Embed Size (px)
Citation preview
EFFICACY OF OMEGA-3 POLYUNSATURATED FATTY ACIDS IN
PREVENTING CANCER-INDUCED CACHEXIA
Josh Nooner, BS, CSCSNSCI – 5843
4/22/16
Introduction
Cachexia: Definition, diagnosis, etiology, complications, treatmentsOmega-3 PUFAs: Roles in treating cachexia, mechanisms, early
studies
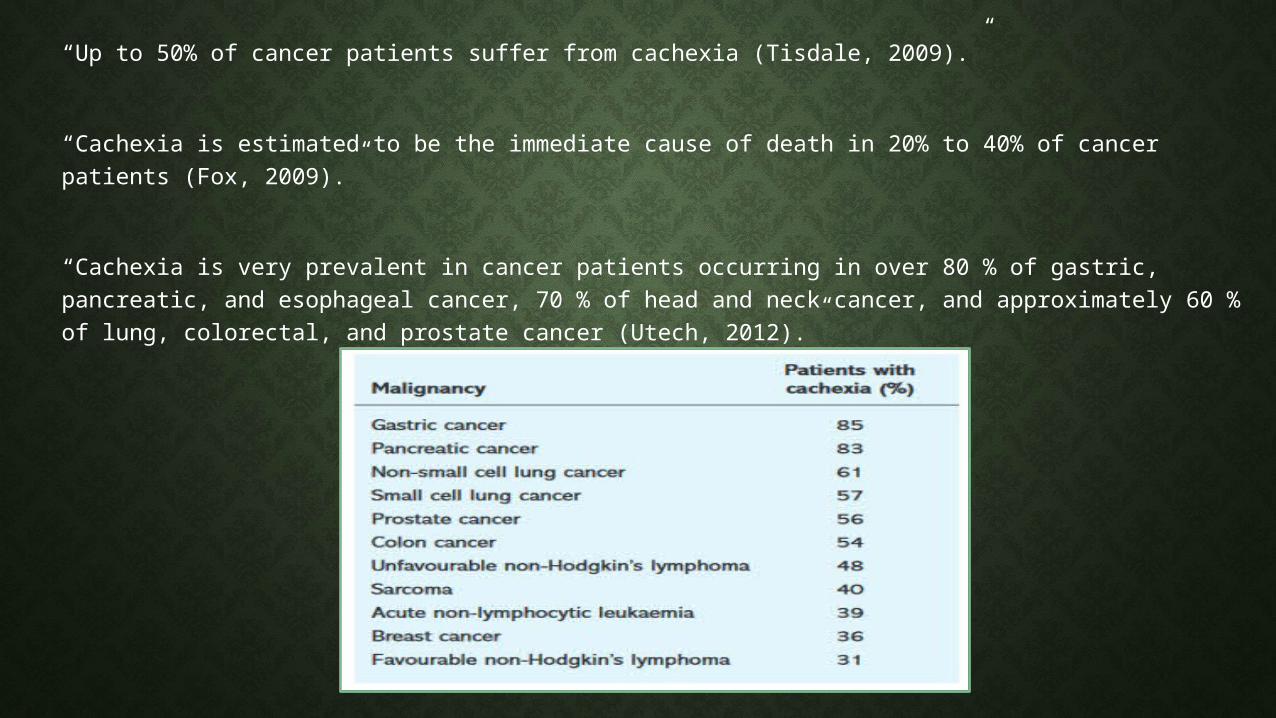
“Up to 50% of cancer patients suffer from cachexia (Tisdale, 2009).”
“Cachexia is estimated to be the immediate cause of death in 20% to 40% of cancer patients (Fox, 2009).”
“Cachexia is very prevalent in cancer patients occurring in over 80 % of gastric, pancreatic, and esophageal cancer, 70 % of head and neck cancer, and approximately 60 % of lung, colorectal, and prostate cancer (Utech, 2012).”
Cachexia In My Family

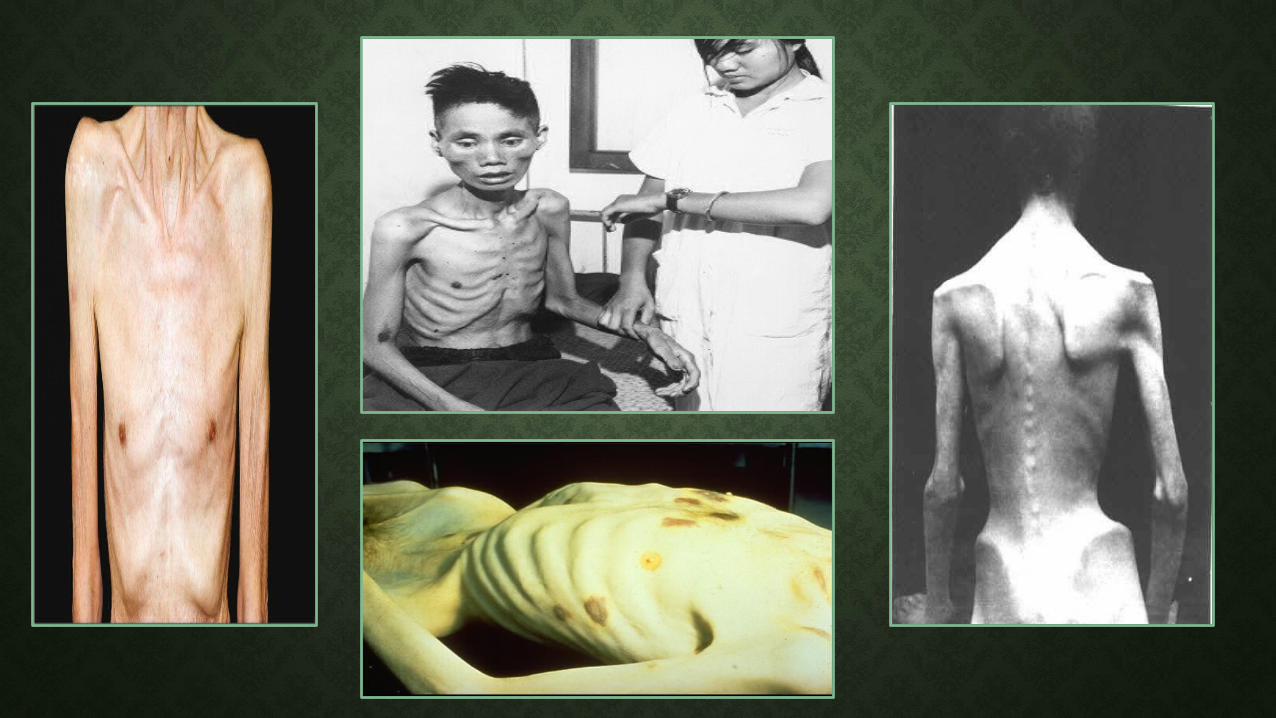
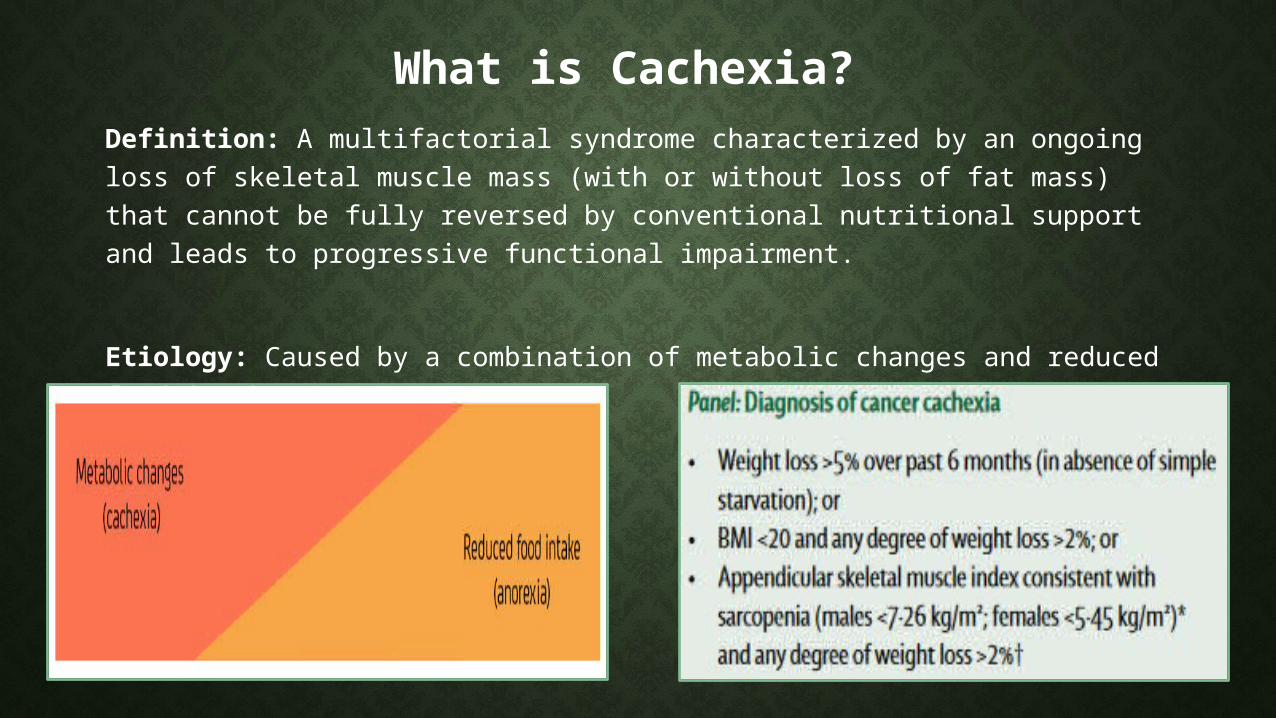
What is Cachexia? Definition: A multifactorial syndrome characterized by an ongoing loss of skeletal muscle mass (with or without loss of fat mass) that cannot be fully reversed by conventional nutritional support and leads to progressive functional impairment.
Etiology: Caused by a combination of metabolic changes and reduced food intake.
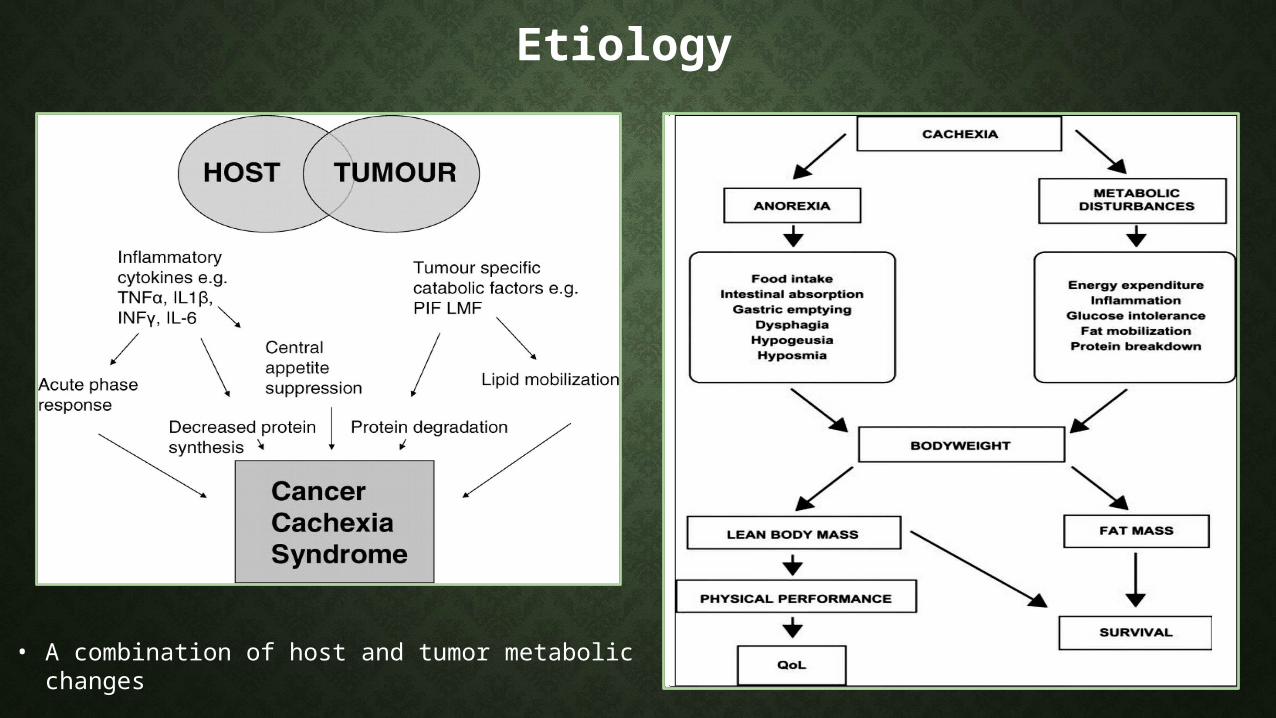
Etiology
• A combination of host and tumor metabolic changes
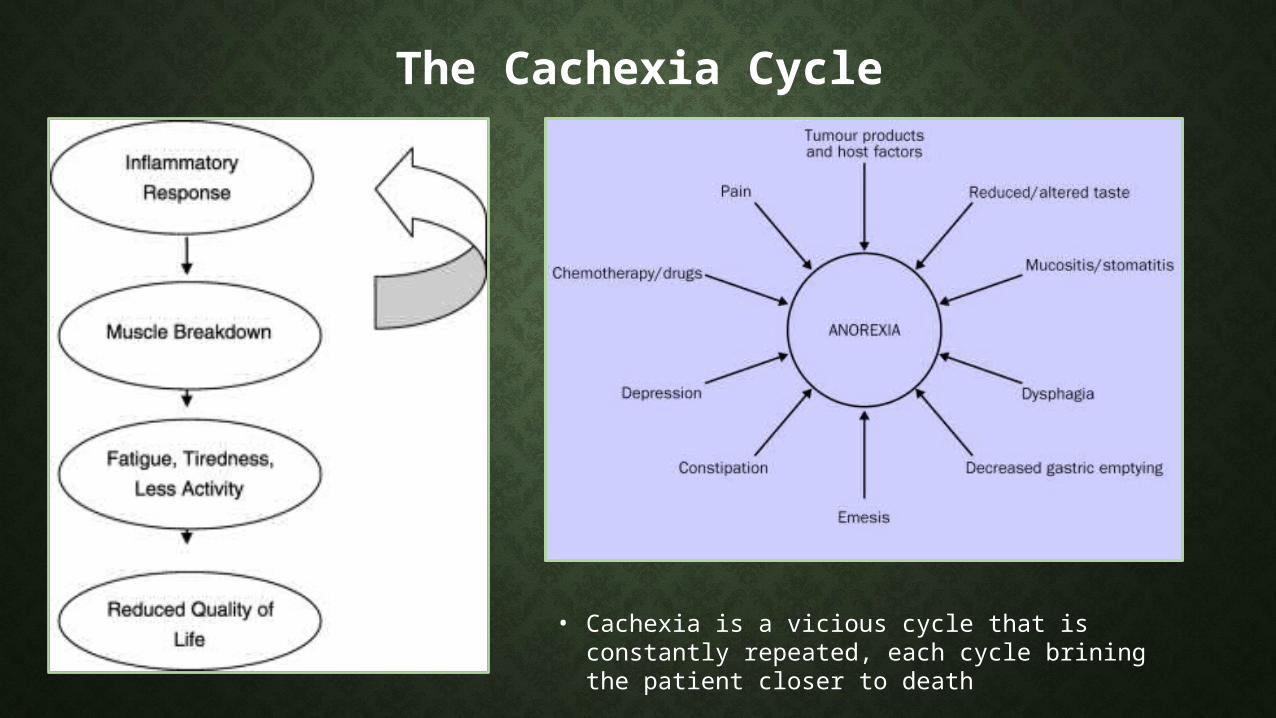
The Cachexia Cycle
• Cachexia is a vicious cycle that is constantly repeated, each cycle brining the patient closer to death
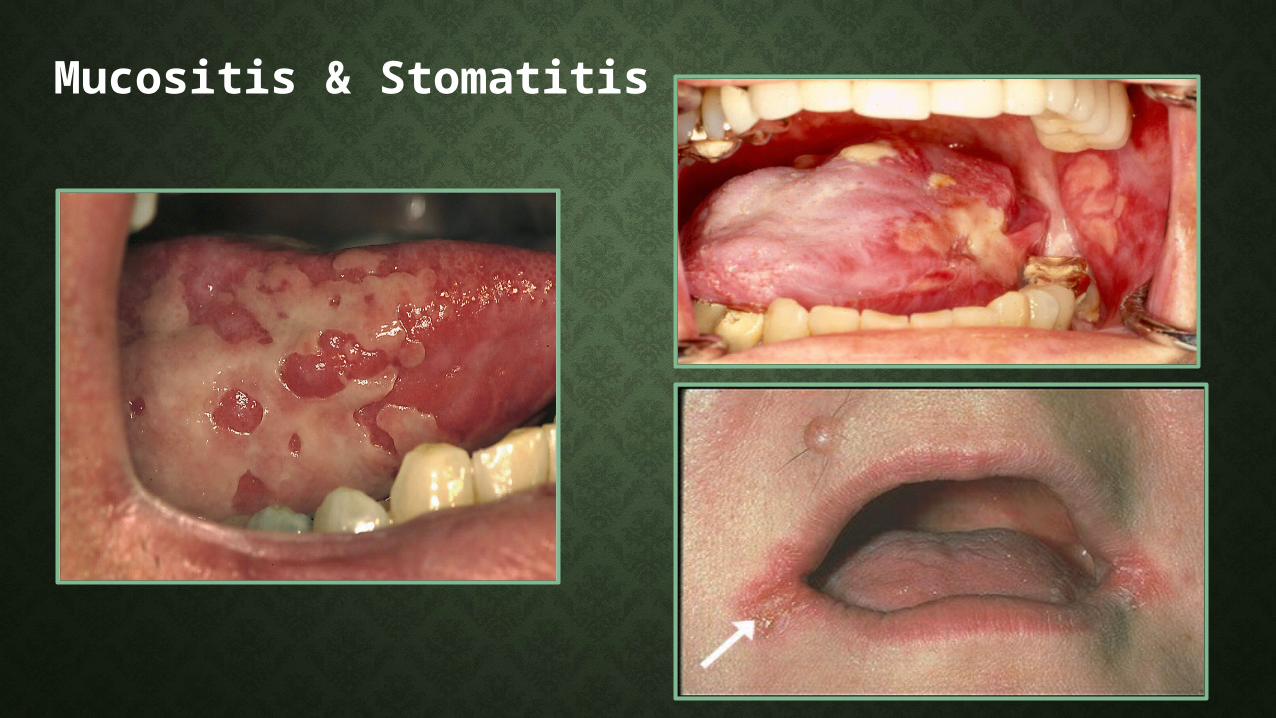
Mucositis & Stomatitis
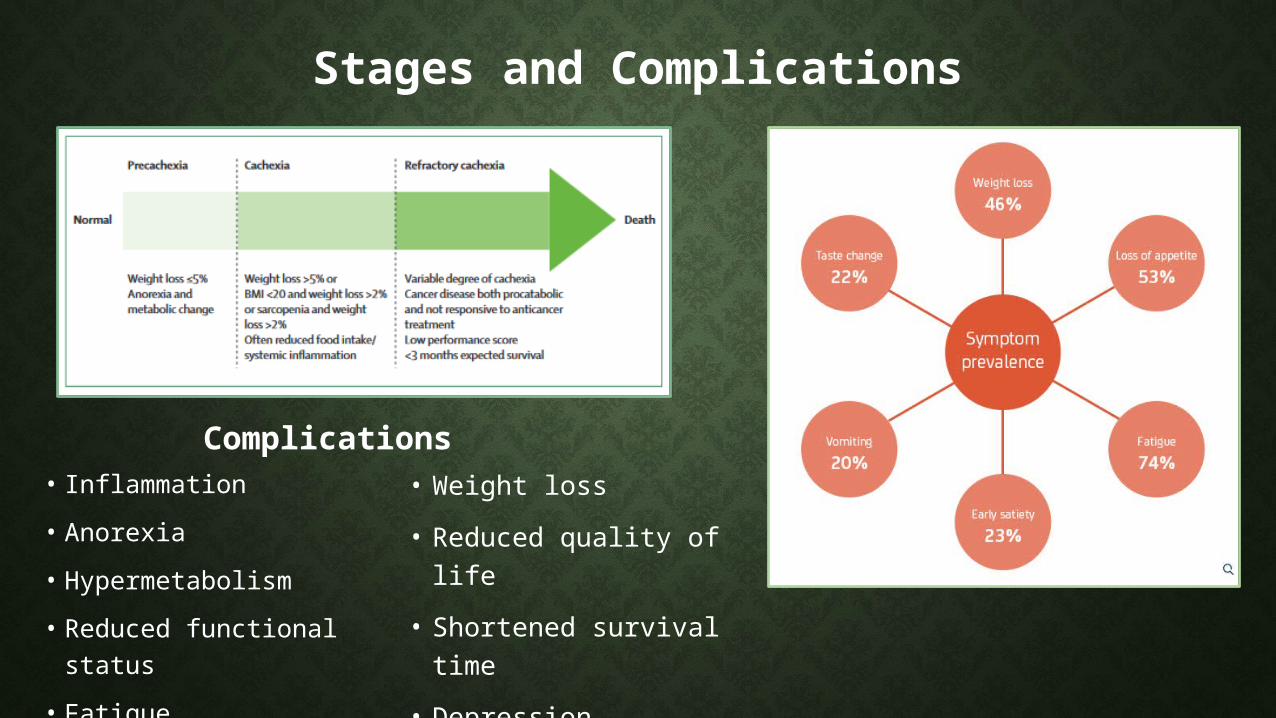
Stages and Complications
• Inflammation• Anorexia• Hypermetabolism • Reduced functional
status• Fatigue
Complications• Weight loss• Reduced quality of
life• Shortened survival
time• Depression• Death
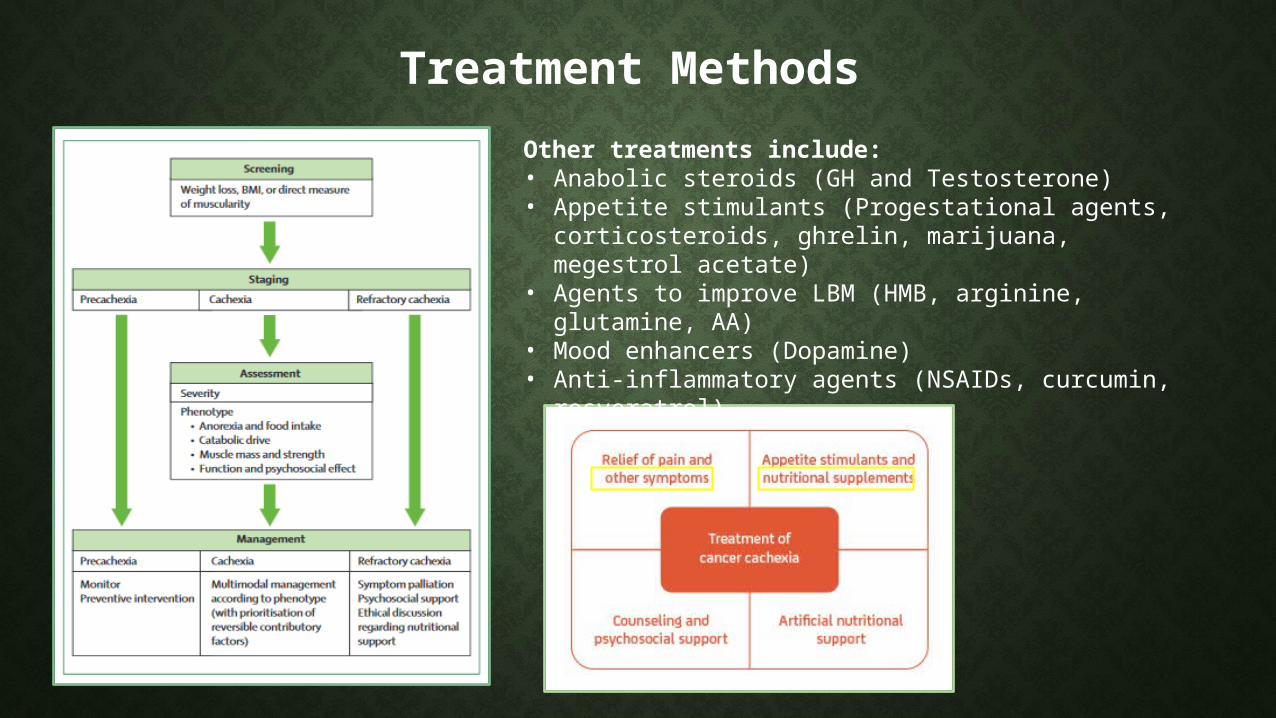
Treatment MethodsOther treatments include:• Anabolic steroids (GH and Testosterone)• Appetite stimulants (Progestational agents,
corticosteroids, ghrelin, marijuana, megestrol acetate)• Agents to improve LBM (HMB, arginine, glutamine,
AA)• Mood enhancers (Dopamine)• Anti-inflammatory agents (NSAIDs, curcumin,
resveratrol)
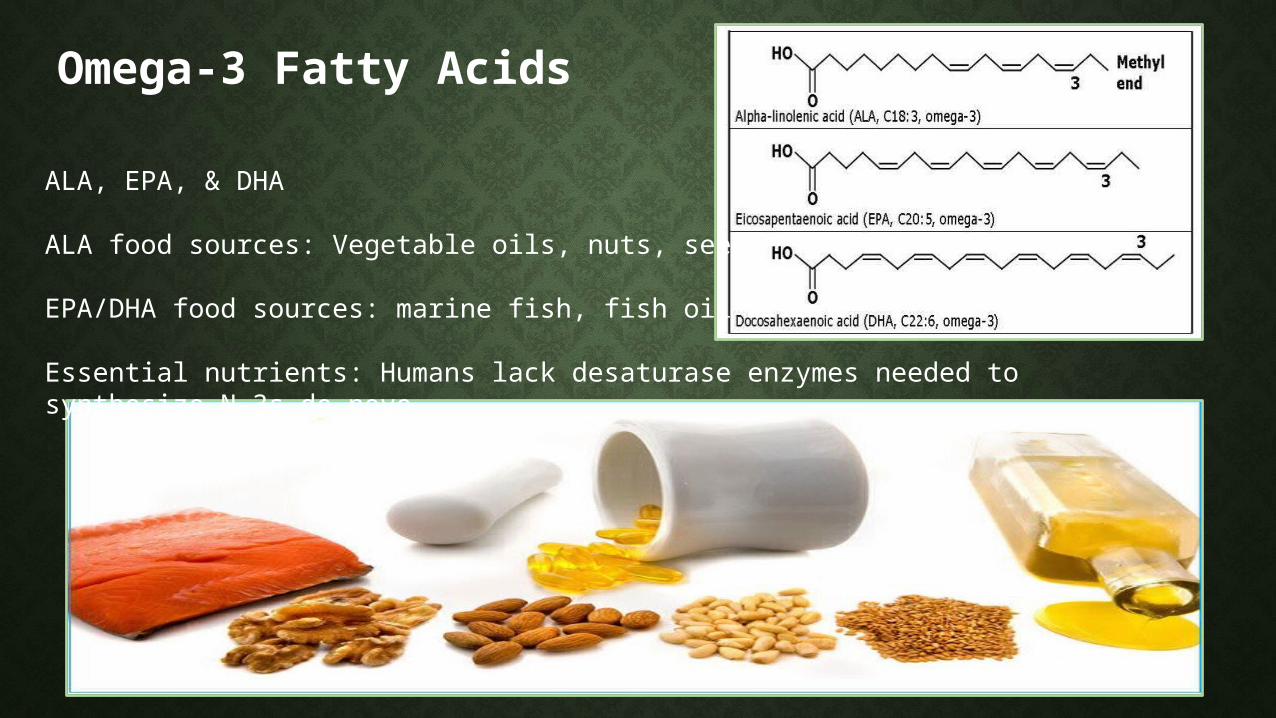
Omega-3 Fatty Acids
ALA, EPA, & DHA
ALA food sources: Vegetable oils, nuts, seeds
EPA/DHA food sources: marine fish, fish oil
Essential nutrients: Humans lack desaturase enzymes needed to synthesize N-3s de novo
Dosage & Side Effects
The AI has been set at 1.6g/day for men and 1.1g/day for women
Most interventional studies use between 1-2g/day
Very few and minimal negative effects: fishy taste, fish burps, GI disturbance, steatorrhea, potential for increased bleeding risk, possible environmental contamination, decreased immunity
FDA ruled that intakes up to 3 g/day are Generally Recognized As Safe (GRAS) and are unlikely to result in bleeding
N-3 PUFA Roles in CachexiaReported effects on cachexia: 1. Suppression of the ubiquitin-proteasome pathway2. Suppression of inflammatory cytokines3. Suppression of the cancer cachectic factor 4. Inhibition of the proteolysis inducing factor 5. Decreased angiogenesis to tumor cells6. Altering estrogen metabolism7. Increased GLUT-4 production and insulin sensitivity 8. Reduce the side effects of chemo9. Increase effectiveness of chemo
Mechanisms of Action
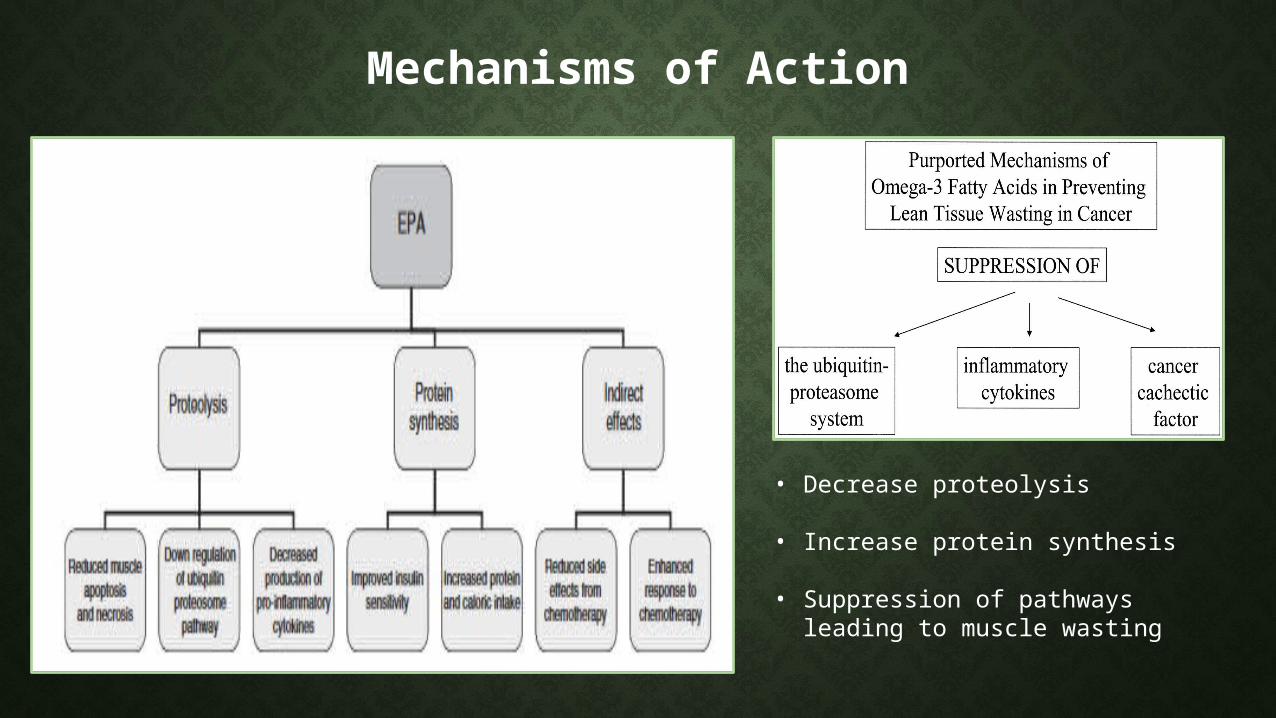
• Decrease proteolysis
• Increase protein synthesis
• Suppression of pathways leading to muscle wasting
Mechanisms of Action
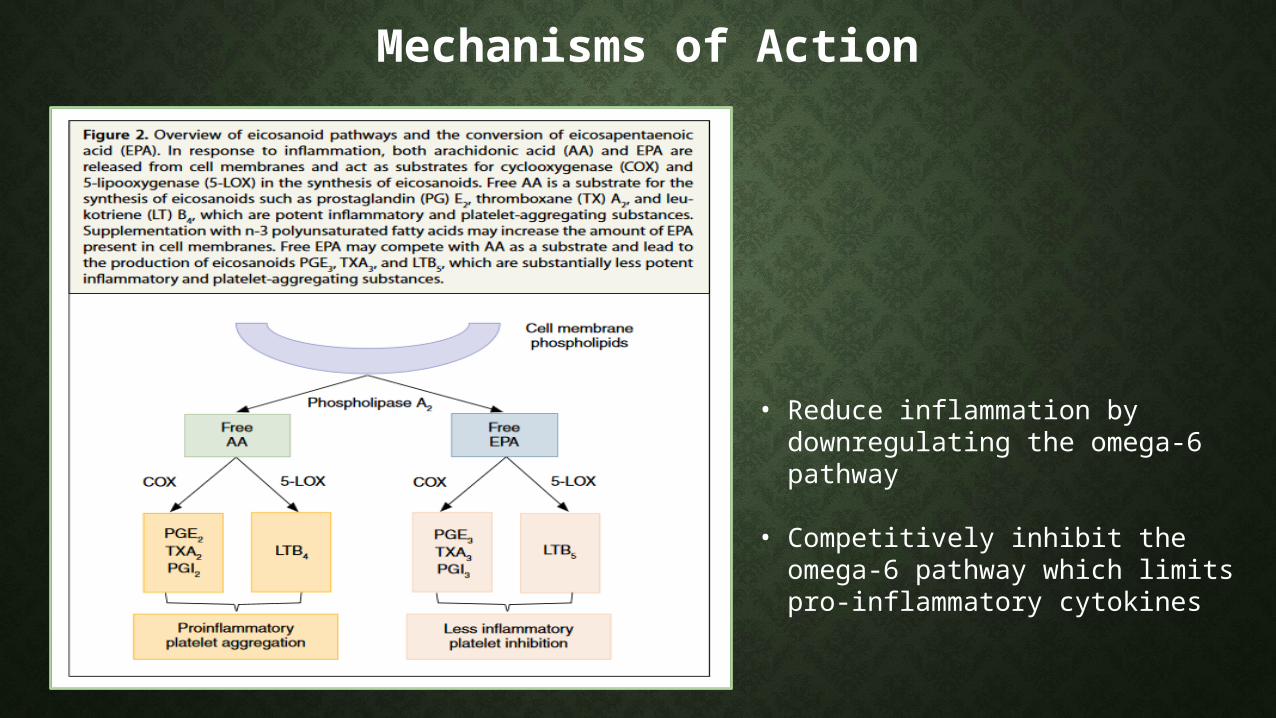
• Reduce inflammation by downregulating the omega-6 pathway
• Competitively inhibit the omega-6 pathway which limits pro-inflammatory cytokines
Early Studies (supporting)
“Alaskan and Greenland Eskimos have lower rates of colon cancer and a higher consumption of n-3 fatty acids than other North Americans (Chang, 1998).”
“It was found that n-3 and n-6 fatty acids supplemented at 20 μg/ml killed human breast, lung, and prostate cancer cells (Begin, 1986).”
“In mice with implanted colon adenocarcinoma, fish oil significantly reduced host body weight loss… and significantly reduced tumor growth rate…Fish oil is a nontoxic, highly effective anticachectic agent (Tisdale, 1990).”
“Relatively low concentrations of EPA are able to inhibit the growth, in vitro, of three human pancreatic cell lines (Falconer, 1994).”
“PUFAs significantly inhibit the proliferation of human blood lymphocytes (Calder, 1992).”
“Dietary supplementation with n-3 fatty acids suppresses interleukin-2 production and mononuclear cell proliferation (Endres, 1993).”
“Administration of EPA to AH-130 bearing rats was completely ineffective either in preventing tissue waste or in reducing tumor growth (Costelli, 1995).”
“Omega-3 PUFAs promote 10x more colon cancer metastasis in the rat liver (Griffini, 1998).”
“A predominant number of studies have shown diminished cell-mediated immune function and delayed type of hypersensitivity as a result of n-3 PUFA supplementation (Furst, 2000).”
Early Studies (opposing)
Controversy While many epidemiological, cell, and animal studies show that N-3 PUFAs are beneficial, there are just as many that show no effect or a negative effect. Furthermore, many human studies, and most large-scale clinical human trials, show no effect or a negative effect.
Secondly, Omega-3 PUFAs have been shown to significantly reduce the immune system. A highly undesirable effect in advanced cancer patients who are already immuno-compromised.
Lastly, most cachectic patients have limited appetites and early satiety. Therefore, the focus should be put on taking advantage of feeding opportunities in order to provide patients with adequate calories and protein, instead of omega-3s.
Literature review
Supporting Articles
Three Percent Dietary Fish Oil Concentrate Increased Efficacy of Doxorubicin Against MDA-MB 231 Breast Cancer Xenografts(Hardman et al. 2001)Purpose: To determine if a small amount of fish oil concentrate (FOC) can be an effective adjuvant to chemotherapy, and to determine if it will increase the toxicity of the drug to the host. Methods: Breast cancer cells were injected into mice who were kept on a diet containing 5% corn oil. After 3 weeks, once the tumor was established, mice were subdivided into two groups Group 1 (CO): Maintained on the corn oil diet Group 2 (FOC): Addition of 3% fish oil to the dietMice were kept on diets for 2 weeks, when Doxorubicin (DOX) was then given for 5 weeks
Measurements: Antioxidants SOD, GPX, tumor growth rate, body weight, blood cell counts
Results
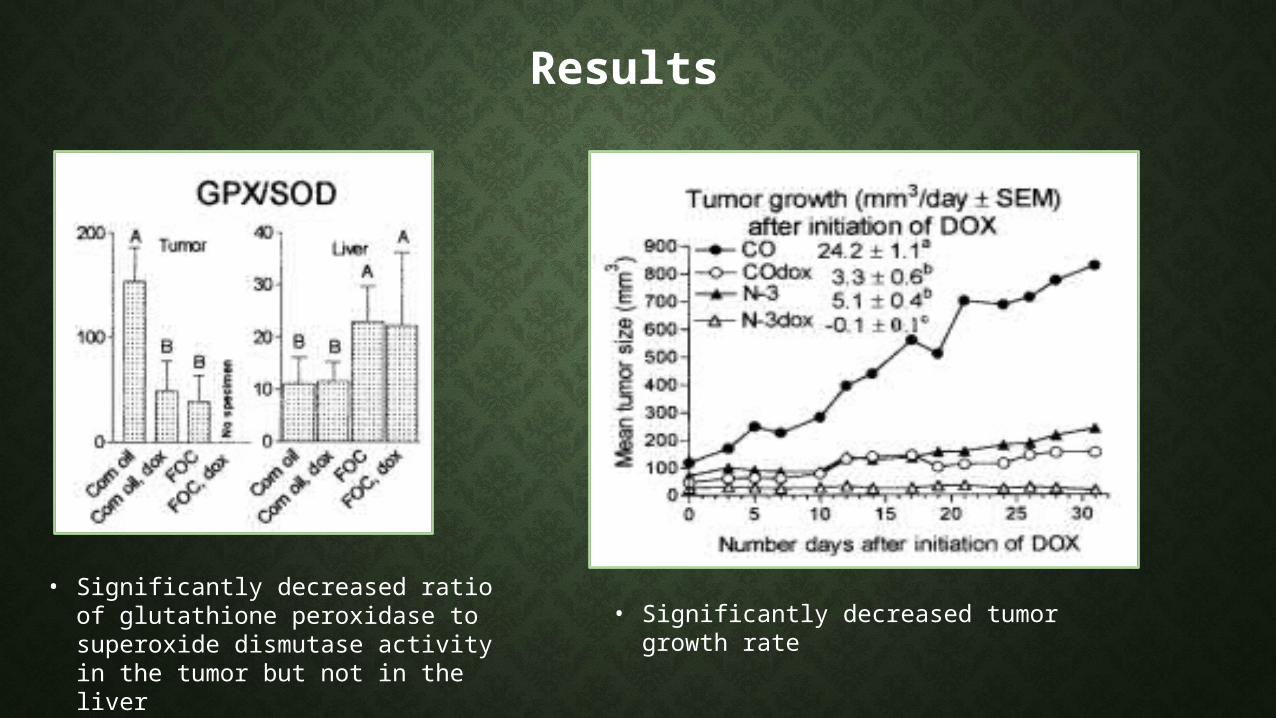
• Significantly decreased ratio of glutathione peroxidase to superoxide dismutase activity in the tumor but not in the liver
• Significantly decreased tumor growth rate
Nutritional Intervention With Fish Oil Provides a Benefit Over Standard of Care for Weight and Skeletal Muscle Mass in Patients With Nonsmall Cell Lung Cancer Receiving Chemotherapy (Murphy et al. 2011)
Purpose: To examine the effect of nutritional intervention with fish oil (FO) on weight and body composition against standard of care (SOC) during the course of chemotherapy.
Methods: Subjects with NSCLC were assigned to 1 of 2 groups for 6 weeksGroup 1 (FO): Standard of care + 2.2g EPA/day (N=16)Group 2 (SOC): Standard of care only (N=24)
Measurements: Skeletal muscle and adipose tissue CT images, blood samples at baseline, 1, and 3 weeks of intervention.
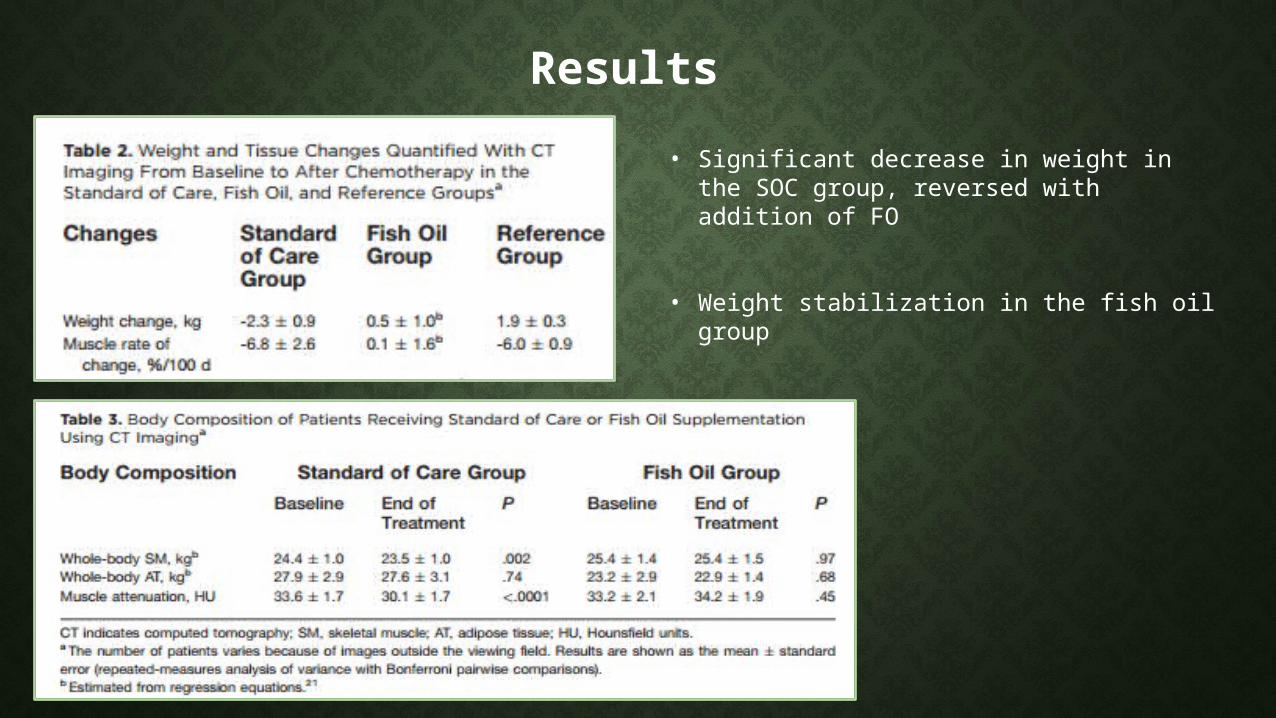
Results • Significant decrease in weight in the SOC
group, reversed with addition of FO
• Weight stabilization in the fish oil group
Effect of n-3 fatty acids on patients with advanced lung cancer: a double-blind, placebo-controlled study(Finocchiaro et al. 2011)
Purpose: To investigate the effect of fish-oil components, EPA + DHA, v. placebo, on inflammatory condition, and oxidative and nutritional statuses, in patients with lung cancer.
Methods: NSCLC patients receiving chemo were divided into two groups for 66 daysGroup 1: 4 capsules (850 mg) of EPA + DHA/day (N=19)Group 2: 850 mg of placebo (N=14)
Measurements: Inflammatory and oxidative parameters and anthropometrics taken at day 0, day 8, day 22, and day 66
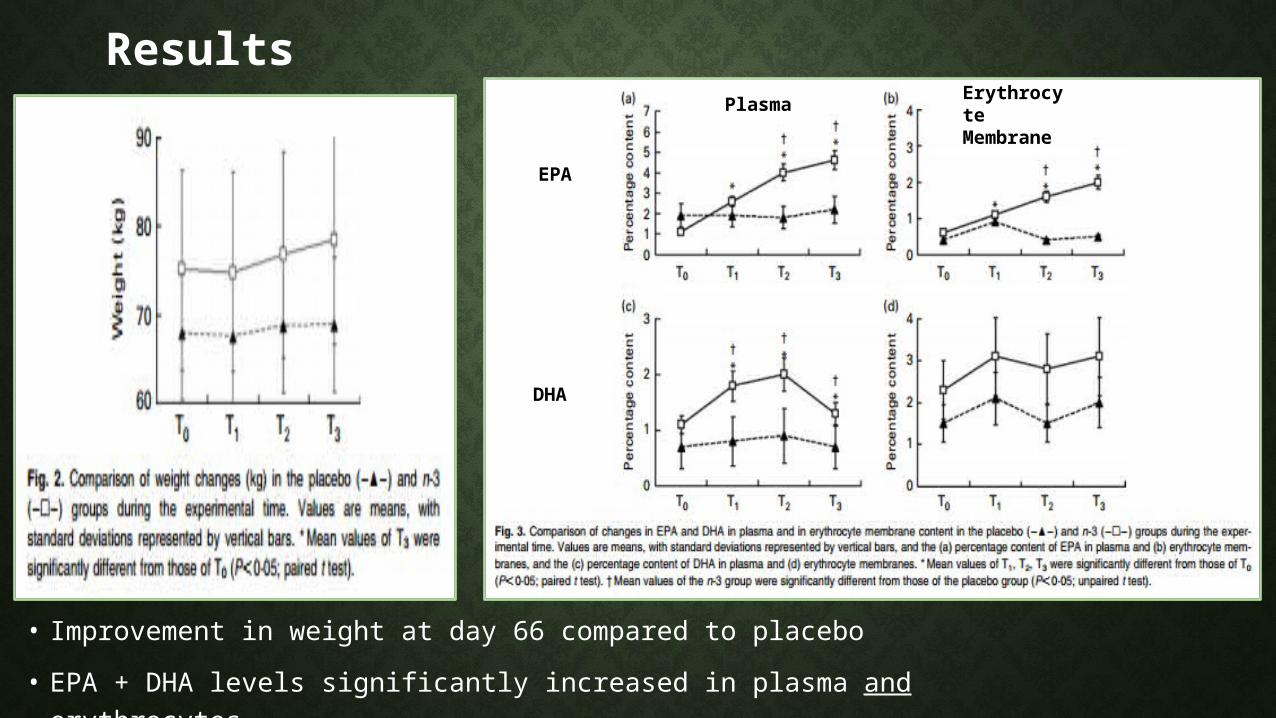
Results
• Improvement in weight at day 66 compared to placebo• EPA + DHA levels significantly increased in plasma and erythrocytes
Plasma Erythrocyte Membrane EPA
DHA
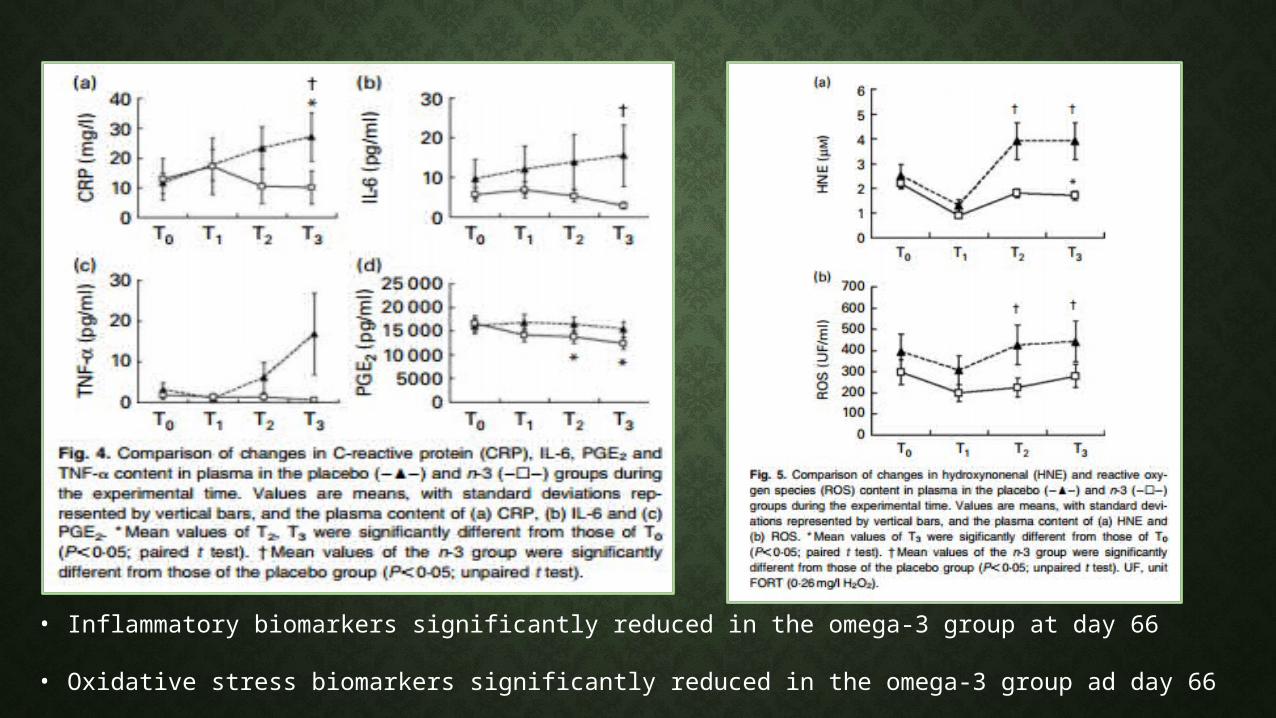
• Inflammatory biomarkers significantly reduced in the omega-3 group at day 66
• Oxidative stress biomarkers significantly reduced in the omega-3 group ad day 66
Omega-3 fatty acid-, micronutrient-, and probiotic-enriched nutrition helps body weight stabilization in head and neck cancer cachexia(Yeh et al. 2013)
Purpose: To evaluate the effects of oral nutritional supplements enriched with omega-3 fatty acids, micronutrients, and probiotics have on the improvement of BW, albumin and prealbumin concentrations, and survival rates in HNC patients with cachexia.
Methods: Subjects with HNC were randomly assigned to one of two groups for 3 months. Group 1: Ethanwell/Ethanyzme (EE) formula: fatty acids, micronutrients, probiotics (N=31)Group 2: Control (Isocal) (N=37)
Measurements: Bodyweight, anthropometrics, and blood samples
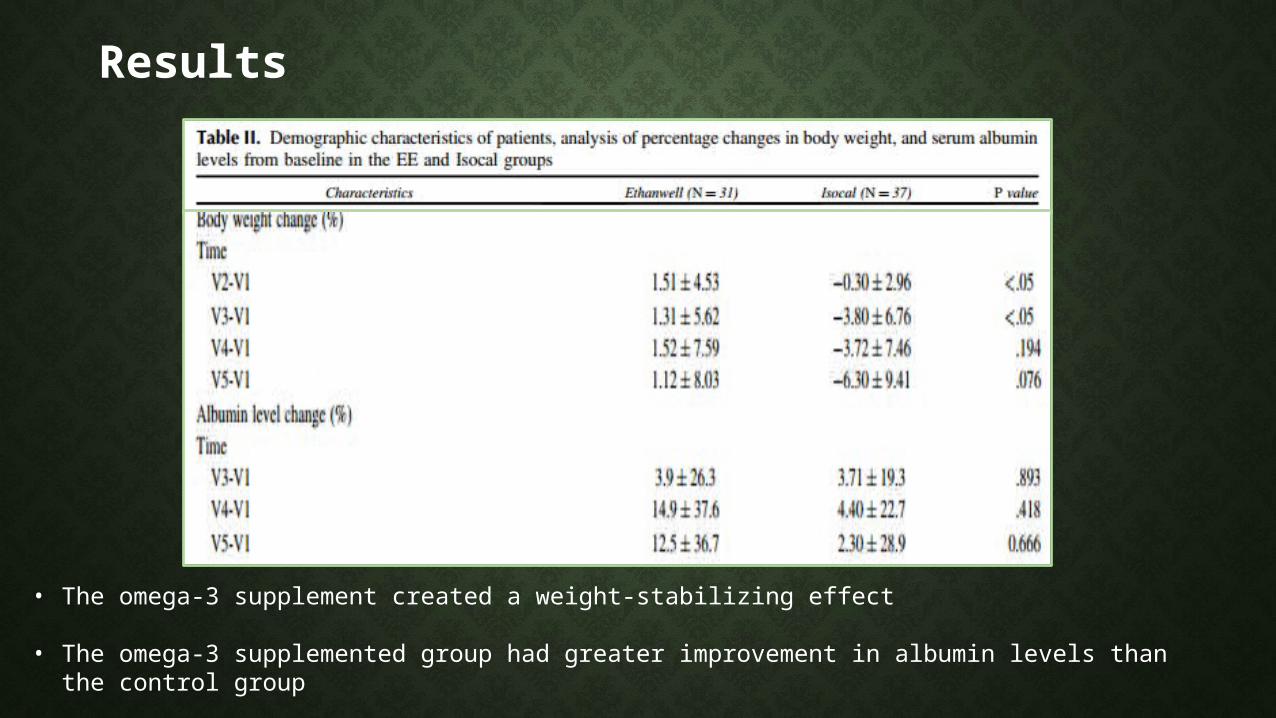
Results
• The omega-3 supplement created a weight-stabilizing effect
• The omega-3 supplemented group had greater improvement in albumin levels than the control group
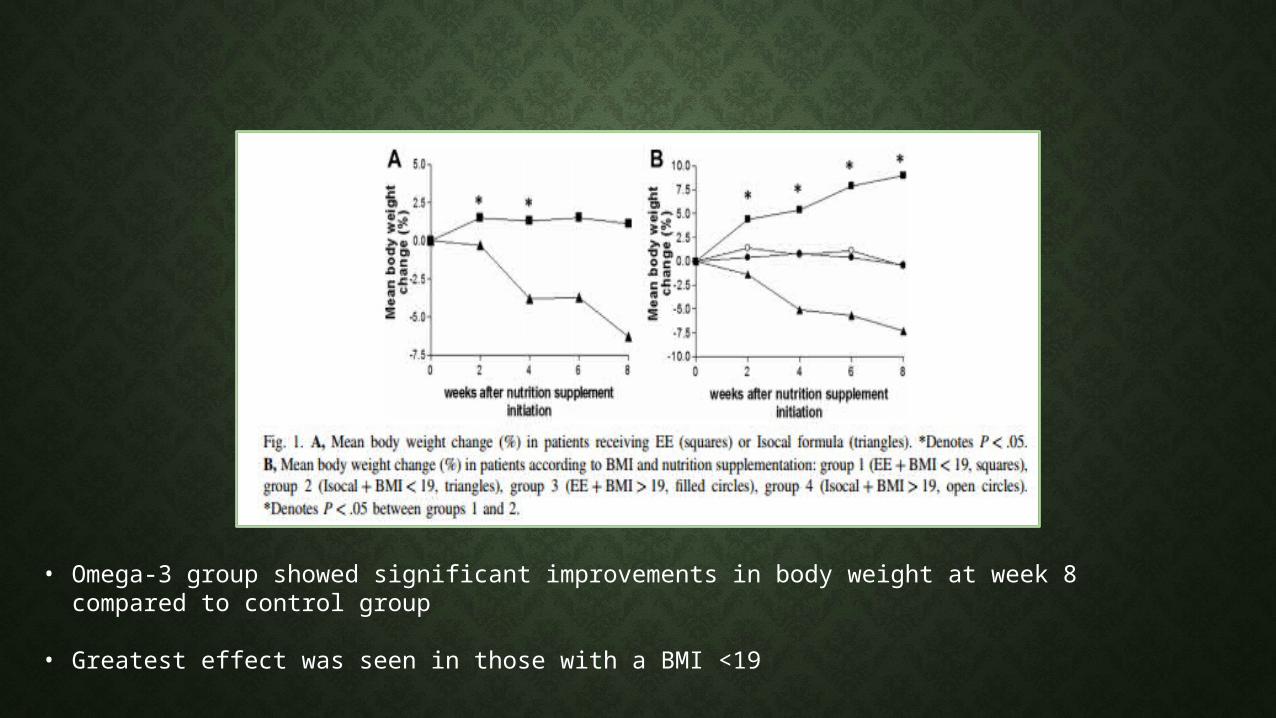
• Omega-3 group showed significant improvements in body weight at week 8 compared to control group
• Greatest effect was seen in those with a BMI <19
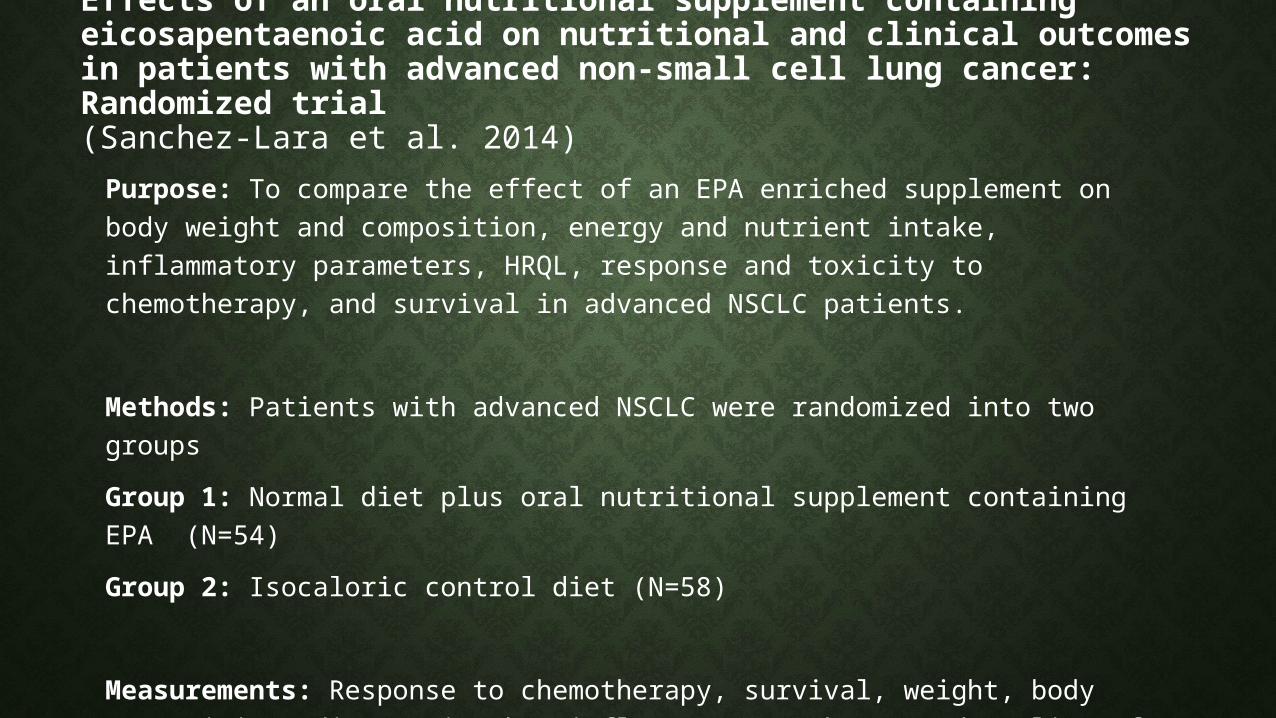
Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomized trial(Sanchez-Lara et al. 2014)
Purpose: To compare the effect of an EPA enriched supplement on body weight and composition, energy and nutrient intake, inflammatory parameters, HRQL, response and toxicity to chemotherapy, and survival in advanced NSCLC patients.
Methods: Patients with advanced NSCLC were randomized into two groups Group 1: Normal diet plus oral nutritional supplement containing EPA (N=54)Group 2: Isocaloric control diet (N=58)
Measurements: Response to chemotherapy, survival, weight, body composition, dietary intake, inflammatory markers, and quality of life
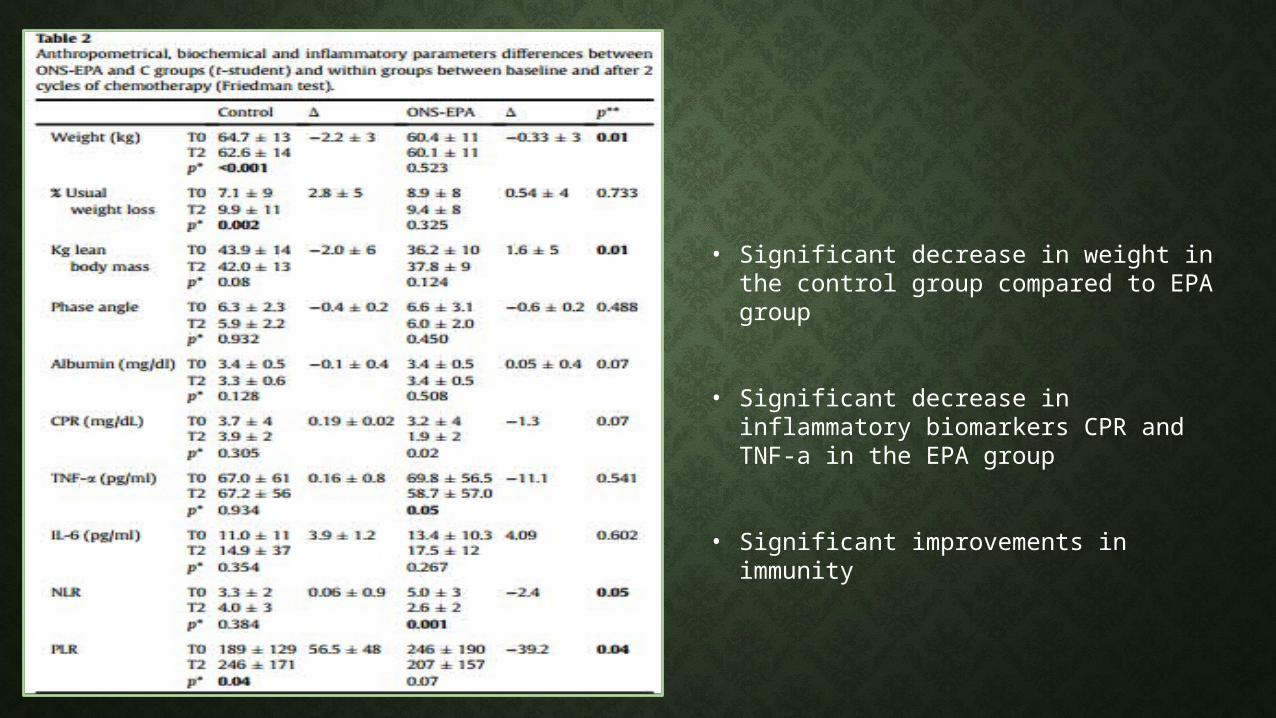
• Significant decrease in weight in the control group compared to EPA group
• Significant decrease in inflammatory biomarkers CPR and TNF-a in the EPA group
• Significant improvements in immunity
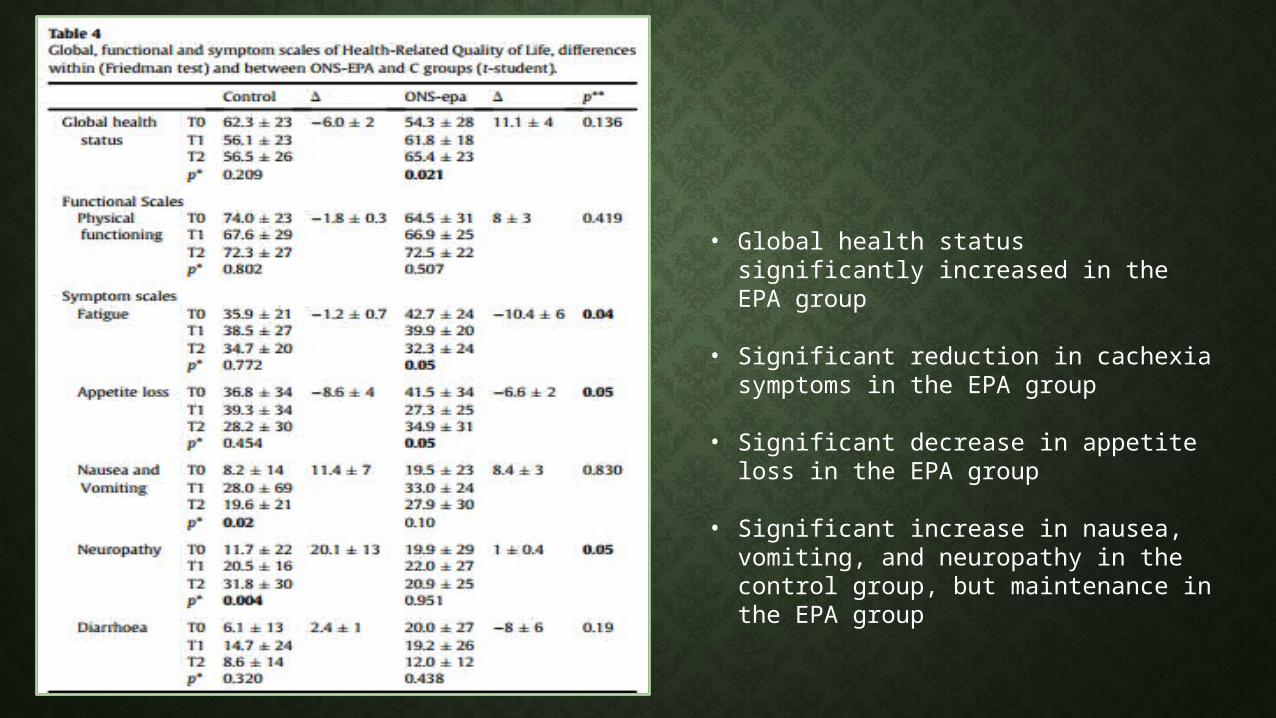
• Global health status significantly increased in the EPA group
• Significant reduction in cachexia symptoms in the EPA group
• Significant decrease in appetite loss in the EPA group
• Significant increase in nausea, vomiting, and neuropathy in the control group, but maintenance in the EPA group
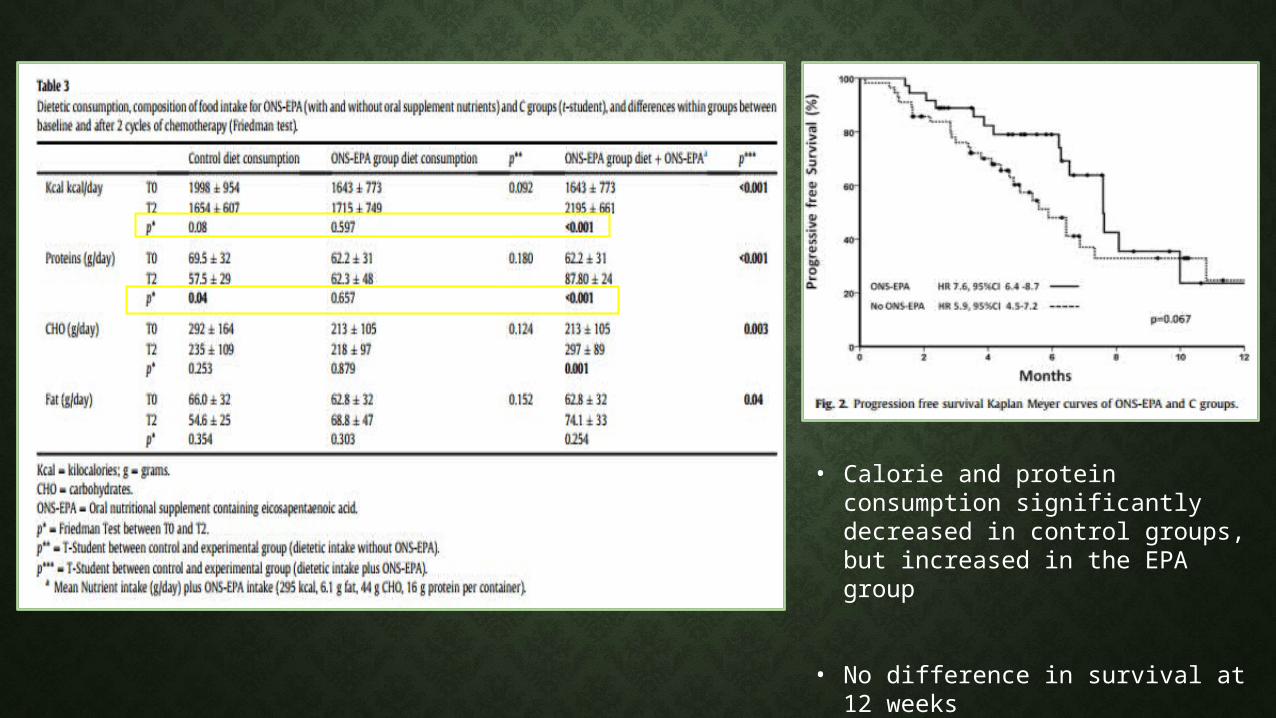
• Calorie and protein consumption significantly decreased in control groups, but increased in the EPA group
• No difference in survival at 12 weeks
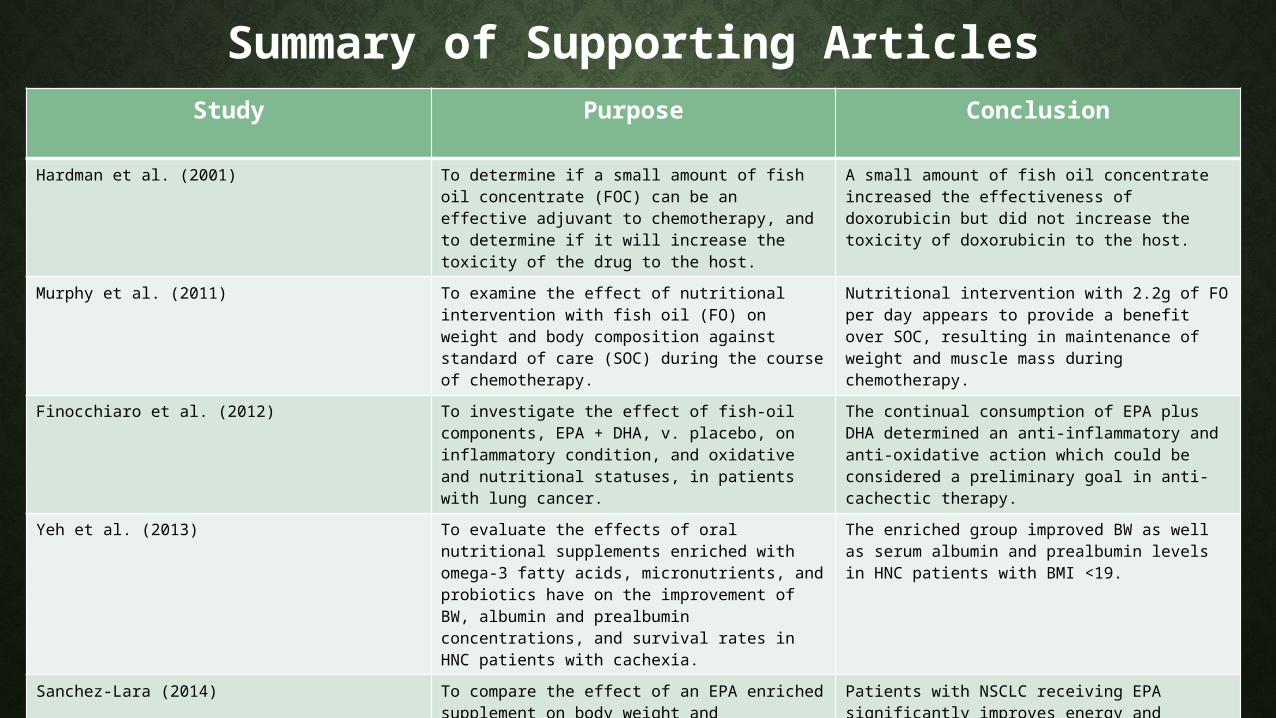
Summary of Supporting ArticlesStudy Purpose Conclusion
Hardman et al. (2001) To determine if a small amount of fish oil concentrate (FOC) can be an effective adjuvant to chemotherapy, and to determine if it will increase the toxicity of the drug to the host.
A small amount of fish oil concentrate increased the effectiveness of doxorubicin but did not increase the toxicity of doxorubicin to the host.
Murphy et al. (2011) To examine the effect of nutritional intervention with fish oil (FO) on weight and body composition against standard of care (SOC) during the course of chemotherapy.
Nutritional intervention with 2.2g of FO per day appears to provide a benefit over SOC, resulting in maintenance of weight and muscle mass during chemotherapy.
Finocchiaro et al. (2012) To investigate the effect of fish-oil components, EPA + DHA, v. placebo, on inflammatory condition, and oxidative and nutritional statuses, in patients with lung cancer.
The continual consumption of EPA plus DHA determined an anti-inflammatory and anti-oxidative action which could be considered a preliminary goal in anti-cachectic therapy.
Yeh et al. (2013) To evaluate the effects of oral nutritional supplements enriched with omega-3 fatty acids, micronutrients, and probiotics have on the improvement of BW, albumin and prealbumin concentrations, and survival rates in HNC patients with cachexia.
The enriched group improved BW as well as serum albumin and prealbumin levels in HNC patients with BMI <19.
Sanchez-Lara (2014) To compare the effect of an EPA enriched supplement on body weight and composition, energy and nutrient intake, inflammatory parameters, HRQL, response and toxicity to chemotherapy, and survival in advanced NSCLC patients.
Patients with NSCLC receiving EPA significantly improves energy and protein intake, body composition, and decreased fatigue, loss of appetite, and neuropathy.
Literature Review
Opposing Articles
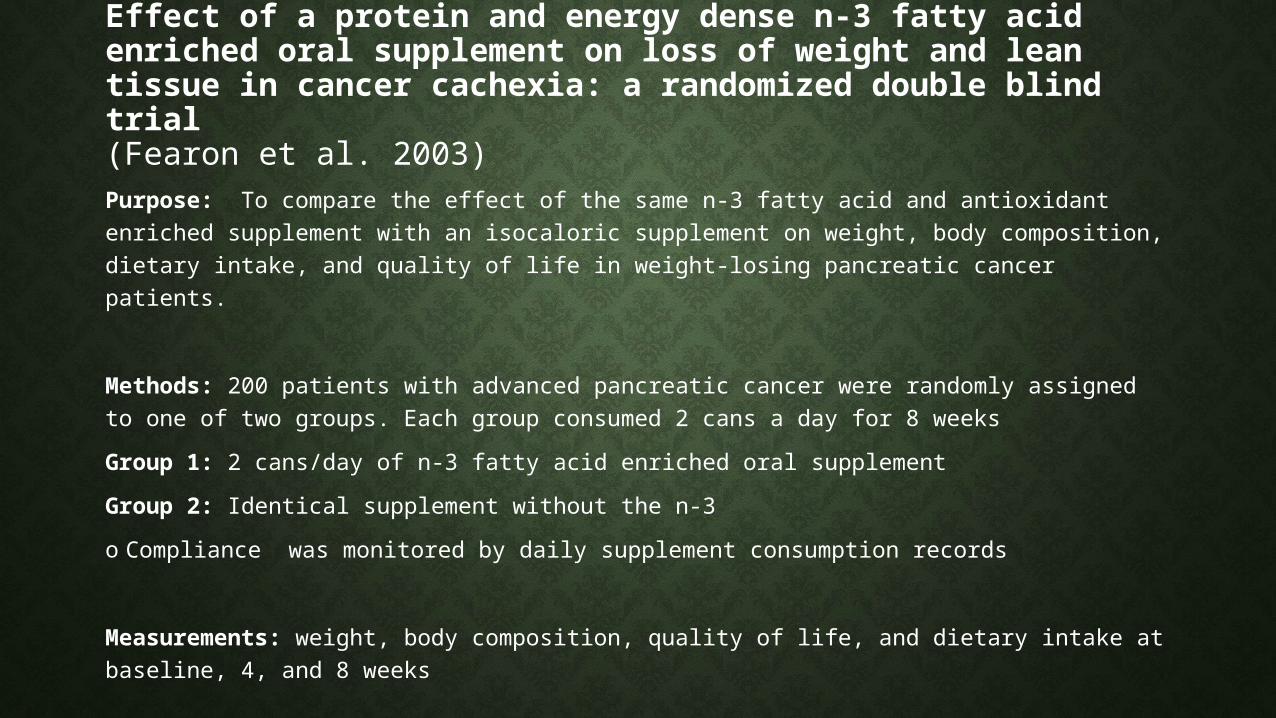
Effect of a protein and energy dense n-3 fatty acid enriched oral supplement on loss of weight and lean tissue in cancer cachexia: a randomized double blind trial(Fearon et al. 2003)Purpose: To compare the effect of the same n-3 fatty acid and antioxidant enriched supplement with an isocaloric supplement on weight, body composition, dietary intake, and quality of life in weight-losing pancreatic cancer patients.
Methods: 200 patients with advanced pancreatic cancer were randomly assigned to one of two groups. Each group consumed 2 cans a day for 8 weeksGroup 1: 2 cans/day of n-3 fatty acid enriched oral supplementGroup 2: Identical supplement without the n-3o Compliance was monitored by daily supplement consumption records
Measurements: weight, body composition, quality of life, and dietary intake at baseline, 4, and 8 weeks
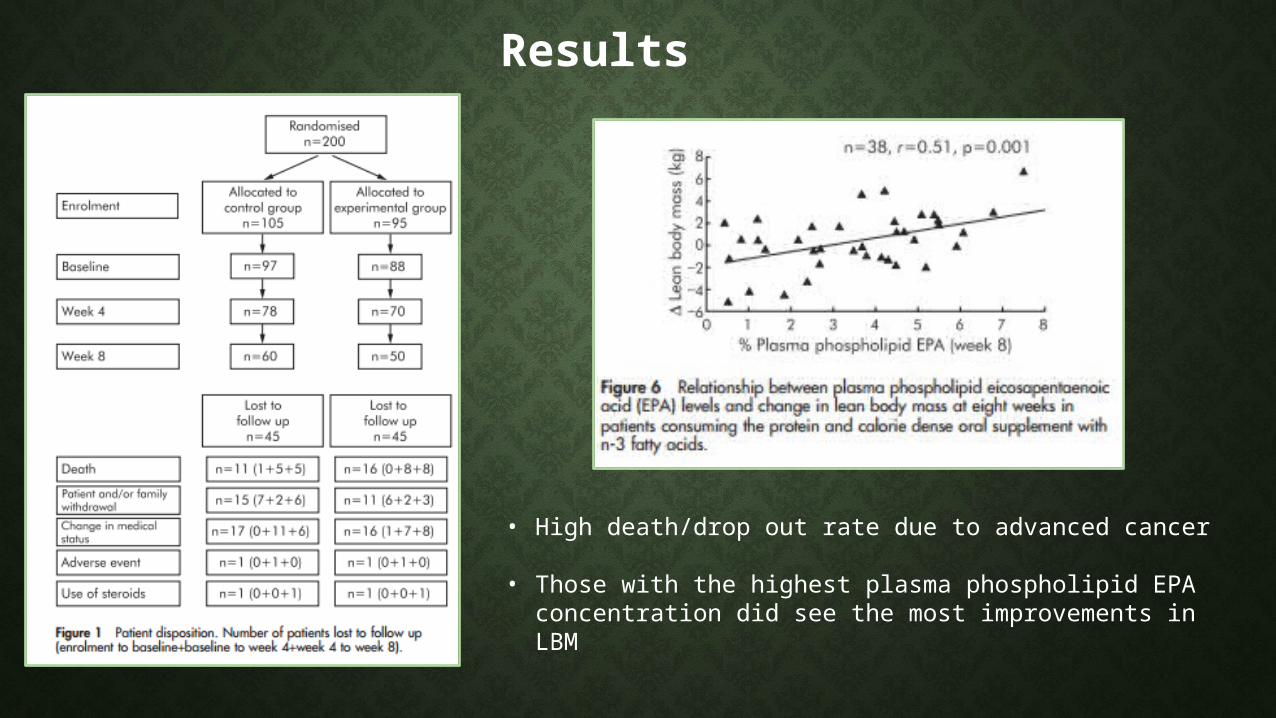
Results
• High death/drop out rate due to advanced cancer
• Those with the highest plasma phospholipid EPA concentration did see the most improvements in LBM
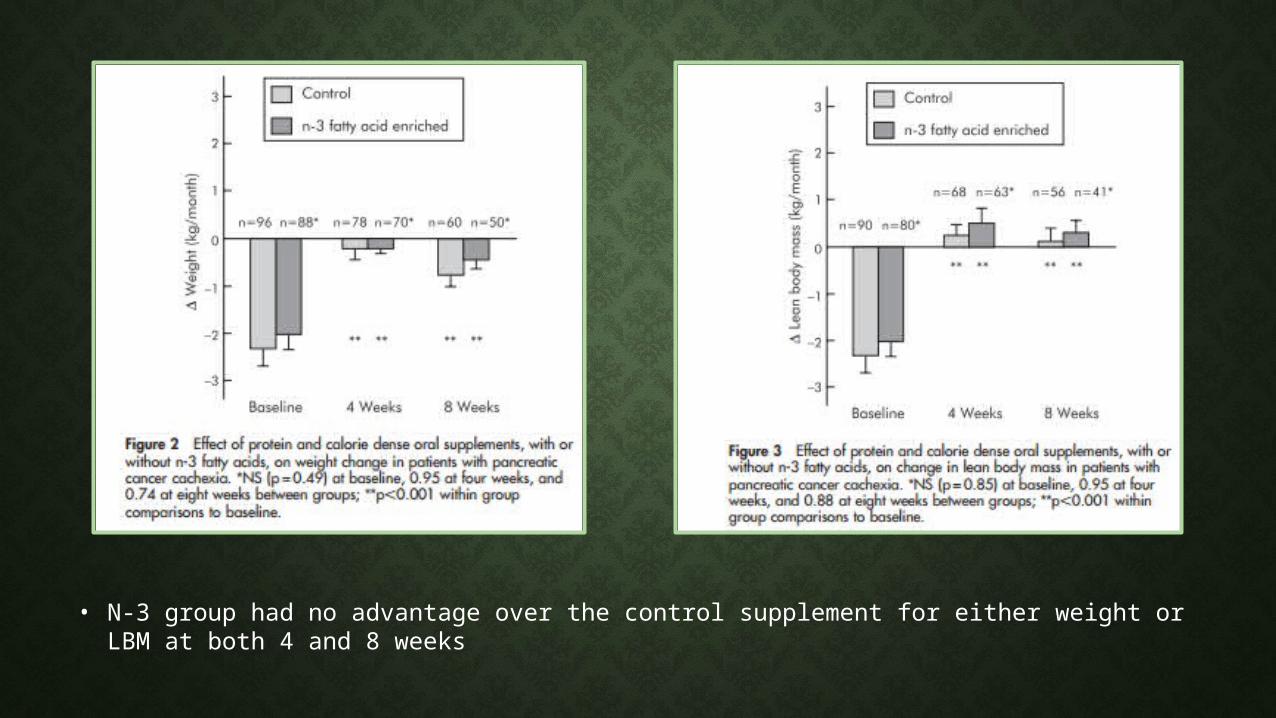
• N-3 group had no advantage over the control supplement for either weight or LBM at both 4 and 8 weeks
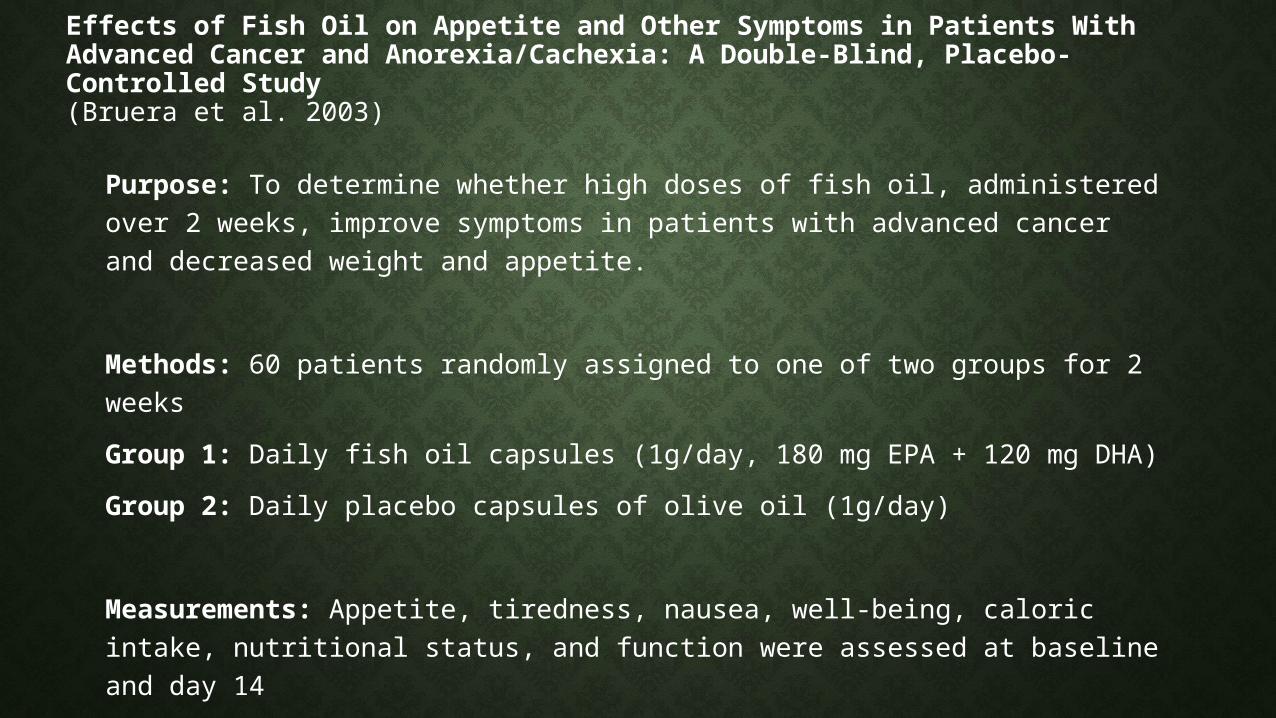
Effects of Fish Oil on Appetite and Other Symptoms in Patients With Advanced Cancer and Anorexia/Cachexia: A Double-Blind, Placebo-Controlled Study (Bruera et al. 2003)
Purpose: To determine whether high doses of fish oil, administered over 2 weeks, improve symptoms in patients with advanced cancer and decreased weight and appetite.
Methods: 60 patients randomly assigned to one of two groups for 2 weeksGroup 1: Daily fish oil capsules (1g/day, 180 mg EPA + 120 mg DHA)Group 2: Daily placebo capsules of olive oil (1g/day)
Measurements: Appetite, tiredness, nausea, well-being, caloric intake, nutritional status, and function were assessed at baseline and day 14
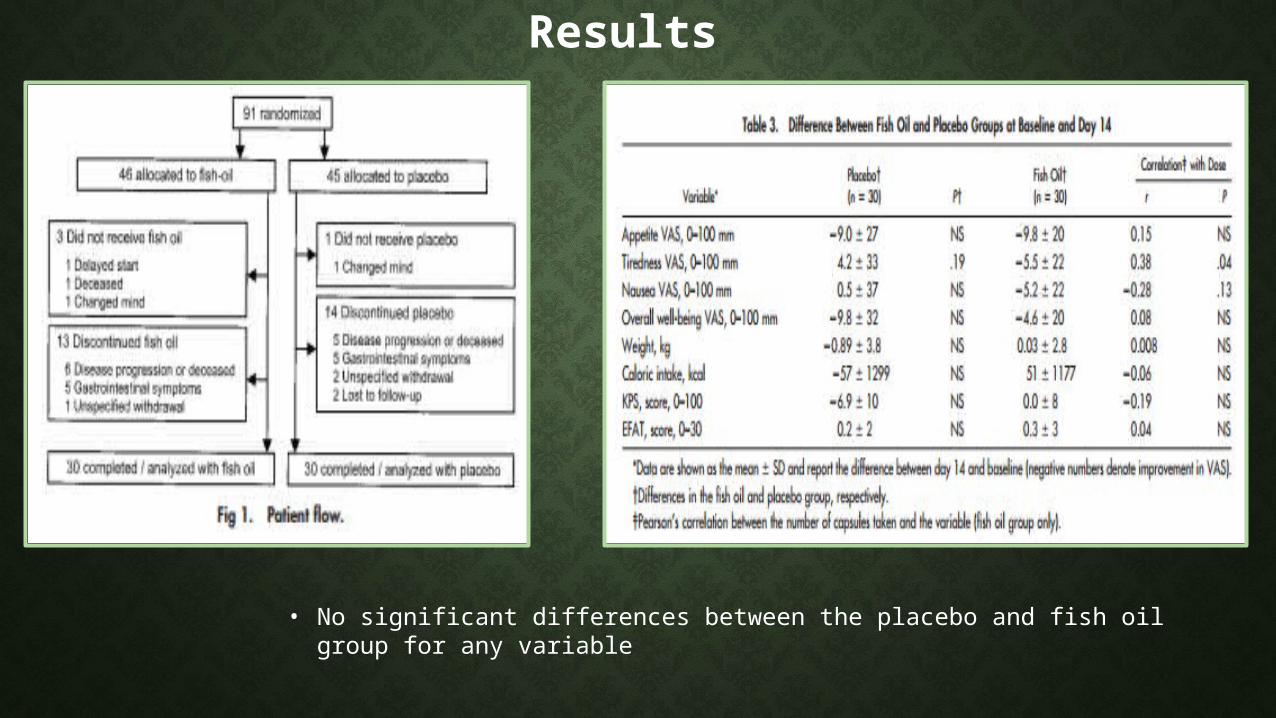
Results
• No significant differences between the placebo and fish oil group for any variable
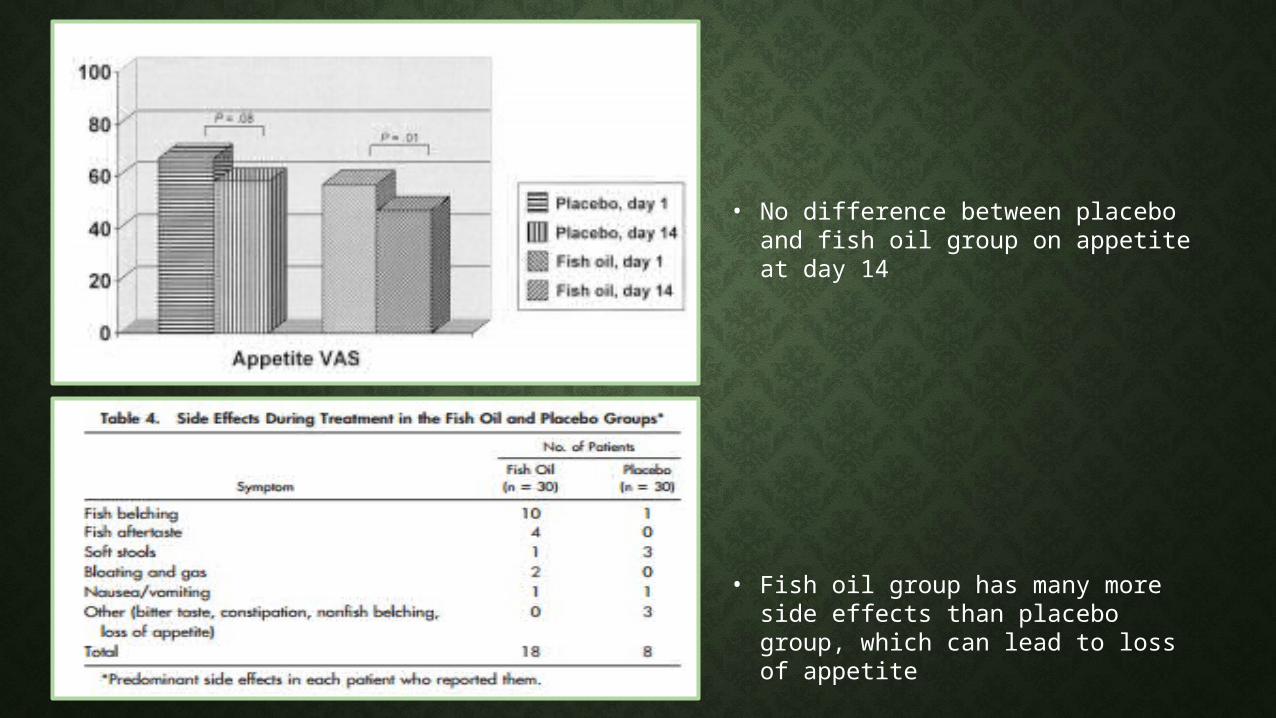
• No difference between placebo and fish oil group on appetite at day 14
• Fish oil group has many more side effects than placebo group, which can lead to loss of appetite
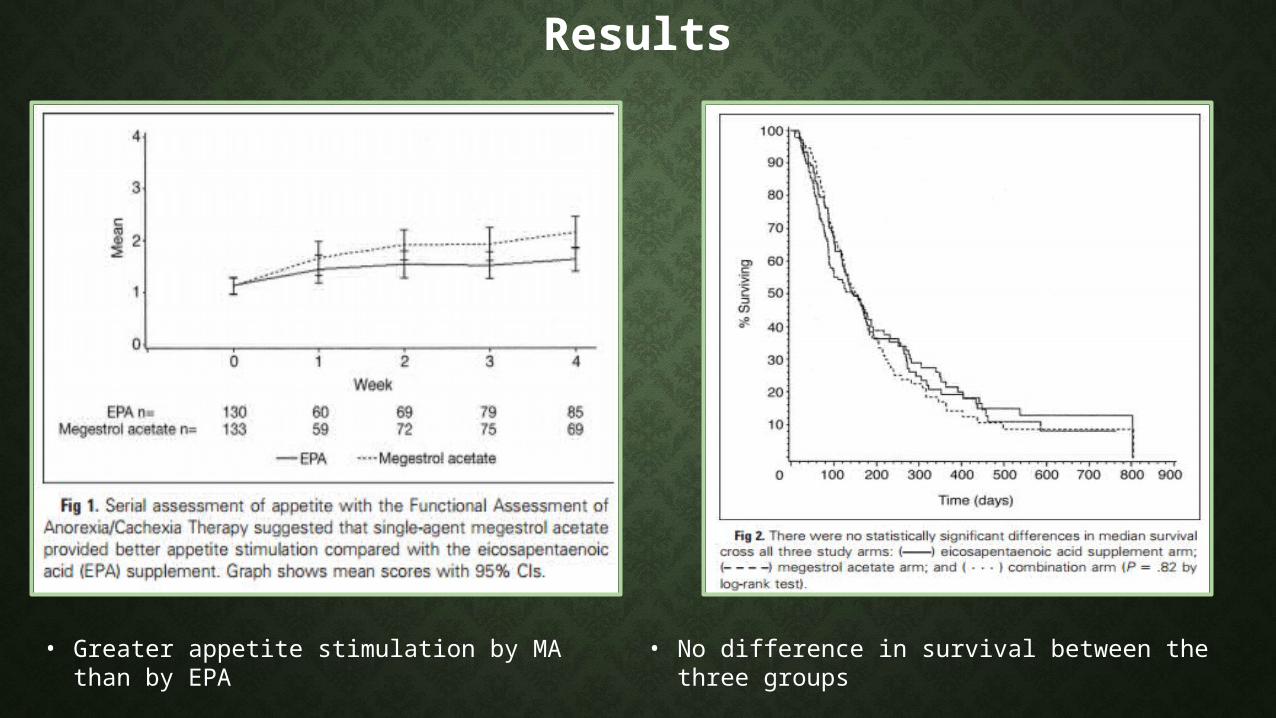
An EPA Supplement vs. Megestrol Acetate vs. Both for Patients with Cancer-Associated Wasting: A North Central Cancer Treatment Group and National Cancer Institute of Canada Collaborative Effort (Jatoi et al. 2004)
Purpose: To determine if an EPA supplement, administered alone or with megestrol acetate, was more effective than MA alone.
Methods: 421 patients with cachexia were randomly assigned to 1 of 3 groups for 3 monthsGroup 1: EPA supplement (1.09g) + placebo (N=141)Group 2: MA liquid suspension (600mg/day) + an isocaloric supplement (N=140)Group 3: Both (N=140)
Measurements: Weight, appetite, survival, quality of life, and toxicities measured every 4 weeks
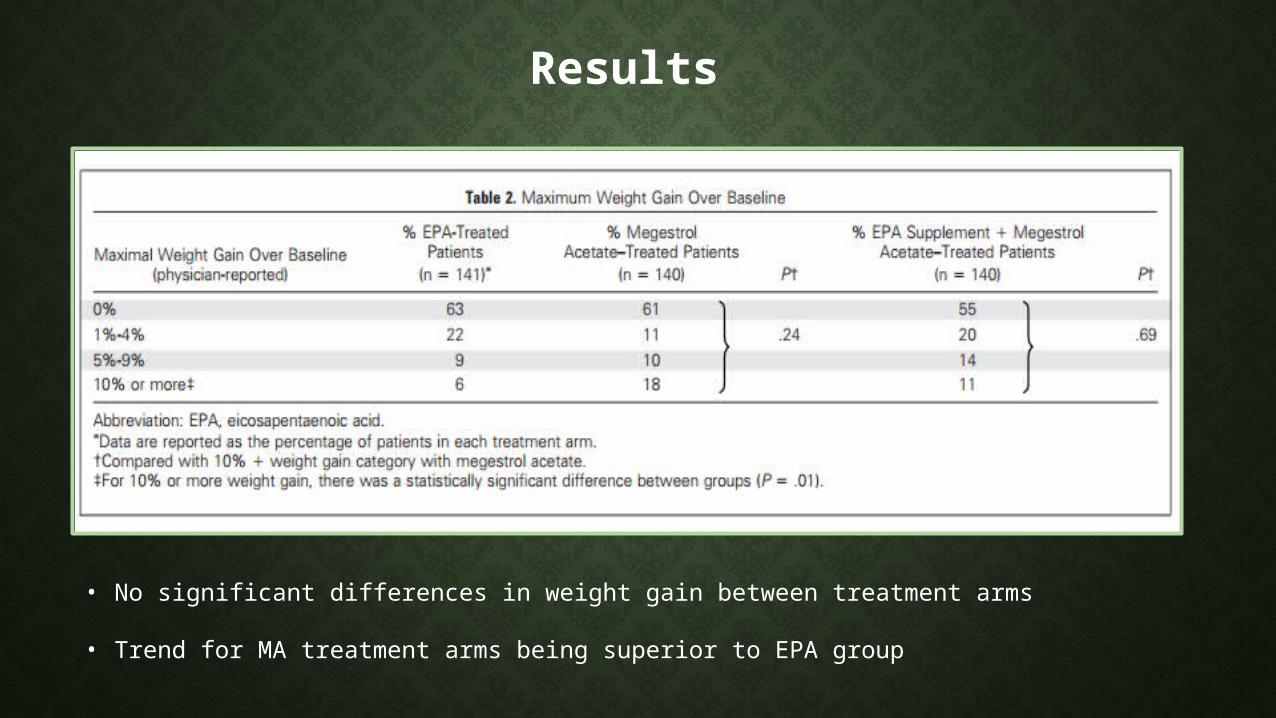
Results
• No significant differences in weight gain between treatment arms
• Trend for MA treatment arms being superior to EPA group
Results
• Greater appetite stimulation by MA than by EPA
• No difference in survival between the three groups
Impact of fish oil and melatonin on cachexia in patients with advanced gastrointestinal cancer: A randomized pilot study (Persson et al. 2005)
Purpose: To determine whether short-term intervention with large doses of FO and/or MLT combined with dietary advice in patients with advanced GI cancer could influence variables associated with cachexia development, notably cytokines.
Methods: 24 patients randomly assigned to one of two groups for 8 weeksGroup 1: Supplemented with 30 ml/day of fish oil (4.9g EPA + 3.2g DHA) (N=14)Group 2: 18 mg/day of melatonin (N=11)
Measurements: Serum levels of TNF-a, IL-IB, IL-2, IL-6, IL-8, and fatty acid concentrations were measured at baseline, week 4, and week 8
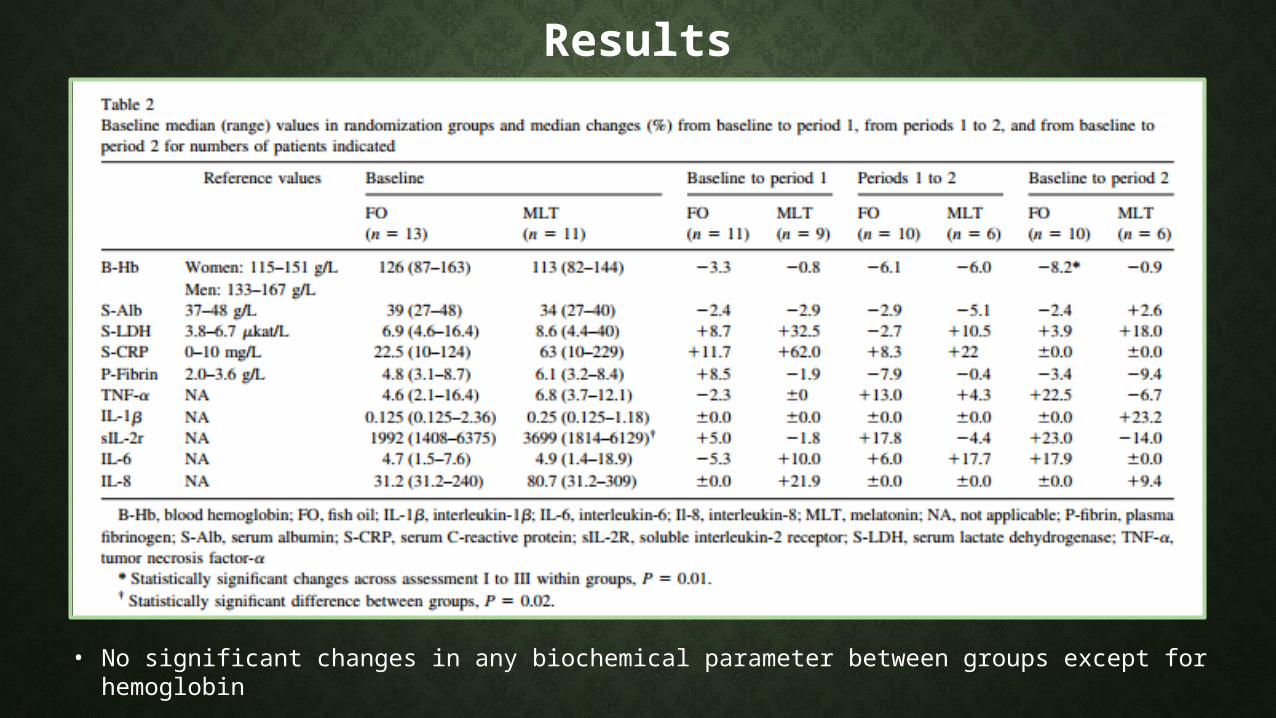
Results
• No significant changes in any biochemical parameter between groups except for hemoglobin
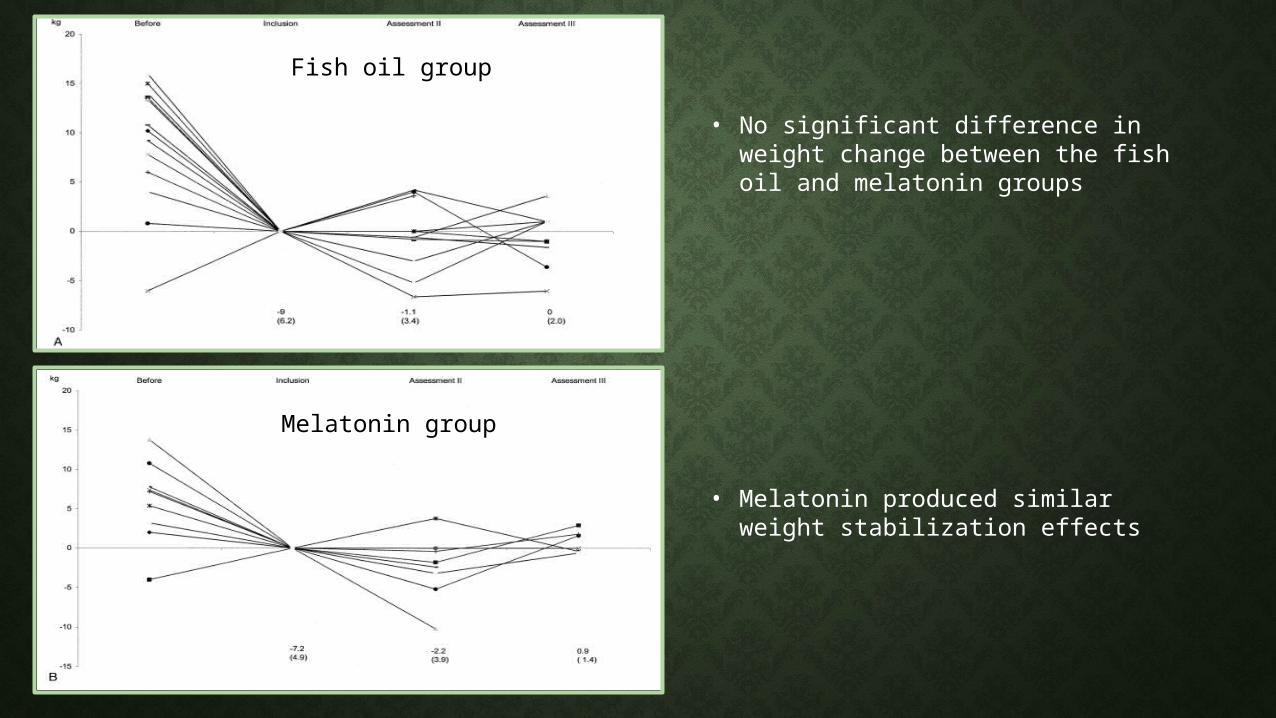
• No significant difference in weight change between the fish oil and melatonin groups
• Melatonin produced similar weight stabilization effects
Fish oil group
Melatonin group
Double-Blind, Placebo-Controlled, Randomized Study of EPA Diester in Patients With Cancer Cachexia (Fearon et al. 2006)
Purpose: To compare EPA diethyl ester with placebo in cachectic cancer patients for effects on weight loss and lean body mass.
Methods: 518 patients with advanced GI or Lung Cancer were randomly assigned to 1 of 3 groups for 8 weeksGroup 1: 2g of EPA daily (N=175)Group 2: 4g of EPA daily (N=172)Group 3: placebo (N=171)
Measurements: Survival, body weight, body composition, CRP, albumin, appetite, physical functioning, and performance status were measured at 4 and 8 weeks.
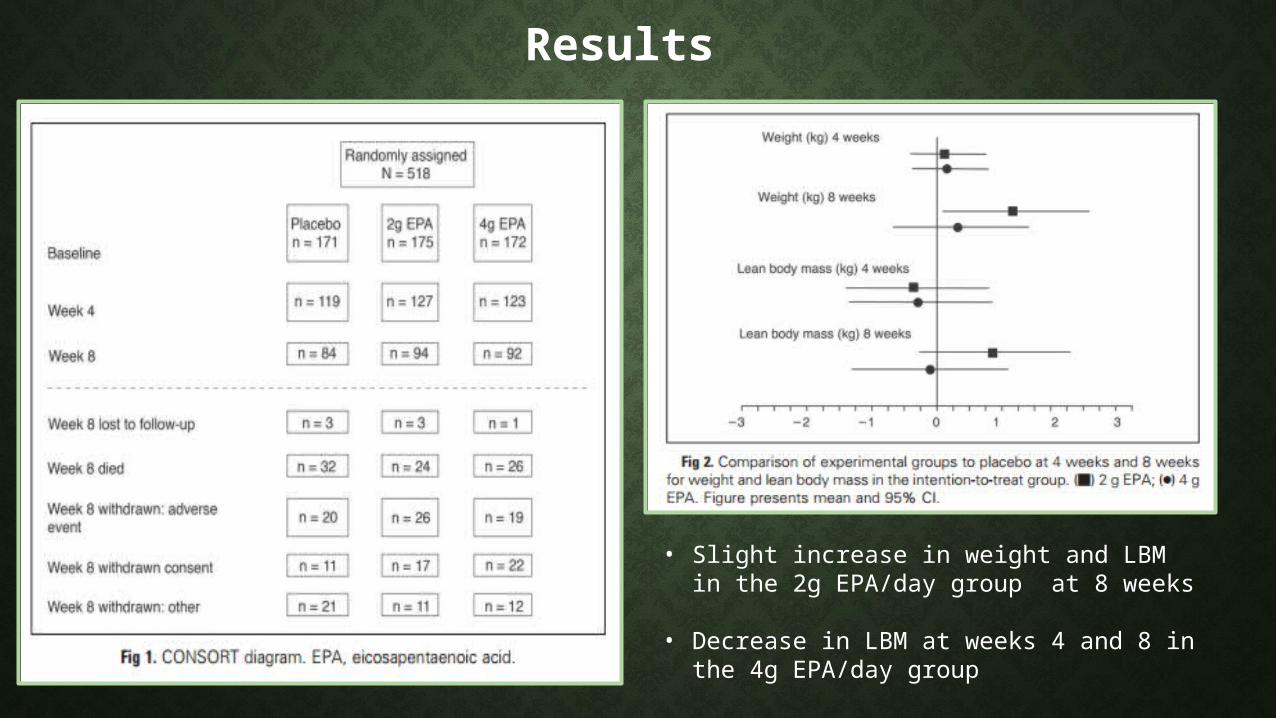
Results
• Slight increase in weight and LBM in the 2g EPA/day group at 8 weeks
• Decrease in LBM at weeks 4 and 8 in the 4g EPA/day group
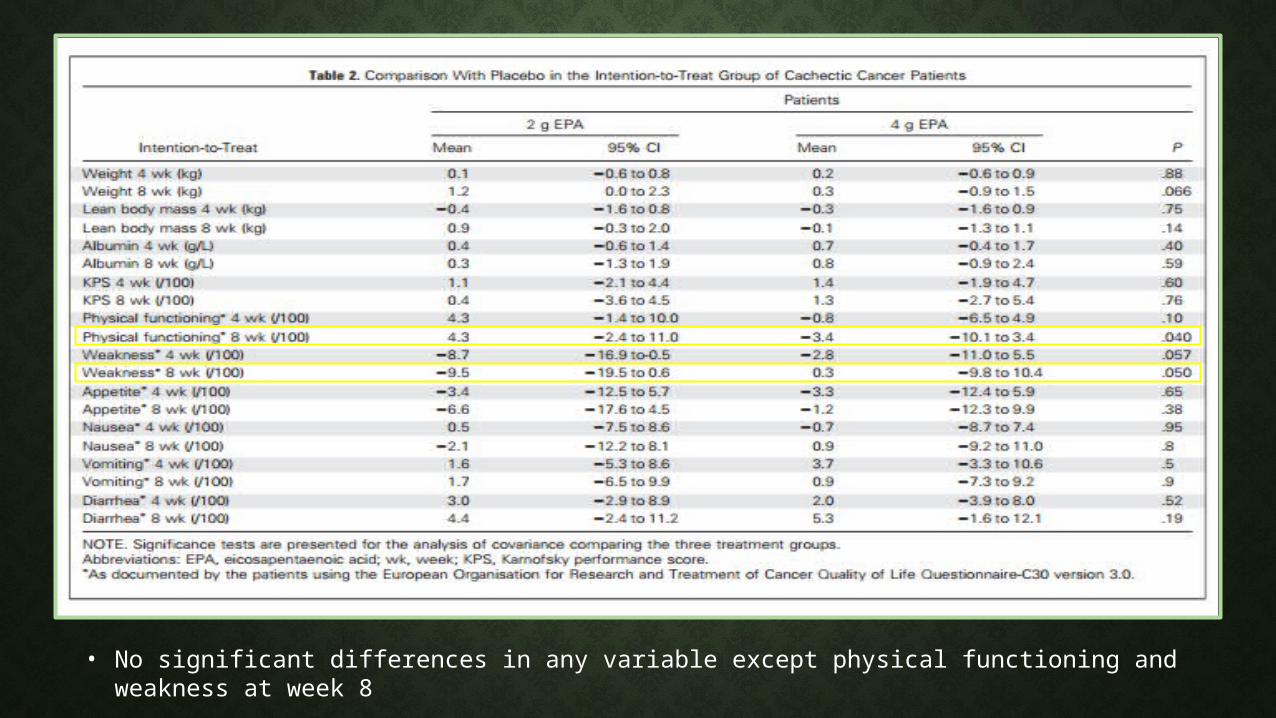
• No significant differences in any variable except physical functioning and weakness at week 8
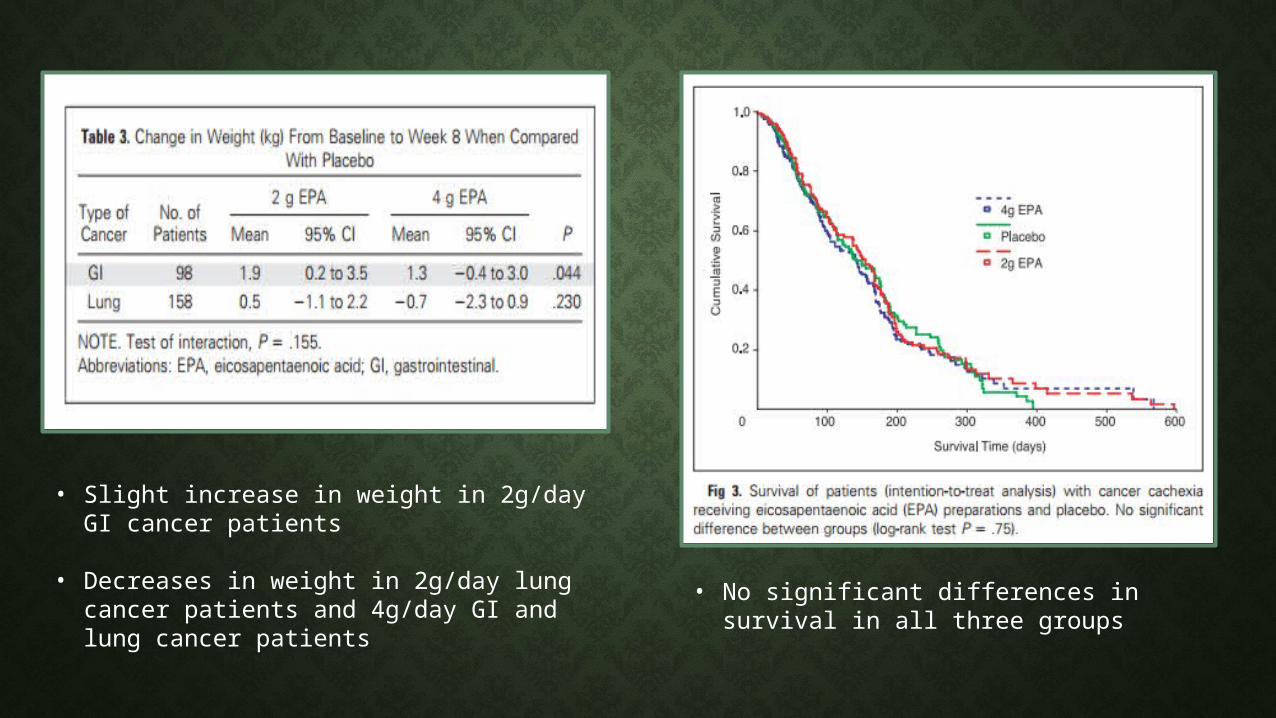
• Slight increase in weight in 2g/day GI cancer patients
• Decreases in weight in 2g/day lung cancer patients and 4g/day GI and lung cancer patients
• No significant differences in survival in all three groups
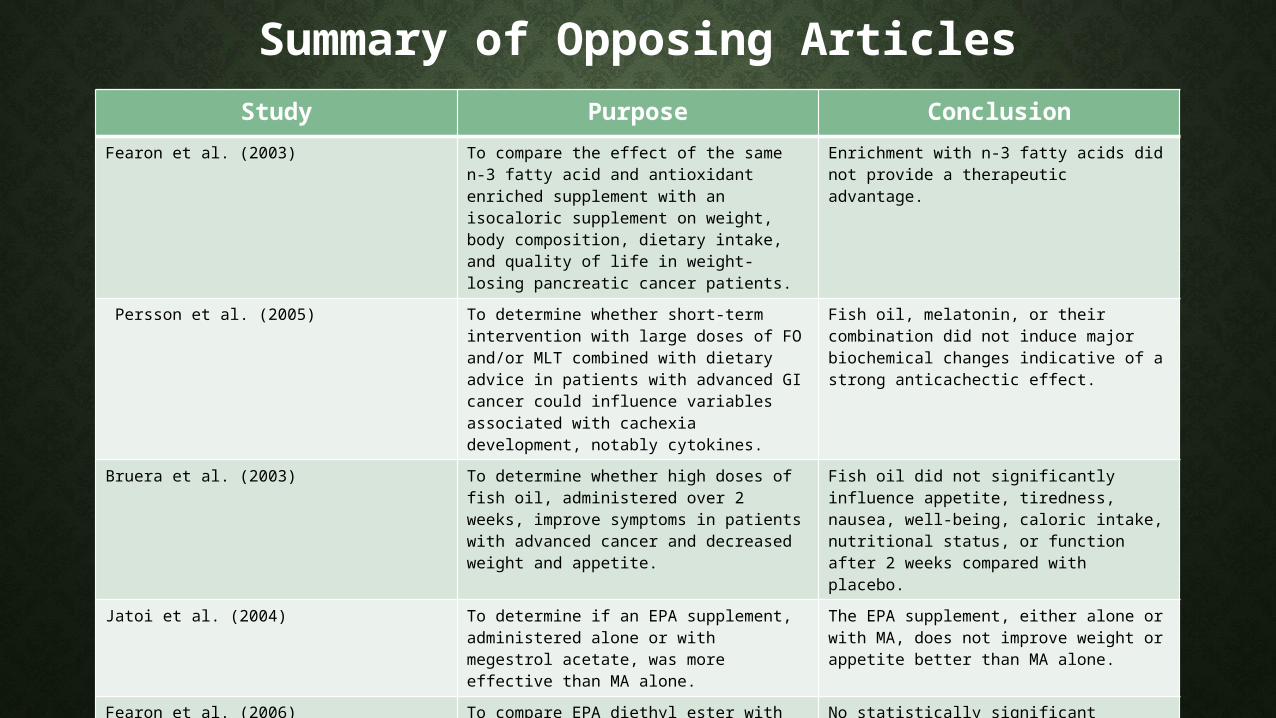
Summary of Opposing ArticlesStudy Purpose Conclusion
Fearon et al. (2003) To compare the effect of the same n-3 fatty acid and antioxidant enriched supplement with an isocaloric supplement on weight, body composition, dietary intake, and quality of life in weight-losing pancreatic cancer patients.
Enrichment with n-3 fatty acids did not provide a therapeutic advantage.
Persson et al. (2005) To determine whether short-term intervention with large doses of FO and/or MLT combined with dietary advice in patients with advanced GI cancer could influence variables associated with cachexia development, notably cytokines.
Fish oil, melatonin, or their combination did not induce major biochemical changes indicative of a strong anticachectic effect.
Bruera et al. (2003) To determine whether high doses of fish oil, administered over 2 weeks, improve symptoms in patients with advanced cancer and decreased weight and appetite.
Fish oil did not significantly influence appetite, tiredness, nausea, well-being, caloric intake, nutritional status, or function after 2 weeks compared with placebo.
Jatoi et al. (2004) To determine if an EPA supplement, administered alone or with megestrol acetate, was more effective than MA alone.
The EPA supplement, either alone or with MA, does not improve weight or appetite better than MA alone.
Fearon et al. (2006) To compare EPA diethyl ester with placebo in cachectic cancer patients for effects on weight loss and lean body mass.
No statistically significant benefit from single agent EPA in the treatment of cancer cachexia.
Discussion
Strengths & WeaknessesStance on the Controversy
ConclusionFuture Research
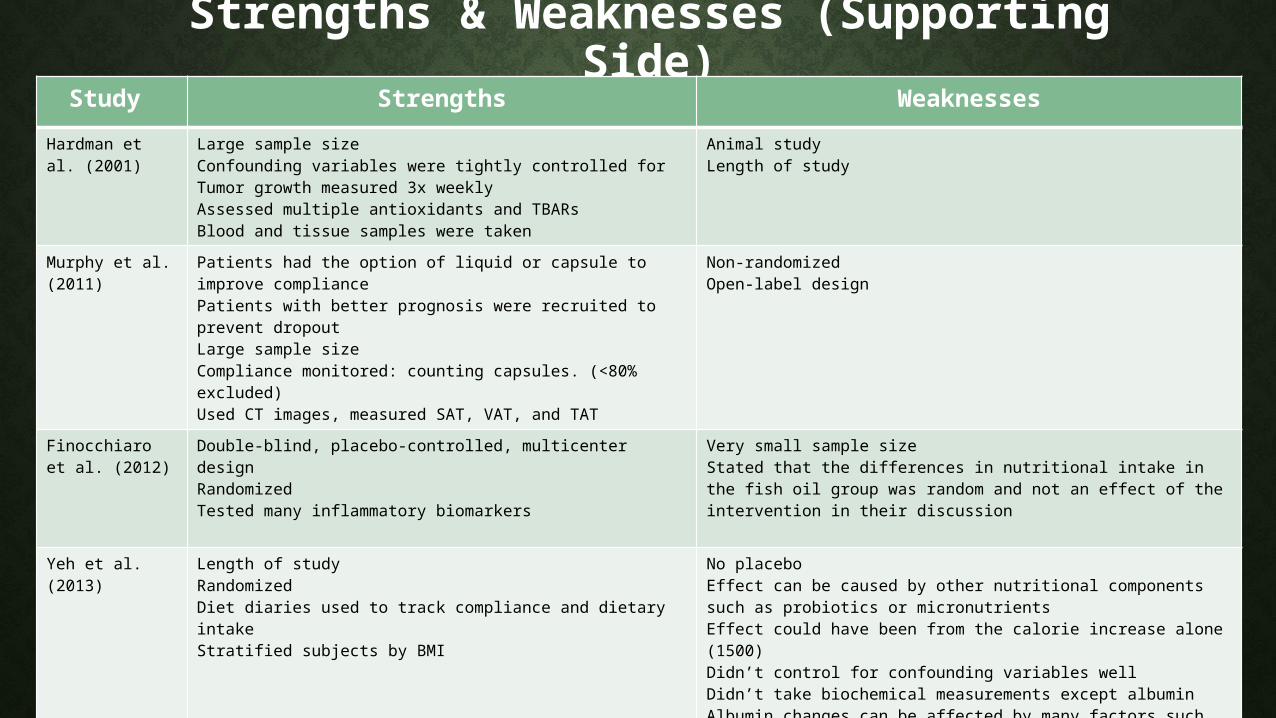
Strengths & Weaknesses (Supporting Side)
Study Strengths WeaknessesHardman et al. (2001)
Large sample size Confounding variables were tightly controlled forTumor growth measured 3x weeklyAssessed multiple antioxidants and TBARsBlood and tissue samples were taken
Animal study Length of study
Murphy et al. (2011)
Patients had the option of liquid or capsule to improve compliancePatients with better prognosis were recruited to prevent dropoutLarge sample sizeCompliance monitored: counting capsules. (<80% excluded)Used CT images, measured SAT, VAT, and TAT
Non-randomizedOpen-label design
Finocchiaro et al. (2012)
Double-blind, placebo-controlled, multicenter designRandomized Tested many inflammatory biomarkers
Very small sample sizeStated that the differences in nutritional intake in the fish oil group was random and not an effect of the intervention in their discussion
Yeh et al. (2013)
Length of study Randomized Diet diaries used to track compliance and dietary intakeStratified subjects by BMI
No placeboEffect can be caused by other nutritional components such as probiotics or micronutrients Effect could have been from the calorie increase alone (1500)Didn’t control for confounding variables wellDidn’t take biochemical measurements except albuminAlbumin changes can be affected by many factors such as inflammation
Sanchez-Lara (2014)
RandomizedMeasured anthropometric, clinical, and biochemical outcomesTracked macronutrient and caloric intake in each group
No placeboUsed BIA to assess body composition Didn’t measure plasma phospholipid levels High rate of attrition
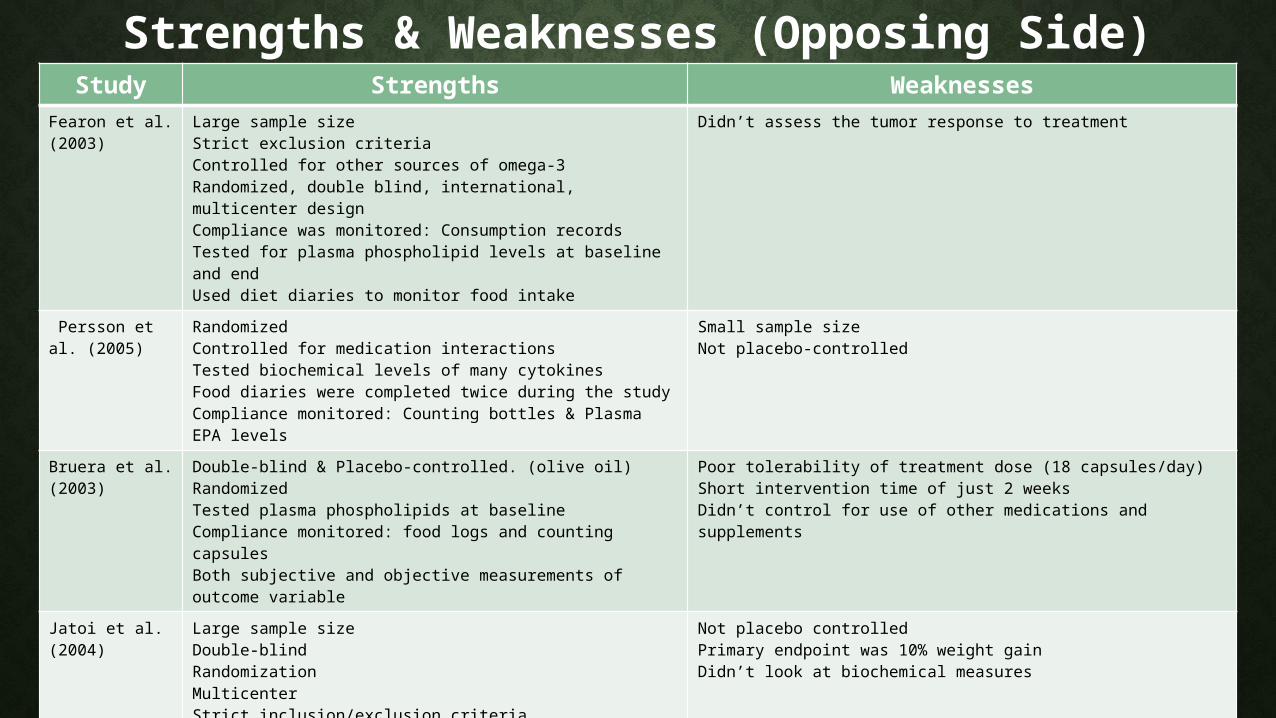
Strengths & Weaknesses (Opposing Side)Study Strengths Weaknesses
Fearon et al. (2003)
Large sample size Strict exclusion criteriaControlled for other sources of omega-3Randomized, double blind, international, multicenter designCompliance was monitored: Consumption records Tested for plasma phospholipid levels at baseline and endUsed diet diaries to monitor food intake
Didn’t assess the tumor response to treatment
Persson et al. (2005)
Randomized Controlled for medication interactionsTested biochemical levels of many cytokinesFood diaries were completed twice during the studyCompliance monitored: Counting bottles & Plasma EPA levels
Small sample sizeNot placebo-controlled
Bruera et al. (2003)
Double-blind & Placebo-controlled. (olive oil)RandomizedTested plasma phospholipids at baselineCompliance monitored: food logs and counting capsulesBoth subjective and objective measurements of outcome variable
Poor tolerability of treatment dose (18 capsules/day)Short intervention time of just 2 weeksDidn’t control for use of other medications and supplements
Jatoi et al. (2004)
Large sample size Double-blindRandomizationMulticenterStrict inclusion/exclusion criteriaControlled for medication interactions
Not placebo controlledPrimary endpoint was 10% weight gainDidn’t look at biochemical measures
Fearon et al. (2006)
Large sample sizeDouble-blind, placebo-controlled, multicenter designRandomizedTested different doses of EPA Controlled for medication interactionsAssessed both clinical and biochemical outcomes
Primary end point is nutritional statusTested two different types of cancer
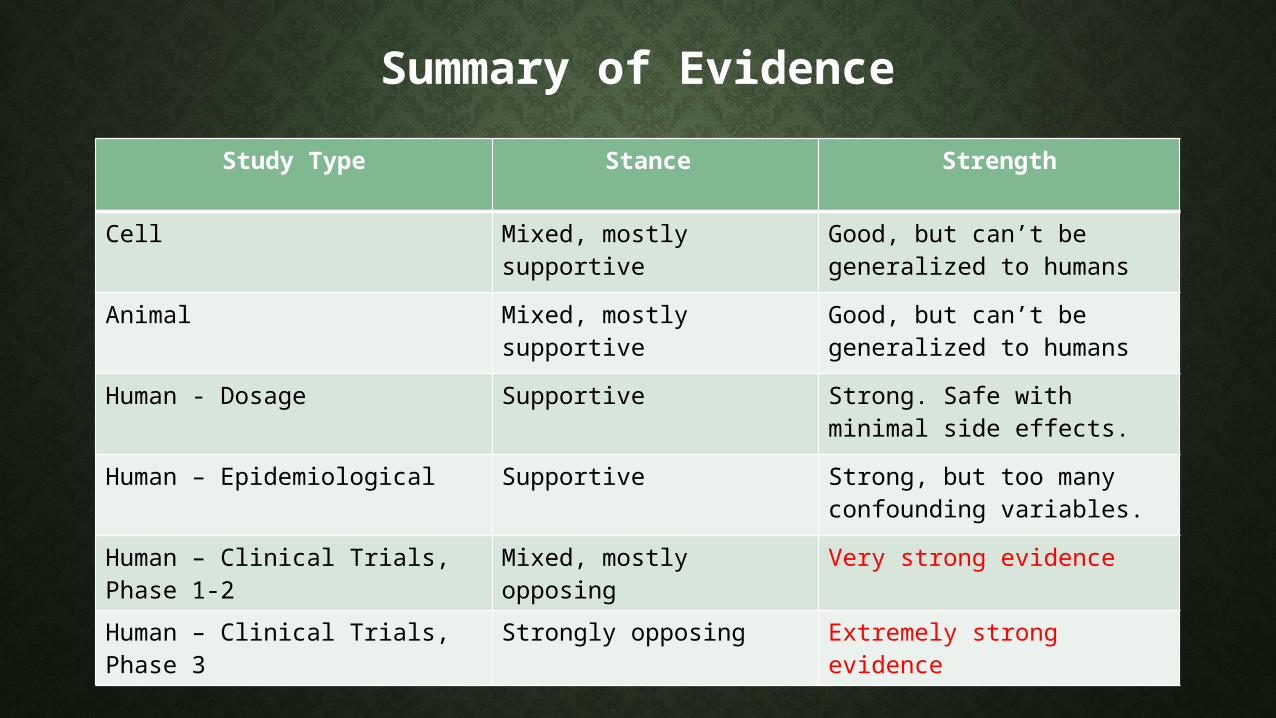
Summary of EvidenceStudy Type Stance Strength
Cell Mixed, mostly supportive Good, but can’t be generalized to humans
Animal Mixed, mostly supportive Good, but can’t be generalized to humans
Human - Dosage Supportive Strong. Safe with minimal side effects.
Human – Epidemiological Supportive Strong, but too many confounding variables.
Human – Clinical Trials, Phase 1-2
Mixed, mostly opposing Very strong evidence
Human – Clinical Trials, Phase 3
Strongly opposing Extremely strong evidence
My Stance on the Controversy After weighing the evidence on both sides of the argument I am in favor of the opposing side.
Omega-3s are safe and have limited side effects, however, they should be avoided in cachexia patients for the following reasons:1) The side effects will likely cause decreased appetite2) Result in missed feeding opportunities 3) Likely cause decreased immune response4) Add to the financial burden of the patient5) Have no benefit over the current standard of care6) Only show improvements if treatment started in early stages (precachexia)7) These improvements are minimal, and are outweighed by these potential negatives8) Both quantity and quality of supporting articles are lacking at this time9) Most studies in support were small and underpowered
Conclusion
At this time, there is not enough evidence to support the use of omega-3 polyunsaturated fatty acids as an adjuvant therapy for treating cancer-induced cachexia.
Future Research 1. How does the stage of cachexia progression affect the effectiveness of omega 3
supplementation?
2. Defining the optimal dose for cachexia patients
3. The effect of comorbidities, genotype, epigenetics, environment, and other dietary factors on the outcome of omega-3 PUFA intervention
4. A deeper understanding of the underlying mechanisms omega-3s use to exert their effects
5. Need more large-scale randomized clinical trials
6. Making methodology comparable between studies

Thank you! Questions?
References• Barber, M. D. (2001). Cancer Cachexia and Its Treatment With Fish-Oil-Enriched Nutritional Supplementation Nutrition, 17, 751-755.
• Barber, M. D., Fearon, K.C., Tisdale, M.J., McMillan, D.C., & Ross, J.A. (2001). Effect of a Fish-Oil Enriched Nutritional Supplement on Metabolic Mediators in Patients With Pancreatic Cancer Cachexia Nutrition and Cancer, 40(2), 118-124.
• Barber, M. D., Ross, J.A., Preston, T., Shenkin, A., & Fearon, K.C. (1999). Fish Oil-Enriched Nutritional Supplement Attenuates Progression of the Acute-Phase Response in Weight-Losing Patients with Advanced Pancreatic Cancer The Journal of Nutrition, 129, 1120-1125.
• Barber, M. D., Ross, J.A., Voss, A.C., Tisdale, M.J., & Fearon, K.C. (1999). The effect of an oral nutritional supplement enriched with fish oil on weight-loss in patients with pancreatic cancer British Journal of Cancer, 81(1), 80-86.
• Bégin, M. E., Ells, G., Das, U. N., & Horrobin, D. F. (1986). Differential killing of human carcinoma cells supplemented with n-3 and n-6 polyunsaturated fatty acids. Journal of the National Cancer Institute, 77(5), 1053-1062.
• Bruera, E., Strasser, F., Palmer, J.L., Willey, J., Calder, K., Amyotte, G., & Baracos, V. (2003). Effect of Fish Oil on Appetite and Other Symptoms in Patients With Advanced Cancer and Anorexia/Cachexia: A Double-Blind, Placebo-Controlled Study Journal of Clinical Oncology, 21(1), 129-134.
• Burns, C. P., Halabi, S., Clamon, G.H., Hars, V., Wagner, B.A. Hohl, R.J., ... Paskett, E. . (1999). Phase I Clinical Study of Fish Oil Fatty Acid Capsules for Patients with Cancer Cachexia: Cancer and Leukemia Group B Study 9473. Clinical Cancer Research, 5, 3942-3947.
• Calder, P. C., & Newsholme, E.A. (1992). Polyunsaturated fatty acids suppress human peripheral blood lymphocyte proliferation and interleukin-2 production Clinical Science, 82, 695-700.
• Chang, W. L., Chapkin, R.S., & Lupton, J.R. (1998). Fish Oil Blocks Azoxymethane-Induced Rat Colon Tumorigenesis by Increasing Cell Differentiation and Apoptosis Rather Than Decreasing Cell Proliferation The Journal of Nutrition, 128, 491-497.
• Cockbain, A. J., Toogood, G.J., & Hull, M.A. (2011). Omega-3 polyunsaturated fatty acids for the treatment and prevention of colorectal cancer. Gut, 1-15.
• Colomer, R., Moreno-Nogueira, J.M., Garcia-Luna, P.P., Garcia-Peris, P., Garcia-de-Lorenzo, A., Zarazaga, A., ... Casimiro, C. . (2007). n-3 Fatty acids, cancer and cachexia: a systematic review of the literature. British Journal of Nutrition, 97, 823-831.
References Cont.• Costelli, P., Llovera, M., Lopez-Soriana, J., Carbo, N., Tessitore, L., Lopez-Soriano, F.J., ... Argiles, J.M. (1995). Lack of effect of
eicosapentaenoic acid in preventing cancer cachexai and inhibiting tumor growth Cancer Letters, 97, 25-32.
• Dewey, A., Baughan, C., Dean, T.P., Higgins, B, & Johnson, I. (2012). Eicosapentaenoic acid (EPA, an omega-3 fatty acid from fish oils) for the treatment of cancer cachexia Cochrane Database of Systematic Reviews(1).
• Endres, S., Meydani, S.N., Ghorbani, R., Schnigler, R., & Dinarello, C.A. (1993). Dietary Supplementation with n-3 fatty acids suppresses interleukin-2 production and mononuclear cell proliferation Journal of Leukocyte Biology, 54(6), 599-603.
• Fearon, K., Strasser, F., Anker, S.D., Bosaeus, I., Bruera, E., Fainsinger, R.L., ... Baracos, V.E. (2011). Definition and classification of cancer cachexia: an international consensus Lancet, 12, 489-495.
• Fearon, K. C., Barber, M.D., Moses, A.G., Ahmedzai, S.H., Taylor, G.S., Tisdale, M.J., & Murray, G.D. (2006). Double-Blind, Placebo-Controlled, Randomized Study of Eicosapentaenoic Acid Diester in Patients With Cancer Cachexia Journal of Clinical Oncology, 24(21), 3401-3407.
• Fearon, K. C., Glass, D.J., Guttridge, D.C. (2012). Cancer Cachexia: Mediators, Signaling, and Metabolic Pathways Cell Metabolism, 16, 153-166.
• Fearon, K. C., von Meyenfeldt, M.F., Moses, A.G., van Geenen, R., Roy, A., Gouma, D.J., ... Tisdale, M.J. (2003). Effect of a protein and energy dense n-3 fatty acid enriched oral supplement on loss of weight and lean tissue in cancer cachexia: a randomised double blind trial. Gut, 52, 1479-1486.
• Fetterman Jr., J. W., & Zdanowicz, M.M. (2009). Therapeutic potential of n-3 polyunsaturated fatty acids in disease. American Journal of Health-System Pharmacy, 66, 1169-1179.
• Finocchiaro, C., Segre, O., Fadda, M., Monge, T., Scigliano, M., Schena, M., & Tinivella, M. (2012). "Effect of n-3 fatty acids on patients with advanced lung cancer: a double blind, placebo-controlled study " British Journal of Nutrition 108: 327-333.
• Fox, K. M., Brooks, J. M., Gandra, S. R., Markus, R., & Chiou, C. F. (2009). Estimation of cachexia among cancer patients based on four definitions. Journal of oncology, 2009.
• Furst, P., & Kuhn, K.S. (2000). Fish oil emulsions: what benefits can they bring? . Clinical Nutrition, 19(1), 7-14.
References Cont.• Giacosa, A., & Rondanelli, M. . (2008). Fish oil and treatment of cancer cachexia Genes and Nutrition, 3, 25-28.
• Gogos, C. A., Ginopoulos, P., Salsa, B., Apostolidou, E., Zoumbos, N.C., & Kalfarentzos, F. (1998). Dietary Omega-3 Polyunsaturated Fatty Acids plus Vitamin E Restore Immunodeficiency and Prolong Survival for Severely Ill Patients with Generalized Malignancy Cancer, 82, 395-402.
• Griffini, P., Fehres, O., Klieverik, L., Vogels, I.M., Tigchelaar, W., Smorenburg, S.M., & Van Noorden, C.J. (1998). Dietary n-3 Polyunsaturated Fatty Acids Promote Colon Carcinoma Metastasis in Rat Liver. Cancer Research, 58, 3312-3319.
• Hardman, W. E. (2002). Omega-3 Fatty Acids to Augment Cancer Therapy The Journal of Nutrition, 132, 3508-3512.
• Hardman, W. E., & Avula, C.P. (2001). Three Percent DIetary Fish Oil Concentrate Increased Efficacy of Doxorubicin Against MDA-MB 231 Breast Cancer Xenografts Clinical Cancer Research, 7, 2041-2049.
• Jatoi, A. (2005). Fish oil, lean tissue, and cancer: is there a role for eicosapentaenoic acid in treating the cancer anorexia/weight loss syndrome? . Critical Reviews in Oncology/Hematology, 55, 37-43.
• Jatoi, A. (2005). n-3 Fatty Acid Supplements for Cancer-Associated Weight Loss. Nutrition in Clinical Practice, 20, 394-399.
• Jatoi, A. R., K., Loprinzi, C.L., Sloan, J.A., Dakhil, S.R., Macdonald, N., ... Christensen, B. (2004). An Eicosapentaenoic Acid Supplement Versus Megestrol Acetate Versus Both for Patients With Cancer-Associated Wasting: A North Central Cancer Treatment Group and National Cancer Institute of Canada Collaborative Effort Journal of Clinical Oncology, 22(12), 2469-2476.
• Llor, X., Pons, E., Roca, A., Alvarez, M., Mane, J., Fernandez-Banares, F., & Gassull, M.A. (2003). The effects of fish oil, olive oil, oleic acid, and linoleic acid on colorectal neoplastic processes. Clinical Nutrition, 22(1), 71-79.
• Murphy, R. A., Mourtzakis, M., Chu, Q.S., Baracos, V.E., Reiman, T., & Mazurak, V.C. (2011). Nutritional Intervention With Fish Oil Provides a Benefit Over Standard of Care for Weight and Skeletal Muscle Mass in Patients With Nonsmall Cell Lung Cancer Receiving Chemotherapy Cancer, 117, 1775-1782.
• Murphy, R. A., Yeung, E., Mazurak, V.C., & Mourtzakis, M. . (2011). Influence of eicosapentaenoic acid supplementation on lean body mass in cancer cachexia British Journal of Cancer, 105, 1469-1473.
References Cont.• Persson, C., Glimelius, B., Ronnelid, J., & Nygren, P. . (2005). Impact of fish oil and melatonin on cachexia in patients with advanced
gastrointestinal cancer: A randomized pilot study. Nutrition, 21, 170-178.
• Roodhart, J. M., Daenen, L.G., Stigter, E.C., Prins, H., Gerrits, J., Houthuijzen, J.M., ... Voest, E.E. (2011). Mesenchymal Stem Cells Induce Resistance to Chemotherapy through the Release of Platinum-Induced Fatty Acids. Cancer Cell, 20, 370-383.
• Roynette, C. E., Calder, P.C., Dupertuis, Y.M., & Pichard, C. (2004). n-3 Polyunsaturated fatty acids and colon cancer prevention Clinical Nutrition, 23, 139-151.
• Sanchez-Lara, K., Turcott, J.G., Juarez-Hernandez, E., Nunez-Valencia, C., Villanueva, G., Guevara, P., & Torre-Vallejo, M. (2014). "Effects of an oral nutritional supplement containing eicosapentaenoic acid on nutritional and clinical outcomes in patients with advanced non-small cell lung cancer: Randomised trial " Clinical Nutrition 33: 1017-1023.
• Stewart, G. D., Skipworth, R.J., & Fearon, K.C. (2006). Cancer cachexia and fatigue Clinical Medicine, 6(2), 140-143.
• Tisdale, M. J. (2009). Mechanisms of Cancer Cachexia. Physiological Reviews, 89, 381-410.
• Tisdale, M. J., & Dhesi, J.K. (1990). Inhibition of Weight Loss by n-3 Fatty Acids in an Experimental Cachexia Model. Cancer Research, 50, 5022-5026.
• Utech, A. E., Tadros, E. M., Hayes, T. G., & Garcia, J. M. (2012). Predicting survival in cancer patients: the role of cachexia and hormonal, nutritional and inflammatory markers. Journal of cachexia, sarcopenia and muscle, 3(4), 245-251.
• Wigmore, S. J., Ross, J.A., Falconer, S., Plester, C.E., Tisdale, M.J., Carter, D.C., & Fearon, K.C. (1996). The Effect of Polyunsaturated Fatty Acids on the Progress of Cachexia in Patients with Pancreatic Cancer Nutrition, 12(1), 27-30.
• Wu, D., & Meydani, S.N. . (1998). n-3 Polyunsaturated fatty acids and immune function Proceedings of the Nutrition Society, 57, 503-509.
• Yeh, K., Wang, H., Chang, J. W., Huang, J., Lai, C., Lan, Y., & Wu, T. (2013). "Omega-3 fatty acid-, micronutrient-, and probiotic-enriched nutrition helps body weight stabilization in head and neck cancer cachexia." Oral Surgery Oral Medicine Oral Pathology Oral Radiology 116(1): 41-48.
• Zuijdgeest-Van Leeuwen, S. D., Dagnelie, P.C., Wattimena, J.L., Van Den Berg, J.W., Van Der Gaast, A., Swart, G.R., & Paul Wilson, J.H. (2000). Eicosapentaenoic acid ethyl ester supplementation in cachectic cancer patients and healthy subjects: effects on lipolysis and lipid oxidation. Clinical Nutrition, 19(6), 417-423.





























