Embed Size (px)
Citation preview

The Metabolic Effects of Intensive Insulin Therapy in Critically Ill
Patients
MB Whyte1, NC Jackson2, F Shojaee-Moradie2, DF Treacher3, RJ Beale3, RH
Jones1, AM Umpleby2
1Dept of Diabetes, Endocrinology and Internal Medicine, GKT School of Medicine, St.Thomas’
Hospital, 2Dept of Diabetes and Endocrinology, Postgraduate Medical School, University of
Surrey, 3Dept Intensive Care Medicine, St.Thomas’ Hospital, London, UK.
Running title: Metabolic Effects of Intensive Insulin Therapy
Address for correspondence
Dr. Martin Whyte
Department of Diabetes and Endocrinology
Kings College Hospital
London
SE5 9RS
Telephone: 020 32991737
Fax: 020 32991730
E mail: [email protected]
Abstract word count 250
Manuscript Word count: 4363 (excluding abstract, tables and figure legends)
Abstract
Aims To investigate the effects of glycaemic control and insulin concentration on lipolysis,
glucose, and protein metabolism in critically-ill medical patients.
Methods. Patients were studied twice. In Study 1, blood glucose (BG) concentrations were
maintained between 7-9mmol/L with intravenous insulin. After Study 1 patients entered 1 of 4
protocols for 48h until Study 2: Low-insulin high-glucose, LIHG (variable insulin, BG 7–
9mmol/L), Low-insulin low-glucose, LILG (variable insulin, BG 4–6mmol/L), High-insulin high-
glucose, HIHG (insulin [2.0 mU kg-1min-1plus insulin requirement from study one], BG 7–
9mmol/L), High-insulin low-glucose, HILG (insulin [2.0 mU kg-1min-1plus insulin requirement
from study one], BG 4-6mmol/L). Age-matched healthy control subjects received two-step
euglycaemic hyperinsulinaemic clamps achieving insulin levels similar to the LI and HI groups.
Results Whole-body proteolysis was higher in patients in study 1 (P<0.006) compared to control
subjects at comparable insulin concentrations and was reduced with LI (P<0.01) and HI (P=0.001)
in control subjects, but not in patients. Endogenous glucose production rate (Ra), glucose
disposal and lipolysis were not different in all patients in study 1 compared to control subjects at
comparable insulin concentrations. Glucose Ra and lipolysis did not change in any of the study 2
patient groups. HI increased glucose disposal in the patients (HIHG, P=0.001; HILG, P=0.07
versus study 1) but this was less than in controls receiving HI (P<0.03).
Conclusions Low-dose intravenous insulin, administered to maintain BG between 7-9 mmol/L is
sufficient to limit lipolysis and endogenous glucose Ra and increase glucose Rd. Neither
hyperinsulinaemia nor normoglycaemia had any protein-sparing effect.
Keywords Insulin, glucose, glycaemic control, critical illness, lipolysis, endogenous glucose
production rate, glucose disposal, proteolysis

Abbreviations
APACHE Acute Physiology and Chronic Health Evaluation
APE atom percent excess
BG blood glucose
CRP C reactive protein
HIHG High-insulin high-glucose
HILG High-insulin low-glucose
KIC α ketoisocaproate
LIHG Low-insulin high-glucose
LILG Low-insulin low-glucose
NOLD Non-oxidative leucine disappearance
Ra Rate of appearance
Rd Rate of disappearance
TPN total parenteral nutrition

Introduction
Critically-ill patients exhibit a stress response characterised by lipolysis, protein
breakdown and hyperglycaemia. Hyperglycaemia was considered to be a beneficial,
adaptive response but recent evidence suggests that it may be detrimental.
Maintenance of normoglycaemia with either a Glucose-Insulin-Potassium infusion
(32) or variable insulin infusion (16; 55; 56) has been reported to improve patient
morbidity and mortality. Post-hoc analysis suggested that the prevailing glycaemia,
rather than insulin dose administered, effects the beneficial outcomes (57). More
recently, debate has intensified following the publication of a multi-center study that
casts doubt over the benefits of glycaemic control in a critical care environment (15).
The metabolic effects of such treatment have yet to be characterised.
Endogenous glucose production rate (Ra) has been shown to be increased by at least
twofold in critical illness, compared to healthy controls (45), however it is not known
how effective a variable insulin infusion is at lowering glucose Ra. Insulin
administration at a rate of 1mg/kg/min was required to overcome hepatic insulin
resistance in septic patients (10) but there was evidence of incomplete suppression (as
reflected by high serum IGFBP-1 levels) in surgical patients (36). Accelerated
lipolysis is also a consistent feature of critical illness and elevated fatty acids can
contribute to insulin resistance. In health, lipolysis is inhibited by low insulin levels
but in critical illness, higher doses may be required (10). The effect of maintenance
of normoglycemia with intensive insulin therapy on lipolysis is also unknown.
Critically-ill patients may experience loss of muscle protein approaching 2% per day
(19). Patient survival (20), duration of intensive care unit (ICU) admission (12), and
time to recovery of normal physiological function (59), are inversely correlated with
loss of lean body mass. Insulin’s effect on protein metabolism has been contentious
1
but it appears primarily to inhibit proteolysis (9; 18; 38; 51) although increased
protein synthesis has also been reported (6). We hypothesised that the anti-catabolic
effects of insulin might explain the benefits of insulin administration to critically-ill
patients.
We have studied the effect of maintaining normoglycaemia with intravenous insulin
on the rate of lipolysis, glucose and protein metabolism in patients requiring tertiary-
level support.
Research Design and Methods
The study protocol was approved by the regional ethics committee. Twenty-five
mechanically-ventilated patients were recruited from the ICU at St.Thomas’ Hospital,
London. Assent was obtained from the patients’ families before their entry into the
study. Patients newly admitted to the ICU (within 36 h) and likely to require
ventilatory support for at least 3 days were considered for inclusion.
Patients were excluded if they had a surgical procedure prior to ICU admission
requiring general anaesthesia or regional block. Patients with diabetes mellitus, acute
or chronic pancreatitis, liver disease, and those receiving oral steroids within one-
month prior to entering the ICU were excluded. Liver disease was defined as any one
of: history of oesophageal varices, biopsy (or ultrasonographic) evidence of cirrhosis,
International normalised ratio (INR) > 1.4, bilirubin concentration more than twice
the normal range, ALT, AST, γGT, or ALP concentration over three times the normal
range. 13 patients were admitted with primary respiratory dysfunction, 3 with sepsis
from a non-respiratory cause, 2 with neurological illness, 2 with cardiac disease and 5
2

with other illnesses. Patients received a variety of vasopressor agents, steroids and
anaesthetic agents (Table 1). Severity of illness was determined by the Acute
Physiology and Chronic Health Evaluation (APACHE) II score.
All patients were studied on two occasions, 48 h apart. Patients receiving enteral
nutrition (Nutrison multifibre™, Nutricia, Zoetermeer, Holland), had the feed stopped
8 h prior to Study 1. All patients received intravenous 20% dextrose (25kcal kg-1day-
1) for at least 8 h before Study 1 (range 10-18 h). Study 1 took place within 36 h of
ICU admission with blood glucose (BG) concentrations maintained between 7-9
mmol/L with intravenous Actrapid insulin (Novo-Nordisk, Bagsvaerd, Denmark).
The insulin infusion was adjusted at hourly intervals to maintain BG between 7 and
9mmol/L for at least 10 h before study 1 (range 10-18 h; figure 1). After study 1
patients entered 1 of 4 protocols for 48h until Study 2: Low-insulin high-glucose,
LIHG (variable insulin infusion to maintain BG 7 – 9mmol/L), Low-insulin low-
glucose, LILG (variable insulin to maintain BG 4 – 6mmol/L), High-insulin high-
glucose, HIHG (insulin infusion rate 2.0mU kg-1min-1 plus insulin requirement from
Study 1), with additional dextrose, as required, to maintain BG 7 –9mmol/L), High-
insulin low-glucose, HILG (insulin infusion rate 2.0mU kg-1min-1 plus insulin
requirement from Study 1) with additional dextrose, as required, to maintain BG 4 -
6mmol/L (figure 1).
Study Protocol (Patients).
Study 1. After baseline sampling, a prime of 170mg of [6,6 2H2]glucose, 0.15mg / kg
of [2H5]glycerol, 1mg / kg of [1-13C]leucine and 0.2 mg / kg [13C]NaHCO3 (CK Gases
Ltd, UK, subsidiary of Cambridge Isotope Laboratories, Massachusetts) was
3

administered (33) followed by continuous infusion of (1.7mg/min) [6,6 2H2]glucose,
(0.61mg kg-1hr-1) [2H5]glycerol and (1mg kg-1hr-1) [1-13C]leucine, for 180 min. During
the 3 h tracer infusion, glucose infusion rate remained constant and if necessary,
intravenous insulin was adjusted every 30min to maintain BG concentrations.
Indwelling arterial and central venous lines were used for blood sampling and for
tracer infusion, respectively. BG was determined on heparinised samples using a
point-of-care Omni 2 blood gas analyser (AVL/Roche, Welwyn Garden City, UK).
Blood samples were taken at baseline and at 150, 160, 170, 175 and 180 min (steady
state) to measure the isotopic enrichment of glucose, glycerol and α-keto-isocaproate
(αKIC) and hormone and metabolite concentrations. Samples were stored at -70˚C
until analysis.
Expired air was collected from the exhaust-port of the ventilator, at the same intervals
as blood sampling to measure isotopic enrichment, and stored in 250ml aluminium-
coated bags (QuinTron® Instrument Company, Milwaukee, Wisconsin USA),
pending transfer into evacuated, septum-capped 10ml glass tubes (Exetainer, Labco
Ltd, High Wycombe), for the measurement of 13CO2 by isotope ratio mass
spectrometry (IRMS). Pulmonary gas exchanges were measured by an open-circuit
indirect calorimeter (Deltatrac™ II metabolic monitor, Datex-Ohmeda, Finland).
Data acquisition was performed until steady-state values were reached over a 30-60
min period, defined as requiring no change in ventilatory settings, no requirement for
large volumes of fluids, and institution or cessation of vasopressors. The values of
VO2 (oxygen consumption) and VCO2 (carbon dioxide production) and the calculated
respiratory quotient (RQ) represent an average of the data obtained over 30 min, with
a coefficient of variation of <10%.
4
After Study 1, enteral feeding (1 kcal/ml; 16% protein, 49% carbohydrate, 35% fat)
was instituted immediately, unless a clinical decision was made not to do so. The
feed was supplemented by intravenous 50% dextrose, as required, to achieve
glycaemic targets. Patients were fed via nasogastric tube according to a standard
feeding protocol. It was the policy of the local ICU to use total parenteral nutrition
(TPN) only if specifically indicated, as such, no patient received TPN. Eight hours
prior to the second isotope study the enteral feed was stopped and replaced with
isocaloric intravenous 20% or 50% dextrose (depending on fluid requirements.)
Study 2. The isotope infusion and sampling protocol of the second isotope study was
identical in methodology to Study 1.
Study Protocol (Control subjects). Five healthy age-matched control subjects (M4,
F1) were studied to quantify the normal dose response effect of insulin on suppression
of proteolysis, lipolysis and glucose production and increase in glucose disposal. All
volunteers were in good health and gave informed consent to the study. Subjects
were fasted from midnight and studied throughout in a semi-recumbent position.
Following baseline blood sampling, a 9 h, primed, constant infusion of [6,6
2H2]glucose, (1.7mg/min), [2H5]glycerol (0.61mg kg-1hr-1), [1-13C]leucine (1mg kg-
1hr-1) was commenced using an IVAC syringe pump (Alaris, San Diego). Insulin was
infused at 0.5mU kg-1min-1 between 180-360 min and 2.0mU kg-1min-1 from 360-540
min. Blood samples were taken at baseline, 150, 160, 170, 175 and 180 min (first
steady-state), 330, 340, 350, 355 and 360 min (second steady-state) and at 510, 520,
530, 535 and 540 min (third steady state) (Figure 2). BG was determined every 5 min
(Yellow Springs Instruments, Yellow Springs, OH) and maintained within 5% of
5

5mmol/L by adjustment of a 20% glucose infusion (IVAC Volumetric pump, Alaris
systems, San Diego) (13), spiked with [6,6-2H2]glucose (‘hot glucose infusion
method’, using 8mg/g glucose for step 1 and 10 mg/g glucose for step 2).
Experimental Methods. Plasma α-KIC enrichment was measured as a quinoxalinol-
tertiarybutyldimethylsilyl derivative as previously described (17). Using a reciprocal
pool model (35), plasma α-KIC enrichment was considered a measure of intracellular
leucine enrichment. 13C enrichment of breath CO2 was measured on a SIRA series II
continuous-flow IRMS (VG Isotech, Cheshire, UK) modified with a Roboprep G+
inlet system (Europa Scientific). The isotopic enrichment of plasma glucose was
determined by the penta-O-trimethylsilyl-D-glucose-o-methoxamine derivative (46)
and glycerol as the tris-trimethylsilyl derivative (60). Plasma and infusate glucose
concentrations were determined using a Clandon Scientific Glucose analyser (Yellow
Springs Instruments, Yellow Springs, OH). Blood lactate concentration was
measured by point-of-care AVL/Roche Omni2 blood gas analyser. Serum NEFA
concentrations were determined spectrophotometrically by Cobas analyser (Roche,
Welwyn Garden City, UK) using a kit from Wako Chemicals Inc (Alpha
Laboratories, Hampshire, UK). Plasma and infusate glycerol concentrations were
measured by direct colorimetry (Randox Laboratories, Crumlin, Co.Antrim, UK) on a
Cobas analyser. Total cholesterol concentration was measured using a kit from ABX
Diagnostics (Montpellier, France) on a Cobas analyser. Serum cortisol concentration
was measured by an automated chemiluminescent assay (Bayer Diagnostics,
Tarrytown, USA). Serum insulin concentrations were measured by an in-house
double-antibody radioimmunoassay (47). C-peptide concentration was measured
using a double-antibody radioimmunoassay (RIA) kit (LINCO Research Inc.
6

St.Charles, Missouri, USA). C-Reactive Protein (CRP) was measured with an
immunoturbidometric assay (Beckman Synchron LX20).
Calculations. The rates of appearance and disappearance of a substrate were
calculated from the dilution of labelled substrate in plasma using a mono-
compartment model and Steele’s equations (2) modified for stable isotopes. During
physiologic and isotopic steady-state, the production rate (Ra) of unlabelled substrate
can be calculated by:
Ra (µmol kg-1min-1) = (Ei / Ep -1) x I
Where Ei = enrichment of infusate (Atom % excess, APE), Ep = enrichment of
substrate in plasma (APE), and I = infusion rate (µmol kg-1min-1). Total glucose Ra
was assumed to equal peripheral glucose disposal (Rd). The endogenous glucose
production rate was estimated by subtraction of the unlabelled glucose infusion rate
from the total glucose Ra. Propofol (Diprivan®) contains glycerol at 22.5mg/ml and
soybean oil at 100mg/ml. We have assumed that 30% of the triglyceride composition
of soybean oil is hydrolysed to glycerol (25). Endogenous glycerol Ra was calculated
by subtracting the rate of glycerol appearance from propofol from the total glycerol
Ra. Leucine oxidation rate was calculated from the CO2 Ra and expired 13CO2 as
previously described (34).
Ox (µmol kg-1min-1) = (ECO2 x VCO2) / EKIC x 0.899
ECO2 is the atoms percent excess of 13CO2 in expired air, EKIC is the [13C]KIC
enrichment, and 0.899 is a recovery factor that accounts for the fraction of 13CO2
formed on oxidation of the tracer but not released from the bicarbonate pool (53).
Non-oxidative leucine disappearance rate (NOLD, a measure of protein synthesis)
7
was calculated by subtracting leucine oxidation rate (Rox) from leucine Ra. Net
protein balance was estimated using the equation (NOLD – Ra), with the assumption
of 8g of leucine for 100g whole body protein (22).
Commercially available dextrose for intravenous infusion contains carbon with a high
natural abundance of 13C isotope: this could affect calculation of leucine oxidation
when first administered. As the patient group received at least 8 h of intravenous
dextrose prior to the 13C-leucine infusion, the rate of 13C release by oxidation of
exogenous carbohydrate would have equilibrated before 13C leucine was infused.
Basal samples were collected prior to the isotope infusion thus allowing correction for
this in the subsequent measurement of leucine oxidation. However, in the control
group dextrose was infused after infusion of the isotopes so the contribution of 13C
isotope to 13CO2 could not be corrected for and leucine oxidation could not be
measured.
Statistical analysis. The primary endpoint was leucine Ra. With 6 patients in each
group the study was powered to detect a difference of 20% in leucine Ra between
Study 1 and Study 2 in the patients with a power of 80% at a two-sided 5 % level of
significance. This was based on previous studies of protein metabolism in ICU in both
surgical patients (26) and septic medical patients (5) whereby the SD for leucine Ra
was between 6 and 16%. Studies have reported an SD for leucine Ra in healthy
subjects to be 8.5% (18). With n=5 in the control subjects the study was powered to
detect a difference of 9.5% in leucine Ra between insulin doses with a power of 80%
at a two-sided 5 % level of significance. The Statistical Package for the Social
Sciences (version 12.0 for Windows software; SPSS Inc, Chertsey UK) was used for
statistical analyses. Between-group comparisons were analysed for statistical
8

significance using repeated-measures ANOVA. Post-hoc analysis was conducted
using Bonferroni’s multiple-comparison test. For within-group comparisons of study
1 to study 2, a paired t test was used. Results are expressed as mean values SEM
unless stated otherwise.
9
Results
Group Characteristics (table1)
The 4 groups differed significantly only as intended with respect to glucose
concentration and insulin infusion rates. The age (60.0 ± 1.3 years) and BMI (25.0 ±
0.9kg/m2) of control subjects were not different to the patients. All subjects survived
the duration of the study although one patient in the HIHG group subsequently died.
Treatment protocols were well tolerated with no short-term adverse effects seen on
gas exchange, renal, hepatic or cardiovascular status. Two glucose measurements
were <3mmol/L during the study but none were <2.2mmol/L. The control subjects’
plasma glucose was 5.03 ± 0.14mmol/L at baseline; 4.34 ± 0.16mmol/L with LD
insulin; and 4.24 ± 0.19 with HD insulin (NS).
Hormone and Plasma Metabolite Concentrations
Serum insulin, plasma C-peptide and serum cortisol concentrations are shown in
Table 2. In the LI study 2 patient groups; insulin concentrations were not different
from the LI control study. In the HI study 2 patient groups, insulin concentrations
were not different from the HI control study. Plasma lactate, serum NEFA, plasma
glycerol and total cholesterol levels are shown in Table 3. Plasma NEFA, glycerol
and total cholesterol concentrations were not different in study 2 compared to study 1
in any of the patient groups. Plasma total cholesterol was significantly lower in all
patient groups (at both study 1 and study 2 compared with fasting control subjects;
P<0.01). Plasma NEFA concentrations were lower in study 1 in all patients (n=25)
when compared to fasting control subjects (NEFA: 0.22 ± 0.04 vs. 0.67 ±
0.11mmol/L, P=0.02) but were higher than in the control study LI step where insulin
levels were comparable (NEFA: 0.04 ± 0.005mmol/L; P<0.001).
10
Kinetic Data
In the control subjects leucine Ra, a measure of proteolysis (figure 3), was reduced
from basal levels by 11.6 ± 1.3% with LI (from 1.78 ± 0.05 to 1.57 ± 0.03µmol kg -
1min-1; P=0.01) and by 21.7 ± 0.9% (to 1.39 ± 0.04µmol kg-1min-1) with HI (P<0.001).
In all patients in Study 1 (n=25), leucine Ra was not different from the fasting control
subjects but was higher than control subjects with comparable insulin concentrations
(LI) (2.00 ± 0.13 vs.1.57 ± 0.03µmol kg-1min-1; P=0.006). Leucine Ra was higher in
the HILG group in Study 2 than control subjects receiving HI (2.1 ± 0.15 vs. 1.39 ±
0.40µmol kg-1min-1; P=0.005). Comparing Study 2 to Study 1, none of the four
treatment regimens altered the rates of leucine Ra, NOLD and leucine oxidation
(figure 3 and table 4) with the result that net protein balance was unaffected (figure 4).
Furthermore, leucine Ra of the combined LI groups (n=13) did not change from study
1 to study 2 (2.07 ± 0.19 vs. 2.13 ± 0.15µmol kg-1min-1); likewise, leucine Ra of the
combined HI groups (n=12) was unchanged from study 1 to study 2 (1.94 ± 0.21 vs.
2.28 ± 0.19µmol kg-1min-1).
In the control subjects, glucose Ra was reduced from basal values with LI (P=0.07)
and was completely suppressed with HI (P=0.003; NS different from zero) (table 5).
Glucose Rd was increased with LI and HI compared to basal (P < 0.001). In all
patients at Study 1 (n=25) endogenous glucose Ra was lower and glucose Rd was
higher than the control subjects during fasting (P<0.001) but were not different from
the LI step in the controls which had comparable insulin levels. In Study 2,
endogenous glucose Ra was lower than Study 1 in the HILG group but was no
different in the other patient groups. Glucose Rd increased in Study 2 in both HI
11

groups (P=0.001 for HIHG; P=0.07 for HILG) compared to Study 1 but this was
lower than glucose Rd in the control study HI step which had comparable insulin
levels, (HILG group study 2, P<0.01; HIHG group study 2, P<0.03).
Glycerol Ra was reduced from basal by LI in the control subjects (P <0.001), with no
further suppression with HI (Table 4). In all patients in Study 1, glycerol Ra was not
different from control subjects receiving LI, and did not suppress further in any group
in Study 2. The glycerol Ra data were not significantly influenced by whether the
patients did or did not receive propofol.
12

Discussion
In this study we sought to determine the effects of glycaemic control and insulin
concentration on intermediary metabolism in critically-ill medical patients, and for the
first time, to measure the effect of insulin on protein turnover in critically ill medical
patients. The results demonstrate that low dose intravenous insulin, administered to
maintain BG between 7-9 mmol/L is sufficient to limit lipolysis and endogenous
glucose Ra and increase glucose Rd as compared to fasting control subjects.
Complete suppression of endogenous glucose Ra was only achieved in the HILG
group. Neither normoglycaemia nor hyperinsulinaemia had any effect on whole body
protein synthesis or proteolysis.
Protein loss characterises the catabolic response to critical illness: this is thought to
arise both from increased proteolysis (24) and diminished protein synthesis (58). The
use of leucine Ra in this study as a measure of proteolysis allows for a more accurate
estimation of protein flux than urinary nitrogen balance (31). Our data show that rates
of proteolysis in patients at study 1 were higher than in control subjects who received
similar insulin doses, even though endogenous glucose production rate was
suppressed which would reduce the requirement for gluconeogenic precursors. This
finding is consistent with previous observations in both normal subjects and surgical
patients that low-dose glucose administration (causing a doubling of insulin
concentration) does not reduce proteolysis (23) (42). Our data also show that the
administration of insulin to achieve supra-physiological concentrations did not
attenuate protein breakdown and had no effect on net protein balance. This finding
was not anticipated. In healthy subjects, insulin inhibits proteolysis in a dose-
dependent manner (51), as we confirmed from our control studies. Although this was
13

a small study, the findings suggest that neither tight glycaemic control or high doses
of insulin are likely to have any clinically significant benefit in terms of protein
balance in critical illness.
Stress-induced hyperglycaemia of critical illness has been attributed to insulin
resistance either at the liver (27) or skeletal muscle (1). Whilst it has been reported
that intensive insulin treatment to maintain tight glycaemic control between 4.4-
6.1mmol/l is unable to overcome hepatic insulin resistance, as assessed by high levels
of serum IGFBP-1 in critically-ill patients (36), our data show that suppression of
hepatic glucose Ra to low levels can occur with an insulin infusion of approximately
1mU kg-1min-1. This is in accord with recent studies in critically-ill patients which
also used kinetic techniques (10; 52) and showed that glycaemic control with an
insulin infusion is achieved by suppression of hepatic glucose production. In study 2,
patients in the HILG group had a level of glycaemia and insulinaemia which was
similar to control subjects receiving HI enabling a direct comparison of rates of
glucose disposal. Glucose Rd was lower than in the control subjects, suggesting the
presence of peripheral insulin resistance - a feature that has previously been reported
both in sepsis and trauma (40; 43) .
As expected, serum cortisol was higher in the patient groups than controls. It is not
yet known how important this is for the induction of peripheral insulin resistance
associated with critical-illness, as over 30 other factors have been proposed (4).
These may be grouped as either hormonal responses (for example glucocorticoid
hypersecretion or low circulating IGF-1) (54) or cytokine-mediated (including TNFα,
14

IL-6) (4). It is noteworthy that attempts to manipulate the cytokine cascade have not
affected the physiologic response to illness (11).
Lipolysis is a consistent feature of critical-illness (30) making the effect on lipolysis
of exogenous insulin an area of interest. In this study, the contribution of exogenous
glycerol was subtracted from the total glycerol Ra to give the endogenous glycerol
Ra. Although the contribution of exogenous glycerol was small (providing less than
5% of the total glycerol Ra) because the rate of release of glycerol from the hydrolysis
of soybean oil within propofol could not be measured directly, the endogenous
glycerol Ra is a very close approximation and not an exact measurement. In study 1
lipolysis (as measured by glycerol Ra and NEFA concentrations) was suppressed by
insulin and no further suppression occurred with HD insulin or tight glycaemic
control. Cardiac NEFA metabolism requires more oxygen per unit energy yield than
glucose, which could therefore have a deleterious effect on myocardial performance
in the hypoxic setting (3). Suppression of NEFA concentrations in the presence of
increased insulin will result in glucose being the prime substrate for myocardial
metabolism which may be beneficial. It is of interest that suppression of NEFA
concentration occurred without the necessity of achieving normoglycaemia.
Hypocholesterolaemia confers a poor prognosis in critically-ill patients (21). We
found that none of the treatment regimens normalised cholesterol, although a study
period of up to 1 week might have been required to do so (37).
A possible limitation to this study is the difference in study duration of the control and
patient groups. Bed-rest itself may cause insulin resistance after 5 to 6 days (48)
although not after 24 hours (39): this might have biased the data of the control group
15
(recumbent for 9-hours). However, it has also been shown that the insulin
responsiveness of protein metabolism after bed-rest remains intact (44) suggesting
that the conclusions drawn from the control studies were valid. The 48 hour duration
of clamp (plus an 8 hour lead-in to study 1) of the patient groups was based on the
expected length of stay of such patients in our ICU being 3 days, which is similar to
reported data (56). Effects of insulin on glucose and glycerol turnover in critically ill
patients have been reported within 500 minutes (10; 52) but we considered that an
effect on leucine turnover would take up to 72 hours (7).
We did not perform studies in the fed state as it would have required using total
parenteral nutrition which is a means of feeding seldom used in our ICU due to
infectious complications (29). It is possible that amino acid supplementation
combined with insulin might have increased whole-body protein synthesis as reported
in healthy subjects (8; 50). This was likely to have been a direct effect of the amino
acids as in the only study examining the action of insulin on protein turnover during
an amino acid clamp (41), it was found that insulin could suppress leucine Ra by 19%
but it had no effect on NOLD. However, systemic insulin infusion, despite
hypoaminoacidaemia, is capable of suppression of leucine Ra (14): as was also seen
in our control studies.
Inherent to the study design was that standard treatments be provided to obtain a
clearer understanding of the effect of glycaemic control in a setting familiar to
physicians and intensivists, this meant that the use of glucocorticoids could not be
controlled between the patient groups. However, we were unable to detect any
difference in leucine Ra at either study 1 or study 2 when patients were categorised as
16
receiving glucocorticoids or not and neither was any correlation seen between cortisol
concentration and leucine Ra. This study was of medical ICU admissions only and
therefore it remains to be seen whether tight glycaemic control can exert a protein-
sparing effect in surgical ICU cases.
To summarise, the use of a variable dose of insulin to maintain blood glucose below
6mmol/L in a medical group of critically-ill patients led to suppression of lipolysis
and near full reduction of hepatic glucose production and increased peripheral glucose
uptake. These effects were also seen with a higher level of glycaemia (7-9mmol/l),
suggesting intravenous insulin which achieves moderate glucose levels rather than
tight glycaemic control is sufficient to reduce fatty acid levels and overproduction of
glucose by the liver. Hyperinsulinaemia increased peripheral glucose disposal but this
failed to reach values seen in health; additionally, hyperinsulinaemia could not
attenuate protein loss. There appears to be a differential effect of resistance to insulin
action in skeletal muscle compared to adipose tissue or the liver. The intracellular
insulin signalling network is highly complex and includes cross-talk between
pathways but the Ras/MAPK pathway has been implicated as being responsible for
the growth and mitogenic effects of insulin (49). It may be that this pathway is
particularly susceptible to interruption during critical illness, perhaps by cytokine
action. Alternatively, it has been shown from studies of knockout mice that IRS-1 has
the predominant role in skeletal muscle and IRS-2 in the liver (28). Furthermore, data
suggests that IRS-1 knockouts affect protein synthesis whereas IRS-2 knockouts
primarily affect glucose regulation (49). It may be hypothesized that insulin receptor
subtypes are differentially affected in critical illness. To conclude, this study suggests
17

that any beneficial effect of tight glycaemic control on morbidity and mortality is not
due to protein sparing.
Acknowledgements
This study was supported by a grant from the Guy’s and St.Thomas’ Charitable
Foundation. The authors wish to thank William Jefferson, Premila Croos and Joanne
Crunden for their technical assistance with this study. We also acknowledge the help
of John Smith, Tony Sherry and the all the clinical staff at the Intensive Care Unit.
18

Reference List
1. Agwunobi AO, Reid C, Maycock P, Little RA and Carlson
GL. Insulin resistance and substrate utilization in human
endotoxemia. J Clin Endocrinol Metab 85: 3770-3778, 2000.
2. ALTSZULER N, DE BODO RC, STEELE R and WALL JS.
Measurement of size and turnover rate of body glucose pool by
the isotope dilution method. Am J Physiol 187: 15-24, 1956.
3. Apstein CS and Taegtmeyer H. Glucose-insulin-potassium in
acute myocardial infarction: the time has come for a large,
prospective trial. Circulation 96: 1074-1077, 1997.
4. Baracos VE. A panoply of anabolic and catabolic mediators.
Curr Opin Clin Nutr Metab Care 3: 169-170, 2000.
5. Beylot M, Chassard D, Chambrier C, Guiraud M, Odeon
M, Beaufrere B and Bouletreau P. Metabolic effects of a D-
beta-hydroxybutyrate infusion in septic patients: inhibition of
lipolysis and glucose production but not leucine oxidation. Crit
Care Med 22: 1091-1098, 1994.
19

6. Biolo G, Declan Fleming RY and Wolfe RR. Physiologic
hyperinsulinemia stimulates protein synthesis and enhances
transport of selected amino acids in human skeletal muscle. J
Clin Invest 95: 811-819, 1995.
7. Carroll PV, Jackson NC, Russell-Jones DL, Treacher DF,
Sonksen PH and Umpleby AM. Combined growth
hormone/insulin-like growth factor I in addition to glutamine-
supplemented TPN results in net protein anabolism in critical
illness. Am J Physiol Endocrinol Metab 286: E151-E157, 2004.
8. Castellino P, Luzi L, Simonson DC, Haymond M and
DeFronzo RA. Effect of insulin and plasma amino acid
concentrations on leucine metabolism in man. Role of substrate
availability on estimates of whole body protein synthesis. J Clin
Invest 80: 1784-1793, 1987.
9. Castellino P, Luzi L, Simonson DC, Haymond M and
Defronzo RA. Effect of insulin and plasma amino acid
concentrations on leucine metabolism in man. Role of substrate
availability on estimates of whole body protein synthesis. J Clin
Invest 80: 1784-1793, 1987.
10. Chambrier C, Laville M, Rhzioual BK, Odeon M,
Bouletreau P and Beylot M. Insulin sensitivity of glucose and
20

fat metabolism in severe sepsis. Clin Sci (Lond) 99: 321-328,
2000.
11. Clark MA, Plank LD, Connolly AB, Streat SJ, Hill AA,
Gupta R, Monk DN, Shenkin A and Hill GL. Effect of a
chimeric antibody to tumor necrosis factor-alpha on cytokine
and physiologic responses in patients with severe sepsis--a
randomized, clinical trial. Crit Care Med 26: 1650-1659, 1998.
12. Cogo PE, Carnielli VP, Rosso F, Cesarone A, Giordano G,
Faggian D, Plebani M, Barreca A and Zacchello F. Protein
turnover, lipolysis, and endogenous hormonal secretion in
critically ill children. Crit Care Med 30: 65-70, 2002.
13. DeFronzo RA, Tobin JD and Andres R. Glucose clamp
technique: a method for quantifying insulin secretion and
resistance. Am J Physiol 237: E214-E223, 1979.
14. Denne SC, Liechty EA, Liu YM, Brechtel G and Baron AD.
Proteolysis in skeletal muscle and whole body in response to
euglycemic hyperinsulinemia in normal adults. Am J Physiol
261: E809-E814, 1991.
15. Finfer S, Chittock DR, Su SY, Blair D, Foster D, Dhingra
V, Bellomo R, Cook D, Dodek P, Henderson WR, Hebert
PC, Heritier S, Heyland DK, McArthur C, McDonald E,
21

Mitchell I, Myburgh JA, Norton R, Potter J, Robinson BG
and Ronco JJ. Intensive versus conventional glucose control in
critically ill patients. N Engl J Med 360: 1283-1297, 2009.
16. Finney SJ, Zekveld C, Elia A and Evans TW. Glucose control
and mortality in critically ill patients. JAMA 290: 2041-2047,
2003.
17. Ford GC, Cheng KN and Halliday D. Analysis of (1-
13C)leucine and (13C)KIC in plasma by capillary gas
chromatography/mass spectrometry in protein turnover studies.
Biomed Mass Spectrom 12: 432-436, 1985.
18. Fukagawa NK, Minaker KL, Rowe JW, Goodman MN,
Matthews DE, Bier DM and Young VR. Insulin-mediated
reduction of whole body protein breakdown. Dose-response
effects on leucine metabolism in postabsorptive men. J Clin
Invest 76: 2306-2311, 1985.
19. Gamrin L, Andersson K, Hultman E, Nilsson E, Essen P
and Wernerman J. Longitudinal changes of biochemical
parameters in muscle during critical illness. Metabolism 46:
756-762, 1997.
22

20. Giner M, Laviano A, Meguid MM and Gleason JR. In 1995 a
correlation between malnutrition and poor outcome in critically
ill patients still exists. Nutrition 12: 23-29, 1996.
21. Gordon BR, Parker TS, Levine DM, Saal SD, Wang JC,
Sloan BJ, Barie PS and Rubin AL. Relationship of
hypolipidemia to cytokine concentrations and outcomes in
critically ill surgical patients. Crit Care Med 29: 1563-1568,
2001.
22. Hankard RG, Darmaun D, Sager BK, D'Amore D, Parsons
WR and Haymond M. Response of glutamine metabolism to
exogenous glutamine in humans. Am J Physiol 269: E663-E670,
1995.
23. Harrison RA, Lewin MR, Halliday D and Clark CG. Leucine
kinetics in surgical patients. I: A study of the effect of surgical
'stress'. Br J Surg 76: 505-508, 1989.
24. Hasselgren PO, James JH, Benson DW, Hall-Angeras M,
Angeras U, Hiyama DT, Li S and Fischer JE. Total and
myofibrillar protein breakdown in different types of rat skeletal
muscle: effects of sepsis and regulation by insulin. Metabolism
38: 634-640, 1989.
23

25. Hultin M, Carneheim C, Rosenqvist K and Olivecrona T.
Intravenous lipid emulsions: removal mechanisms as compared
to chylomicrons. J Lipid Res 36: 2174-2184, 1995.
26. Jackson NC, Carroll PV, Russell-Jones DL, Sonksen PH,
Treacher DF and Umpleby AM. The metabolic consequences
of critical illness: acute effects on glutamine and protein
metabolism. Am J Physiol 276: E163-E170, 1999.
27. Jeevanandam M, Young DH and Schiller WR. Glucose
turnover, oxidation, and indices of recycling in severely
traumatized patients. J Trauma 30: 582-589, 1990.
28. Kido Y, Burks DJ, Withers D, Bruning JC, Kahn CR, White
MF and Accili D. Tissue-specific insulin resistance in mice with
mutations in the insulin receptor, IRS-1, and IRS-2. J Clin Invest
105: 199-205, 2000.
29. Klein S, Kinney J, Jeejeebhoy K, Alpers D, Hellerstein M,
Murray M and Twomey P. Nutrition support in clinical
practice: review of published data and recommendations for
future research directions. Summary of a conference sponsored
by the National Institutes of Health, American Society for
Parenteral and Enteral Nutrition, and American Society for
Clinical Nutrition. Am J Clin Nutr 66: 683-706, 1997.
24

30. Klein S, Peters EJ, Shangraw RE and Wolfe RR. Lipolytic
response to metabolic stress in critically ill patients. Crit Care
Med 19: 776-779, 1991.
31. Konstantinides FN, Konstantinides NN, Li JC, Myaya ME
and Cerra FB. Urinary urea nitrogen: too insensitive for
calculating nitrogen balance studies in surgical clinical nutrition.
JPEN J Parenter Enteral Nutr 15: 189-193, 1991.
32. Malmberg K, Ryden L, Efendic S, Herlitz J, Nicol P,
Waldenstrom A, Wedel H and Welin L. Randomized trial of
insulin-glucose infusion followed by subcutaneous insulin
treatment in diabetic patients with acute myocardial infarction
(DIGAMI study): effects on mortality at 1 year. J Am Coll Cardiol
26: 57-65, 1995.
33. Matthews DE, Bier DM, Rennie MJ, Edwards RH, Halliday
D, Millward DJ and Clugston GA. Regulation of leucine
metabolism in man: a stable isotope study. Science 214: 1129-
1131, 1981.
34. Matthews DE, Motil KJ, Rohrbaugh DK, Burke JF, Young
VR and Bier DM. Measurement of leucine metabolism in man
from a primed, continuous infusion of L-[1-3C]leucine. Am J
Physiol 238: E473-E479, 1980.
25

35. Matthews DE, Schwarz HP, Yang RD, Motil KJ, Young VR
and Bier DM. Relationship of plasma leucine and alpha-
ketoisocaproate during a L-[1-13C]leucine infusion in man: a
method for measuring human intracellular leucine tracer
enrichment. Metabolism 31: 1105-1112, 1982.
36. Mesotten D, Delhanty PJ, Vanderhoydonc F, Hardman
KV, Weekers F, Baxter RC and Van den Berghe GH.
Regulation of insulin-like growth factor binding protein-1 during
protracted critical illness. J Clin Endocrinol Metab 87: 5516-
5523, 2002.
37. Mesotten D, Swinnen JV, Vanderhoydonc F, Wouters PJ
and Van den Berghe GH. Contribution of circulating lipids to
the improved outcome of critical illness by glycemic control
with intensive insulin therapy. J Clin Endocrinol Metab 89: 219-
226, 2004.
38. Nair KS, Ford GC, Ekberg K, Fernqvist-Forbes E and
Wahren J. Protein dynamics in whole body and in splanchnic
and leg tissues in type I diabetic patients. J Clin Invest 95: 2926-
2937, 1995.
39. Nygren J, Thorell A, Brismar K, Karpe F and Ljungqvist O.
Short-term hypocaloric nutrition but not bed rest decrease
26
insulin sensitivity and IGF-I bioavailability in healthy subjects:
the importance of glucagon. Nutrition 13: 945-951, 1997.
40. Rusavy Z, Sramek V, Lacigova S, Novak I, Tesinsky P and
Macdonald IA. Influence of insulin on glucose metabolism and
energy expenditure in septic patients. Crit Care 8: R213-R220,
2004.
41. Russell-Jones DL, Umpleby AM, Hennessy TR, Bowes SB,
Shojaee-Moradie F, Hopkins KD, Jackson NC, Kelly JM,
Jones RH and Sonksen PH. Use of a leucine clamp to
demonstrate that IGF-I actively stimulates protein synthesis in
normal humans. Am J Physiol 267: E591-E598, 1994.
42. Schricker T, Klubien K, Wykes L and Carli F. Effect of
epidural blockade on protein, glucose, and lipid metabolism in
the fasted state and during dextrose infusion in volunteers.
Anesthesiology 92: 62-69, 2000.
43. Shangraw RE, Jahoor F, Miyoshi H, Neff WA, Stuart CA,
Herndon DN and Wolfe RR. Differentiation between septic
and postburn insulin resistance. Metabolism 38: 983-989, 1989.
44. Shangraw RE, Stuart CA, Prince MJ, Peters EJ and Wolfe
RR. Insulin responsiveness of protein metabolism in vivo
27

following bedrest in humans. Am J Physiol 255: E548-E558,
1988.
45. Shaw JH, Klein S and Wolfe RR. Assessment of alanine, urea,
and glucose interrelationships in normal subjects and in
patients with sepsis with stable isotopic tracers. Surgery 97:
557-568, 1985.
46. Shojaee-Moradie F, Jackson NC, Jones RH, Mallet AI,
Hovorka R and Umpleby AM. Quantitative measurement of
3-O-methyl-D-glucose by gas chromatography-mass
spectrometry as a measure of glucose transport in vivo. J Mass
Spectrom 31: 961-966, 1996.
47. Sonksen PH. Hormones in Human Blood: Detection and Assay.
176-199. 1976. Cambridge, MA, Harvard University Press.
Ref Type: Generic
48. Stuart CA, Shangraw RE, Prince MJ, Peters EJ and Wolfe
RR. Bed-rest-induced insulin resistance occurs primarily in
muscle. Metabolism 37: 802-806, 1988.
49. Taniguchi CM, Emanuelli B and Kahn CR. Critical nodes in
signalling pathways: insights into insulin action. Nat Rev Mol
Cell Biol 7: 85-96, 2006.
28
50. Tessari P, Inchiostro S, Biolo G, Trevisan R, Fantin G,
Marescotti MC, Iori E, Tiengo A and Crepaldi G. Differential
effects of hyperinsulinemia and hyperaminoacidemia on
leucine-carbon metabolism in vivo. Evidence for distinct
mechanisms in regulation of net amino acid deposition. J Clin
Invest 79: 1062-1069, 1987.
51. Tessari P, Inchiostro S, Biolo G, Trevisan R, Fantin G,
Marescotti MC, Iori E, Tiengo A and Crepaldi G. Differential
effects of hyperinsulinemia and hyperaminoacidemia on
leucine-carbon metabolism in vivo. Evidence for distinct
mechanisms in regulation of net amino acid deposition. J Clin
Invest 79: 1062-1069, 1987.
52. Thorell A, Rooyackers O, Myrenfors P, Soop M, Nygren J
and Ljungqvist OH. Intensive insulin treatment in critically ill
trauma patients normalizes glucose by reducing endogenous
glucose production. J Clin Endocrinol Metab 89: 5382-5386,
2004.
53. Tissot S, Delafosse B, Normand S, Bouffard Y, Annat G,
Viale JP, Pachiaudi C, Riou JP and Motin J. Recovery of
[13C]bicarbonate as respiratory 13CO2 in mechanically
ventilated patients. Am J Clin Nutr 57: 202-206, 1993.
29

54. Van den Berghe GH. Endocrine evaluation of patients with
critical illness. Endocrinol Metab Clin North Am 32: 385-410,
2003.
55. Van den Berghe GH, Wilmer A, Hermans G, Meersseman
W, Wouters PJ, Milants I, Van WE, Bobbaers H and
Bouillon R. Intensive insulin therapy in the medical ICU. N Engl
J Med 354: 449-461, 2006.
56. Van den Berghe GH, Wouters P, Weekers F, Verwaest C,
Bruyninckx F, Schetz M, Vlasselaers D, Ferdinande P,
Lauwers P and Bouillon R. Intensive insulin therapy in the
critically ill patients. N Engl J Med 345: 1359-1367, 2001.
57. Van den Berghe GH, Wouters PJ, Bouillon R, Weekers F,
Verwaest C, Schetz M, Vlasselaers D, Ferdinande P and
Lauwers P. Outcome benefit of intensive insulin therapy in the
critically ill: Insulin dose versus glycemic control. Crit Care Med
31: 359-366, 2003.
58. Vary TC and Kimball SR. Sepsis-induced changes in protein
synthesis: differential effects on fast- and slow-twitch muscles.
Am J Physiol 262: C1513-C1519, 1992.
59. Wilmore DW. Postoperative protein sparing. World J Surg 23:
545-552, 1999.
30

60. Wolfe RR. Glycerol Flux. Radioactive and stable isotope tracers
in biomedicine. 325-326. 1992. New York, Wiley-Liss.
Ref Type: Generic
31
Figure 1
Subject recruited to study Study 1 Study 2
LILG
LIHG
HILG
HIHG
10 - 18 h 48 h
Blood glucose7 – 9 mmol/L
32

Figure 2
Primed, constant infusion of stable isotopes of leucine, glucose and glycerol
Insulin 0.5 mU kg-1min-1
Insulin 2.0 mU kg-1min-1
0 330 360 510 540 min
Blood samples
Indirect calorimetry
Variable glucose infusion
150 180
33
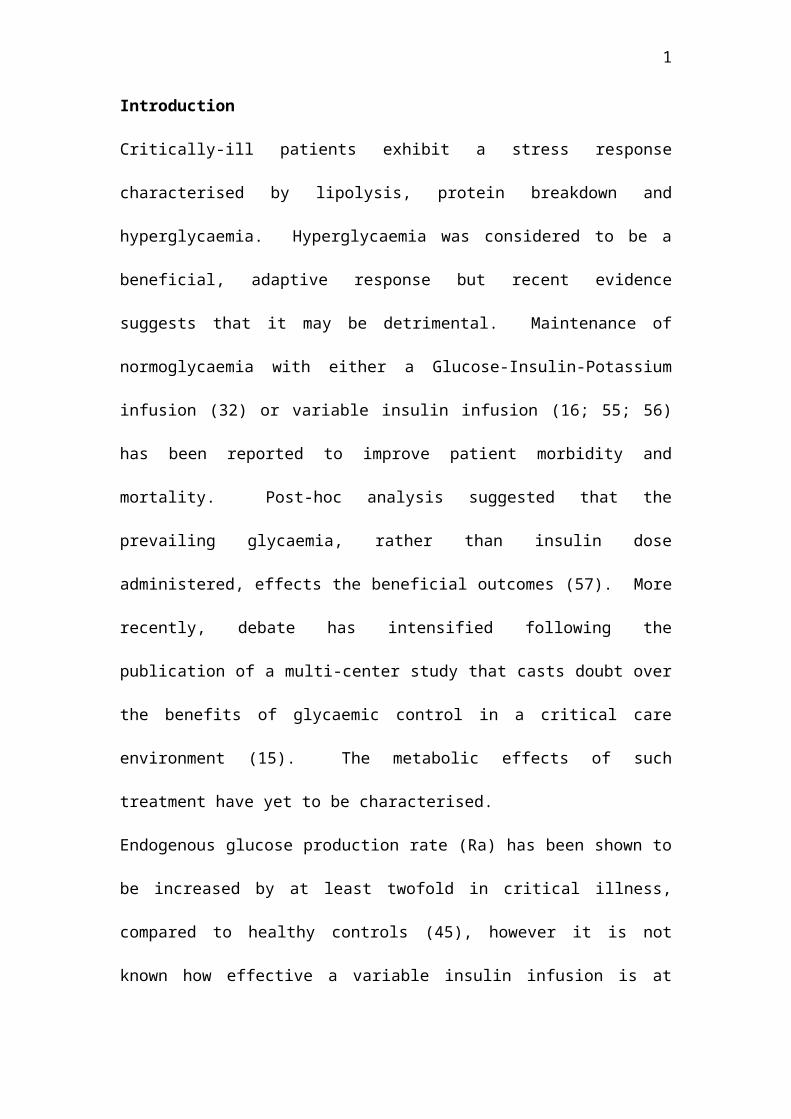
Figure 3. Leucine Ra
34

Figure 4. Net protein balance
35

Figure Legends
Figure 1. Study protocol for patients. Low-insulin high-glucose, LIHG (variable
insulin with BG of 7 – 9mmol/L; n=7), Low-insulin low-glucose, LILG (variable
insulin with BG of 4 – 6mmol/L; n=6), High-insulin high-glucose, HIHG (high dose
insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement from study one with
BG of 7 – 9mmol/L; n=6), High-insulin low-glucose, HILG (high dose insulin
infusion [2.0 mU kg-1min-1] plus the insulin requirement from study one with BG of 4
– 6mmol/L; n=6).
Figure 2. Study protocol for control subjects.
Figure 3. Rate of leucine appearance (leucine Ra) in the patient group. Low-insulin
high-glucose, LIHG (variable insulin with BG of 7 – 9mmol/L; n=7), Low-insulin
low-glucose, LILG (variable insulin with BG of 4 – 6mmol/L; n=6), High-insulin
high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
requirement from study one with BG of 7 – 9mmol/L; n=6), High-insulin low-
glucose, HILG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
requirement from study one with BG of 4 – 6mmol/L; n=6). Low-dose insulin (0.5
mU kg-1min-1), LI. High-dose insulin (2.0 mU kg-1min-1), HI. Mean ± SEM.
Figure 4. Calculated net protein balance over a 24 hour period. Study one (black
boxes) and study two (hatched boxes). Low-insulin high-glucose, LIHG (variable
insulin with BG of 7 – 9mmol/L; n=7), Low-insulin low-glucose, LILG (variable
insulin with BG of 4 – 6mmol/L; n=6), High-insulin high-glucose, HIHG (high dose
36
insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement from study one with
BG of 7 – 9mmol/L; n=6), High-insulin low-glucose, HILG (high dose insulin
infusion [2.0 mU kg-1min-1] plus the insulin requirement from study one with BG of 4
– 6mmol/L; n=6). Mean ± SEM.
37

Table 1. Group Characteristics
LILG
(n=6)
LIHG
(n=7)
HILG
(n=6)
HIHG
(n=6)
Gender (M/F) 4 / 2 6 / 1 3 / 3 4 / 2
Age (yr) 70.8 ± 5.1 66.0 ± 4.4 68.5 ± 2.6 58.2 ± 7.4
BMI (kg/m2) 24.8 ± 2.4 25.3 ± 1.8 27.1 ± 3.0 27.3 ± 2.7
APACHE II Study 1 17.2 ± 2.8 15.9 ± 1.4 15.0 ± 2.6 19.2 ± 2.9
Study 2 15.4 ± 1.5 17.0 ± 1.8 18.3 ± 3.6 18.3 ± 2.8
Plasma glucose
(mmol/L)
Study 1 7.94 ± 0.92 7.41 ± 0.44 8.02 ± 0.47 8.46 ± 0.69
Study 2 5.60 ± 0.43 a 8.81 ± 0.41 4.76 ± 0.39 a 8.09 ± 0.47
Insulin infusion
(U/h)
Study 1 5.28 ± 1.26 3.97 ± 0.7 4.02 ± 0.85 5.73 ± 1.93
Study 2 5.03 ± 1.76 2.09 ± 0.73 13.57 ± 1.61 a b 15.48 ± 2.67 a b
Inotropes (n) Study 1 5 4 3 2
Study 2 0 1 2 0
Glucocorticoids
(n)
Study 1 5 6 4 2
Study 2 3 6 3 2
Propofol (n) Study 1 4 5 3 6
Study 2 2 4 3 6
Heparin (n) Study 1 1 1 2 3
Study 2 1 1 3 3
CRP (mg/L) Study 1 118.3 ± 28.7 150.0 ± 48.8 180.8 ± 50.6 72.8 ± 26.0
Study 2 79.3 ± 24.1 83.7 ± 29.7 129.8 ± 29.6 45.5 ± 16.1
Mean daily caloric intake (kcal/day)
1725 ± 107 1779 ± 222 2885 ± 344 4217 ± 678 b
Data are mean ± SEM. a P ≤ 0.01 v study 1, b P < 0.001 v low-insulin groups.
Low-insulin high-glucose, LIHG (variable insulin with BG of 7 – 9mmol/L), Low-
insulin low-glucose, LILG (variable insulin with BG of 4 – 6mmol/L), High-insulin
38
high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
requirement from study one with BG of 7 – 9mmol/L), High-insulin low-glucose,
HILG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement
from study one with BG of 4 – 6mmol/L). Acute Physiology and Chronic Health
Evaluation score II (APACHE II), C-reactive protein (CRP).
39
Table 2. Hormone Concentration
Insulin
(pmol/L)
C-peptide
(nmol/L)
Cortisol
(nmol/L)
LILG
(n=6)
Study 1 287.24 ± 75.70 3.19 ± 1.04 920.55 ± 410.67
Study 2 293.18 ± 81.73 0.53 ± 0.13 a 825.05 ± 222.21
LIHG
(n=7)
Study 1 221.69 ± 28.80 2.56 ± 0.34 1276.58 ± 416.07
Study 2 193.58 ± 27.24 2.50 ± 0.45 840.51 ± 129.65
HILG
(n=6)
Study 1 224.54 ± 28.45 2.43 ± 0.79 1122.27 ± 303.49
Study 2 1435.79 ± 204.05 a 0.28 ± 0.053 a 924.43 ± 211.96
HIHG
(n=6)
Study 1 340.04 ± 94.82 1.60 ± 0.49 1796.04 ± 626.68
Study 2 1769.12 ± 480.99 a 1.51 ± 0.69 1563.18 ± 632.37
Control
subjects
(n=5)
Basal 24.93 ± 5.60 0.70 ± 0.11 268.94 ± 22.08
LI 318.63 ± 26.20 b 0.42 ± 0.036 c 344.80 ± 40.73
HI 1922.85 ± 192.50 b 0.37 ± 0.066 c 365.25 ± 98.93
Data are mean ± SEM. a P < 0.05 v study 1, b P < 0.001 v basal control, c P < 0.05 v
basal control. Low-insulin high-glucose, LIHG (variable insulin with BG of 7 –
9mmol/L), Low-insulin low-glucose, LILG (variable insulin with BG of 4 –
6mmol/L), High-insulin high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-
1min-1] plus the insulin requirement from study one with BG of 7 – 9mmol/L), High-
insulin low-glucose, HILG (high dose insulin infusion [2.0 mU kg-1min-1] plus the
insulin requirement from study one). Low-dose insulin (0.5 mU kg-1min-1), LD.
High-dose insulin (2.0 mU kg-1min-1), HD.
40

Table 3. Plasma Metabolite Concentration
Lactate
(mmol/L)
NEFA
(mmol/L)
Glycerol
(µmol/L)
Total
Cholesterol
(mmol/L)
LILG
(n=6)
Study 1 1.63 ± 0.36 0.19 ± 0.07 75.68 ± 19.70 2.16 ± 0.39 a
Study 2 1.67 ± 0.16 0.42 ± 0.27 68.72 ± 18.15 b 2.56 ± 0.31 a
LIHG
(n=7)
Study 1 1.65 ± 0.34 0.25 ± 0.09 73.87 ± 12.38 2.42 ± 0.29 a
Study 2 1.53 ± 0.34 0.22 ± 0.05 c 58.14 ± 7.45 b 2.68 ± 0.39 a
HILG
(n=6)
Study 1 1.84 ± 0.43 0.27 ± 0.13 68.30 ± 24.32 2.34 ± 0.33 a
Study 2 1.70 ± 0.22 0.07 ± 0.02 c 63.26 ± 10.96 b 2.34 ± 0.35 a
HIHG
(n=6)
Study 1 1.86 ± 0.32 0.19 ± 0.05 74.14 ± 18.02 2.88 ± 0.46 a
Study 2 2.15 ± 0.17 0.15 ± 0.05 c 101.88 ± 12.93 c 2.92 ± 0.35 a
Control
subjects
(n=5)
Basal - 0.67 ± 0.11 62.20 ± 5.30 4.88 ± 0.38
LI - 0.04 ± 0.005 d 8.42 ± 2.06 d -
HI - 0.02 ± 0.006 d 7.74 ± 1.48 d -
Data are mean ± SEM. a P ≤ 0.01 v basal control, b P < 0.001 v LD and HD control, c P < 0.05 v
HD controls, d P < 0.001 v basal control.
Low-insulin high-glucose, LIHG (variable insulin with BG of 7 – 9mmol/L), Low-
insulin low-glucose, LILG (variable insulin with BG of 4 – 6mmol/L), High-insulin
high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
requirement from study one with BG of 7 – 9mmol/L), High-insulin low-glucose,
HILG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement
41
from study one with BG of 4 – 6mmol/L). Low-dose insulin (0.5 mU kg-1min-1), LI.
High-dose insulin (2.0 mU kg-1min-1), HI.
42

Table 4 Glycerol production rate, leucine oxidation rate and NOLD
Glycerol Ra
(µmol kg-1min-1)
Leucine
oxidation
(µmol kg-1min-1)
NOLD
(µmol kg-1min-1)
LILG
(n=6)
Study 1 1.74 ± 0.28 0.40 ± 0.08 1.57 ± 0.20
Study 2 1.66 ± 0.24 0.44 ± 0.10 1.61 ± 0.18
LIHG
(n=7)
Study 1 1.37 ± 0.21 0.48 ± 0.09 1.69 ± 0.23
Study 2 1.30 ± 0.21 0.48 ± 0.05 1.63 ± 0.19
HILG
(n=6)
Study 1 1.94 ± 0.71 0.24 ± 0.03 1.65 ± 0.08
Study 2 1.90 ± 0.28 0.35 ± 0.03 1.66 ± 0.12
HIHG
(n=6)
Study 1 1.45 ± 0.11 0.29 ± 0.04 1.27 ± 0.08
Study 2 2.67 ± 0.71 0.34 ± 0.05 1.98 ± 0.31
Control
subjects
(n=5)
Basal 4.07 ± 0.45 - -
LI 1.33 ± 0.17 a - -
HI 1.22 ± 0.16 a - -
Data are mean ± SEM. a P < 0.05 v basal control.
Low-insulin high-glucose, LIHG (variable insulin with BG of 7 – 9mmol/L), Low-
insulin low-glucose, LILG (variable insulin with BG of 4 – 6mmol/L), High-insulin
high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
43

requirement from study one with BG of 7 – 9mmol/L), High-insulin low-glucose,
HILG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement
from study one). Low-dose insulin (0.5 mU kg-1min-1), LI. High-dose insulin (2.0
mU kg-1min-1), HI. Endogenous glucose rate of appearance (Endog glucose Ra),
glucose rate of disappearance (glucose Rd), glycerol rate of appearance (glycerol Ra),
non-oxidative leucine disposal (NOLD).
Table 5. Glucose turnover data and RQ
44

Endog Glucose Ra
(mg kg-1min-1)
Glucose Rd
(mg kg-1min-1)
RQ
LILG
(n=6)
Study 1 0.069 ± 0.54 3.80 ± 0.69 0.83 ± 0.03
Study 2 0.61 ± 0.40 3.89 ± 0.65 0.88 ± 0.02
LIHG
(n=7)
Study 1 0.61 ± 0.45 4.09 ± 0.34 0.80 ± 0.04
Study 2 0.87 ± 0.24 4.36 ± 0.20 0.79 ± 0.03
HILG
(n=6)
Study 1 0.51 ± 0.32 4.27 ± 0.68 0.81 ± 0.02
Study 2 -1.10 ± 0.57 a h 7.04 ± 0.80 b c d 1.02 ± 0.03 a b
HIHG
(n=6)
Study 1 0.67 ± 0.32 4.07 ± 0.46 0.84 ± 0.05
Study 2 0.20 ± 0.33 h 7.46 ± 0.87 a b c e 1.02 ± 0.02 a b
Control
subjects
(n=5)
Basal 1.89 ± 0.058 1.89 ± 0.058 0.82 ± 0.02 c
LI 0.46 ± 0.59 4.58 ± 0.32 f 0.88 ± 0.01 c
HI -0.92 ± 0.41 f h 10.15 ± 0.57 f g 0.99 ± 0.03
Data are mean ± SEM. a P < 0.007 v HILG group at study 1, b P < 0.02 v LILG group at
study 2, c P < 0.03 v HI control, d P = 0.05 v LIHG at study 2, e P < 0.02 v LIHG group
at study 2, f P ≤ 0.05 v basal control, g P < 0.003 v LI control, h NS different from zero
Low-insulin high-glucose, LIHG (variable insulin with BG of 7 – 9mmol/L), Low-
insulin low-glucose, LILG (variable insulin with BG of 4 – 6 mmol/L), High-insulin
high-glucose, HIHG (high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin
requirement from study one with BG of 7 – 9mmol/L), High-insulin low-glucose, HILG
(high dose insulin infusion [2.0 mU kg-1min-1] plus the insulin requirement from study
one with BG of 4 – 6mmol/L). Low-dose insulin (0.5 mU kg-1min-1), LI. High-dose
insulin (2.0 mU kg-1min-1), HI. Endogenous glucose rate of appearance (Endog glucose
45
Ra), glucose rate of disappearance (glucose Rd), glycerol rate of appearance (glycerol
Ra), non-oxidative leucine disposal (NOLD).
46

![INDEX [] · INDEX Grinders Hammers Drills Drivers Mixers Saws Planers PICTOGRAPH Double Insulation Variable Speed Reversing Operation ... AJP-55 33 AJP-1210 33 AJP-1310 33 AJP-1410](https://img.dokumen.tips/doc/110x75/5b95ee9e09d3f2205c8d5951/index-index-grinders-hammers-drills-drivers-mixers-saws-planers-pictograph.jpg)



























