Embed Size (px)
Citation preview
A Liver D
PHT
FBA
a
Rb
t
IoLpsl“AtwrPsDf((R(pda
TCr
D
C
T
movs[twCcd
R
[
d
TDTM
AB
a
Ab
c
16 Abstracts / Digestive and
REDICTIVE RISK FACTORS OF RECURRENCE OFEPATOCELLULAR CARCINOMA AFTER LIVERRANSPLANTATION
. Gentili a, Q. Lai b, M. Giusto a, G. Mennini b, P.B.erloco b, M. Rossi b, A. De Santis a, S.Ginanni Corradini a,.F. Attili a, M. Merli a
II Division of Gastroenterology. La Sapienza University ofome, ItalyDepartment of General Surgery and Organ Transplanta-
ion. La Sapienza University of Rome, Italy
ntroduction. Liver transplantation (LT) is considered theptimal treatment for hepatocellular carcinoma (HCC). SinceT based on the Milan criteria (MC) has been shown torovide good disease-free survival, to excellent long-termurvival and a low incidence of recurrence. We have ana-yzed individual tumor characteristics applying the new scoreup-to-seven criteria” [1].im. We analyzed our experience with LT for HCC to iden-
ify predictive risk factors of HCC recurrence. Outcomesere compared for patients with HCC recurrence and patients
ecurrence free after LT.atients and methods. We retrospectively studied 109 con-ecutive HCC patients transplanted from January 1988 toecember 2007. We excluded all the patients who died from
actors other than tumour recurrence within the first yearn = 24). Clinical data, eligibility to MC and San FranciscoUCSF) criteria were considered.esults. 85 patients were enrolled, 19 with recurrence
group A) and 66 without recurrence (group B). Allatients in Group A deceased for HCC recurrence, with aisease-free survival mean follow-up of 12.3 ± 7.2 monthsnd an overall-survival mean follow-up of 23.9 ± 19.8
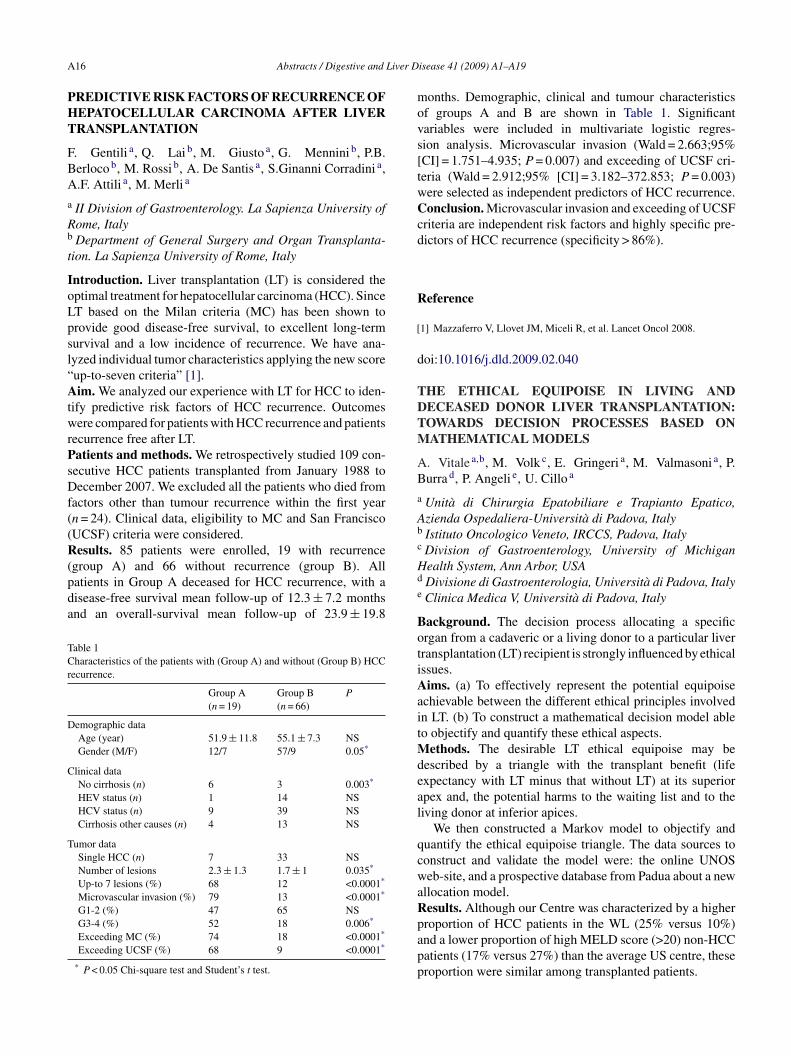
able 1haracteristics of the patients with (Group A) and without (Group B) HCC
ecurrence.
Group A(n = 19)
Group B(n = 66)
P
emographic dataAge (year) 51.9 ± 11.8 55.1 ± 7.3 NSGender (M/F) 12/7 57/9 0.05*
linical dataNo cirrhosis (n) 6 3 0.003*
HEV status (n) 1 14 NSHCV status (n) 9 39 NSCirrhosis other causes (n) 4 13 NS
umor dataSingle HCC (n) 7 33 NSNumber of lesions 2.3 ± 1.3 1.7 ± 1 0.035*
Up-to 7 lesions (%) 68 12 <0.0001*
Microvascular invasion (%) 79 13 <0.0001*
G1-2 (%) 47 65 NSG3-4 (%) 52 18 0.006*
Exceeding MC (%) 74 18 <0.0001*
Exceeding UCSF (%) 68 9 <0.0001*
* P < 0.05 Chi-square test and Student’s t test.
Hd
e
BotiAaitMdeal
qcwaRpapp
isease 41 (2009) A1–A19
onths. Demographic, clinical and tumour characteristicsf groups A and B are shown in Table 1. Significantariables were included in multivariate logistic regres-ion analysis. Microvascular invasion (Wald = 2.663;95%CI] = 1.751–4.935; P = 0.007) and exceeding of UCSF cri-eria (Wald = 2.912;95% [CI] = 3.182–372.853; P = 0.003)ere selected as independent predictors of HCC recurrence.onclusion. Microvascular invasion and exceeding of UCSF
riteria are independent risk factors and highly specific pre-ictors of HCC recurrence (specificity > 86%).
eference
1] Mazzaferro V, Llovet JM, Miceli R, et al. Lancet Oncol 2008.
oi:10.1016/j.dld.2009.02.040
HE ETHICAL EQUIPOISE IN LIVING ANDECEASED DONOR LIVER TRANSPLANTATION:OWARDS DECISION PROCESSES BASED ONATHEMATICAL MODELS
. Vitale a,b, M. Volk c, E. Gringeri a, M. Valmasoni a, P.urra d, P. Angeli e, U. Cillo a
Unità di Chirurgia Epatobiliare e Trapianto Epatico,zienda Ospedaliera-Università di Padova, ItalyIstituto Oncologico Veneto, IRCCS, Padova, ItalyDivision of Gastroenterology, University of Michiganealth System, Ann Arbor, USADivisione di Gastroenterologia, Università di Padova, ItalyClinica Medica V, Università di Padova, Italy
ackground. The decision process allocating a specificrgan from a cadaveric or a living donor to a particular liverransplantation (LT) recipient is strongly influenced by ethicalssues.ims. (a) To effectively represent the potential equipoise
chievable between the different ethical principles involvedn LT. (b) To construct a mathematical decision model ableo objectify and quantify these ethical aspects.
ethods. The desirable LT ethical equipoise may beescribed by a triangle with the transplant benefit (lifexpectancy with LT minus that without LT) at its superiorpex and, the potential harms to the waiting list and to theiving donor at inferior apices.
We then constructed a Markov model to objectify anduantify the ethical equipoise triangle. The data sources toonstruct and validate the model were: the online UNOSeb-site, and a prospective database from Padua about a new
llocation model.esults. Although our Centre was characterized by a higher
roportion of HCC patients in the WL (25% versus 10%)nd a lower proportion of high MELD score (>20) non-HCCatients (17% versus 27%) than the average US centre, theseroportion were similar among transplanted patients.




























