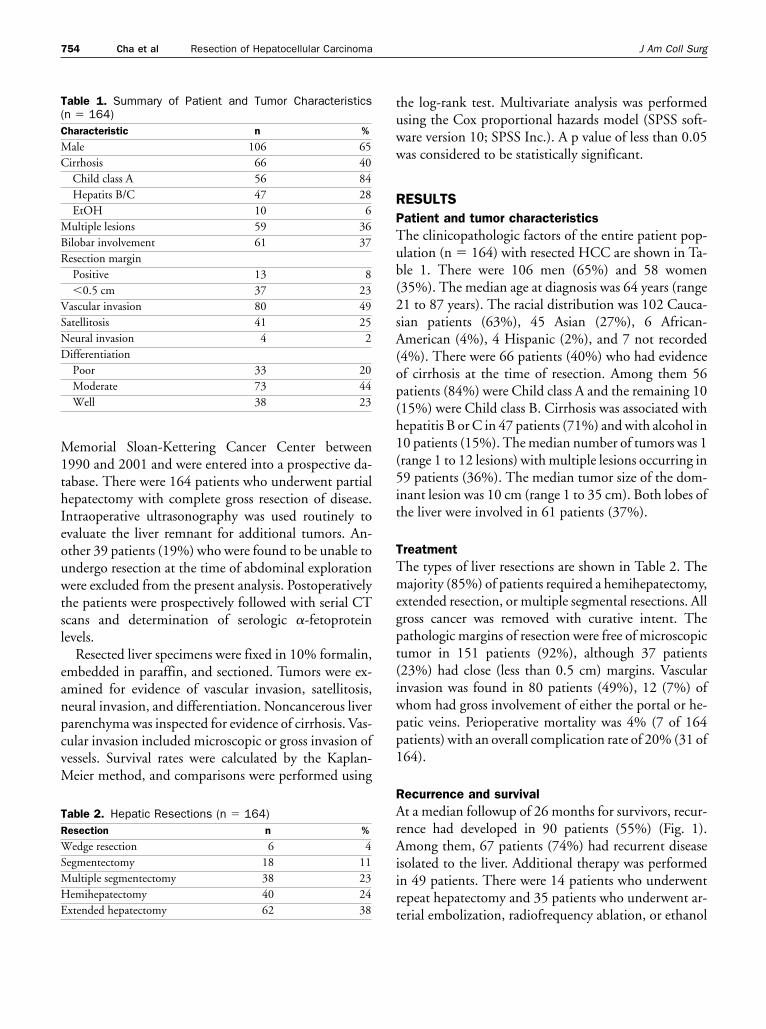
ablation. The 1-, 3-, and 5-year actuarial survival fromthe time of hepatic resection was 79%, 51%, and 40%and the median survival was 36 months (Fig. 2).Recurrence-free survival was 25% at 5 years and mediantime to recurrence was 24 months (range 1 to 274months) (Fig. 3). Once tumor recurred survival was lim-ited (Fig. 4). The actuarial 1-, 3-, and 5-year survivalfrom the time of first recurrence was 48%, 21%, and 0%with a median of 11 months.
Tumor size and vascular invasion were the only signif-icant predictors of recurrence on multivariate analysis(Table 3). Predictors of postrecurrence survival areshown in Table 4. Tumor vascular invasion was the onlyimportant predictor of postrecurrence survival on mul-tivariate analysis.
DISCUSSIONThis study demonstrates that tumor recurrence is com-mon after complete resection of HCC. Recurrence de-velops either from residual microscopic disease that re-mains after resection or from de novo cancer that arisesin the setting of hepatitis or cirrhosis. Investigators inAsia have also noted the high rate of recurrence,20 withYamamoto and colleagues21 reporting a 74% recurrencerate at 5 years in 386 patients treated with hepatic resec-tion. Poon and colleagues22 reported that recurrence oc-curred in 50% of patients at a median followup of 48months and a 5-year disease-free survival of 36% afterpartial hepatectomy despite a higher incidence of hepa-titis infection in this population than in the currentstudy. Nagasue and associates8 reported that recurrent
Figure 1. Recurrence after partial hepatectomy for hepatocellular carcinoma. EMBO, hepaticartery embolization; EtOH, alcohol injection; NED, no evidence of disease.
Figure 2. Overall survival after hepatectomy for hepatocellular car-cinoma (n � 164). Figure 3. Recurrence-free survival (n � 164).
755Vol. 197, No. 5, November 2003 Cha et al Resection of Hepatocellular Carcinoma
disease accounted for 60% of late deaths after partialhepatectomy with the remainder mostly from liver fail-ure or gastrointestinal hemorrhage. By contrast, in thecurrent study the vast majority of deaths occurring be-yond 3 years (87%) were from recurrent disease (20 of23 patients) and no death from progressive liver failurewas observed.
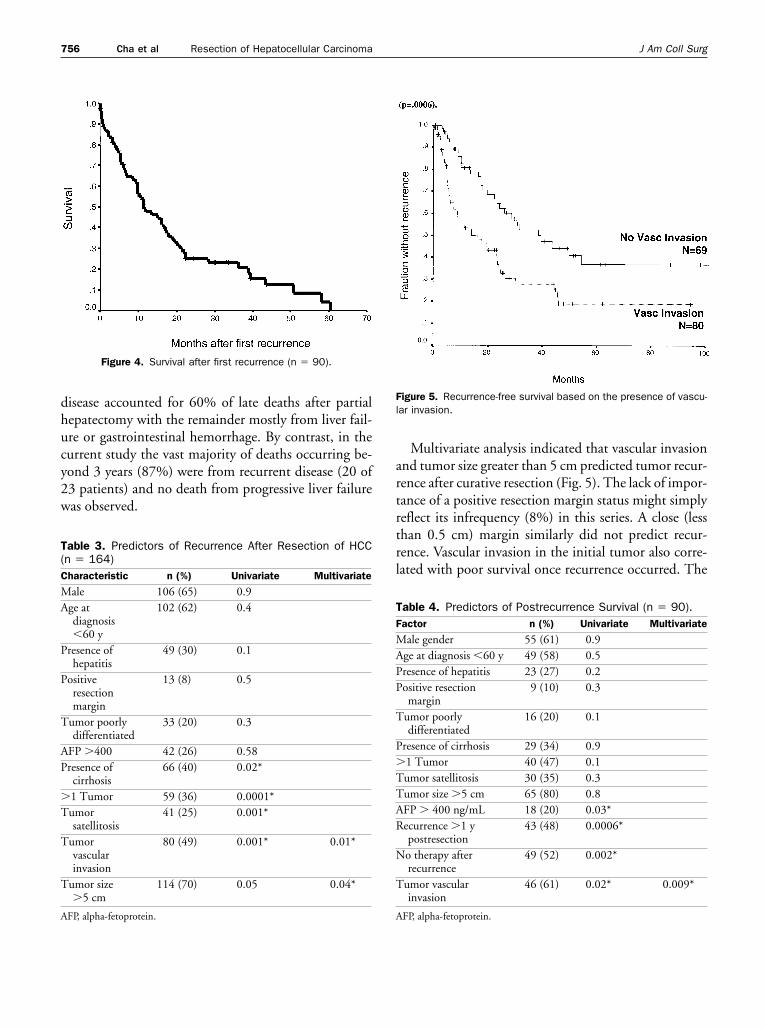
Multivariate analysis indicated that vascular invasionand tumor size greater than 5 cm predicted tumor recur-rence after curative resection (Fig. 5). The lack of impor-tance of a positive resection margin status might simplyreflect its infrequency (8%) in this series. A close (lessthan 0.5 cm) margin similarly did not predict recur-rence. Vascular invasion in the initial tumor also corre-lated with poor survival once recurrence occurred. The
Table 4. Predictors of Postrecurrence Survival (n � 90).Factor n (%) Univariate Multivariate
Male gender 55 (61) 0.9Age at diagnosis �60 y 49 (58) 0.5Presence of hepatitis 23 (27) 0.2Positive resection
margin9 (10) 0.3
Tumor poorlydifferentiated
16 (20) 0.1
Presence of cirrhosis 29 (34) 0.9�1 Tumor 40 (47) 0.1Tumor satellitosis 30 (35) 0.3Tumor size �5 cm 65 (80) 0.8AFP � 400 ng/mL 18 (20) 0.03*Recurrence �1 y
postresection43 (48) 0.0006*
No therapy afterrecurrence
49 (52) 0.002*
Tumor vascularinvasion
46 (61) 0.02* 0.009*
AFP, alpha-fetoprotein.
Figure 5. Recurrence-free survival based on the presence of vascu-lar invasion.
Figure 4. Survival after first recurrence (n � 90).
Table 3. Predictors of Recurrence After Resection of HCC(n � 164)Characteristic n (%) Univariate Multivariate
Male 106 (65) 0.9Age at
diagnosis�60 y
102 (62) 0.4
Presence ofhepatitis
49 (30) 0.1
Positiveresectionmargin
13 (8) 0.5
Tumor poorlydifferentiated
33 (20) 0.3
AFP �400 42 (26) 0.58Presence of
cirrhosis66 (40) 0.02*
�1 Tumor 59 (36) 0.0001*Tumor
satellitosis41 (25) 0.001*
Tumorvascularinvasion
80 (49) 0.001* 0.01*
Tumor size�5 cm
114 (70) 0.05 0.04*
AFP, alpha-fetoprotein.
756 Cha et al Resection of Hepatocellular Carcinoma J Am Coll Surg

identification of patients at high risk for recurrence afterpartial hepatectomy raises the question of whether thissubset of patients should receive additional therapy.Most patients with gross vascular invasion can be iden-tified preoperatively with radiologic imaging, but themajority of patients with vascular invasion have micro-scopic invasion and are identified only at pathologic ex-amination. In either case these patients would be treatedwith adjuvant chemotherapy if an effective option wereavailable. As another strategy some investigators are nowconsidering performing a prophylactic liver transplantfor patients with small tumors who are found to havevascular invasion after hepatic resection because of thehigh likelihood of subsequent tumor recurrence.
Once tumor recurrence developed an ablative or sur-gical procedure was performed in 67% of patients. Sur-vival was better in this subset than in the patients whodid not receive further treatment, but this is likely due topatient selection. Repeat hepatectomy was performed in16% of patients with recurrent disease and in patientswho had a repeat resection had a statistically better over-all survival compared with those who did not(p � 0.006). Others have reported that repeat hepatec-tomy is possible in 10% to 29% of patients with recur-rent HCC.23,24 Though some authors claim they achievea survival similar to that after initial resection with5-year rates ranging from 27% to 50%,24-26 we found amedian survival of only 11 months after repeathepatectomy.
This study demonstrated that 74% of recurrences areisolated to the liver, suggesting a role for regional therapyafter hepatectomy. One possible therapy is hepatic arte-rial radioembolization. In a randomized controlled trialby Lau and colleagues27 an improved survival was seen at3 years (86% versus 46%) in 21 patients with adjuvantarterial iodine-131 lipiodol after curative resection; butthis was a small trial and longer followup and a broaderexperience have not been reported. Adjuvant hepaticarterial infusion chemotherapy is an area of current in-vestigation at our institution because of the responsesthat we observed in pilot trials.28
In summary this study demonstrates that the liver isthe predominant location of first recurrence after resec-tion of hepatocellular carcinoma and that once recur-rence occurs, survival is limited. The data suggest thataggressive therapy at the time of recurrence is warranted,particularly when targeted to the liver. Vascular invasionand tumor size greater than 5 cm are predictive of recur-
rence and may identify a cohort of patients in whomadjuvant therapy should be tested. These data emphasizethe need for effective adjuvant therapy in hepatocellularcarcinoma, a disease in which tumor biology dictatesrecurrence despite optimal surgical technique.
Author ContributionsStudy conception and design: Cha, Fong, Jarnagin,
Blumgart, DeMatteoAcqusition of data: Cha, Fong, Jarnagin, Blumgart,
DeMatteoAnalysis and interpretation of data: Cha, Blumgart,
DeMatteoDrafting of manuscript: Cha, DeMatteoCritical revision: Cha, Fong, Jarnagin, Blumgart,
DeMatteoSupervision: Fong, Jarnagin, Blumgart, DeMatteo
REFERENCES
1. Okuda K, Kojiro M, Okuda H. Neoplasms of the liver. In: SchiffL, Schiff R, eds. Diseases of the liver. Philadelphia: Lippincott;1993:1236–1296.
2. Di Biscegli, Carithers RL, Gores GJ. Hepatocellular carcinoma.Hepatology 1998;28:1161–1165.
3. El Serag, Mason AC. Rising incidence of hepatocellular carci-noma in the United States. N Engl J Med 1999;340:745–750.
4. Okuda K, Ohtsuki T, Obata H, et al. Natural history of hepa-tocellular carcinoma and prognosis in relation to treatment.Study of 850 patients. Cancer 1985;56:918–928.
5. Nagasue N, Yukaya H, Hamada T, et al. The natural history ofhepatocellular carcinoma. A study of 100 untreated cases. Can-cer 1984;54:1461–1465.
6. Bismuth H, Houssin D, Ornowski J, Meriggi F. Liver resectionsin cirrhotic patients: a Western experience. World J Surg 1986;10:311–317.
7. The Liver Cancer Study Group of Japan. Predictive factors forlong term prognosis after partial hepatectomy for patients withhepatocellular carcinoma in Japan. Cancer 1994;74:2772–2780.
8. Nagasue N, Kohno H, Chang YC, et al. Liver resection forhepatocellular carcinoma. Results of 229 consecutive patientsduring 11 years. Ann Surg 1993;217:375–384.
9. Higuchi T, Nakamura T, Uchino H. Effect of age on antipyrinemetabolism in patients with gastric cancer. J Natl Cancer Inst1980;65:897–900.
10. Kanematsu T, Takenaka K, Matsumata T, et al. Limited hepaticresection effective for selected cirrhotic patients with primaryliver cancer. Ann Surg 1984;199:51–56.
11. Chen MF, Hwang TL, Jeng LB, et al. Hepatic resection in 120patients with hepatocellular carcinoma. Arch Surg 1989;124:1025–1028.
12. Nagao T, Inoue S, Goto S, et al. Hepatic resection for hepato-cellular carcinoma. Clinical features and long-term prognosis.Ann Surg 1987;205:33–40.
13. Bismuth H, Chiche L, Adam R, et al. Liver resection versus
757Vol. 197, No. 5, November 2003 Cha et al Resection of Hepatocellular Carcinoma
transplantation for hepatocellular carcinoma in cirrhotic pa-tients. Ann Surg 1993;218:145–151.
14. Bismuth H, Chiche L, Castaing D. Surgical treatment of hepa-tocellular carcinomas in noncirrhotic liver: experience with 68liver resections. World J Surg 1995;19:35–41.
15. Fuster J, Garcia V, Grande L, et al. Hepatocellular carcinomaand cirrhosis. Results of surgical treatment in a European series.Ann Surg 1996;223:297–302.
16. Fong Y, Sun RL, Jarnagin W, Blumgart LH. An analysis of 412cases of hepatocellular carcinoma at a Western center. Ann Surg1999;229:790–799.
17. Poon RT, Fan ST, Lo CM, et al. Improving survival results afterresection of hepatocellular carcinoma: a prospective study of377 patients over 10 years. Ann Surg 2001;234:63–70.
18. Grazi GL, Ercolani G, Pierangeli F, et al. Improved results ofliver resection for hepatocellular carcinoma on cirrhosis give theprocedure added value. Ann Surg 2001;234:71–78.
19. Cha C, DeMatteo RP, Blumgart LH. Surgery and ablative ther-apy for hepatocellular carcinoma. J Clin Gastroenterol 35:S130–S137.
20. Shirabe K, Takenaka K, Taketomi A, et al. Postoperative hepa-titis status as a significant risk factor for recurrence in cirrhoticpatients with small hepatocellular carcinoma. Cancer 1996;77:1050–1055.
21. Yamamoto J, Kosuge T, Takayama T, et al. Recurrence of hep-atocellular carcinoma after surgery. Br J Surg 1996;83:1219–1222.
22. Poon RT, Fan ST, Lo CM, et al. Long-term survival and patternof recurrence after resection of small hepatocellular carcinoma inpatients with preserved liver function: implications for a strategyof salvage transplantation. Ann Surg 2002;235:373–382.
23. Chen MF, Hwang TL, Jeng LB, et al. Postoperative recurrenceof hepatocellular carcinoma. Two hundred five consecutive pa-tients who underwent hepatic resection in 15 years. Arch Surg1994;129:738–742.
24. Nagasue N, Yukaya H, Chang YC, et al. Assessment of patternand treatment of intrahepatic recurrence after resection of hep-atocellular carcinoma. Surg Gynecol Obstet 1990;171:217–222.
25. Shimada M, Matsumata T, Taketomi A, et al. Repeat hepatec-tomy for recurrent hepatocellular carcinoma. Surgery 1994;115:703–706.
26. Hu RH, Lee PH, Yu SC, et al. Surgical resection for recurrenthepatocellular carcinoma: prognosis and analysis of risk factors.Surgery 1996;120:23–29.
27. Lau WY, Leung TW, Ho SK, et al. Adjuvant intra-arterialiodine-131-labelled lipiodol for resectable hepatocellular carci-noma: a prospective randomised trial. Lancet 1999;353:797–801.
28. Atiq OT, Kemeny N, Niedzwiecki D, Botet J. Treatment ofunresectable primary liver cancer with intrahepatic fluorode-oxyuridine and mitomycin C through an implantable pump.Cancer 1992;69:920–924.
758 Cha et al Resection of Hepatocellular Carcinoma J Am Coll Surg



![Laparoscopic liver resection for hepatocellular …cholecystectomy, laparoscopic surgery has become a popular surgical technique[4] and has been applied to solid organs. Initial laparoscopic](https://img.dokumen.tips/doc/110x75/5f8a33d84d8e121417484e5b/laparoscopic-liver-resection-for-hepatocellular-cholecystectomy-laparoscopic-surgery.jpg)









![Recurrence after Endoscopic Curative Resection of Mucosal ... · the local recurrence rate has been reported to be 0-0.4 [5-7]. In cases of local recurrence, although rare, it has](https://img.dokumen.tips/doc/110x75/5e7829da0b72bb34c9783106/recurrence-after-endoscopic-curative-resection-of-mucosal-the-local-recurrence.jpg)















