Embed Size (px)
Citation preview

Am J Cancer 2003; 2 (2): 95-109REVIEW ARTICLE 1175-6357/03/0002-0095/$30.00/0
© Adis Data Information BV 2003. All rights reserved.
Postmenopausal Metastatic Breast CancerA Review of First-Line Treatment Options
Laura Assersohn and Stephen R.D. Johnston
Breast Unit, Royal Marsden Hospital, London, UK
Contents
Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 951. Endocrine Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
1.1 Anti-Estrogens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 971.2 Aromatase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 981.3 Clinical Efficacy After Tamoxifen . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 991.4 Aromatase Inhibitors vs Tamoxifen as First-Line Treatment of Metastatic Disease . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 991.5 Future Directions with Endocrine Treatments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100
2. Chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1002.1 Anthracyclines . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1012.2 Taxanes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1012.3 Taxanes as Single Agent First-Line Chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1012.4 Combination of an Anthracycline and a Taxane . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1032.5 Other Chemotherapy Agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1042.6 High-Dose Chemotherapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104
3. Bisphosphonates . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1054. Novel Biological Therapies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 105
4.1 Trastuzumab. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1054.2 Tyrosine Kinase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1064.3 Farnesyl Transferase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 106
Endocrine therapy and chemotherapy play important roles in the management of postmenopausal womenAbstractwith metastatic breast cancer. This paper specifically reviews the indications and options for first-line treatmentof metastatic breast cancer and recent advances are highlighted, with particular attention to randomized,controlled, phase III clinical trials.
Until recently, tamoxifen was standard first-line endocrine treatment for patients with metastatic breastcancer. Now, potent third generation aromatase inhibitors, such as letrozole and anastrozole, have shownsuperiority to tamoxifen as first-line endocrine treatment and provide an alternative for postmenopausal women.
The most active chemotherapy agents for patients with advanced breast cancer have, until recently, been theanthracyclines, doxorubicin and epirubicin. However, their increasing use in the adjuvant setting has resulted in aneed for novel active non-cross-resistant cytotoxic drugs for metastatic breast cancer. Real progress has beenmade with the introduction of the taxanes, paclitaxel and docetaxel. Other developments include the use of singleagent cytotoxics such as vinorelbine, the oral fluoropyrimidine capecitabine and gemcitabine, all of which havesome activity following either taxanes or anthracyclines, along with a low toxicity profile. Bisphosphonates arebone-specific palliative treatments that have been instituted on the basis of their impact on symptoms andskeletal related morbidity.

96 Assersohn & Johnston
Finally, the era of biological therapy in the clinic for patients with breast cancer has been heralded with thedevelopment and introduction of trastuzumab, a humanized monoclonal antibody which targets the cell surfacegrowth factor receptor HER2/neu. Importantly, each of these new treatment options has provided an incrementalimprovement in efficacy over previous standard first-line therapies.
Breast cancer is the second most common cause of cancer-relat- X-ray, bone scan, and liver imaging. For many patients, radiologi-ed death in Western Europe and North American women. In the cal evaluation may be undertaken by computerized tomographyUK, breast cancer is the leading cause of death amongst women (CT) scans. Cytological or histological documentation of recurrentaged 35–54, and the most common cause of death due to malig- or metastatic disease should be obtained whenever possible withnancy with over 13 000 deaths in 1998.[1,2] Women develop assessment of estrogen receptor (ER) and progesterone receptoradvanced breast cancer when there is a recurrence of disease at (PgR) levels and HER2/neu status either at the time of recurrencedistant sites, including bone, liver, lung or soft tissue, that are not or, if not possible, on the initial primary breast carcinoma.amenable to surgery and thus, by convention, have become incur- Adjuvant endocrine and cytotoxic systemic therapies are in-able. Around 50% of women initially presenting with early or creasingly used in early breast cancer to eliminate micrometastaticlocalized breast cancer which is managed surgically will eventual- disease and have been shown to improve survival significantly.[4,5]
ly develop advanced or metastatic breast cancer. The two primary The interval since completion of such treatment and the develop-goals in the treatment of such patients are improvement or mainte- ment of metastases (disease-free interval) is important in deter-nance of quality of life, and prolongation of survival. This is mining which treatment options may be successful in the advancedachieved predominantly by employing systemic anticancer drugs setting.[6] Other clinical factors, such as site(s) of disease involved(endocrine therapy and chemotherapy) to induce tumor regression, and ER and/or PgR status help determine the initial systemicin conjunction with effective supportive care therapies to alleviate treatment, particularly the choice between endocrine therapy ortumor and/or treatment related symptoms. chemotherapy (table I). In addition, the choice of a specific drug or
Although median survival for women with metastatic breast regimen for an individual is dependent on the prior therapiescancer is in the range of 2–3 years, there is wide variability in the received in the adjuvant setting, together with the likelihood ofcourse of the disease. This is important for the individual patient benefit balanced against a given drug’s adverse effect and tolera-and the interpretation of clinical trials. Such heterogeneity encom- bility profile.passes those few patients who die of their disease within weeks ofdiagnosis and those who live for many years. Median survival is in 1. Endocrine Therapythe range of 2–3 years but, in one series, up to 20% of patients whorespond to chemotherapy may remain alive up to 10 years later.[3] Hormonal manipulation has been recognized as a treatmentSome patients have predominantly visceral disease while for modality for breast cancer for over 100 years. Estrogen is anothers, it is confined to bone or soft tissue. important promotor in the pathogenesis of breast cancer and as
Patients with a new diagnosis of metastatic breast cancer re- endocrine maneuvers are an effective and relatively non-toxicquire re-staging to evaluate the extent of disease prior to decisions treatment, it is important to reliably identify those patients whoon the most appropriate treatment. This includes blood test, such will benefit. Seventy-five percent of primary breast cancers ex-as complete full blood count, renal function, serum calcium, and press ER and/or PgR and, therefore, may be dependent on estrogenliver function tests, along with radiological evaluation with chest for their growth. Routine immunohistochemical assays, which can
Table I. Clinical factors in postmenopausal women with metastatic breast carcinoma that may predict initial response to endocrine therapy
Factors predictive for response to endocrine treatment ER- and/or PgR-positive tumor
Soft tissue sites of disease (skin, lymph nodes)
Long disease free interval since primary therapy for early breast cancer
Factors making initial endocrine therapy less appropriate ER- and PgR-negative tumor
Symptomatic visceral metatases (e.g. lymphangitis carcinomatosis, progressiveliver metastases)
Short disease free interval (12–18 months)
ER = estrogen receptor; PgR = progesterone receptor.
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

Postmenopausal Metastatic Breast Cancer 97
be performed on archival paraffin-embedded tissue, mean that this activity with fulvestrant may delay or prevent tumor regrowth thatinformation should be available for all breast cancer patients. is commonly seen with tamoxifen. In a small phase II study,[11]
While concern has been raised that ER expression in metastatic fulvestrant produced an objective response rate of 36.8% andbreast cancer may not represent that observed in the primary durable remissions of at least 2 years in tamoxifen-resistant tumorstumor, studies have consistently shown that a large number of ER- in postmenopausal women. This compares favorably with stan-positive tumors retain receptor expression at relapse with metastat- dard second-line endocrine therapy, which usually produces medi-ic breast cancer.[7,8] an remissions of 1 year.
Two large recent phase III trials have shown that fulvestrant,which is administered as a subcutaneous injection, is as effective1.1 Anti-Estrogensas anastrozole as second-line therapy following tamoxifen fai-lure.[12,13] However, the real test will be whether the reducedIn hormone-dependent breast cancer cells, estrogen binds toagonist profile of fulvestrant improves the efficacy over tamoxifennuclear ER resulting in dimerization of receptor, which interactswhen given as first-line therapy, and the results of a large prospec-with DNA at specific estrogen response elements (ERE) upstreamtive, randomized, controlled trial are awaited.of estrogen-dependent genes. This in turn results in the activation
Nonsteroidal SERMs are anti-estrogen compounds that have aand transcription of these genes, including those involved in cellreduced agonist profile on breast and gynecological tissues. How-growth. Tamoxifen is an oral, nonsteroidal, competitive ER antag-ever, phase III trials which involved randomizing betweenonist, which has been standard first-line endocrine therapy oftoremifene or idoxifene (tamoxifen-like SERMs) and tamoxifen inchoice for hormone-sensitive advanced breast cancer. Tamoxifenmore than 1500 patients, demonstrated no benefit over tamox-and the newer selective estrogen receptor modulators (SERMs) actifen.[14] As first-line therapy for advanced breast cancer, medianby competitively inhibiting the binding of estradiol to the ER.response rate was 31% with a median time to progression of 7While tamoxifen-liganded ER complex still binds to estrogenmonths. The other main class of SERMs include the benzothi-response elements, the transcriptional activation of AF2 regulatedophene derivatives raloxifene and arzoxifene. While raloxifene isgenes is inhibited. The partial agonist activity of tamoxifen is, inapproved for osteoporosis prevention, very limited phase II datapart, due to the fact that some genes (those regulated by the AF1exist on its activity in metastatic breast cancer.[15,16] To date, theredomain of ER) remain activated. High response rates (50–60%)is no evidence that SERMs have significant activity followinghave been reported with tamoxifen for those with ER-positivetamoxifen failure, and likewise no randomized data to show anydisease with a median duration of response of 8–14 months.[9]
superiority over tamoxifen as first-line treatment.However, after an initial response to tamoxifen, resistance usuallydevelops, leading to disease progression, even though the tumors As it appears that cross-resistance with tamoxifen occurs withremain endocrine-sensitive.[10] Furthermore, most patients will these agents, it was anticipated that one of the SERMs may replacehave already received tamoxifen in the adjuvant setting, and some tamoxifen as first-line adjuvant hormone therapy due to compara-patients may relapse with metastatic disease while still taking ble efficacy and fewer tolerability problems. However, the aro-tamoxifen. Nevertheless, at present, first-line endocrine treatment matase inhibitors may well prove to be a more effective treatmentwith tamoxifen is indicated in the metastatic setting if it has not option in this scenario, although concerns remain regarding pro-been previously administered as adjuvant therapy, or if the patient tection from bone loss. While the use of SERMs appears to behas stopped anti-estrogen therapy for more than 1 year. In addi- promising in the treatment of breast cancer, their real potentialtion, the tumor should be ER- and/or PgR-positive or, if the tumor may be as disease prevention agents, encompassing breast cancer,is of unknown ER/PgR status, clinical factors, such as predom- cardiovascular disease, and bone mineral density loss in postmen-inantly bone or soft tissue disease, may indicate that endocrine opausal women, and thus substituting hormone replacement ther-treatment is an appropriate treatment option. apy. As it has been shown that tamoxifen may reduce breast cancer
Pure steroidal anti-estrogens, such as fulvestrant (previously incidence, although with an associated increased risk of endome-ICI 182,780), have been developed which appear to lack any trial cancer and thrombotic events, the current Study of Tamoxifenestrogen-like agonist activity and, as such, may cause less en- and Raloxifene (STAR) chemoprevention trial is comparing thedometrial proliferation or thromboembolism than tamoxifen. This effects of raloxifene and tamoxifen.[17] Thus, the potential existslack of agonist activity relates to the different mechanism of that raloxifene may reduce breast cancer incidence with an im-action, whereby fulvestrant binds to ER but prevents dimerization proved tolerability profile compared with tamoxifen and it isand DNA binding, in turn causing the down-regulation of ER hoped that this trial will also clarify which patients will deriveprotein levels. Preclinical studies suggested that the lack of agonist benefit from chemoprevention.
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)
98 Assersohn & Johnston
CH2
O
O
O
O
OH
NH2
C2H5
N OO
H
Aminoglutethimide
FormestaneExemestane
NN
N
NC CN
Letrozole
Nonsteroidal inhibitors
Steroidal inactivators
NN
N
NC CNCH3
CH3 CH3
CH3
Anastrozole
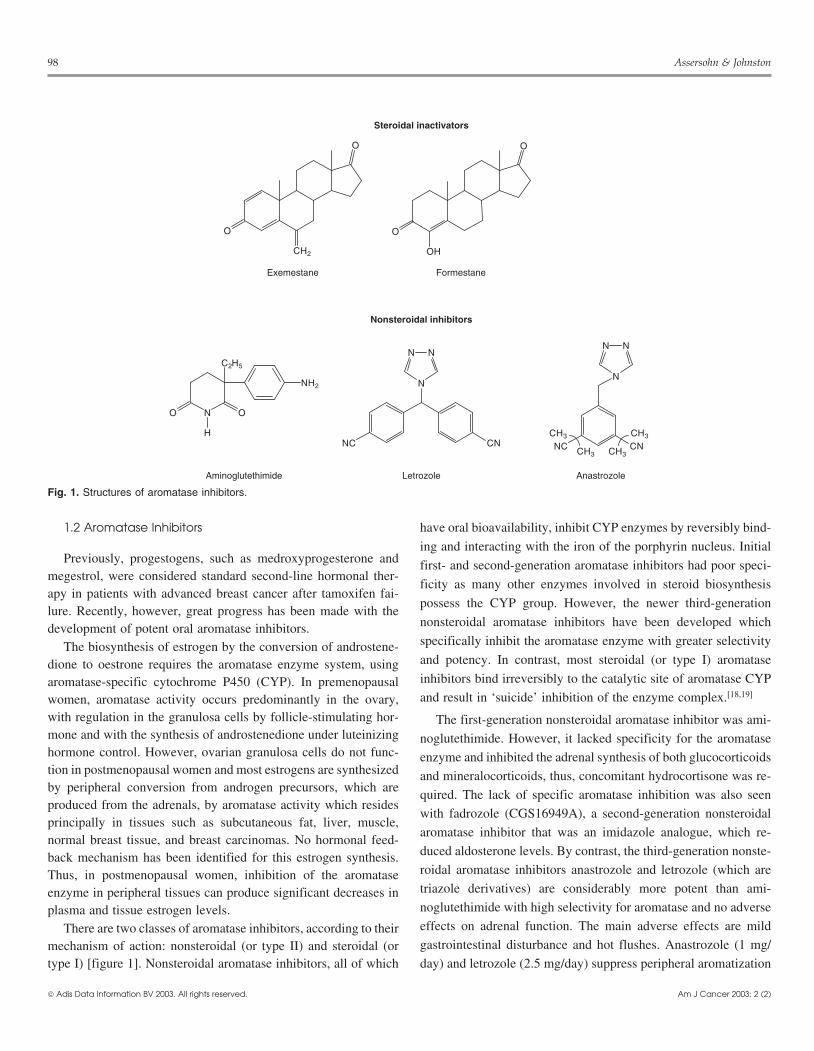
Fig. 1. Structures of aromatase inhibitors.
1.2 Aromatase Inhibitors have oral bioavailability, inhibit CYP enzymes by reversibly bind-
ing and interacting with the iron of the porphyrin nucleus. InitialPreviously, progestogens, such as medroxyprogesterone and first- and second-generation aromatase inhibitors had poor speci-
megestrol, were considered standard second-line hormonal ther-ficity as many other enzymes involved in steroid biosynthesis
apy in patients with advanced breast cancer after tamoxifen fai-possess the CYP group. However, the newer third-generation
lure. Recently, however, great progress has been made with thenonsteroidal aromatase inhibitors have been developed whichdevelopment of potent oral aromatase inhibitors.specifically inhibit the aromatase enzyme with greater selectivityThe biosynthesis of estrogen by the conversion of androstene-and potency. In contrast, most steroidal (or type I) aromatasedione to oestrone requires the aromatase enzyme system, usinginhibitors bind irreversibly to the catalytic site of aromatase CYParomatase-specific cytochrome P450 (CYP). In premenopausaland result in ‘suicide’ inhibition of the enzyme complex.[18,19]women, aromatase activity occurs predominantly in the ovary,
with regulation in the granulosa cells by follicle-stimulating hor- The first-generation nonsteroidal aromatase inhibitor was ami-mone and with the synthesis of androstenedione under luteinizing noglutethimide. However, it lacked specificity for the aromatasehormone control. However, ovarian granulosa cells do not func- enzyme and inhibited the adrenal synthesis of both glucocorticoidstion in postmenopausal women and most estrogens are synthesized and mineralocorticoids, thus, concomitant hydrocortisone was re-by peripheral conversion from androgen precursors, which are
quired. The lack of specific aromatase inhibition was also seenproduced from the adrenals, by aromatase activity which resides
with fadrozole (CGS16949A), a second-generation nonsteroidalprincipally in tissues such as subcutaneous fat, liver, muscle,
aromatase inhibitor that was an imidazole analogue, which re-normal breast tissue, and breast carcinomas. No hormonal feed-
duced aldosterone levels. By contrast, the third-generation nonste-back mechanism has been identified for this estrogen synthesis.roidal aromatase inhibitors anastrozole and letrozole (which areThus, in postmenopausal women, inhibition of the aromatasetriazole derivatives) are considerably more potent than ami-enzyme in peripheral tissues can produce significant decreases innoglutethimide with high selectivity for aromatase and no adverseplasma and tissue estrogen levels.effects on adrenal function. The main adverse effects are mildThere are two classes of aromatase inhibitors, according to theirgastrointestinal disturbance and hot flushes. Anastrozole (1 mg/mechanism of action: nonsteroidal (or type II) and steroidal (or
type I) [figure 1]. Nonsteroidal aromatase inhibitors, all of which day) and letrozole (2.5 mg/day) suppress peripheral aromatization
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

Postmenopausal Metastatic Breast Cancer 99
by more than 95% and estradiol levels by 85% to less than 3 ρmol/ impressive for two reasons. The improved response duration seenL.[20] in those who benefited is significant; for example, in the letrozole
study, the median response duration was more than 33 months,compared with 18 months for megestrol.[23] The impact on overall1.3 Clinical Efficacy After Tamoxifensurvival for an endocrine agent is also important; there was anabsolute improvement in 2-year survival for anastrozole fromTwo phase III studies randomized a total of 764 postmenopaus-46.3% to 56.1% with a gain in median survival of 4 months.[22]
al women with advanced breast cancer who had progressed onSuch improvements in clinical endpoints for each of the new third-tamoxifen treatment, either as previous treatment for metastaticgeneration oral nonsteroidal aromatase inhibitors, together withbreast cancer or as adjuvant therapy, to anastrozole (1 or 10 mg/their consistently superior tolerability profile over megestrol (re-day) or megestrol (40mg four times daily). Although equivalentduced weight gain and thromboembolic events), defined their roleefficacy for anastrozole and megestrol was seen in terms ofas standard treatment after tamoxifen failure. As most patientsobjective response rates (10.3 and 7.9%, respectively) and diseasehave received tamoxifen as adjuvant treatment, much of the recentstabilization for 6 months (25.1 and 26.1%, respectively), anas-use of aromatase inhibitors has been first-line treatment, albeit introzole was better tolerated.[21] A subsequent analysis with medianpatients with tamoxifen-resistant disease. However, it rapidly be-follow-up of 31 months demonstrated a significant improvementcame important to compare these new endocrine agents directlyin overall survival for anastrozole (hazard ratio 0.78, p = 0.02).[22]
against tamoxifen as first-line therapy in hormone-sensitive pa-Another study demonstrated that letrozole significantly improvedtients who had not received or relapsed on adjuvant tamoxifen.the objective response rate (hazard ratio 1.82, p = 0.04) and time to
treatment progression (TTP) compared with megestrol in post-menopausal women with advanced breast cancer who had pre- 1.4 Aromatase Inhibitors vs Tamoxifen as First-Lineviously received anti-estrogen treatment.[23] However, no impact Treatment of Metastatic Diseaseon survival was detected in this study. A second more recent studyof letrozole vs megestrol showed that both drugs were equally Recent randomized phase III trials comparing a nonsteroidaleffective.[24] aromatase inhibitor and tamoxifen have challenged tamoxifen as
Exemestane is an orally active, third-generation type I steroidal the first-line endocrine agent of choice in metastatic breast cancerinhibitor. A phase II study demonstrated its efficacy after develop- (table II).[29-31] By instituting maximal estrogen blockade, theyment of tamoxifen resistance.[25] Likewise, a phase II study in may provide superior control of hormone-sensitive breast cancer,postmenopausal women with metastatic breast cancer who had thus circumventing the problem of acquired tamoxifen resistance.progressed after treatment with a nonsteroidal aromatase inhibitor The data are too immature at present for survival analyses in the(such as aminoglutethimide, anastrozole, letrozole) demonstrated three trials.that exemestane (25 mg/day) had a response rate (complete re- Two parallel trials compared anastrozole with tamoxifen assponse [CR] and partial response [PR]) of 6.6% and overall first-line treatment for patients with metastatic breast cancer. Aclinical benefit (CR, PR, and stable disease [SD] ≥24 weeks) of European study randomized more than 650 patients and demon-24.3%.[26] strated nearly identical response rates and TTP.[30] Only 288 (45%)
Another phase II study, in 80 postmenopausal women who had patients were known to be ER- and/or PgR-positive. TTP was 8.2progressed on aminoglutethimide, demonstrated an objective re- months and 8.3 months for anastrozole and tamoxifen, respective-sponse rate of 26% to a higher 200mg dose of exemestane with ly. Overall response rate (CR and PR) was similar for the twodisease stabilization of ≥24 weeks in an additional 13% of pa- treatments (32.9% of anastrozole and 32.6% of tamoxifen pa-tients.[27] These results suggest a lack of cross-resistance between tients) as was clinical benefit (CR + PR + SD ≥24 weeks) [56.2nonsteroidal and steroidal aromatase inhibitors. A recent phase III and 55.5% for patients receiving anastrozole and tamoxifen, re-trial demonstrated a significantly superior median TTP (20.3 vs spectively]. Both treatments were well tolerated with reduced16.6 weeks, p = 0.037) with exemestane compared with megestrol thromboembolic events and vaginal bleeding seen in the anas-in postmenopausal women following previous tamoxifen.[28] Me- trozole treatment arm compared with the tamoxifen arm. Thesedian survival was 123.4 weeks in the megestrol-treated patients results differed from the parallel North American study that ran-but had not been reached in the exemestane treated group (p = domized approximately 350 patients, of whom 85% were known0.039). to be ER- and/or PgR-positive.[29] This study demonstrated anas-
These results for aromatase inhibitors in women with metastat- trozole to be significantly superior to tamoxifen for TTP (11.1 vsic breast cancer who have progressed on tamoxifen are particularly 5.6 months, respectively, p = 0.005) and clinical benefit (CR + PR
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

100 Assersohn & Johnston
Table II. Phase III trials of aromatase inhibitors versus tamoxifen as first-line endocrine treatment for postmenopausal women with advanced breast cancer
Investigator n Treatment ER-positive (%) Response rate (%) Time to progression (mo)
Bonneterre et al.[30] 668 Anastrozole 146 (42.9) 32.9 8.2
Tamoxifen 142 (43.2) 32.6 8.3
Nabholtz et al.[29] 353 Anastrozole 145 (84.7) 21.0 11.1a
Tamoxifen 156 (85.7) 17.0 5.6
Mouridsen et al.[31] 907 Letrozole 294 (65) 30.0a 9.4a
Tamoxifen 305 (67) 20.0 6.0
Dirix et al.[32] 122 Exemestane ND 44.6b ND
Tamoxifen ND 14.3 ND
a p < 0.05 vs comparator.
b Preliminary data – trial not complete.
n = number of patients; ND = no data.
+ SD ≥24 weeks) [59 and 46% of patients, respectively, p = A randomized phase II study has compared exemestane totamoxifen as first-line treatment in 122 postmenopausal women0.0098]. Overall objective tumor response was similar (21 andwith metastatic disease.[32] Eleven patients in each treatment arm17%, respectively). It was thought that the results of the twohad received adjuvant tamoxifen. Exemestane demonstrated aparallel studies were dissimilar largely because of the different44.6% response rate with a further 10.7% patients showing diseasepercentage of patients with ER- and/or PgR-positive tumors (45%stabilization for 6 months or more, while tamoxifen had a 14.3%in the European study and 85% in US study). It was planned fromresponse rate.the outset to combine the results of the two studies. Therefore, a
subset analysis of patients with ER-positive tumors from both1.5 Future Directions with Endocrine Treatments
trials was performed and anastrozole was significantly better thanIt remains to be determined whether or not the superior re-tamoxifen with an improved TTP (10.7 vs 6.4 months, p =
sponse rates and TTP seen with anastrozole and letrozole will0.022).[33] This confirmed that anastrozole is at least equivalent to,translate into significant survival advantages over tamoxifen inand possibly superior to, tamoxifen in the first-line setting.metastatic disease. Nevertheless, preliminary results have suggest-
More recently, a single large prospective phase III study hased that the aromatase inhibitors may provide an important addition
been reported in which more than 900 women with metastaticto tamoxifen in the ongoing adjuvant trials in early breast can-
breast cancer were randomized to first-line endocrine treatment cer.[34] At present, as a result of these phase III trials, a nonster-with letrozole or tamoxifen.[31] Ten percent of patients had pre- oidal aromatase inhibitor, using anastrozole or letrozole, has be-viously received chemotherapy for metastatic disease and only come the standard first-line endocrine treatment in postmenopaus-15% had prior tamoxifen in the adjuvant setting which had been al women with metastatic breast cancer. In the future, ifcompleted more than 12 months prior to study entry. Sixty-six nonsteroidal aromatase inhibitors are employed in the adjuvantpercent of patients with tumors were known to be ER- and/or PgR- setting, it will become important to see which endocrine agentspositive. TTP was significantly longer for letrozole compared with remain the first-line treatment of choice in metastatic disease. Ittamoxifen (9.4 vs 6.0 months, p < 0.0001). Overall response rate remains unclear, however, to what extent there is non-cross-(CR + PR) was higher for letrozole (30 vs 20%, p = 0.0006) as was resistance between steroidal and nonsteroidal aromatase inhibi-clinical benefit (CR + PR + SD ≥24 weeks) [49 vs 38%, p = 0.001]. tors, and whether one class of drug can be used in sequence after
the other. Further clinical trials in this area are needed. Likewise,The benefit for letrozole over tamoxifen appeared irrespective ofstudies of the pure steroidal anti-estrogen fulvestrant are beingdominant site of disease, receptor status or prior adjuvant therapy.undertaken in patients who have progressed on aromatase inhibi-In particular, it is noteworthy that a significantly higher responsetors to define the role of this drug in such a setting.rate was seen in the subset of patients who had received prior
adjuvant tamoxifen (29% for letrozole vs 8% for tamoxifen, p =2. Chemotherapy
0.002). Likewise in those with visceral as the dominant site ofdisease, letrozole was consistently superior to tamoxifen (26% for The role of chemotherapy as palliation for patients with meta-letrozole vs 16% for tamoxifen, p = 0.02). static breast cancer is well established. Chemotherapy is the first-
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

Postmenopausal Metastatic Breast Cancer 101
line treatment of choice for patients in whom rapid tumor control performed a randomized study that compared two dose schedulesis required, such as those patients with extensive or symptomatic of FEC (FEC-75 with epirubicin at 75mg/m2 and FEC-50 withvisceral involvement and those patients with ER-/PgR- (hormone epirubicin at 50 mg/m2) with single agent epirubicin.[43] FEC wasinsensitive) tumors. In addition, those patients that have become superior to single agent epirubicin and FEC-75 produced higherrefractory to endocrine therapy are then considered candidates for response rates, along with overall survival (p = 0.006), comparedchemotherapy. with FEC-50. However, there is no convincing evidence that
further epirubicin dose escalations substantially improve responseFirst-line chemotherapy achieves an objective tumor responserates.[44]in 40–60% patients with a median response duration of 6–12
months. Although there have been no randomized studies to assess Combination anthracycline chemotherapy is, however, fre-palliative chemotherapy against best supportive care, retrospective quently employed as adjuvant chemotherapy, based on furtherstudies in the pre-taxane era have shown that chemotherapy is incremental improvements in overall survival compared with non-probably associated with only 9–12 months gain in survival.[35] anthracycline-based chemotherapy.[4] Thus, anthracyclines areNevertheless, it is widely accepted that those patients who obtain limited in their use, both in terms of efficacy and the risk ofan objective response (CR + PR) to chemotherapy are more likely cumulative cardiac toxicity, as first-line metastatic treatment. Into have significant relief of their symptoms.[36] Unfortunately only the subgroup of patients that have progressed on an anthracycline-a small fraction of patients obtain a CR, and, of these, less than based combination, either as first-line therapy for metastatic dis-20% are maintained beyond 5 years.[3] In addition, different com- ease or after having relapsed within a few months of adjuvantbination regimens of additional chemotherapy immediately fol- chemotherapy, the response rates to further conventional chemo-lowing a patient’s best response to an induction chemotherapy therapy have been poor (<20–30%) with median durations ofregimen, in the pre-taxane era did not improve overall survi- response of only 3–6 months.[45] There has been an urgent need,val.[37-39] It has not been proven whether single agent chemothera- therefore, to find novel cytotoxic agents which are effective fol-py or combination chemotherapy is preferable for first-line treat- lowing prior anthracycline exposure.ment, and treatment decisions are based primarily on which prior
2.2 Taxanestherapies an individual patient has received, the disease or treat-ment free-interval since prior therapy, the patient’s clinical condi-
The taxanes – paclitaxel and docetaxel – promote the formationtion and the likely toxicities of any given therapy. Likewiseof stable microtubules that resist depolymerization during cellcombinations of chemotherapy and hormone therapy have notdivision, leading to cell cycle arrest at the G2/M phase of the cellshown an overall survival advantage as first-line treatment ofcycle. They were introduced in the mid 1990s after a period of 15metastatic breast cancer over the sequential use of these agents.[40]
years in which little progress had been made in development ofnovel cytotoxic agents for breast cancer. Several randomized
2.1 Anthracyclines phase III trials have evaluated the efficacy of these drugs assecond-line therapy, particularly in those patients with anthra-
The anthracyclines, doxorubicin and epirubicin, inhibit RNA cycline-resistant disease. Docetaxel had a significantly higherand protein synthesis and interfere with DNA replication and response rate and TTP when compared with methotrexate/transcription. In addition, they generate cytotoxic-free radicals, fluorouracil[46] and additional overall survival benefit when com-which block DNA cleavage by topoisomerase II and inhibit heli- pared with mitomycin/vinblastine.[47] However, in a third trial,case activity. Doxorubicin is one of the most active and widely response rates were not significantly different for docetaxel com-employed cytotoxic drugs in metastatic breast cancer. It has re- pared with the combination of vinorelbine and fluorouracil assponse rates of 40% as a single agent while anthracycline combi- second-line treatment.[48] Overall, this level of activity in patientsnations, such as doxorubicin and cyclophosphamide (AC), and who had received or progressed on previous anthracycline chemo-fluorouracil, doxorubicin and cyclophosphamide (FAC), have therapy was impressive, and led to the rapid introduction offirst-line response rates of 50–60%. Epirubicin is an anthracycline taxanes for metastatic breast cancer in this setting.analogue that has similar efficacy but less toxicity than dox-orubicin at equipotent therapeutic doses.[41]
2.3 Taxanes as Single Agent First-Line ChemotherapyIn a randomized study comparing the fluorouracil, epirubicin
and cyclophosphamide (FEC) and FAC regimens, FEC had Several studies have looked at taxanes for metastatic breastequivalent response rates, TTP, and survival, but less gastrointesti- cancer in those patients who have not previously received annal, hematological, and cardiac toxicities.[42] The same group also anthracycline in the adjuvant setting (table III). In a randomized
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

102 Assersohn & Johnston
Table III. Randomzied controlled trials of single agent taxanes (docetaxel or paclitaxel) versus anthracyclines in first-line treatment of metastatic breastcancer
Investigator n Treatment (dose [mg/m2]) Response rate (%) Median time to Median overall survivalprogression (wk) (mo)
Chan et al.[49] 326 Docetaxel (100) 47.8a 26a 15.0
Doxorubicin (75) 33.3 21 14.0
Sledge et al.[50] 739 Paclitaxel (175) 33 26 22.2
Doxorubicin (60) 34 27 20.1
Paclitaxel (150) + doxorubicin (50) 46a 35a 22.4
Paridaens et al.[51] 331 Paclitaxel (200) 25 17 15.6
Doxorubicin (75) 41a 32a 18.3
Bishop et al.[52] 209 Paclitaxel (200) 29 23 17.3a
CMFP 35 28 13.9
a p < 0.05 vs comparator.
CMFP = cyclophosphamide/methotrexate/fluorouracil/prednisolone; n = number of patients.
study comparing docetaxel (100 mg/m2) to doxorubicin (75 mg/ median progression free survival (32 vs 17 weeks, respectively).m2), superior response rates (47.8 vs 33.3%, p < 0.008, respective- There was a significantly higher incidence of grade 4 neutropenia,ly) and TTP (26 vs 21 weeks, not significant) were seen for febrile neutropenia, vomiting, and stomatitis, in patients treateddocetaxel.[49] All 326 patients had previously progressed on an with doxorubicin, and significantly higher grade 3 or 4 sensoryalkylating-containing regimen, although 70% of patients received neurotoxicity in patients treated with paclitaxel. Finally, a thirddocetaxel or doxorubicin as second-line therapy for metastatic multicenter study conducted by the Eastern Cooperative Oncologybreast cancer, having received an alkylating-containing regimen as Group (ECOG) involved a three-arm randomization between dox-first-line treatment for metastatic breast cancer. The remaining orubicin (60 mg/m2), paclitaxel (175 mg/m2) and the combination30% of patients received either drug as true first-line treatment (doxorubicin 50 mg/m2 and paclitaxel 150 mg/m2) as first-linehaving relapsed more than 12 months after adjuvant alkylating metastatic breast cancer treatment in patients who had not pre-cyclophosphamide, methotrexate, and fluorouracil (CMF)-based viously received an anthracycline as adjuvant treatment[50] (tablechemotherapy. Although grade 4 neutropenia was similar in both III). Although response rates between the single arms of dox-treatment groups, the incidence of febrile neutropenia and severe orubicin and paclitaxel were similar (34 and 33%, respectively),infection was significantly higher in those treated with dox- the combination of the two was significantly superior (46%). Thisorubicin (16 vs 8%, p = 0.02). Nausea, vomiting, and stomatitis, translated into similar TTP for single agent doxorubicin andoccurred more frequently in the doxorubicin group while diarrhea, paclitaxel (27 and 26 weeks, respectively) but significantly superi-skin toxicity, nail changes, allergy, and neurotoxicity, were more or TTP for the combination arm (35 weeks). Overall survival,frequently seen in those treated with docetaxel. however, was similar for the three arms (doxorubicin 20.1 months,
paclitaxel 22.2 months, and combination 22.4 months), thus dem-Paclitaxel was compared with a non-anthracycline-based regi-onstrating that sequential monotherapy does not compromise sur-men, cyclophosphamide, methotrexate, fluorouracil andvival compared with combination anthracycline-taxane chemo-prednisolone (CMFP), in previously untreated metastatic breasttherapy.cancer patients as first-line therapy.[52] Although response rates
and median TTP were similar, on multivariate analysis, overall Both paclitaxel and docetaxel may also be administered accord-survival was significantly improved for patients treated with ing to a weekly schedule in an attempt to reduce toxicity. Althoughpaclitaxel (table III). A multicenter study conducted by the Euro- possibly better tolerated than the 3-weekly schedule in terms ofpean Organization for Research and Treatment of Cancer myelosuppression and hypersensitivity reactions, based on non-(EORTC) randomized more than 300 patients to paclitaxel or randomized comparisons, the dose-limiting toxicity for weeklydoxorubicin therapy.[51] It permitted crossover to the alternate taxanes, especially paclitaxel, is peripheral neuropathy. Dose-therapy after progression on the initial chemotherapy. Dox- limiting toxicities for weekly docetaxel are particularly asthenia,orubicin (75 mg/m2) was significantly superior to paclitaxel (200 edema, and onycholysis. From phase II trial data, it appears thatmg/m2) in terms of response rate (41 vs 25%, respectively) and clinical efficacy is maintained with dosage schedules of paclitaxel
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)
Postmenopausal Metastatic Breast Cancer 103
Table IV. Randomized controlled trials of anthracycline/taxane combinations as first-line treatment in metastatic breast cancer
Investigator n Treatment (dose [mg/m2])a Response rate (%) Time to progression(wk)
Jassem et al.[55] 267 Doxorubicin (50) + Paclitaxel (220) 68b 33b
FAC (500,50,500) 55 25
Biganzoli et al.[56] 275 Doxorubicin (60) + Paclitaxel (175) 63 ND
Doxorubicin (60) + Cyclophosphamide (600) ND ND
Luck et al.[57] 560 Epirubicin (60) + Paclitaxel (175) 46 39
Epirubicin (60) + Cyclophosphamide (600) 41 33
Carmichael[58] 705 Epirubicin (75) + Paclitaxel (200) 67 26
Epirubicin (75) + Cyclophosphamide (600) 56 27
Nabholtz et al.[59] 429 Doxorubicin (50) + Docetaxel (75) 60b 37b
Doxorubicin (60) + Cyclophosphamide (600) 47 32
Mackey et al.[60] 484 Docetaxel (75), Doxorubicin (50) + Cyclophosphamide 55b 31(500)
FAC (500, 50, 500) 44 29
a All chemotherapy given on day 1, except for Jassem et al.[55] in which doxorubicin and paclitaxel were administered on days 1 and 2, respectively.
b p < 0.05 vs comparator.
FAC = fluorouracil/doxorubicin/cyclophosphamide; n = number of patients; ND = no data.
(75–80 mg/m2/week) and docetaxel (35–40 mg/m2/week).[53,54] nificant improvement in response rate[56-58] (table IV). There wereThe results of randomized controlled trials for these new schedules differences in dose and schedule of paclitaxel between theseare awaited. studies, which may account for the differences, and the optimal
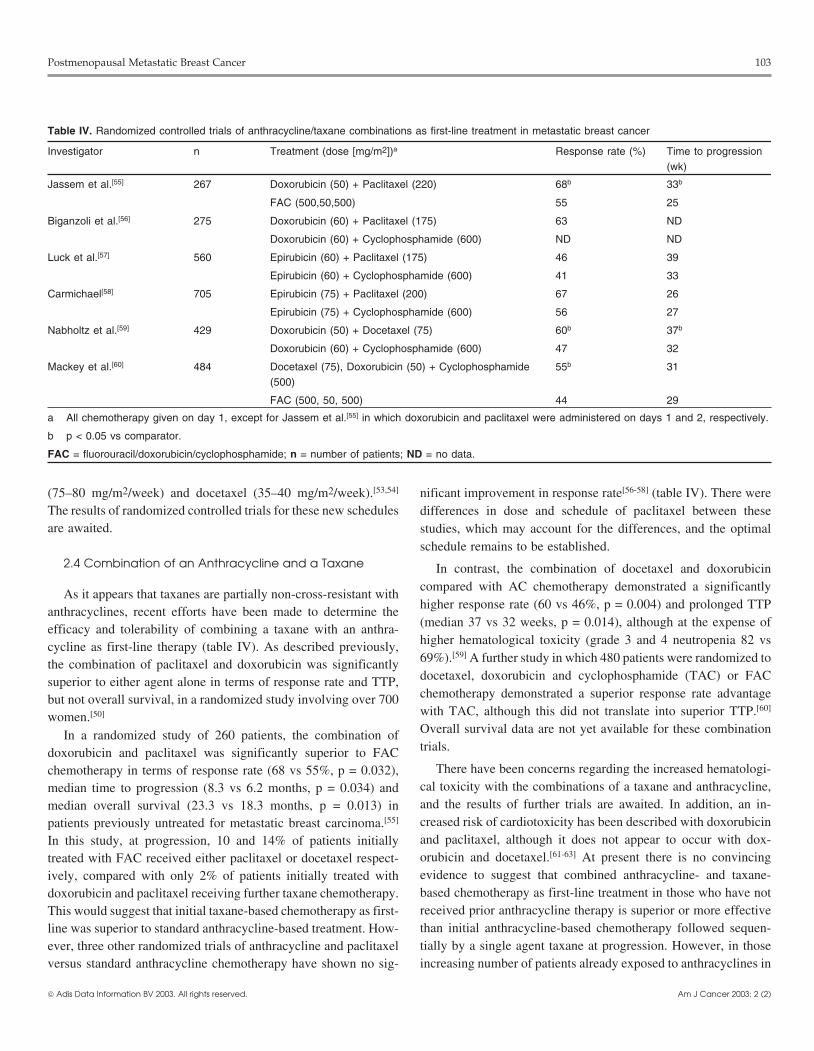
schedule remains to be established.2.4 Combination of an Anthracycline and a Taxane In contrast, the combination of docetaxel and doxorubicin
compared with AC chemotherapy demonstrated a significantlyAs it appears that taxanes are partially non-cross-resistant with
higher response rate (60 vs 46%, p = 0.004) and prolonged TTPanthracyclines, recent efforts have been made to determine the
(median 37 vs 32 weeks, p = 0.014), although at the expense ofefficacy and tolerability of combining a taxane with an anthra-higher hematological toxicity (grade 3 and 4 neutropenia 82 vscycline as first-line therapy (table IV). As described previously,69%).[59] A further study in which 480 patients were randomized tothe combination of paclitaxel and doxorubicin was significantlydocetaxel, doxorubicin and cyclophosphamide (TAC) or FACsuperior to either agent alone in terms of response rate and TTP,chemotherapy demonstrated a superior response rate advantagebut not overall survival, in a randomized study involving over 700with TAC, although this did not translate into superior TTP.[60]
women.[50]
Overall survival data are not yet available for these combinationIn a randomized study of 260 patients, the combination oftrials.doxorubicin and paclitaxel was significantly superior to FAC
There have been concerns regarding the increased hematologi-chemotherapy in terms of response rate (68 vs 55%, p = 0.032),cal toxicity with the combinations of a taxane and anthracycline,median time to progression (8.3 vs 6.2 months, p = 0.034) andand the results of further trials are awaited. In addition, an in-median overall survival (23.3 vs 18.3 months, p = 0.013) increased risk of cardiotoxicity has been described with doxorubicinpatients previously untreated for metastatic breast carcinoma.[55]
and paclitaxel, although it does not appear to occur with dox-In this study, at progression, 10 and 14% of patients initiallyorubicin and docetaxel.[61-63] At present there is no convincingtreated with FAC received either paclitaxel or docetaxel respect-evidence to suggest that combined anthracycline- and taxane-ively, compared with only 2% of patients initially treated withbased chemotherapy as first-line treatment in those who have notdoxorubicin and paclitaxel receiving further taxane chemotherapy.received prior anthracycline therapy is superior or more effectiveThis would suggest that initial taxane-based chemotherapy as first-than initial anthracycline-based chemotherapy followed sequen-line was superior to standard anthracycline-based treatment. How-tially by a single agent taxane at progression. However, in thoseever, three other randomized trials of anthracycline and paclitaxelincreasing number of patients already exposed to anthracyclines inversus standard anthracycline chemotherapy have shown no sig-
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

104 Assersohn & Johnston
the adjuvant setting, taxanes are now the chemotherapy drug of nal toxicity, although the dose-limiting toxicity is neutropenia.choice for first-line metastatic breast cancer. Likewise, unlike the earlier vinca alkaloid vincristine, vinorelbine
causes minimal peripheral neuropathy. Response rates of 20–40%have been reported with vinorelbine used as a single agent (25–35
2.5 Other Chemotherapy Agents mg/m2 day 1 and 8 every 3 weeks) in patients who had progressedon anthracycline and taxane treatment.[70,71] In a small random-ized, controlled trial which compared vinorelbine versusAt present, there are several studies investigating the combina-
tion of a taxane and anthracycline as adjuvant chemotherapy in melphalan in women who had received prior anthracyclines, vi-early breast cancer.[64,65] With increasing utilization of these agents norelbine was associated with a higher response rate.[72] Morein the adjuvant setting, the need to identify new non-cross-resistant recently, vinorelbine has been found to be effective when given inalternative chemotherapy agents for use in the metastatic setting combination with fluorouracil, either as a 5-day regimen or as ahas become more important. The fluoropyrimidine, fluorouracil, continuous infusion. This regimen appears to have high levels ofhas been widely used in patients with breast cancer for several activity of 50–60% in those pretreated with anthracyclines/tax-decades. Several oral fluorouracil compounds have recently been anes, and an oral-based combination of vinorelbine and/ordeveloped. Capecitabine is the first to be approved by the Food capecitabine is being proposed as a viable new treatment optionand Drug Administration (FDA) in US for the treatment of patients for these pretreated patients.with metastatic breast cancer who have previously received an-
Gemcitabine is a nucleoside analogue that has been investigat-thracycline and taxane treatment.
ed within phase II studies in metastatic breast cancer patients whoIn one phase II study in which 147 women had progressed on
have previously received an anthracycline although no phase IIIprior anthracycline and paclitaxel treatment, capecitabine (2510
data exists as yet. In a phase II study involving 43 patientsmg/m2/day in 2 divided doses for 14 days, every 3 weeks) pro-
receiving gemcitabine as second-line treatment (1200 mg/m2duced a response rate of 20%, with a median duration of response
weekly for 3 weeks, followed by a 1 week rest), overall responseof 8.1 months and overall survival of 12.8 months.[66] The drug israte was 28% and treatment-limiting toxicity was asthenia withwell tolerated, and the most frequent toxicities include plantargrade 4 neutropenia in 5% of patients.[73] A further trial evaluatedpalmar erythema, diarrhea, and mucositis. A further study random-gemcitabine (1250 mg/m2 weekly for 3 weeks, followed by a 1ized 95 postmenopausal women within a phase II study to cyclo-week rest) as second- (n = 6) and third-line (n = 18) treatment.[74]
phosphamide 600 mg/m2, methotrexate 40 mg/m2, andResponse rates were 33 and 6% and the incidence of grade 3/4fluorouracil 600 mg/m2 (CMF) or capecitabine (1255 mg/m2 twiceleukopenia was 66 and 22% in patients receiving gemcitabine asdaily for 2 out of 3 weeks) as first-line chemotherapy for patientssecond- and third-line treatment, respectively. Further studies arewith metastatic breast cancer. Although the overall response raterequired to determine the role of gemcitabine in patients withwas 30% (95% confidence interval [CI] 19–43%) for capecitabinemetastatic breast cancer.and 16% (95% CI 5–33%) for CMF, there was no significant
difference in time to disease progression (4.1 months withcapecitabine vs 3.0 months with CMF).[67] This study has been
2.6 High-Dose Chemotherapycriticized, however, as the 3-weekly CMF regimen was employed,which has previously been shown to be inferior to the ‘classical’
Peripheral blood stem-cell harvesting has allowed chemothera-4-weekly CMF regimen.[68] However, a further large, phase IIpy of greater than 5-fold increase in dose intensity to be delivered.study in which 126 patients, who had previously received anthra-Although initial phase II trials reported high response rates usingcycline and taxane chemotherapy, were treated with capecitabinethis approach, patient selection was a confounding factor in the(1250 mg/m2 twice daily for 2 out of 3 weeks) demonstrated aninterpretation of its true efficacy.[75] Recently, two large random-objective response rate of 29% with TTP of 4.6 months.[69] There-ized studies in metastatic breast cancer were reported. They didfore, as an oral-based chemotherapy, capecitabine may have anot demonstrate a survival advantage for high-dose chemotherapyuseful role in the management of metastatic breast cancer.with hematopoietic stem cell support as first-line treatment forA novel vinca alkaloid, vinorelbine, has demonstrated activitymetastatic breast cancer compared with conventional maintenancein patients with metastatic breast cancer. Although it is a cellchemotherapy.[76-78] Therefore, the use of high-dose chemotherapycycle-specific microtubule inhibitor, it contrasts with taxanes inwith stem cell support in this setting is not recommended outsidethat it destabilizes the microtubules. In addition, it has a goodthe context of a clinical trial.toxicity profile with a low incidence of alopecia and gastrointesti-
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

Postmenopausal Metastatic Breast Cancer 105
3. Bisphosphonates apy have been published, and may help identify those who willbenefit most.[84,85]
The use of bisphosphonates represents a major therapeuticUp to 50% of women who develop metastatic breast canceradvance in the management of skeletal morbidity caused by meta-present with bone metastases, sometimes as the only site ofstatic breast cancer. IV bisphosphonates are more effective indisease. Such patients frequently have indolent disease and mayrelieving bone pain than oral treatment.[86] Likewise, they maysurvive for many years. Bisphosphonates, such as oral clodronateprevent new bone metastases and decrease the frequency of patho-and intravenous (IV) pamidronate, are bone-specific palliativelogical fractures. At present, randomized trials are being per-treatments that inhibit tumor-related osteoclast-induced bone re-formed in the adjuvant setting to determine whether or not bis-sorption. Four randomized, double-blind, placebo-controlled trialsphosphonates may delay or prevent bone metastases in womenhave demonstrated that in breast cancer patients with predom-diagnosed with early breast cancer.inantly lytic bony metastases, bisphosphonates can improve quali-
ty of life by reducing bone pain and reducing the incidence of4. Novel Biological Therapiesskeletal complications such as fracture, spinal cord compression,
and hypercalcaemia, together with the need for radiotherapy.[79-82]The major limitations of conventional endocrine and chemo-
In an initial study of 173 patients, oral clodronate (1600 mg/ therapy in advanced breast cancer are intrinsic and acquired resis-day) compared with placebo significantly reduced the number of tance. Novel biological therapies are being developed to targethypercalcemic episodes (28 vs 52, p < 0.01) and the incidence of different components of the internal signal transduction pathway.vertebral fractures (84 vs 124 per 100 patients years, p < 0.025).[79]
Although such therapies may circumvent drug resistance, theA further study involving 382 women with at least one lytic bone greater opportunity may lie in the setting of minimal residuallesion, compared IV pamidronate (90mg as 2-hour infusion every disease for which trials of maintenance therapy following chemo-4 weeks for 1 year) with placebo infusion, in conjunction with therapy-induced remission are required to assess whether thesechemoendocrine therapy.[81] Patients treated with pamidronate had agents can prolong time to disease progression. The most promis-significantly longer time to first skeletal complication (median ing targets have come from our increased understanding of breast13.1 vs 7.0 months, p = 0.005) and fewer of them developed such cancer biology, and include growth factor receptors and theircomplications (43 vs 56%, p = 0.008). The mean number of ligands (epidermal growth factor receptor [EGFR], HER2/neu),skeletal-related events per year was 2.1 in the pamidronate group intracellular signal transduction pathways and protein kinasescompared with 3.3 in the placebo group (p < 0.005). Two other involved in cell cycle regulation. The first such therapy to demon-studies with IV pamidronate demonstrated similar significant re- strate clinical efficacy and reach the clinic is the monoclonalduction of skeletal complications and palliation of symptoms, in antibody directed against HER2/neu, trastuzumab.particular bone pain.[80,83] These two studies have recently beencombined and published with a longer follow-up.[82] Seven hun- 4.1 Trastuzumabdred and fifty-four patients received 24 cycles of IV pamidronateor placebo every 3–4 weeks in addition to hormone therapy or Trastuzumab is a humanized monoclonal antibody that binds tochemotherapy. the cell surface growth factor receptor HER2/neu (also known as
c-erb-B2). Approximately 25–30% of breast cancers over-expressHowever, none of these studies have demonstrated an impactHER2/neu protein due to gene amplification. HER2/neu overex-on overall survival. Similar trials employing IV clodronate havepression is associated with an adverse prognosis and relativenot been performed in patients with metastatic breast cancer, andresistance to conventional therapies such as endocrine treatment orthe optimal dosage and duration of treatment is unknown. In spitechemotherapy.[87] The administration of trastuzumab, either aloneof this, there is little doubt that the use of these drugs in conjunc-or in conjunction with conventional chemotherapy treatment, of-tion with other systemic treatments (chemotherapy or endocrinefers the opportunity of modulating aberrant growth factor activitytherapy) in metastatic breast cancer patients, in whom osteolyticin tumors from patients with resistant disease.bone metastases are present, significantly reduces skeletal related
morbidity. The use of bisphosphonates should not necessarily be In initial phase II studies with metastatic breast cancer patients,stopped when metastatic bone disease progresses as these agents trastuzumab as monotherapy was well-tolerated and demonstratedare best employed on a long-term basis to reduce the complica- clinical effect with duration of response between 5.1 and 9.1tions of such disease. Specific guidelines on the use of these agents months.[88-90] In a study of 222 women who had received prioras palliative treatment in women with metastatic breast cancer anthracycline/taxane chemotherapy, an objective response rate ofwho may or may not be receiving endocrine therapy or chemother- 15% was seen with a median response duration of 9.1 months.[90]
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)

106 Assersohn & Johnston
In a more recent randomized study of trastuzumab in two dosage preclinical studies suggested that, when given in combination withschedules given as first-line monotherapy for metastatic breast several different cytotoxic drugs including taxanes and anthra-cancer in 114 patients, an objective response rate of 26% was seen cyclines, ZD-1839 enhanced their antitumor activity.[95] This inter-with median response duration of 9 months, with no difference action did not always appear to be dependent on overexpression ofbetween the two dosage schedules.[91] Response rates in 111 EGFR, and the mechanism of any enhanced cytotoxic effect withassessable patients with HER2 overexpression (ie 3+ or 2+ stain- chemotherapy remains unclear.ing detected by immunohistochemistry) were 35% (95% CI Recent evidence also suggested that peptide growth factor24.4–44.7%) and none (95% CI 0–15.5%), respectively. As mono- receptors such as EGFR or HER2 become up-regulated/activatedtherapy, the drug was extremely well tolerated with minimal in endocrine resistant breast cancer,[96,97] and experiments demon-toxicity, although it does require weekly IV administration until strated that an EGFR-TK inhibitor such as ZD-1839 may treat, ordisease progression. This latter study suggested that maximal perhaps even prevent, endocrine-resistance in breast cancerbenefit may be found in HER 3+, one expression for trastuzumab; cells.[98,99] Clinical trials are now being undertaken in breast canceras first-line treatment, although randomized controlled trials are with EGFR-TK inhibitors.urgently required to compare this approach to conventional treat-
4.3 Farnesyl Transferase Inhibitorsment options. Nevertheless, for a subgroup of patients with moreaggressive ‘resistant’ disease, trastuzumab represents a significant
A key component of the signal transduction pathway is the Rasnew treatment option.protein, which becomes attached to the inner plasma membrane,In a randomized study of first-line treatment in HER-2/neuthus providing a link between activated transmembrane growthover-expressing metastatic breast cancer, 469 women were treatedfactors and downstream intracellular kinases which ultimatelywith AC chemotherapy or paclitaxel every 3 weeks for 6 cyclestrigger cell growth. Ras functions as a relay switch whose activitywith and without trastuzumab.[92] Overall, the addition of tras-is dependent upon the enzyme farnesyl transferase. Specific inhib-tuzumab to chemotherapy increased response rate (50 vs 32%, p <itors of farnesyl transferase (FTIs) were initially developed to0.001), duration of response (median 9.1 vs 6.1 months, p < 0001),prevent the post-translational processing of Ras, thereby inhibitingTTP (7.4 vs 4.6 months, p < 0.001) and overall survival (median,cell growth. Breast carcinomas are known to contain a very low25.1 vs 20.3 months, p = 0.046). Addition of trastuzumab to thefrequency of Ras mutations (<2%), although aberrant function ofAC regimen increased TTP from 6.1 to 7.8 months (p < 0.001) andthe Ras signal transduction pathway is thought to be common inaddition of trastuzumab to paclitaxel increased the TTP from 3.0human breast cancer, due to permanent upstream growth factorto 6.9 months (p < 0.001). The most important adverse event ofactivation.[100] A phase II clinical study of R115777 in 41 womentrastuzumab was cardiac dysfunction when given concurrentlywith advanced breast cancer demonstrated clinical activity for anwith AC chemotherapy (27% of patients) and it will, therefore, beFTI, including 4 partial responses seen in sites of visceral and softimportant to explore combinations of trastuzumab with chemo-tissue disease, together with prolonged stable disease in an addi-therapy that is devoid of cardiotoxicity.[93] The impact on survivaltional 6 patients.[101] The drug was well tolerated, although dose-is particularly impressive given that a high percentage of womenrelated myelosuppression was the most frequent drug-related tox-on the chemotherapy alone arm crossed over to trastuzumab aticity. In view of preclinical data suggesting synergy with conven-progression, and this reinforces the view that the early introductiontional cytotoxic agents, studies are now examining how FTIs canin first-line treatment may be the most effective use of thisbe combined with either cytotoxic or endocrine therapies fortreatment.breast cancer.
4.2 Tyrosine Kinase Inhibitors 5. Conclusion
Several inhibitors of EGFR tyrosine kinase (EGFR-TK) are in Endocrine therapy represents the mainstay of first-line treat-development. These include ZD-1839 (Iressa™), an orally active ment of postmenopausal women with ER- and/or PgR-positivelow molecular weight synthetic anilinoquinazoline that is a potent metastatic breast cancer who do not have life-threatening visceraland selective inhibitor of EGFR-TK. In experimental models, involvement. The role of chemotherapy as first-line treatment forincluding human breast cancer cells, ZD-1839 given as a single women in whom rapid tumor control is required, such as thoseagent induced a dose-dependent antiproliferative effect that with extensive or symptomatic visceral involvement, or for wo-delayed tumor growth.[94] The effect appears to be cytostatic, as men in whom the tumor is ER- and PgR-negative or hormone-following drug withdrawal tumor growth continued. Additional refractory metastatic breast cancer, is widely accepted.
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)
Postmenopausal Metastatic Breast Cancer 107
13. Osbourne CK, Pippen J, Jones SE, et al. Double-blind randomized trial comparingSeveral new therapies have been developed for treatment ofthe efficacy and tolerability of fulvestrant versus anastrozole in post-menopaus-
patients with metastatic breast cancer in recent years, including al women with advanced breast cancer progressing after prior endocrine ther-apy. J Clin Oncol 2002; 16: 3386-95potent third-generation aromatase inhibitors, taxanes for use as
14. Johnston S. Endocrine manipulation in advanced breast cancer: recent advanceschemotherapy treatment in anthracycline pretreated disease andwith SERM therapies. Clin Cancer Res 2001; 7 Suppl. 1: 4376s-87s
bisphosphonates for the palliative treatment of bone metastases. 15. Gradishar W, Glusman J, Vogel C, et al. Raloxifene HCL, a new endocrine agent,is active in estrogen receptor positive (ER+) metastatic breast cancer. BreastWell conducted randomized, controlled clinical trials have demon-Cancer Res Treat 1997; 46: 53
strated that these represent a significant incremental improvement16. Cummings S, Eckert S, Krueger K, et al. The effect of raloxifene on risk of breast
in the treatment of patients with metastatic breast cancer. cancer in postmenopausal women: results from the multiple outcomes ofraloxifene evaluation (MORE) randomized trial. JAMA 1999; 281: 2189-97Nevertheless, the problem of the development of drug resis-
17. Fisher B, Costantino J, Wickerham D, et al. Tamoxifen for prevention of breasttance persists. As a result of the expanded biological understand- cancer: report of the National Surgical Adjuvant Breast and Bowel Project P-1
study. J Natl Cancer Inst 1998; 90 (18): 1371-88ing of tumor development and progression, the development of18. Brodie A, Njar V. Aromatase inhibitors and breast cancer. Semin Oncol 1996; 23novel therapeutic agents continues. Trastuzumab heralds the new
(4 Suppl. 9): 10-20era of biological therapy and could represent the first of several 19. Miller WR. Aromatase inhibitors. Endocr Relat Cancer 1996; 3 (1): 65-79targeted therapies that will be utilized to enhance the efficacy of 20. Geisler J, Haynes B, Anker G, et al. Influence of letrozole and anastrozole on total
body aromatization and plasma estrogen levels in postmenopausal breast cancerexisting treatment options. It is expected that the new generationpatients evaluated in a randomized, cross-over study. J Clin Oncol 2002: 20;
of biological agents, either alone or in conjunction with standard 751-57
21. Buzdar A, Jonat W, Howell A, et al. Anastrozole, a potent and selective aromatasetherapies, could provide a further significant impact on futureinhibitor, versus megestrol acetate in post-menopausal women with advancedtreatment options, thus giving new hope to the thousands ofbreast cancer: results of overview analysis of 2 phase III trials. J Clin Oncol
women who will continue to develop and die from metastatic 1996; 14: 2000-11
22. Buzdar A, Jonat W, Howell A, et al. Anastrozole vs megestrol acetate in thebreast cancer.treatment of postmenopausal women with advanced breast carcinoma: resultsof a survival update based on a combined analysis of data from two maturephase III trials. Cancer 1998; 83: 1142-52Acknowledgements
23. Dombernowsky P, Smith I, Falkson G, et al. Letrozole, a new oral aromataseinhibitor for advanced breast cancer: double-blind randomized trial showing aThe author has received funding from the Jansen Research Foundation,dose effect and improved efficacy and tolerability compared with megestrolAstraZenica and Novatis.acetate. J Clin Oncol 1998; 16 (2): 453-61
24. Buzdar A, Douma J, Davidson N, et al. Phase III, multicenter, double-blind,randomized study of letrozole, an aromatase inhibitor, for advanced breastReferencescancer versus megestrol acetate. J Clin Oncol 2001; 19 (14): 3357-66
1. Office for National Statistics. Mortality statistics: review of the Register General25. Kvinnsland S, Anker G, Dirix L, et al. High activity and tolerability demonstratedon deaths by sex and age, England and Wales, 1999. London: The Stationery
for exemestane in postmenopausal women with metastatic breast cancer whoOffice, 2000had previously failed on tamoxifen treatment. Eur J Cancer 2000; 36: 976-822. Cancer Research Campaign. Cancer Research Campaign, CRC Cancer Stats;
26. Lonning P, Bajetta E, Murray R, et al. Activity of exemestane in metastatic breastMortality UK, London. Available from URL: http://www.crc.org.uk/cancer/cancer after failure of nonsteroidal aromatase inhibitors: a phase II trial. J Clinpageimages/csmortality.pdf [Accessed 2002 Jul 19]Oncol 2000; 18 (11): 2234-443. Greenberg P, Hortobagyi G, Smith T, et al. Long-term follow-up of patients with
27. Thurlimann B, Paridaens R, Serin D, et al. Third-line hormonal treatment withcomplete remission following combination chemotherapy for metastatic breastexemestane in postmenopausal patients with advanced breast cancer progress-cancer. J Clin Oncol 1996; 14: 2197-205ing on aminoglutethimide: a phase II multicentre multinational study: Exemes-4. Early Breast Cancer Trialists’ Collaborative Group. Polychemotherapy for earlytane Study Group. Eur J Cancer 1997; 33 (11): 1767-73breast cancer: an overview of the randomised trials. Lancet 1998; 352: 930-42
28. Kaufmann M, Bajetta E, Dirix L, et al. Exemestane is superior to megestrol acetate5. Early Breast Cancer Trialists’ Collaborative Group. Tamoxifen for early breastafter tamoxifen failure in postmenopausal women with advanced breast cancer:cancer: an overview of the randomised trials. Lancet 1998; 351: 1451-67results of a phase III randomized double-blind trial. J Clin Oncol 2000; 18 (7):6. Rubens R, Bajetta E, Bonneterre J, et al. Treatment of relapse of breast cancer after1399-411adjuvant systemic therapy. Eur J Cancer 1994; 30A: 106-11
29. Nabholtz J, Buzdar A, Pollak M, et al. Anastrozole is superior to tamoxifen as first-7. Encarnacion C, Ciocca D, McGuire W, et al. Measurement of steroid hormoneline therapy for advanced breast cancer in postmenopausal women: results of areceptors in breast cancer patients on tamoxifen. Breast Cancer Res Treat 1993;North American multicenter randomized trial. J Clin Oncol 2000; 18 (22):26: 237-463758-678. Johnston SR, Saccani Jotti G, Smith IE, et al. Changes in estrogen receptor,
30. Bonneterre J, Thurlimann B, Robertson J, et al. Anastrozole versus tamoxifen asprogesterone receptor, and pS2 expression in tamoxifen-resistant human breastfirst-line therapy for advanced breast cancer in 668 postmenopausal women:cancer. Cancer Res 1995; 55 (15): 3331-8results of the tamoxifen or Arimidex randomized group efficacy and tolerability9. Goldhirsch A. Breast cancer. In: Cavalli F, Hansen H, Kaye S, editors. Textbook ofstudy. J Clin Oncol 2000; 18 (22): 3748-57medical oncology. London: Martin Dunitz, 1997: 53-87
31. Mouridsen H, Gershanovich M, Sun Y, et al. Superior efficacy of letrozole versus10. Johnston SRD. Acquired tamoxifen resistance in human breast cancer: potentialtamoxifen as first-line therapy for postmenopausal women with advancedmechanisms and clinical implications. Anticancer Drugs 1997; 8 (10): 911-30breast cancer: results of a phase III study of the International Letrozole Breast11. Howell A, DeFriend D, Robertson J, et al. Response to a specific antioestrogenCancer Group. J Clin Oncol 2001; 19 (10): 2596-606(ICI 182780) in tamoxifen-resistant breast cancer. Lancet 1995; 345: 29-30
12. Howell A, Robertson JRF, Albano J, et al. Fulvestrant is as effective as anastrozole 32. Dirix L, Piccart M, Lohrisch C, et al. Efficacy of and tolerance to exemestanein post-menopausal women with advanced breast cancerprogressing after prior versus tamoxifen in first line hormone therapy of postmenopausal metastatictreatment. J Clin Oncol 2002; 16: 3396-402 breast cancer patients: a European Organisation for the Research and Treatment
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)
108 Assersohn & Johnston
of cancer (EORTC Breast Group) Phase II trial with Pharmacia and Upjohn. 53. Perez EA, Vogel CL, Irwin DH, Krishner JJ, Patel R. Multicenter Phase II trial ofProc Am Soc Clin Oncol 2001; 20: 114a weekly paclitaxel in women with metastatic breast cancer. J Clin Oncol 2001;
18: 4216-3333. Buzdar A, Nabholtz J, Robertson J, et al. Anastrozole (Arimidex) versus tamoxifenas first-line therapy for advanced breast cancer (ABC) in postmenopausal (PM) 54. Burstein H, Manola J, Younger J, et al. Docetaxel administered on a weekly basiswomen – combined analysis from two identically designed multicenter trials for metastatic breast cancer. J Clin Oncol 2000; 19: 1212-9[abstract 609D]. Proc Am Soc Clin Oncol 2000; 19: 154A 55. Jassem J, Pienkowski T, Pluzanska A, et al. Doxorubicin and paclitaxel versus
34. ATAC Trialists’ Group. Anastrozole alone or in combination with tamoxifen fluorouracil, doxorubicin, and cyclophopshamide as first-line therapy for wo-versus tamoxifen alone for adjuvant treatment of postmenopausal women with men with metastatic breast cancer: final results of a randomized phase IIIearly breast cancer: first results of the ATAC Randomised Trial. Lancet 2002; multicenter trial. J Clin Oncol 2001; 19 (6): 1707-15359: 2131-9 56. Biganzoli L, Cufer T, Bruning P, et al. Doxorubicin and paclitaxel versus
35. Cold S, Jensen N, Brincker H. The influence of chemotherapy on survival after doxorubicin and cyclophosphamide as first line chemtoherapy in metastaticrecurrence in breast cancer: a population based study of patients treated in the breast cancer: the European Organisation for Research and Treatment of cancer1950s, 1960s, and 1970s. Eur J Cancer 1993; 29: 1146-52 10961 multicenter phase III trial. J Clin Oncol 2002; 20: 3114-21
36. Geels P, Eisenhauer E, Bezjak A, et al. Palliative effect of chemotherapy: objective 57. Luck H, Thomssen C, Untch M, et al. Multicentric phase III study in first linetumor response is associated with symptom improvement in patients with treatment of advanced metastatic breast cancer (ABC): epirubicin/paclitaxelmetastatic breast cancer. J Clin Oncol 2000; 18 (12): 2395-405 (ET) vs epirubicin/cyclophosphamide (EC) – a study of the AGO Breast Cancer
Group. Proc Am Soc Clin Oncol 2000; 19: 73A37. Falkson G, Gelman R, Glick J, et al. Metastatic breast cancer: higher versus lowdose maintenance treatment when only a partial response or a no change status 58. Carmichael J. UKCCR trial of epirubicin and cyclophosphamide vs epirubicin andis obtained following doxorubicin induction treatment: an Eastern Cooperative taxolin the first line treamtnet of women with metastatic breast cancer [abstractOncology Group study. Ann Oncol 1992; 3 (9): 768-70 84a]. Proc Am Soc Clin Oncol 2001; 20: 22
38. Falkson G, Gelman R, Pandya K, et al. Eastern Cooperative Oncology Group 59. Nabholtz J-M, Falkson G, Campos D, et al. Doccetexal and doxorubicin comparedrandomized trials of observation versus maintenance therapy for patients with with doxorubicin and cyclophosphamide as first-line chemotherapy for meta-metastatic breast cancer in complete remission following induction treatment. J static breast caner; results of a randomised, multicenter phase III trial. J ClinClin Oncol 1998; 16 (5): 1669-76 Oncol 2003; 21: 968-75
39. Muss H, Case L, Richards II F, et al. Interrupted versus continuous chemotherapy 60. Mackey J, Paterson A, Dirix L, et al. Final results of the phase III randomized trialin patients with metastatic breast cancer. N Engl J Med 1991; 325 (19): 1342-8 comparing docetaxel (T), doxorubicin (A) and cyclophosphamide (C) to FAC
as first line chemotherapy for patients with metastatic breast cancer [abstract40. Perez E. Current management of metastatic breast cancer. Semin Oncol 1999; 26 (4137]. Proc Am Soc Clin Oncol 2002; 21: 35aSuppl. 12): 1-10
61. Sparano J, O’Neill A, Schaefer P, et al. Phase II trial of doxorubicin and docetaxel41. Camaggi C, Strocchi E, Carisi P. Epirubicin metabolism and pharmacokineticsplus granulocyte colony-stimultating factor in metastatic breast cancer: Easternafter conventional- and high-dose intravenous administration: a cross-overCooperative Oncology Group Study E1196. J Clin Oncol 2000; 18: 2369-77study. Cancer Chemother Pharmacol 1993; 32: 301-9
62. Sparano J, Hu P, Rao R, et al. Phase II trial of doxorubicn and paclitaxel plus42. French Epirubicin Study Group. A prospective randomized phase III trial compar-granulocyte colony-stimulating factor in metastatic breast cancer: an Easterning combination chemotherapy with cyclophosphamide, fluorouracil and withCooperative Oncology Group Study. J Clin Oncol 1999; 17: 3828-34either doxorubicin or epirubicin. J Clin Oncol 1988; 6: 679-88
63. Gianni L, Munzone E, Capri G, et al. Paclitaxel by 3-hour infusion in combination43. French Epirubicin Study Group. A prospective randomized trial comparingwith bolus doxorubicin in women with untreated metastatic breast cancer: highepirubicin monochemotherapy to two fluorouracil, cylophosphamide, andantitumor efficacy and cardiac effects in a dose-finding and sequence-findingepirubicin regimens differing in epirubicin dose in advanced breast cancerstudy. J Clin Oncol 1995; 13 (11): 2688-99patients. J Clin Oncol 1991; 9: 305-12
64. Nabholtz J, Pienkowski T, Mackey J, et al. Phase III trial comparing TAC44. Biganzoli L, Piccart M. The bigger the better? Or what we know and what we still(docetaxel, doxorubicin, cyclophosphamide) with FAC (5-fluorouracil, dox-need to learn about anthracycline dose per course, dose density and cumulativeorubicin, cyclophosphamide) in the adjuvant treatment of node positive breastdose in the treatment of breast cancer. Ann Oncol 1997; 8: 1177-82cancer aptients: interim analysis of the BCIRG 001 study [abstract 141]. Proc45. Buzdar A, Hortobagyi G, Prye D, et al. Second-line chemotherapy for metastaticAm Soc Clin Oncol 2002; 21: 36abreast cancer including quality of life issues. Breast 1996; 5: 312-7
65. Buzdar AU, Singletary SE, Valero V, et al. Evaluation of paclitaxel in adjuvant46. Sjostrom J, Blomqvist C, Mouridsen H, et al. Docetaxel compared with sequentialchemotherapy for patients with operable breast cancer; preliminary results of amethotrexate and 5-fluorouracil in advanced breast cancer after anthracyclineprospective randomised trial. Clin Cancer Res 2002; 8: 1073-9failure: a randomised phase III study with cross-over on progression by the
66. Blum J, Jones S, Buzdar A, et al. Multicenter phase II study of capecitabine inScandinavian Breast Cancer Group. Eur J Cancer 1999; 35: 1194-201paclitaxel-refractory metastatic breast cancer. J Clin Oncol 1999; 17: 485-9347. Nabholtz J, Senn J, Beswoda W, et al. Prospective randomised trial of docetaxel vs
67. O’Shaughnessy J, Blum J, Moiseyenko V, et al. Randomized, open-label, phase IImitomycin plus vinblastine in patients with metastatic breast cancer progressingtrial of oral capecitabine (Xeloda) vs a reference arm of intravenous CMFdespite previous anthracycline-containing chemotherapy. J Clin Oncol 1999;(cyclophosphamide, methotrexate and 5-fluorouracil) as first line therapy for17: 1413-24advanced/metastatic breast cancer. Ann Oncol 2001; 12 (9): 1247-5448. Bonneterre J, Roche H, Monnier A, et al. Taxotere vs 5-FU and Navelbine as
68. Engelsman E, Klijn J, Rubens R, et al. “Classical” CMF versus a 3-weeklysecond-line chemotherapy in patients wiith metastatic breast cancer. Proc Amintravenous CMF schedule in postmenopausal patients with advanced breastSoc Clin Oncol 1997; 16: A564cancer: an EORTC Breast Cancer Co-Operative Group Phase III Trial (10808).49. Chan S, Friedrichs K, Noel D, et al. Prospective randomised phase III trial ofEur J Cancer 1991; 27 (8): 966-70docetaxel vs doxorubicin in patients with metastatic breast cancer. J Clin Oncol
1999; 17: 2341-54 69. Fumoleau P, Largillier R, Trillet-Lenoir V, et al. Capecitabine (Xeloda) in patientswith advanced breast cancer, previously treated with anthracyclines and tax-50. Sledge GW, Neuberg D, Bernando P, et al. Phase III trial of doxorubicin vsanes: results of a large phase II study [abstract 247]. Proc Am Soc Clin Oncolpaclitaxel vs doxorubicin + paclitaxel as front-line chemotherapy for metastatic2002; 21: 62abreast cancer; an intergroup trial [abstract]. J Clin Oncol 2003; 21: 588-92
70. Degardin M, Bonneterre J, Hecquet B, et al. Vinorelbine (navelbine) as a salvage51. Paridaens R, Biganzoli L, Bruning P, et al. Paclitaxel vs doxorubicin as first-linetreatment for advanced breast cancer. Ann Oncol 1994; 5: 423-6single agent chemotherapy for metastatic breast cancer; a European Organisa-
tion for Research and Treatment of Cancer randomised study with cross-over. J 71. Marty M, Extra J, Dieras V, et al. A review of the antitumour activity ofClin Oncol 2000; 18: 724-33 vinorelbine in breast cancer. Drugs 1992; 44 Suppl. 4: 29-35
52. Bishop J, Dewar J, Toner G, et al. Initial paclitaxel improves outcome compared 72. Jones S, Winer E, Vogel C, et al. Randomized comparison of vinorelbine andwith CMFP combination chemotherapy as front-line therapy in untreated melphalan in anthracycline-refractory advanced breast cancer. J Clin Oncolmetastatic breast cancer. J Clin Oncol 1999; 17: 2355-64 1995; 13 (10): 2567-74
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)
Postmenopausal Metastatic Breast Cancer 109
73. Spielmann M, Kalla S, Llombart-Cussac A, et al. Activity of gemcitabine in 89. Pegram MD, Lipton A, Hayes DF, et al. Phase II study of receptor-enhancedmetastatic breast cancer patients previously treated with anthracycline-contain- chemosensitivity using recombinant humanized anti-p185HER2/neu monoclo-ing regimens. Eur J Cancer 1997; 33 Suppl. 8: A663 nal antibody plus cisplatin in patients with HER2/neu-overexpressing metastat-
74. Brodowicz T, Moslinger R, Herscovici V, et al. Second- and third-line treatent of ic breast cancer refractory to chemotherapy treatment. J Clin Oncol 1998; 16metastatic breast cancer with gemcitabine. Eur J Cancer 1998; 34 Suppl. 5: (8): 2659-71A180
90. Cobleigh M, Vogel C, Tripathy D, et al. Multinational study of the efficacy and75. Rahman Z, Frye D, Buzdar A, et al. Impact of selection process on response rate safety of humanized anti-HER2 monoclonal antibody in women who have
and long-term survival of potential high-dose chemotherapy candidates treatedHER2-overexpressiing metastatic breast cancer that has progressed after chem-with standard-dose doxorubicin-containing chemotherapy in patients with met-otherapy for metastatic disease. J Clin Oncol 1999; 17 (9): 2639-48astatic breast cancer. J Clin Oncol 1997; 15: 3171-7
91. Vogel C, Cobleigh M, Tripathy D, et al. Efficacy and safety of trastuzumab as a76. Lotz J, Cure H, Janvier M, et al. High-dose chemotherapy with haemopoieticsingle agent in first-line treatment of HER2-overexpressing metastatic breasttransplantation for metastatic breast cancer: results of the French protocol
PEGASE 04 [abstract 161]. Proc Am Soc Clin Oncol 1999; 18: 43a cancer. J Clin Oncol 2002; 20 (3): 719-26
92. Slamon J, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal77. Stadtmauer E, O’Neill A, Goldstein L, et al. Conventional-dose chemotherapycompared with high-dose chemotherapy plus autologous haematopoetic stem antibody against HER2 for metastatic breast cancer that overexpreses HER2. Ncell transplant group. N Engl J Med 2000; 342: 1069-76 Engl J Med 2001; 344: 783-92
78. Stadtmauer E, O’Neill A, Goldstein L, et al. Conventional-dose chemotherapy 93. Seidman A, Hudis C, Pierri M, et al. Cardiac dysfunction in the trastuzumabcompared with high-dose chemotherapy plus autologous stem-cell transplanta- clinical trials experience. J Clin Oncol 2002; 20 (5): 1215-21tion for metastatic breast cancer: 5-year update of the “Philadelphia Trial”
94. Ciardiello F, Caputo R, Bianco R, et al. Antitumor effect and potentiation of[abstract 169]. Proc Am Soc Clin Oncol 2002; 21: 43acytotoxic drugs activity in human cancer cells by ZD1839 (Iressa), an epider-
79. Paterson A, Powles T, Kanis J, et al. Double-blind controlled trial of oralmal growth factor receptor-selective tyrosine kinase inhibitor. Clin Cancer Resclodronate in patients with bone metastases from breast cancer. J Clin Oncol2000; 6: 2053-631993; 11: 59-65
95. Sirotnak F, Zakowski M, Miller V, et al. Efficacy of cytotoxic agents against80. Conte P, Latrielle J, Mauriac L, et al. Delay in progression of bone metastases inhuman tumor xenografts is markedly enhanced by co-administration of ZD1839breast cancer patients treated with intravenous pamidronate: results from a
multinational randomised controlled trial. J Clin Oncol 1996; 14: 2552-9 (Iressa), an inhibtor of EGFR tyrosine kinase. Clin Cancer Res 2000; 6:
4885-9281. Hortobagyi G, Theriault R, Porter L, et al. Efficacy of pamidronate in reducingskeletal complications in patients with breast cancer and lytic bone metastases. 96. Jeng M, Yue W, Eischied A, et al. Role of MAP kinase in the enhanced cellN Engl J Med 1996; 335: 1785-91 proliferation of long-term estrogen deprived human breast cancer cells. Breast
82. Lipton A, Theriault R, Hortobagyi G, et al. Pamidronate prevents skeletal Cancer Res Treat 2000; 62: 167-75complications and is effective palliative treatment in women with breast carci- 97. McClelland R, Barrow D, Madden T, et al. Enhanced epidermal growth factornoma and osteolytic bone metastases. Cancer 2000; 88: 1082-90
receptor signaling in MCF7 breast cancer cells after long-term culture in the83. Theriault R, Lipton A, Hortobagyi G, et al. Pamidronate reduces skeletal morbidity presence of the pure antiestrogen ICI 182,780 (Faslodex). Endocrinology 2001;
in women with advanced breast cancer and lytic bone lesions: a randomized,142 (7): 2776-88
placebo-controlled trial-protocol 18 Aredia Breast Cancer Study Group. J Clin98. Nicholson R, Hutcheson I, Harper M, et al. Modulation of epidermal growth factorOncol 1999; 17: 846-54
receptor in endocrine-resistant, oestrogen receptor-positive breast cancer. En-84. Breast Specialty Group of the British Association of Surgical Oncology. Thedocr Relat Cancer 2001; 8: 175-82management of metastatic bone disease in the United Kingdom. Eur J Surg
Oncol 1999; 25: 3-23 99. Gee J, Hutcheson I, Knowlden J, et al. The EGFR-selective tyrosine kinase
inhibitor ZD1839 (Iressa) is an effective inhibitor of tamoxifen-resistant breast85. Hillner B, Ingle J, Berenson J, et al. American Society of Clinical Oncologyguideline on the role of bisphosphonates in breast cancer: American Society of cancer growth. Proc Am Soc Clin Oncol 2001; 20: A282Oncology Bisphosphonates Expert Panel. J Clin Oncol 2000; 18: 1378-91 100. Clark G, Der CJ. Aberrant function of the Ras signal transduction pathway in
86. Diel I, Marschner N, Kindler M, et al. Continual oral versus intravenous interval human breast cancer. Breast Cancer Res Treat 1995; 35: 133-44therapy with bisphosphonates in patients with breast cancer and bone metasta-
101. Johnston S, Hickish T, Ellis P, et al. Clinical activity with the farnesyl transferaseses [abstract 488A]. Proc Am Soc Clin Oncol 1999; 18: 128
inhibitor R115777 in patients with advanced breast cancer: relationship with87. Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of tumour phenotype. Breast Cancer Res Treat 2000; 32: A28
relapse and survival with amplification of the HER-2/neu oncogene. Science1987; 235 (4785): 177-82
88. Baselga J, Tripathy D, Mendelsohn J, et al. Phase II study of weekly intravenous Correspondence and offprints: Dr Stephen R.D. Johnston, Breast Unit, Royalrecombinant humanized Anti-p185HER2 monoclonal antibody in patients with
Marsden Hospital, Fulham Road, London, SW3 6JJ, UK.HER2/neu-overexpressing metastatic breast cancer. J Clin Oncol 1996; 14 (3):737-44 E-mail: [email protected]
© Adis Data Information BV 2003. All rights reserved. Am J Cancer 2003; 2 (2)





























