Embed Size (px)
Citation preview

Chronic Kidney Disease-Related Mineral and Bone Disorder:
Public Health Problem
Kerry Willis PhD
National Kidney Foundation

0
5
10
15
20
25
30
35
1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996
Year of ESRD Incidence or Transplantation
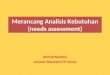
21.5
19.8
4.1
2.0
1999 annual report of the US Renal Data System
Dea
ths/
100
pat
ien
t-ye
ars
Dialysis All ESRD Cadaveric Transplant Living Related Transplant
Adjusted 1st Year Patient Death Rates by Treatment Modality and Year of Incidence, 1986-96

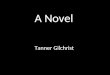
0.01
100
10
1
0.1
An
nu
al m
ort
alit
y (%
)
25–34 45–54 65–74 8535–44 55–64 75–84
Age (years)
Cardiovascular Mortality in the General Population and in Dialysis Patients
General populationMale Female
BlackWhite
Dialysis populationMale Female
BlackWhite

NKF’s Clinical Practice Guidelines
• Evidence Based Review• Publication and Dissemination• Implementation • Reassess Impact• Update

DOQI KDIGOK/DOQI
DialysisAnemiaAccess
Nutrition (00)Dialysis (’01)*Anemia (’01)*Access(‘01)*CKD class. (’02)Bone/Mineral (’03) Lipids (’03)Htn (’04)CV (’05)Diabetes (’07)
Hep C (’08)Bone/Mineral (’08)
1997 2005
*updates
http://www.kidney.org/professionals/kdoqi
1999
http://www.kdigo.org/welcome.htm

NKF-K/DOQI Definition of CKD
Structural or functional abnormalities of the kidneys for >3 months, as manifested by either:
1. Kidney damage, with or without decreased GFR, as defined by
• pathologic abnormalities• markers of kidney damage
– urinary abnormalities (proteinuria)– blood abnormalities (renal tubular syndromes)– imaging abnormalities
• kidney transplantation2. GFR <60 ml/min/1.73 m2, with or without kidney
damage

Stage Description GFR (ml/min/1.73 m2)
1 Kidney damage with normal or GFR
90
2 Kidney damage with mild GFR 60-89
3 Moderate GFR 30-59
4 Severe GFR 15-29
5 Kidney failure < 15 (or dialysis)
KDOQI: CKD Staging

CKD is a Public Health Problem
• CKD is common
• CKD is harmful
• We have treatment

CKDCKDdeathdeathCKDCKDdeathdeath
ComplicationsComplicationsComplicationsComplications
Screening for CKD
risk factors:diabetes
hypertensionage >60
family historyUS ethnic minorities
CKD riskreduction;
Screening forCKD
Diagnosis& treatment;
Treat comorbid
conditions;Slow
progression
Estimateprogression;
Treatcomplications;
Prepare forreplacement
Replacementby dialysis
& transplant
NormalNormalNormalNormal IncreasedIncreasedriskrisk
IncreasedIncreasedriskrisk
KidneyKidneyfailurefailureKidneyKidneyfailurefailureDamageDamageDamageDamage GFRGFR GFRGFR
11.3 m11.3 m5.6%5.6%
7.7 m7.7 m7.7 m7.7 m3.8%3.8%
0.3 m0.3 m0.2%0.2%
Conceptual Model for CKD

KI (2007) 71, 31-38. Levin et. al.
Prevalence of Abnormal Mineral Metabolism in CKD
>4.6

K/DOQI Clinical Practice Guidelineson Bone Metabolism and Disease
in Chronic Kidney Disease
Published October 2003

KDOQI Clinical Practice Guidelines for Bone Metabolism and Disease in Chronic Kidney Disease
Chair: Vice-Chair:Shaul G. Massry, MD Jack W. Coburn, MDKECK School of Medicine VA Greater Los Angeles Work Group Members:Glenn M. Chertow, MD, MPH James T. McCarthy, MDUniversity of California, San Francisco Mayo Clinic
Keith Hruska, MD Sharon Moe, MDBarnes Jewish Hospital Indiana University
Craig Langman, MD Isidro B. Salusky, MDChildren’s Memorial Hospital UCLA School of Medicine
Hartmut Malluche, MD Donald J. Sherrard, MDUniversity of Kentucky VA Puget Sound
Kevin Martin, MD, BCh Miroslaw Smogorzewski, MDSt. Louis University University of Southern California
Linda M. McCann, RD, CSR, LD Kline Bolton, MDSatellite Dialysis Centers RPA Liaison

K/DOQI™ Clinical Practice Guidelineson Bone Metabolism Target Levels
CKD Stage 3
CKD Stage 4
CKD Stage 5
(on dialysis)
P(mg/dL)
2.7 - 4.6 2.7 - 4.6 3.5 - 5.5*
Ca(mg/dL)
“Normal” “Normal”
8.4 - 9.5; Hypercalcemia =
>10.2
Intact PTH
(pg/mL)35 - 70 70 - 110
150 - 300*
*Evidence

Treatment Recommendations(Stages 3 & 4)
• Decrease total body phosphorus burden by dietary restriction and phosphorus binder therapy- 2.7- 4.6 mg/dL; begin when EITHER elevated serum phosphorus OR elevated serum PTH
• Treat elevated PTH with active oral vitamin D sterol to target of 35-70 (CKD 3) or 70-110 (CKD 4) pg/mL by intact assay
• Normalize serum calcium

• Normalize serum phosphorus by diet and phosphorus binder therapy- 3.5-5.5 mg/dL (1.13 -1.78 mmol/L); limit elemental calcium intake from binders to 1500 mg/day
• Treat elevated PTH with active vitamin D sterol to target of 150-300 pg/mL (16-32 pmol/L) by intact assay
• Normalize serum calcium- ideally 8.4 -9.5 mg/dL (2.10-2.38 mmol/L), and always < 10.2 mg/dL (2.55 mmol/L); Ca X P < 55 mg2/dL2
Treatment RecommendationsStage 5 (dialysis)

Abnormal boneAbnormal bone
AgeAge
Oxidation (OxLDL)Oxidation (OxLDL)
DiabetesDiabetes
HTNHTN
Advanced glycationAdvanced glycation end-productsend-products
SmokingSmoking
GeneticsGenetics
DyslipidemiaDyslipidemiaCarbonyl stressCarbonyl stress
Low fetuin-ALow fetuin-A
Traditional Risk Factors Non-traditional Risk Factors
Elevated IL-1, Il-6, TNFElevated IL-1, Il-6, TNF
HomocysteineHomocysteine
Abnormal mineral metabolismAbnormal mineral metabolism
FracturesFracturesCardiovascular Cardiovascular disease in CKDdisease in CKD

Classification Issues in Bone and Mineral Disorders
• The term renal osteodystrophy is used to describe different entities
• The predominant use is to describe a disorder of bone remodeling. However this does not take into account new data that there is increased morbidity/mortality of abnormal serum biochemistries (i.e. phosphorus), nor increased awareness of vascular disease related to bone and mineral disorders in CKD patients.

Definition, Evaluation and Classification of Renal Osteodystrophy:
A position statement from Kidney Disease Improving Global Outcomes (KDIGO)
April, 2006

Standardization of Terms
• The term renal osteodystrophy (ROD) should be used exclusively to define the bone pathology associated with CKD.
• The clinical, biochemical, and imaging abnormalities should be defined more broadly as a clinical entity or syndrome called Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD).

Definition of CKD-MBD
A systemic disorder of mineral and bone metabolism due to CKD manifested by either one or a combination of the following:– Abnormalities of calcium, phosphorus, PTH, or
vitamin D metabolism
– Abnormalities in bone turnover, mineralization, volume, linear growth, or strength
– Vascular or other soft tissue calcification
Moe et al Kidney International June 2006

A Framework for Classification of CKD-MBD
Type*Laboratory
AbnormalitiesBone Disease
Calcification of Vascular or Other
Soft Tissue
L + - -
LB + + -
LC + - +
LBC + + +
* L = laboratory abnormalities (of calcium, phosphorus, PTH, alkaline phosphatase or vitamin D metabolism); B = bone disease (abnormalities in bone turnover, mineralization, volume, linear growth, or strength); C = calcification of vascular or other soft tissue.
Kidney International June 2006

www.kdigo.org

Summary1. CKD is defined using eGFR and classified into 5
stages2. This classification can help predict clinical outcomes3. Early detection and treatment can improve patient
outcomes4. There is a link between CVD and bone and mineral
disease in CKD5. New CKD-MBD classification will form the basis for
updated, international clinical practice guidelines

Population Attributable Risk of All Cause Mortality in CKD 5D
• 17.5% Mineral metabolism abnormalities (Phosphorus > 5.0 mg/dl, Calcium >
10 mg/dl, intact PTH > 600 pg/ml)• 11.3% Anemia (hgb < 11 g/dl)• 5.1% Inefficient Dialysis (URR < 65%)
Corollary: We should be able to significantly improve mortality of CKD patients by improving control of mineral metabolism
Block et al JASN 2004Block et al JASN 2004