Embed Size (px)
Citation preview
Preconception Carefor
Women with Diabetes
Objectives and GoalsTo Understand…
Preconception Care (PCC): definition and purpose
The role that PCC plays for women with diabetes Identify different aspects of pregnancy
readiness Pregnancy Spacing for better health
Preconception Care: Definition
“Preconception care is comprised of interventions that aim to identify and modify
biomedical behavior and social risks
to a woman’s health or pregnancy outcome through prevention and management, emphasizing those factors to be acted on before conception...”(CDC, 2009)
Every woman, every time (MOD, 2001)
Preconception Care
Sweet Success PCC Goals… To Prevent excess spontaneous abortions and
congenital malformations in infants of diabetic mothers Achieve A1C levels < 6.5% Assure effective contraception until stable and
acceptable glycemia is achieved Identify, evaluate, and treat long-term diabetic
complications (GFC, in print)
Main Elementsin the SS Model of Care…
1. Physician directed medical assessment, laboratory testing, treatment, maternal and fetal care.
2. Patient education about interaction of diabetes and pregnancy, and self-care
3. Educator-directed assessment and education of diabetes self-management skills
4. Mental health professional counseling when indicated to assess coping, reduce stress and improve adherence to diabetic treatment plan
(GFC, in print)

Risks to Moms…
Pyelonephritis Preterm delivery Traumatic delivery Operative delivery Progression of disease
Hypoglycemia Pregnancy Loss Pre-eclampsia Polyhydramnios Hyperglycemia Diabetic Ketoacidosis

Risks for Babies…
Organogenesis largely completed by week 8 of gestation
Poorly controlled blood glucose in this period of time risks of anomalies &SAB
Poorly controlled blood glucose risk and predisposes to chronic diseases including diabetes (Diabetes Care, January 2003)
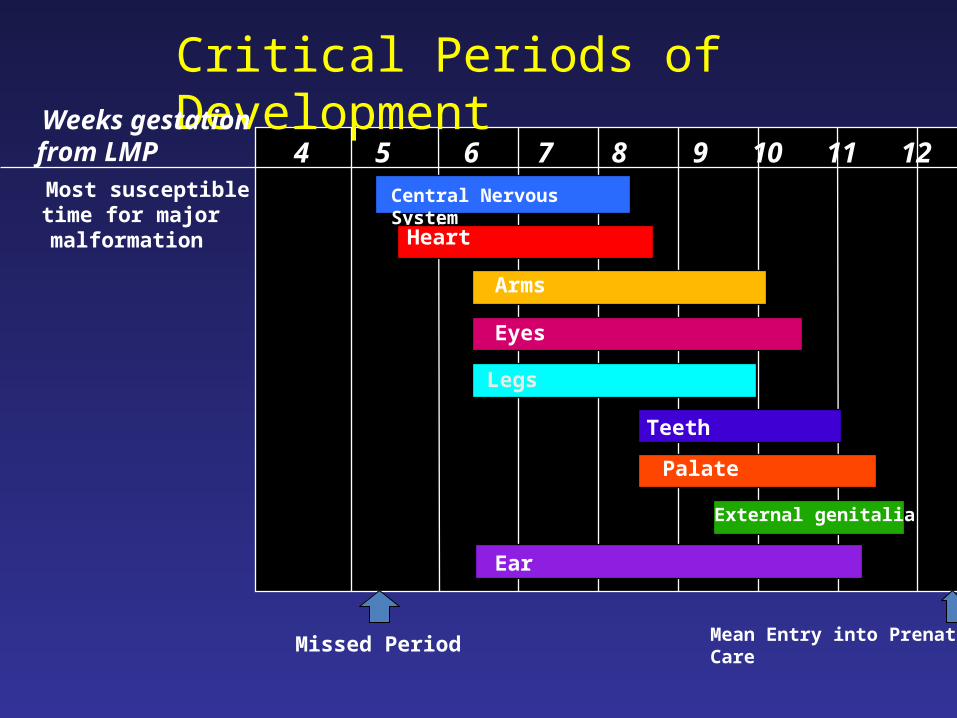
Critical Periods of Development
4 5 6 7 8 9 10 11 12
Weeks gestationfrom LMP
Central Nervous System
Heart
Arms
Eyes
Legs
Teeth
Palate
External genitalia
Ear
Missed Period Mean Entry into Prenatal Care
Most susceptibletime for majormalformation
Why Plan and Change?
Preconception Care Identifies risks Provides interventions tooptimal outcomes Maximizes maternal health Builds more effective patient/provider relationship prior to conception Improves early access to prenatal care Reduces poor outcomes Creates rewarding experience for couples
The Big PCC Picture…Team-Work!
Readiness for pregnancy Complete medical examination Laboratory Evaluation Normal Blood glucose control Planned Pregnancy
Readiness for Pregnancy…Healthy Coping
General Mental Health Diabetic Self-Care High-Risk Factors Network of Social Support Resources/consultations
Complete Medical Exam…History Assessment
Type of diabetes Risk for diabetes (previously pre-diabetes) Age at onset, including duration Status of medical conditions/treatments
organ involvement hospitalizations complications pregnancy history
Co-morbidities Current Medications Alcohol or chemical substance use
Medical Exam… Physical Assessment*
Metabolic control Blood pressure Cardiovascular examination Retinal Renal Neurological Dental Evaluation Foot Exam Immunological Status Pelvic exam/pap smear
*Thefocus of assessment is to evaluate level of end organ damage, retina, kidney, vasculature, heart and nervous system and any other medical conditions
Medical Exam and Labs…
1. Metabolic Control: A1c: Goal < 6.5 Fasting Lipid Profile: HDL: >50 mg/dL Triglycerides (TG) <150 mg/dL Total LDL Cholesterol <100 mg/dL
recommendation with DM & CAD < 70 mg/dL Serum TSH screening and or free thyroxin level Celiac disease screening in type 1
Medical Exam and Labs…
2. Blood pressure Controlled. Goal: < 130/80
3. Cardiovascular exam / Electrocardiogram (EKG/ECG) Consider testing or referral for peripheral atherosclerotic vascular disease if a woman is at high risk or demonstrates signs and symptoms.
EKG: women > 34; DM1 >10 years, DM2; or with signs and symptoms of angina, or exercise intolerance.
4. Dilated retinal exam: Ophthalmologist knowledgeable in diabetic eye conditions.
Medical Exam and Labs…
5. Renal status to test for potential nephropathy: Random urine: Normal random
microalbumin/creatinine<30mg/day
If abnormal:
24 hour urine collection is for total protein, and or/creatinine Total protein <150 mg/mg per 24 hours
Serum creatinine 0.7-0 .9

Medical Exam and Labs…..
6. Neurological:
Assessment of autonomic dysfunction
Hypoglycemia unawareness, orthostatic hypotension, excessive nausea and vomiting
Gastrointestinal autonomic neuropathy or gastroparesis
Medical Exam and Labs…
7. Dental Examination: Refer if woman does not have regular dental health care.
8. Foot exam: By PCP or podiatrist.
8. Immunological Status: Update all pertinent immunizations. (GFC, in print)
Summary of Laboratory Evaluation
Recommended PCC testing:
A1c Complete Blood Count Serum TSH/T4 Random Urine
Serum Creatinine 24 hour urine protein Microalbumin
Lipid profile
Planned Pregnancy…Management Includes
Contraception is utilized until glycemic control is achieved Smoking cessation Nutritional Supplementation
Folate 400µg/day 4 mg/day with Hx neural tube defect or cleft palate defect Multiple Vitamin
Medications compatible with pregnancy 1. Intensive insulin regimen2. Medical nutrition therapy 3. Activity evaluation
Intensive Glycemic Control
Current regimen Set realistic goals Insulin adjustments Evaluate self-management skills
Hypo/hyperglycemia Safeguards Signs and Symptoms Glucagon Ketones
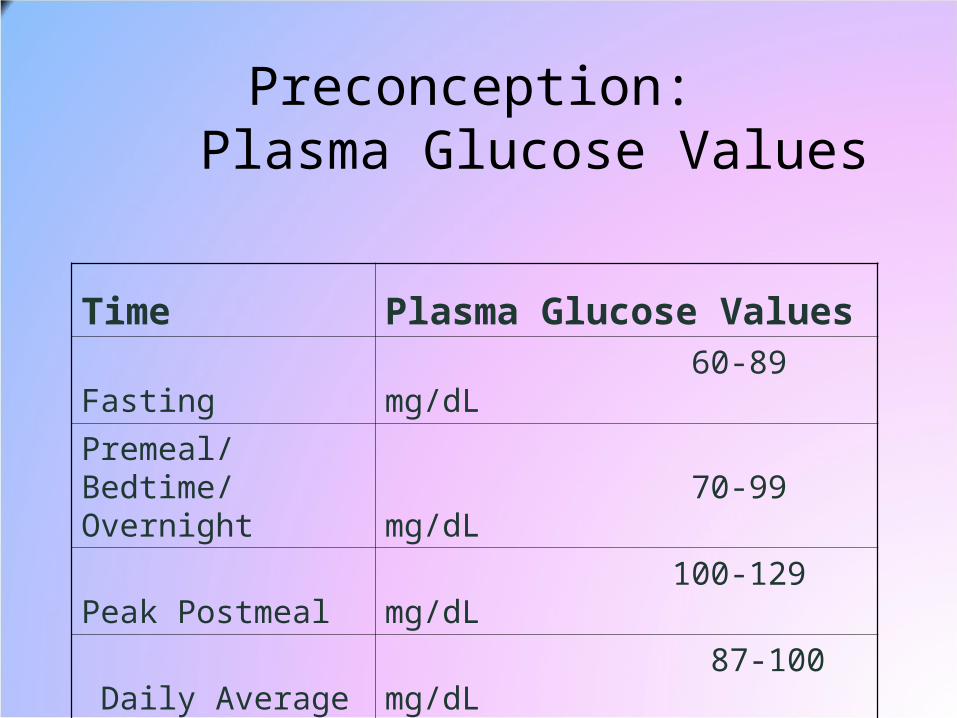
Preconception: Plasma Glucose Values
Time Plasma Glucose ValuesFasting 60-89 mg/dL
Premeal/Bedtime/ Overnight 70-99 mg/dL
Peak Postmeal 100-129 mg/dL
Daily Average 87-100 mg/dL
Medical Nutrition Therapy…Healthy Eating
Determine energy needs Achieve desirable body weight Maintain balance in diet plan Evaluate adherence Educate about diet issues and pregnancy Reinforce importance of dietary
supplements
Activity Evaluation…Being Active
Endorphins to enhance mental well-being Improves insulin sensitivity Improves strength and endurance Improves BMI Improves cardiovascular status Enhances a healthy lifestyle Safeguards against hyperglycemic episodes
Any contraindications? Limitations?
Management Continues with Optimal Control…
Blood pressure normalization Cardiovascular/Neurologic
Stability Stabilized retinopathy A1c < 6.5 % Evaluate Insulin Therapy
During Gestation
Early Referral to Sweet Success Program Management will continue for optimal
control Psychosocial wellbeing Glycemic control Cardiovascular Retinal Renal Metabolic Fetal wellbeing
Preconception Care for Women with GDM History
Pregnancy History Converted? Contraception? Weight reduction achieved? Exercise? Current Diet? Folate? MVI/PNV? Immunizations/General Health? Utilize the “teachable moment”
Preconception Care…for GDM Patients
If Postpartum Screen was NEGATIVE: Test fasting every year thereafter Test every 3rd year using 2 hour OGTT Test at next PCC or at first prenatal visit Attain normal BMI, life style of healthy coping, healthy
eating; being active is recommended
If Postpartum Screen was POSITIVE: She should present for preconception care
Other Conditions Requiring Preconception Care:
Polycystic Ovary Syndrome A clinical diagnosis of chronic
hyperandrogenism and anovulation The leading cause of infertility The most common endocrinopathy
affecting 6-10% of women of reproductive age.
Not all have cysts Many are normal weight
Clinical Features Associated with PCOS
Menstrual dysfunction-as early as age 12 15-30% have regular menses Infertility and /or miscarriage
Facial and upper back acne Obesity in ~ 60% Excessive hair growth Androgenetic alopecia Acanthosis Nigricans in ~ 30% Ovarian cortex containing multiple atretic follicles in ~
80%
Metabolic Aberrations in PCOS
Most significant is
Insulin Resistance (IR) with compensatoryHyperinsulinemia
Endocrinopathy with PCOS
Chronically elevated Luteinizing hormone to FSH (LH:FSH = 3:1)
↑ Levels free testosterone (usually ovarian source but can also be adrenal)
↓ Sex hormone-binding globulin Normal prolactin except for ~15% who have
slight elevations
Insulin Sensitizers to Treat Insulin Resistance and Secondary Infertility
Multinational study: Metformin vs. placebo for obese women with PCOS34% ovulation vs. 4 % in placebo group90% Metformin plus clomid vs. 8% in
placebo group8 fold increase in conception when taking
Metformin (Nestler et al. 2002)
PCOS and Type 2 DM
35 % of women with PCOS have clinical IGT and do not know it.
10 % of women with PCOS are diagnosed with Type 2 DM by age 40(Ehrman et al. Diabetes Care, Jan 1999)
PCOS and GDM
Hypothesized that all have insulin resistance with compensatory hyperinsulinemia
~ 40% PCOS develop GDM
40 -52% GDM’s have PCOS ovarian morphology
Resources
www.cdph.ca.gov/programs/cdappFor Sweet Success information www.marchofdimes.orgFor California Preconception Initiative Professional Resources for PCC www.everywoman.org For California Preconception link
(provider/consumer link) www.cdc.gov/NCBDDD/preconceptional/default
.htm For Centers for Disease Control & Prevention link
OK… Now…
Get Pregnant…
……………………………………..FAST….
.
Thank You!
Contact Information
Gretchen Page , MPH, CNM Manager, Inland Counties Regional Perinatal Programs,
LLUMC/Children’s Hospital (909) [email protected]