Embed Size (px)
Citation preview

Case reports 51
Figure 1. Permanent histological section shows a mixture of
smooth muscle, thick-walled small and large blood vessels, and mature fatty tissue. Some cells have atypical nuclei and a few mitotic figures can be seen ( x 100).
general population. Moreover, renal angiomyolipoma is predominantly a disease of middle-aged women (Price and Mostofi, 1965; Farrow et al., 1968; Hajdu and Foote, 1969), whereas injury occurs predominantly to younger men. Two patients with sudden onset of symptomatology similar to our patient have had kidney injury associated with trivial injury (Price and Mostofi, 1965). Both underwent retroperi- toneal exploration and nephrectomy. Histopathological examination in each case showed a highly vascular angio- myolipoma.
The frozen section report that this tumour was malignant is not unusual. Microscopically, the increased cellularity, pleomorphism, and increased mitotic activity of the smooth muscle component may result in a mistaken diagnosis of leiomyosarcoma (Price and Mostofi, 1965; Hajdu and Foote, 1969). Gross observation of this tumour may show a strik- ing resemblance to renal cell carcinoma because of its yellow colour, intratumoural haemorrhages, and propensity for extracapsular extension. The presence of atypical histolo- gical features on frozen section leads to frequent misdiag- nosis during laparotomy. After a thorough evaluation of the
opposite kidney in patients with renal angiomyolipoma, nephrectomy is curative.
There is an association of angiomyolipoma with tuberous sclerosis (epilepsy, mental retardation, adenoma sebaceum). About 80 per cent of people with tuberous sclerosis will have a renal angiomyolipoma. However, fewer than 40 per cent of patients with angiomyolipomas have one or more of the features of the tuberous sclerosis complex, i.e. cutaneous lesions, retinal phacomas, visceral or cerebral angiomas (Farrow et al., 1968). Our patient did not have any of the features of tuberous sclerosis.
Acknowledgements The author gratefully acknowledges the assistance of Ann Peters and Gail DUMUC~ at Good Samaritan Medical Center in the preparation of this material.
References
Esho J. O., Ireland G. W. and Cass, A. S. (1973) Renal trauma and
pre-existing lesions of kidney. Urobgy 1, 134. Farrow G. M., Harrison Jr, E. G., Utz D. C. et al. (1968) Renal
angiomyolipoma. A clinicopathologic study of 32 cases. Cancer 22, 564.
Hajdu S. I., Foote Jr, F. W. (1969) Angiomyolipoma of the kidney.
Report of 27 cases and review of the literature. J Urd. 102, 396.
Price Jr, E. B. and Mostofi F. K. (1965) Symptomatic angiomyo- lipoma of the kidney. Cancer 18, 761.
Winter C. C., Chiang M. S. and Wiecher F. (1981) Renal carcinoma discovered after trauma. Ur&gy 18, 492.
Paper accepted 13 October 1988
Requests for reprints should be addressed to: Thomas L. Wachtel MD,
Director, Trauma Service, Good Samaritan Medical Center, 1130 E. McDowell Road, Suite B-2, Phoenix, Arizona, 85006, USA.
Posterior dislocation of the elbow with an osteochondral fracture
N. S. Shankar and A. D. Craxford North Tyneside General Hospital, North Shields, Tyne and Wear
Case report
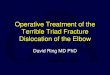
A 23-year-old man fell on his outstretched hand while playing football such that he injured his right elbow. There was no sign of neurovascular deficit. Radiographs revealed a posterior dislocation of the joint with a bony fragment lying in the trochlear notch and a defect in the anterior margin of the olecranon process. (Fig, 1).
0 1989 Butterworth & Co (Publishers) Ltd 0020-1383/89/010051~2 $03.00
After manipulation, screening with the image intensifier showed the fragment to be preventing full extension. At opera- tion, the osteochondral fracture was found to involve nearly half of the posterior aspect of the trochlear notch. There was also some superficial abrasion over the posterior surface of the capitellum and an undisplaced marginal fracture of the head of the radius. The
52 Injury: the British Journal of Accident Surgery (1989) Vol. 20/No. 1
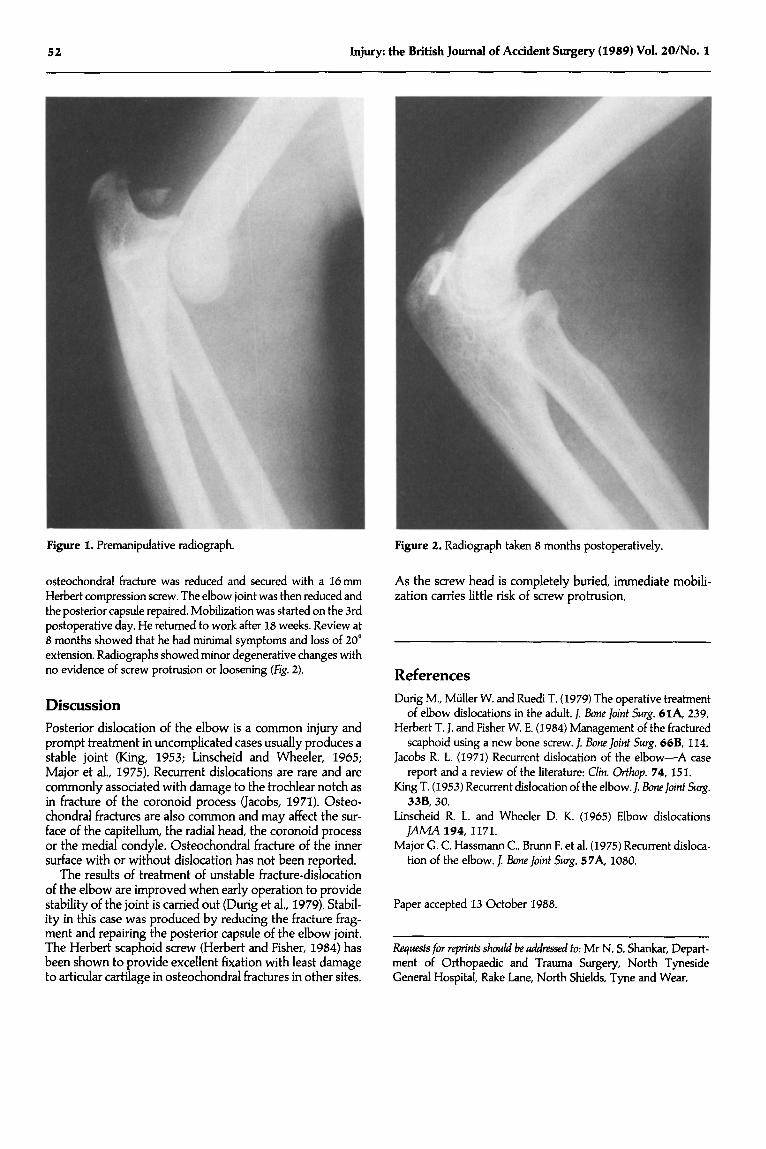
Figure 1. Premanipulative radiograph. Figure 2. Radiograph taken 8 months postoperatively.
osteochondral fracture was reduced and secured with a lbmm
Herbert compression screw. The elbow joint was then reduced and the posterior capsule repaired. Mobilization was started on the 3rd postoperative day. He returned to work after 18 weeks. Review at 8 months showed that he had minimal symptoms and loss of 20” extension. Radiographs showed minor degenerative changes with no evidence of screw protrusion or loosening (Fig. 2).
As the screw head is completely buried, immediate mobili- zation carries little risk of screw protrusion.
References
Discussion
Posterior dislocation of the elbow is a common injury and prompt treatment in uncomplicated cases usually produces a stable joint (King, 1953; Linscheid and Wheeler, 1965; Major et al., 197.9. Recurrent dislocations are rare and are commonly associated with damage to the trochlear notch as in fracture of the coronoid process (Jacobs, 1971). Osteo- chondral fractures are also common and may affect the sur- face of the capitellum, the radial head, the coronoid process or the medial condyle. Osteochondral fracture of the inner surface with or without dislocation has not been reported.
Dung M., Miiller W. and Ruedi T. (1979) The operative treatment of elbow dislocations in the adult. J. Bone]oint Strrg. 6lA, 239.
Herbert T. J. and Fisher W. E. (1984) Management of the fractured scaphoid using a new bone screw. J. Bone]oint Surg. 66B, 114.
Jacobs R. L. (1971) Recurrent dislocation of the elbow-A case report and a review of the literature: Clin. O&op. 74, 15 1.
King T. (1953) Recurrent dislocation of the elbow.]. BoneJoint S~rg. 33B, 30.
Linscheid R. L. and Wheeler D. K. (1965) Elbow dislocations JAA4A 194,117l.
Major G. C. Hassmann C., Brunn F. et al. (1975) Recurrent disloca- tion of the elbow. J Bone Joint Stlrg. 5 7A. 1080.
The results of treatment of unstable fracture-dislocation of the elbow are improved when early operation to provide stability of the joint is carried out (Durig et al., 1979). Stabil- ity in this case was produced by reducing the fracture frag- ment and repairing the posterior capsule of the elbow joint. The Herbert scaphoid screw (Herbert and Fisher, 1984) has been shown to provide excellent fixation with least damage to articular cartilage in osteochondral fractures in other sites.
Paper accepted 13 October 1988.
Requests for reprints should be addressed to: Mr N. S. Shankar, Depart- ment of Orthopaedic and Trauma Surgery, North Tyneside General Hospital, Rake Lane, North Shields, Tyne and Wear.